
Irrigation in Endodontics: Polyhexanide Is a Promising Antibacterial Polymer in Root Canal Treatment
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
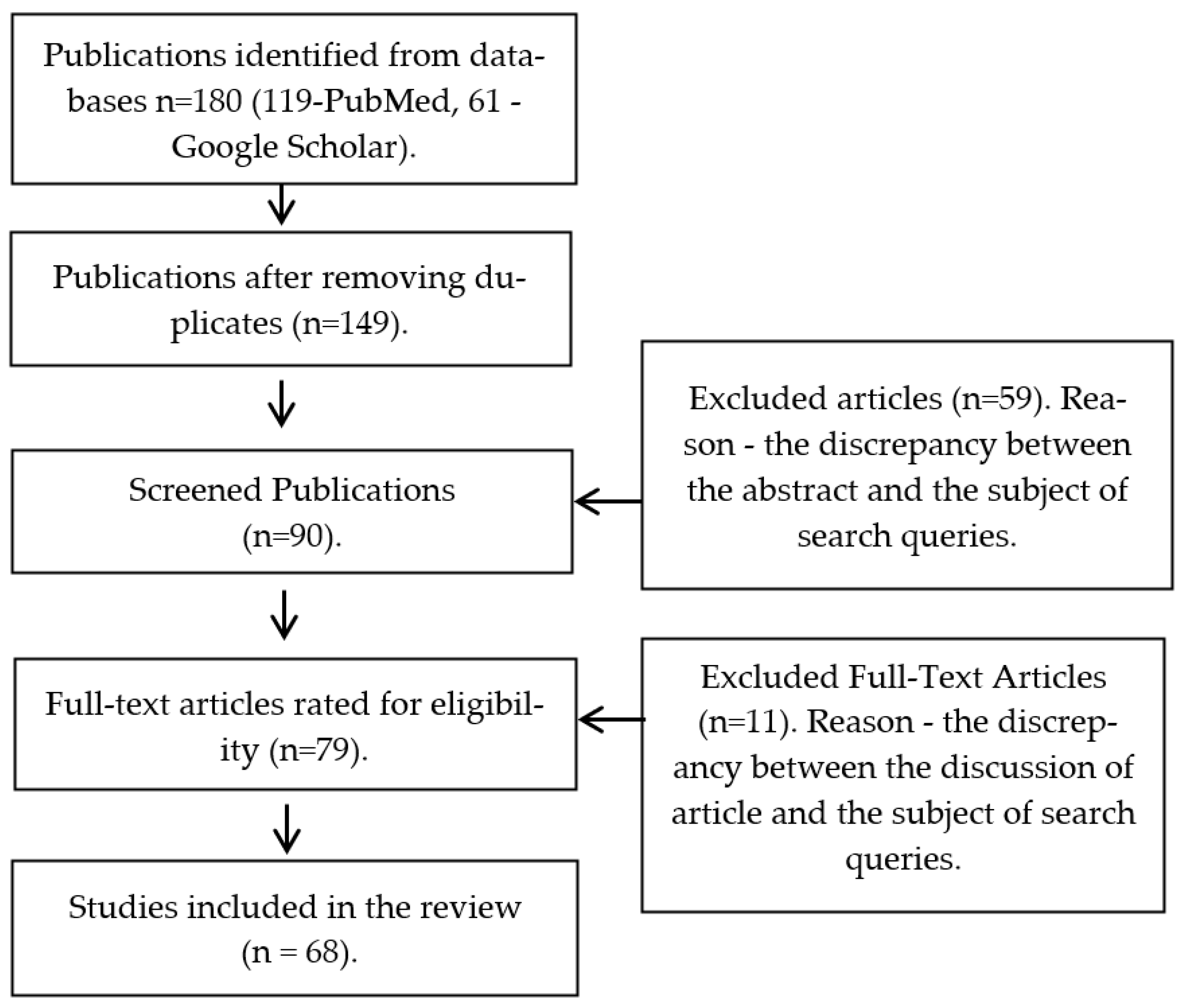
2. Materials and Methods
- (1)
- Articles for the period from 2004 to 2023;
- (2)
- An article describes the composition of the microflora that causes diseases of the pulp and apical periodontium;
- (3)
- An article describes the use of various irrigants in endodontics (sodium hypochlorite, chlorhexidine, EDTA, and citric acid), as well as their interactions with each other;
- (4)
- The research describes the outcomes of polyhexanide use in general medicine and dentistry;
- (5)
- The article describes the spectrum of polyhexanide antimicrobial activity in the bacteria responsible for the occurrence of periodontitis.
3. Results
4. Discussion
4.1. The Role of Root Canal Medical Treatment in the Pulp and Apical Periodontal Inflammatory Diseases. Properties of Irrigants
4.2. General Information about Irrigants
4.3. Interactions between Irrigants
4.4. Polyhexanide Is a Promising Irrigant. General Information and Application in Medicine

{kind=link}
| Authors, Year of Publication | Title of the Article | Polyhexanide Form | Research Method | Tested Microorganisms | Main Conclusions |
|---|---|---|---|---|---|
| Esra Uzer Celik et al, 2016 [60] | Antimicrobial activity of different disinfectants against cariogenic microorganisms | PHMB 0.2% (2000 mg/L) solution | Spectrophotometry to detect MIC, microbial growth on TSA agar to determine the MBC | S. mutans, L. acidophilus, A. viscosus, L. rhamnosus | The lowest MIC and MBC against S. mutans (60 mg/L) were obtained from PHBM. The values of MIC and MBC for other microorganisms ranged from 20 to 120 mg/L |
| Wei Dong; Rui Chen; Yue-Ting Lin; Zi-Xiao Huang; Guang-Jie Bao and Xiang-Yi He, 2020 [60] | A novel zinc oxide eugenol modified by polyhexamethylene biguanide: Physical and antimicrobial properties | Zinc oxide eugenol sealers modified with different concentrations of PHMB (0.05, 0.1, 0.2, 0.4, 0.6, and 0.8%) | The microbiological direct contact test (DCT) | Enterococcus faecalis | Antimicrobial activity of the modified filling material at the level of 85% for 14 days |
| Nai, Z.; Han, Y.; Huang, Z.; Wang, J.; and He, X., 2020 [62] | Physical and biological properties of a novel root canal sealer modified by polyhexamethylene guanidine. | Zinc oxide eugenol fabricated with polyhexamethylene guanidine: 0.8, 1.0, 1.2, and 1.4% | Agar diffusion test and measuring the diameter of inhibition zone | E. faecalis, C. albicans, E. coli, S. aureus | The largest growth retardation zone after incubation at 37 C was demonstrated for E. coli—46.24 mm |
| Zhu, K.; Zheng, L.; Xing, J.; Chen, S.; Chen, R.; and Ren, L., 2022 [63] | Mechanical, antibacterial, biocompatible and microleakage evaluation of glass ionomer cement modified by nanohydroxyapatite/polyhexamethylene biguanide. | Glass ionomer cement modified with nanohydroxyapatite/polyhexamethylene biguanide (0.2, 0.4%) | Direct contact test, WST-8 assay | S. mutans | Modified GIC’s antibacterial rate vigorously raised to 88.5% compared with pure GIC. Addition of PHMB 0.4% increased the level of antimicrobial activity up to 96.5% |
| Mikic, I.M.; Andrasevic, A.T.; Prpic-Mehicic, G.; Matijevic, J.; Tadin, A.; and Simeon, P. P., 2013 [11] | The effect of polyhexamethylen biguanide on microorganisms in root canal | Bigvasan IB10 (Arch Chemicals. Inc., Norwalk, UK)—polyhexamethylen biguanide (PHMB) in concentration of 0.2% | Counting of colony-forming units during cultivation on blood agar after PHMB use and average colony-forming units per milliliter (CFU/mL) was calculated and log10-transformed | E. faecalis, P. aeruginosa, C. albicans | In eight of eleven samples infected with E. faecalis, no bacterial growth was obtained after irrigation with 0.2% polyhexanide, in three samples the contamination was 101–103 CFU/mL, in six samples infected with C. Albicans there was no further cell growth after treatment with Polyhexanide, and in five samples the contamination was 101 CFU/mL |
| Mikić, I.M.; Cigić, L.; Kero, D.; Govorko, D.K.; Mehičić, G.P.; and Simeon, P., 2018 [65] | Antimicrobial effectiveness of polyhexamethylene biguanide on Enterococcus faecalis, Staphylococcus epidermidis and Candida albicans. | 0.2% PHMB solution | Counting of colony-forming units during cultivation on blood agar after PHMB, then multiplied with the dilution factor and converted to CFU/mL | E. faecalis, S. epidermidis and C. albicans | The PHMB was significantly more efficient at reducing the number of all three tested microorganisms. The elimination of enterococcus and Candida was determined from 103–104 to 0 CFU/mL |
| Dammaschke, T.; Jung, N.; Harks, I.; and Schafer, E., 2013 [66] | The effect of different root canal medicaments on the elimination of Entero-coccus faecalis ex vivo. | Prontosan (B. Braun Meslungen AG, Melsungen, Germany)—0.1% PHMB | The CFU was counted at 8-fold magnification using a stereomicroscope, then multiplied with the dilution factor and converted to CFU/mL, subsequently | E. faecalis | Polyhexanide showed the lowest values of activity against E. faecalis compared with CHX 2% gel, 1% powder, Povidone-iodine, and ChKM |
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Henriques, L.C.F.; de Brito, L.C.N.; Tavares, W.L.F.; Teles, R.P.; Vieira, L.Q.; Teles, F.R.F.; Sobrinho, A.P.R. Microbial ecosystem analysis in root canal infections refractory to endodontic treatment. J. Endod. 2016, 42, 1239–1245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Orrų, B.; Lista, P.; Bertelli, M.; Unfer, V. Safety assessment of Polyhexamethylene biguanide. IJMDAT 2019, 2, e210. [Google Scholar] [CrossRef]
- Vitt, A.; Babenka, A.; Boström, E.A.; Gustafsson, A.; Lira Junior, R.; Slizen, V.; Sorsa, T.; Tervahartiala, T.; Buhlin, K. Adjunctive Antiseptic Irrigation of Periodontal Pockets: Effects on Microbial and Cytokine Profiles. Dent. J. 2020, 8, 124. [Google Scholar] [CrossRef] [PubMed]
- Qian, W.; Ma, T.; Ye, M. Microbiota in the apical root canal system of tooth with apical periodontitis. BMC Genom. 2019, 20, 175–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouillaguet, S.; Manoil, D.; Girard, M.; Louis, J.; Gaïa, N.; Leo, S.; Schrenzel, J.; Lazarevic, V. Root Microbiota in Primary and Secondary Apical Periodontitis. Front. Microbiol. 2018, 9, 2374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hübner, N.O.; Kramer, A. Review on the efficacy, safety and clinical applications of polihexanide, a modern wound antiseptic. Ski. Pharmacol. Physiol. 2010, 23 (Suppl. 1), 17–27. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rôças, I.N. Microbiology of apical periodontitis. In Essential Endodontology: Prevention and Treatment of Apical Periodontitis, 3rd ed.; Ørstavik, D., Ed.; John Willey & Sons Ltd.: Chichester, UK, 2019; pp. 91–142. [Google Scholar] [CrossRef]
- Hashemi, M.M.; Holden, B.S.; Coburn, J.; Taylor, M.F.; Weber, S.; Hilton, B.; Savage, P.B. Proteomic analysis of resistance of Gram-negative bacteria to chlorhexidine and impacts on susceptibility to colistin, antimicrobial peptides, and ceragenins. Front. Microbiol. 2019, 10, 210. [Google Scholar] [CrossRef] [Green Version]
- Lenselink, E.; Andriessen, A. A cohort study on the efficacy of a polyhexa-nide-containing biocellulose dressing in the treatment of biofilms in wounds. J. Wound Care 2011, 20, 534–539. [Google Scholar] [CrossRef]
- Josic, U.; Mazzitelli, C.; Maravic, T.; Fidler, A.; Breschi, L.; Mazzoni, A. Biofilm in Endodontics: In Vitro Cultivation Possibilities, Sonic-, Ultrasonic- and Laser-Assisted Removal Techniques and Evaluation of the Cleaning Efficacy. Polymers 2022, 14, 1334. [Google Scholar] [CrossRef]
- Mikic, I.M.; Andrasevic, A.T.; Prpic-Mehicic, G.; Matijevic, J.; Tadin, A.; Simeon, P.P. The effect of polyhexamethylen biguanide on microorganisms in root canal/Utjecaj poliheksametilenova bigvanida na mikroorganizme u korijenskom kanalu zuba. Acta Stomatol. Croat. 2013, 47, 120–127. [Google Scholar] [CrossRef]
- Kandaswamy, D.; Venkateshbabu, N. Root canal irrigants. J. Conserv. Dent. 2010, 13, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, A.; Bolla, N.; Sarath, R.K.; Ram, C.S. Assessment of precipitate formation on interaction of irrigants used in different combinations: An in vitro study. Indian J. Dent. Res. 2013, 24, 451. [Google Scholar] [CrossRef] [PubMed]
- Topbas, C.; Adiguzel, O. Endodontic Irrigation Solutions: A Review: Endodontic Irrigation Solutions. Int. Dent. Res. 2017, 7, 54–61. [Google Scholar] [CrossRef] [Green Version]
- Arratia, M.M.; de Lourdes Lanzagorta Rebollo, M.; Flores, F.J.P.; Contreras, R.G.; Soriano, J.L.M.; Fernández Presas, A.M. Detection of Para-Chloroaniline Resulting from the Interaction between Sodium Hypochlorite and Chlorhexidine Analyzed by Mass Spectrometry. Am. J. Anal. Chem. 2019, 10, 629–640. [Google Scholar] [CrossRef] [Green Version]
- Gomes, B.P.; Vianna, M.E.; Zaia, A.A.; Almeida, J.F.A.; Souza-Filho, F.J.; Ferraz, C.C. Chlorhexidine in endodontics. Braz. Dent. J. 2013, 24, 89–102. [Google Scholar] [CrossRef] [PubMed]
- Prado, M.; Júnior, H.M.S.; Rezende, C.M.; Pinto, A.C.; Faria, R.B.; Simão, R.A.; Gomes, B.P. Interactions between irrigants commonly used in endodontic practice: A chemical analysis. J. Endod. 2013, 39, 505–510. [Google Scholar] [CrossRef] [PubMed]
- Mampilly, J.; Shetty, K.V.; Shetty, H.S. Endodontic irrigating solutions, disinfection devices and techniques: A review. IOSR J. Dent. Med. Sci. 2020, 19, 986–997. [Google Scholar] [CrossRef] [Green Version]
- Jena, A.; Sahoo, S.K.; Govind, S. Root canal irrigants: A review of their interactions, benefits, and limitations. Compend. Contin. Educ. Dent. 2015, 36, 256–261. [Google Scholar]
- Wright, P.P.; Kahler, B.; Walsh, L.J. Alkaline Sodium Hypochlorite Irrigant and Its Chemical Interactions. Materials 2017, 10, 1147. [Google Scholar] [CrossRef] [Green Version]
- Dirk, W. Lachenmeier. Antiseptic Drugs and Disinfectants. In Side Effects of Drugs Annual; Ray, S.D., Ed.; Elsevier: Amsterdam, The Netherlands, 2016; Volume 38, Chapter 22; pp. 211–216. [Google Scholar] [CrossRef]
- Agrawal Vineet, S.; Rajesh, M.; Sonali, K.; Mukesh, P. A Contemporary Overview of Endodontic Irrigants—A Review. J. Dent. App. 2014, 1, 105–115. [Google Scholar]
- Abraham, S.; Raj, J.D.; Venugopal, M. Endodontic irrigants: A comprehensive review. J. Pharm. Sci. Res. 2015, 7, 5–9. [Google Scholar]
- Anna, H.; Barnabás, P.; Zsolt, L.; Romána, Z. Tracking of the degradation process of chlorhexidine digluconate and ethylenediaminetetraacetic acid in the presence of hyper-pure chlorine dioxide in endodontic disinfection. J. Pharm. Biomed. Anal. 2019, 164, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Abusrewil, S.; Brown, J.L.; Delaney, C.D.; Butcher, M.C.; Kean, R.; Gamal, D.; Scott, J.A.; McLean, W.; Ramage, G. Filling the Void: An Optimized Polymicrobial Interkingdom Biofilm Model for Assessing Novel Antimicrobial Agents in Endodontic Infection. Microorganisms 2020, 8, 1988. [Google Scholar] [CrossRef] [PubMed]
- Marion, J.; Pavan, K.; Arruda, M.E.B.F.; Nakashima, L.; Morais, C.A.H. Chlorhexidine and its applications in Endodontics: A literature review. Dent. Press Endod 2013, 3, 36–54. [Google Scholar]
- Sabadin, N.; Böttcher, D.E.; Hoppe, C.B.; Santos, R.B.D.; Grecca, F.S. Resin-based sealer penetration into dentinal tubules after the use of 2% chlorhexidine gel and 17% EDTA: In vitro study. Braz. J. Oral Sci. 2014, 13, 308–313. [Google Scholar] [CrossRef] [Green Version]
- Rusu, D.; Stratul, S.-I.; Sarbu, C.; Roman, A.; Anghel, A.; Didilescu, A.; Jentsch, H. Evaluation of a hydrophobic gel adhering to the gingiva in comparison with a standard water-soluble 1% chlorhexidine gel after scaling and root planing in patients with moderate chronic periodontitis. A randomized clinical trial. Int. J. Dent. Hyg. 2017, 15, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, Z.; Giardino, L.; Palazzi, F.; Asgary, S. Agonistic and Antagonistic Interactions between Chlorhexidine and Other Endodontic Agents: A Critical Review. Iran Endod J. 2015, 10, 1–5. [Google Scholar] [CrossRef]
- Bernardi, A.; Teixeira, C.S. The properties of chlorhexidine and undesired effects of its use in endodontics. Quintessence Int. 2015, 46, 575–582. [Google Scholar] [CrossRef]
- Noor, S.S.S.E. Chlorhexidine: Its properties and effects. Res. J. Pharm. Technol. 2016, 9, 1755–1760. [Google Scholar] [CrossRef]
- Clarkson, R.M.; Podlich, H.M.; Moule, A.J. Influence of ethylenediaminetetraacetic acid on the active chlorine content of sodium hypochlorite solutions when mixed in various proportions. J. Endod. 2011, 37, 538–543. [Google Scholar] [CrossRef]
- Niazi, S.A.; Al-Ali, W.M.; Patel, S.; Foschi, F.; Mannocci, F. Synergistic effect of 2% chlorhexidine combined with proteolytic enzymes on biofilm disruption and killing. Int. Endod. J. 2015, 48, 1157–1167. [Google Scholar] [CrossRef] [PubMed]
- Prada, I.; Micó-Muñoz, P.; Giner-Lluesma, T.; Micó-Martínez, P.; Collado-Castellano, N.; Manzano-Saiz, A. Influence of microbiology on endodontic failure. Literature review. Med. Oral Patol. Oral Cir. Bucal. 2019, 24, e364. [Google Scholar] [CrossRef] [PubMed]
- Lisa, E.L.; Carac, G.; Lupu, I.T.; Iliescu, A.; Iliescu, A.A. Chemical Interactions among Some Antimicrobial Solutions and Chelating Agents Used in Endodontics for Irrigation of Infected Root Canals. Rev. Chim. 2017, 68, 1490–1495. [Google Scholar] [CrossRef]
- Verspecht, T.; Rodriguez Herrero, E.; Khodaparast, L.; Khodaparast, L.; Boon, N.; Bernaerts, K.; Quirynen, M.; Teughels, W. Development of antiseptic adaptation and cross-adapatation in selected oral pathogens in vitro. Sci. Rep. 2019, 9, 8326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez Herrero, E.; Boon, N.; Pauwels, M.; Bernaerts, K.; Slomka, V.; Quirynen, M.; Teughels, W. Necrotrophic growth of periodontopathogens is a novel virulence factor in oral biofilms. Sci. Rep. 2017, 7, 1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alegre, O.; Yévenes, I.; Parada, J.; Maggiolo, S.; Fernández, E. Determination of residual parachloroaniline produced by endodontic treatment after the use of 5% sodium hypochlorite and 2% chlorhexidine combined: An ex-vivo study. Rev. Clin. Periodoncia Implantol. Rehabil. 2017, 10, 145–148. [Google Scholar] [CrossRef] [Green Version]
- Kaehn, K. Polihexanide: A safe and highly effective biocide. Ski. Pharmacol. Physiol. 2010, 23 (Suppl. 1), 7–16. [Google Scholar] [CrossRef] [PubMed]
- De Paula, G.F.; Netto, G.I.; Mattoso, L.H.C. Physical and Chemical Characterization of Poly(hexamethylene biguanide) Hydrochlo-ride. Polymers 2011, 3, 928–941. [Google Scholar] [CrossRef]
- Niro, A.; Pignatelli, F.; Fallico, M.; Sborgia, A.; Passidomo, F.; Gigliola, S.; Nacucchi, A.; Sborgia, G.; Boscia, G.; Alessio, G.; et al. Polyhexamethylene biguanide hydrochloride (PHMB)-properties and application of an antiseptic agent. A narrative review. Eur. J. Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Ntow-Boahene, W.; Papandronicou, I.; Miculob, J.; Good, L. Fungal cell barriers and organelles are disrupted by Polyhexamethylene biguanide (PHMB). Res. Sq. 2022; preprint. [Google Scholar] [CrossRef]
- Eberlein, T.; Assadian, O. Clinical Use of Polihexanide on Acute and Chronic Wounds for Antisepsis and Decontamination. Ski. Pharmacol. Physiol. 2010, 23, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Dissemond, J.; Gerber, V.; Kramer, A.; Riepe, G.; Strohal, R.; Vasel-Biergans, A.; Eberlein, T. A practice-oriented recommendation for treatment of critically colonised and locally infected wounds using polyhexanide. J. Tissue Viability 2010, 19, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.C.; Harding, A.; Gil, J.; Parajon, F.; Valdes, J.; Solis, M.; Higa, A. Effectiveness of a polyhexa-nide irrigation solution on methicillin-resistant Staphylococcus aureus biofilms in a porcine wound model. Int. Wound J. 2017, 14, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Wang, D.; Ma, L.Z. Effect of Polyhexamethylene Biguanide in Combination with Undecylenamidopropyl Betaine or PslG on Biofilm Clearance. Int. J. Mol. Sci. 2021, 22, 768. [Google Scholar] [CrossRef] [PubMed]
- Minnich, K.E. The effect of a wound care solution containing polyhexanide and betaine on bacterial counts: Results of an in vitro study. Ostomy-Wound Manag. 2012, 58, 32. [Google Scholar]
- Koburger, T.; Hübner, N.-O.; Braun, M.; Siebert, J.; Kramer, A. Standardized comparison of antiseptic efficacy of triclosan, PVP–iodine, octenidine dihydrochloride, polyhexanide and chlorhexidine digluconate. J. Antimicrob. Chemother. 2010, 65, 1712–1719. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramasamy, S.; Muthusamy, S.; Nagarajan, S.; Nath, A.V.; Savarimuthu, J.S.; Jayaprakash, J.; Gurunadhan, R.M. Fabrication of collagen with polyhexamethylene biguanide: A potential scaffold for infected wounds. J. Biomed. Mater. Res. Part B Appl. Biomater. 2022, 110, 535–546. [Google Scholar] [CrossRef]
- Timmers, M.S.; Graafland, N.; Bernards, A.T.; Nelissen, R.G.H.H.; Van Dissel, J.T.; Jukema, G.N. Negative pressure wound treatment with polyvinyl alcohol foam and polyhexanide antiseptic solution instillation in posttraumatic osteomyelitis. Wound Repair Regen. 2009, 17, 278–286. [Google Scholar] [CrossRef]
- Brill, F.H.H.; Gabriel, H.; Brill, H.; Klock, J.H.; Steinmann, J.; Arndt, A. Decolonization potential of 0.02% polyhexanide irrigation solution in urethral catheters under practice-like in vitro conditions. BMC Urol. 2018, 18, 49. [Google Scholar] [CrossRef] [Green Version]
- Brill, F.H.H.; Hambach, J.; Utpatel, C.; Mogrovejo, D.C.; Gabriel, H.; Klock, J.H.; Steinmann, J.; Arndt, A. Biofilm reduction potential of 0.02% polyhexanide irrigation solution in several types of urethral catheters. BMC Urol. 2021, 21, 58. [Google Scholar] [CrossRef]
- Andersen, L.; Bertelsen, M.; Buitenhuis, V.; Carstensen, A.; Hannibalsen, J.; Larsen, B.H.; Hvirvlkær, R.; Malinowska, Z.A.; Pedersen, B.; Würtz, S.U.-B. Maintenance of indwelling urinary catheters with a novel polyhexanide-based solution: User experience. Br. J. Nurs. 2020, 29, 18–28. [Google Scholar] [CrossRef]
- Gentile, A.; Gerli, S.; Di Renzo, G.C. A new non-invasive approach based on polyhexamethylene biguanide increases the regression rate of HPV infection. BMC Clin. Pathol. 2012, 12, 17. [Google Scholar] [CrossRef] [Green Version]
- Zimmer, M.; Huras, H.; Kaminski, P.; Karowicz-Bilinska, A.; Drews, K.; Fuchs, T.; Pomorski, M. Polish Society of Gynecologists and Obstetricians recommendation on the use of antiseptics for treatment of inflammatory vaginitis. Ginekol. Polska. 2020, 91, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Papa, V.; van Der Meulen, I.J.; Rottey, S.; Sallet, G.; Overweel, I.; op’t Hof, M.; Dart, J.K.G. Ocular safety of high doses Polyhexanide (PHMB) in healthy volunteers. Investig. Ophthalmol. Vis. Sci. 2017, 58, 5170. [Google Scholar]
- Behrens-Baumann, W.; Seibold, M.; Hofmüller, W.; Walter, S.; Haeberle, H.; Wecke, T.; Tintelnot, K. Benefit of polyhexamethylene biguanide in Fusarium keratitis. Ophthalmic Res. 2012, 48, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Jhanji, V.; Satpathy, G.; Sharma, N.; Khokhar, S.; Agarwal, T. Coinfection with Acanthamoe-ba and Pseudomonas in contact lens–associated keratitis. Optom. Vis. Sci. 2013, 90, e53–e55. [Google Scholar] [CrossRef] [PubMed]
- Tuft, S.; Bunce, C.; De, S.; Thomas, J. Utility of investigation for suspected microbial keratitis: A diagnostic accuracy study. Eye 2023, 37, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Uzer Celik, E.; Tunac, A.T.; Ates, M.; Sen, B.H. Antimicrobial activity of different disinfectants against cariogenic microorganisms. Braz. Oral Res. 2016, 30, e125. [Google Scholar] [CrossRef] [Green Version]
- Dong, W.; Chen, R.; Lin, Y.T.; Huang, Z.X.; Bao, G.J.; He, X.Y. A novel zinc oxide eugenol modified by polyhexamethylene biguanide: Physical and antimicrobial properties. Dent. Mater. J. 2020, 39, 200–205. [Google Scholar] [CrossRef]
- Nai, Z.; Han, Y.; Huang, Z.; Wang, J.; He, X. Physical and biological properties of a novel root canal sealer modified by polyhexamethylene guanidine. Dent. Mater. J. 2020, 39, 141–147. [Google Scholar] [CrossRef]
- Zhu, K.; Zheng, L.; Xing, J.; Chen, S.; Chen, R.; Ren, L. Mechanical, antibacterial, biocompatible and microleakage evaluation of glass ionomer cement modified by nanohydroxyapatite/polyhexamethylene biguanide. Dent. Mater. J. 2022, 41, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Mergoni, G.; Percudani, D.; Lodi, G.; Bertani, P.; Manfredi, M. Prevalence of Candida species in endodontic infections: Systematic review and meta-analysis. J. Endod. 2018, 44, 1616–1625. [Google Scholar] [CrossRef] [PubMed]
- Mikić, I.M.; Cigić, L.; Kero, D.; Govorko, D.K.; Mehičić, G.P.; Simeon, P. Antimicrobial effectiveness of polyhexamethylene biguanide on Enterococcus faecalis, Staphylococcus epidermidis and Candida albicans. Med. Glas. 2018, 15, 132–138. [Google Scholar] [CrossRef]
- Dammaschke, T.; Jung, N.; Harks, I.; Schafer, E. The effect of different root canal medicaments on the elimination of Enterococcus faecalis ex vivo. Eur. J. Dent. 2013, 7, 442–448. [Google Scholar] [CrossRef]
- Rita, C.; Nikhil, V.; Surapaneni, S.K. Determination of Minimum Inhibitory Concentration (MIC) of a PolyHexamethylene Biguanide (PHMB) Solution: A Potential Root Canal Irrigant. Annu. Res. Rev. Biol. 2017, 15, 1–7. [Google Scholar] [CrossRef]
- Khan, A.; Nikhil, V.; Pandey, A.; Chaturvedi, P. Effectiveness of polyhexamethylene biguanide, chlorhexidine, and calcium hydroxide intracanal medicament against intraradicular mature polymicrobial biofilm: A microbiological study. J. Conserv. Dent. 2022, 25, 536–540. [Google Scholar] [CrossRef] [PubMed]

| Sodium Hypo-chlorite | Chlorhexidine | EDTA | Citric Acid | |
|---|---|---|---|---|
| Sodium hypochlorite | The formation of an insoluble red-brown or orange-brown precipitate-parachloraniline (PCA) [12,13,18,35,36,37,38]. | The neutralization reaction occurs with the formation of HOCl, which then decomposes with the release of a small amount of free chlorine and oxygen, which reduces its antibacterial and proteolytic properties [20,36,37]. | There is a decrease in the effectiveness of sodium hypochlorite, which is similar to that described for NaOCl and EDTA [36]. | |
| Chlorhexidine | A white-milk precipitate is formed—a “white cloud reaction”. The precipitate is made up of crystals of pure chlorhexidine, which dissolves with a pH change [32,36,37]. | With citric acid chlorhexidine forms a milky solution, which is similar to that described for EDTA [36]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khabadze, Z.; Generalova, Y.; Kulikova, A.; Podoprigora, I.; Abdulkerimova, S.; Bakaev, Y.; Makeeva, M.; Dashtieva, M.; Balashova, M.; Gadzhiev, F.; et al. Irrigation in Endodontics: Polyhexanide Is a Promising Antibacterial Polymer in Root Canal Treatment. Dent. J. 2023, 11, 65. https://doi.org/10.3390/dj11030065
Khabadze Z, Generalova Y, Kulikova A, Podoprigora I, Abdulkerimova S, Bakaev Y, Makeeva M, Dashtieva M, Balashova M, Gadzhiev F, et al. Irrigation in Endodontics: Polyhexanide Is a Promising Antibacterial Polymer in Root Canal Treatment. Dentistry Journal. 2023; 11(3):65. https://doi.org/10.3390/dj11030065
Chicago/Turabian StyleKhabadze, Zurab, Yulia Generalova, Alena Kulikova, Irina Podoprigora, Saida Abdulkerimova, Yusup Bakaev, Mariya Makeeva, Marina Dashtieva, Mariya Balashova, Fakhri Gadzhiev, and et al. 2023. "Irrigation in Endodontics: Polyhexanide Is a Promising Antibacterial Polymer in Root Canal Treatment" Dentistry Journal 11, no. 3: 65. https://doi.org/10.3390/dj11030065