
Comparative Study of Transmission of 2940 nm Wavelength in Six Different Aesthetic Orthodontic Brackets


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
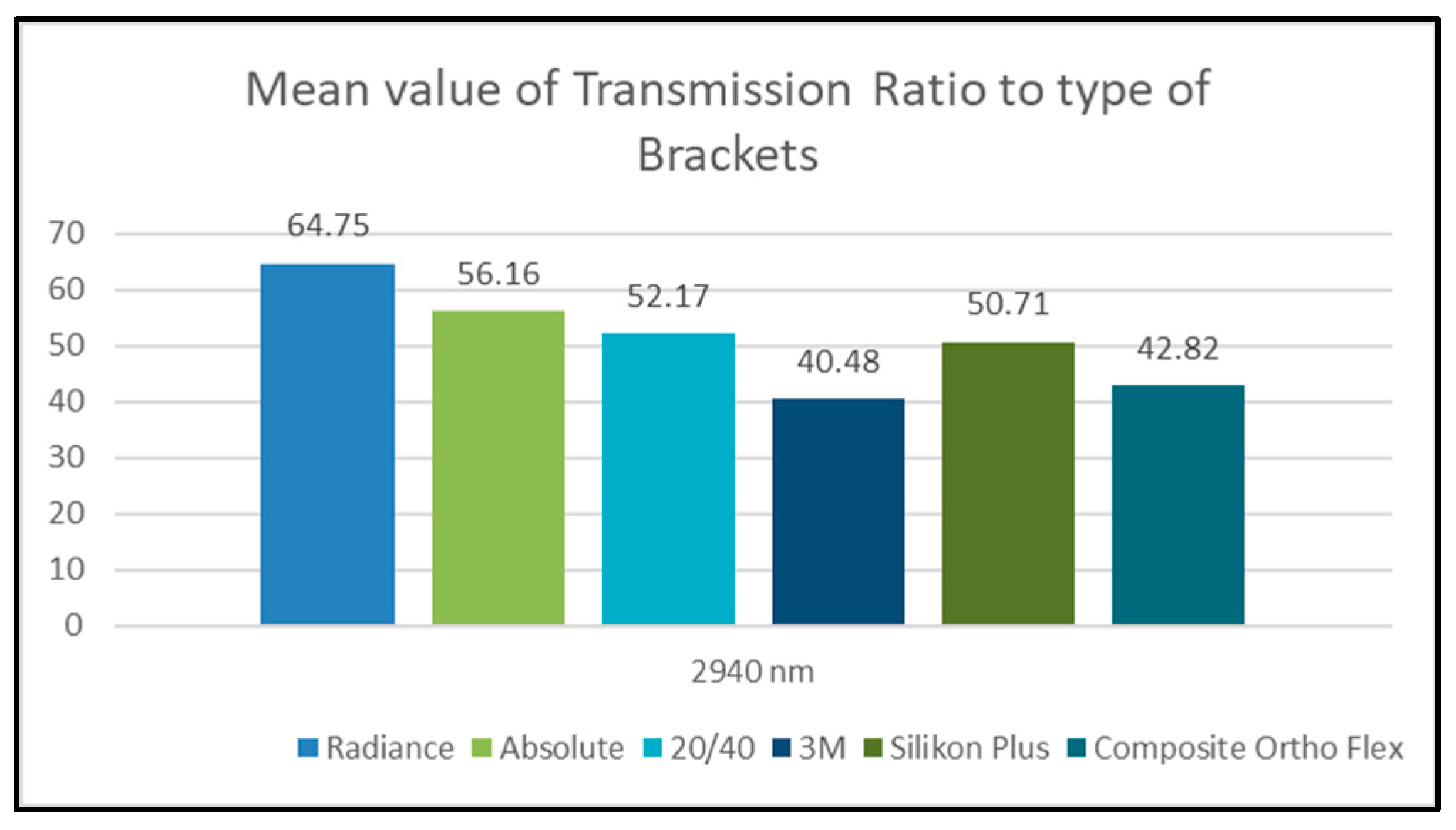
Effect of Type of Bracket on Transmission Ratio Values at 2940 nm Wavelength
- -
- One-Way ANOVA test results:
- -
- Bonferroni post-hoc test results:
- -
- The transmission ratio values of the Radiance group were greater than those of all the other groups.
- -
- The transmission ratio values of the Absolute group were greater than those of four other groups (20/40, 3M, Silkon Plus, and Composite Ortho Flex).
- -
- The transmission ratio values of the 20/40 group were greater than those of three other groups (3M, Silkon Plus, and Composite Ortho Flex).
- -
- The transmission ratio values of the Silkon Plus group were greater than those of both the 3M and Composite Ortho Flex groups.
- -
- The transmission ratio values of the Composite Ortho Flex group were greater than those of the 3M group (Figure 3).
4. Discussion
5. Conclusions
- Among the studied aesthetic brackets, the monocrystalline sapphire brackets have the highest transmissibility for the 2940 nm wavelength.
- The thick polycrystalline and composite brackets have the lowest transmissibility for the 2940 nm wavelength.
- The high transmission values of the tested wavelength within the monocrystalline sapphire brackets indicate that less pulse power and energy are required from the laser in order to achieve ablative debonding.
- After testing all the other related factors, the good transmission values of the silicon brackets lead us to consider using a 2940 nm wavelength laser for debonding.
- The relatively high transmission values of the monocrystalline sapphire brackets increase the possibility that they can be debonded using a hard tissue laser with a thermal ablation mechanism.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alakus Sabuncuoglu, F.; Ersahan, S.; Erturk, E. Debonding of ceramic brackets by Er:YAG laser. J. Istanb. Univ. Fac. Dent. 2016, 50, 24–30. [Google Scholar] [CrossRef]
- Matos, D.S.; Kuchler, E.C.; Borsatto, M.C.; Matsumoto, M.A.N.; Marques, F.V.; Romano, F.L. CO2 laser irradiation for debonding ceramic orthodontic brackets. Braz. Dent. J. 2021, 32, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Azzeh, E.; Feldon, P. Laser debonding of ceramic brackets: A comprehensive review. Am. J. Orthod. Dentofac. Orthop. 2003, 123, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Swartz, M.L. Ceramic brackets. J. Clin. Orthod. 1988, 22, 82–88. [Google Scholar]
- Namura, Y.; Uchida, Y. Influence of masticating cycles and chewing patterns on inadvertent enamel wear caused by zirconia brackets. Eur. J. Oral Sci. 2022, 130, e12831. [Google Scholar] [CrossRef] [PubMed]
- Gohring, T.N.; Gallo, L.; Luthy, H. Effect of water storage, thermocycling, the incorporation and site of placement of glass-fibers on the flexural strength of veneering composite. Dent. Mater. 2005, 21, 761–772. [Google Scholar] [CrossRef] [PubMed]
- Rantala, L.I.; Lastumaki, T.M.; Peltomaki, T.; Vallittu, P.K. Fatigue resistance of removable orthodontic appliance reinforced with glass fibre weave. J. Oral Rehabil. 2003, 30, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.H.; Kao, C.T. The shear bond strength of composite brackets on porcelain teeth. Eur. J. Orthod. 2001, 23, 433–439. [Google Scholar] [CrossRef] [Green Version]
- Faltermeier, A.; Rosentritt, M.; Faltermeier, R.; Müssig, D. Influence of fibre and filler reinforcement of plastic brackets: An in vitro study. Eur. J. Orthod. 2007, 29, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Faltermeier, A.; Rosentritt, M.; Reicheneder, C.; Mussig, D. Experimental composite brackets: Influence of filler level on the mechanical properties. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 699.e9–699.e14. [Google Scholar] [CrossRef]
- Ghaffari, H.; Mirhashemi, A.; Baherimoghadam, T.; Azmi, A.; Rasooli, R. Effect of Surface Treatment on Enamel Cracks After Orthodontic Bracket Debonding: Er,Cr:YSGG Laser-Etching Versus Acid-Etching. J. Dent. 2017, 14, 259–266. [Google Scholar]
- Ajwa, N.; Alfayez, H.; Al-Oqab, H.; Melibary, R.; Alzamil, Y. The Effect of Erbium-Doped Yttrium Aluminum Garnet Laser in Debonding of Orthodontic Brackets: A Systematic Review of the Literature. Photobiomodul. Photomed. Laser Surg. 2021, 39, 725–733. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.S.; Tamish, N.M.; Elkalza, A.R. Assessment of chemical, ultrasonic, diode laser, and Er:YAG laser application on debonding of ceramic brackets. BMC Oral Health 2022, 22, 79. [Google Scholar] [CrossRef] [PubMed]
- Williams, O.L.; Bishara, S.E. Patient discomfort levels at the time of debonding: A pilot study. Am. J. Orthod. Dentofac. Orthop. 1992, 101, 313–317. [Google Scholar] [CrossRef] [PubMed]
- Arici, S.; Minors, C. The force levels required to mechanically debond ceramic brackets: An in vitro comparative study. Eur. J. Orthod. 2000, 22, 327–334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theodorakopoulou, L.P.; Sadowsky, P.L.; Jacobson, A.; Lacefield, W., Jr. Evaluation of the debonding characteristics of 2 ceramic brackets: An in vitro study. Am. J. Orthod. Dentofac. Orthop. 2004, 125, 329–336. [Google Scholar] [CrossRef] [PubMed]
- Bishara, S.E.; Fehr, D.E. Ceramic brackets: Something old, something new, a review. Semin. Orthod. 1997, 3, 178–188. [Google Scholar] [CrossRef]
- Krell, K.V.; Courey, J.M.; Bishara, S.E. Orthodontic bracket removal using conventional and ultrasonic debonding techniques, enamel loss, and time requirements. Am. J. Orthod. Dentofac. Orthop. 1993, 103, 258–266. [Google Scholar] [CrossRef]
- Bishara, S.E.; Trulove, T.S. Comparisons of different debonding techniques for ceramic brackets: An in vitro study. Part II. Findings and clinical implications. Am. J. Orthod. Dentofac. Orthop. 1990, 98, 263–273. [Google Scholar] [CrossRef]
- Sinha, P.K.; Nanda, R.S. The effect of different bonding and debonding techniques on debonding ceramic orthodontic brackets. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 132–137. [Google Scholar] [CrossRef]
- Bishara, S.E.; Fonseca, J.M.; Boyer, D.B. The use of debonding pliers in the removal of ceramic brackets: Force levels and enamel cracks. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Karamouzos, A.; Athanasiou, A.E.; Papadopoulos, M.A. Clinical characteristics and properties of ceramic brackets: A comprehensive review. Am. J. Orthod. Dentofac. Orthop. 1997, 112, 34–40. [Google Scholar] [CrossRef] [PubMed]
- Jena, A.K.; Duggal, R.; Mehrotra, A.K. Physical properties and clinical characteristics of ceramic brackets; a comprehensive review. Biomater. Artif. Organs 2007, 20, 101–115. [Google Scholar]
- Russell, J.S. Aesthetic orthodontic brackets. J. Orthod. 2005, 32, 146–163. [Google Scholar] [CrossRef]
- Ghafari, J. Problems associated with ceramic brackets suggest limiting use to selected teeth. Angle Orthod. 1992, 62, 145–152. [Google Scholar] [CrossRef]
- Vukovich, M.E.; Wood, D.P.; Daley, T.D. Heat generated by grinding during removal of ceramic brackets. Am. J. Orthod. Dentofac. Orthop. 1991, 99, 505–512. [Google Scholar] [CrossRef]
- Boyer, D.B.; Engelhardt, G.; Bishara, S.E. Debonding orthodontic ceramic brackets by ultrasonic instrumentation. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 262–266. [Google Scholar] [CrossRef]
- Sheridan, J.J.; Brawley, G.; Hastings, J. Electrothermal debracketing. Part II. An in vivo study. Am. J. Orthod. 1986, 89, 141–145. [Google Scholar] [CrossRef]
- Dovgan, J.S.; Walton, R.; Bishara, S.E. Comment on electrothermal debonding. Am. J. Orthod. Dentofac. Orthop. 1996, 109, 15A. [Google Scholar]
- Hayakawa, K. Nd: YAG laser for debonding ceramic orthodontic brackets. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 638–647. [Google Scholar] [CrossRef]
- Rickabaugh, J.L.; Marangoni, R.D.; McCaffrey, K.K. Ceramic bracket debonding with the carbon dioxide laser. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Dostalova, T.; Jelinkova, H.; Sulc, J.; Nemec, M.; Jelinek, M.; Fibrich, M.; Michalik, P.; Miyagi, M.; Seydlova, M. Ceramic bracket debonding by Tm:YAP laser irradiation. Photomed. Laser Surg. 2011, 29, 477–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarp, A.S.K.; Gülsoy, M. Ceramic bracket debonding with ytterbium fiber laser. Lasers Med. Sci. 2010, 26, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Stein, S.; Kleye, A.; Schauseil, M.; Hellak, A.; Korbmacher-Steiner, H.; Braun, A. 445-nm diode laser-assisted debonding of self-ligating ceramic brackets. Biomed. Technik. Biomed. Eng. 2017, 62, 513–520. [Google Scholar] [CrossRef]
- Mesaroș, A.; Mesaroș, M.; Buduru, S. Orthodontic Bracket Removal Using LASER-Technology—A Short Systematic Literature Review of the Past 30 Years. Materials 2022, 15, 548. [Google Scholar] [CrossRef]
- Hamadah, O.; Bachir, W.; Zamzam, M. Thermal Effect of Er:YAG Laser Pulse Durations on Teeth During Ceramic Bracket Debonding. Dent. Med. Probl. 2016, 53, 352–357. [Google Scholar] [CrossRef] [Green Version]
- Bishara, S.E.; Ostby, A.W.; Laffoon, J.; Warren, J.J. Enamel cracks and ceramic bracket failure during debonding in vitro. Angle Orthod. 2008, 78, 1078–1083. [Google Scholar] [CrossRef]
- Oztoprak, M.O.; Nalbantgil, D.; Erdem, A.S.; Tozlu, M.; Arun, T. Debonding of ceramic brackets by a new scanning laser method. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 195–200. [Google Scholar] [CrossRef]
- Dostalova, T.; Jelinkova, H.; Remes, M.; Šulc, J.; Němec, M. The Use of the Er:YAG Laser for Bracket Debonding and Its Effect on Enamel Damage. Photomed. Laser Surg. 2016, 34, 394–399. [Google Scholar] [CrossRef]
- Tozlu, M.; Oztoprak, M.O.; Arun, T. Comparison of shear bond strengths of ceramic brackets after different time lags between lasing and debonding. Lasers Med. Sci. 2011, 27, 1151–1155. [Google Scholar] [CrossRef]
- Eliades, T.; Johnston, W.M.; Eliades, G. Direct light transmittance through ceramic brackets. Am. J. Orthod. Dentofac. Orthop. 1995, 107, 11–19. [Google Scholar] [CrossRef]
- Hoteit, M.; Nammour, S.; Zeinoun, T. Assessment of microcracks and shear bond strength after debonding orthodontic ceramic brackets on enamel priorly etched by different Er,Cr:YSGG and Er:YAG laser settings without acid application: An in vitro study. Int. Orthod. 2019, 17, 744–757. [Google Scholar] [CrossRef] [PubMed]
- Mundethu, A.R.; Gutknecht, N.; Franzen, R. Rapid debonding of polycrystalline ceramic orthodontic brackets with an Er:YAG laser: An in vitro study. Lasers Med. Sci. 2013, 29, 1551–1556. [Google Scholar] [CrossRef]
- Anwar Alebrahim, M.; Krafft, C.; Sekhaneh, W.; Sigusch, B.; Popp, J. ATR-FTIR and Raman spectroscopy of primary and permanent teeth. Biomed. Spectrosc. Imaging 2014, 3, 15–27. [Google Scholar] [CrossRef]
- Mohamed, J.P. Evaluating the Type of Light Transmittance in Mono Crystalline, Poly Crystalline and Sapphire Brackets—An Invitro Spectrofluorometer Study. J. Clin. Diagn. Res. 2016, 10, ZC18–ZC21. [Google Scholar] [CrossRef]
- Kwasny, M.; Polkowski, J.; Bombalska, A. A Study on the Photopolymerization Kinetics of Selected Dental Resins Using Fourier Infrared Spectroscopy (FTIR). Materials 2022, 15, 5850. [Google Scholar] [CrossRef]
- Nishikicho, K. IRPrestige-21. Available online: http://www.prophelab.com (accessed on 6 February 2023).
- Ansari, M.Y. Shear Bond Strength of Ceramic Brackets with Different Base Designs: Comparative In-vitro Study. J. Clin. Diagn. Res. 2016, 10, ZC64–ZC68. [Google Scholar] [CrossRef]
- Abe, R.; Endo, T.; Shimooka, S. Effects of tooth bleaching on shear bond strength of brackets rebonded with a self-etching adhesive system. Odontology 2011, 99, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Tocchio, R.M.; Williams, P.T.; Mayer, F.J.; Standing, K.G. Laser debonding of ceramic orthodontic brackets. Am. J. Orthod. Dentofac. Orthop. 1993, 103, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Grzech-Leśniak, K.; Matys, J.; Żmuda-Stawowiak, D.; Mroczka, K.; Dominiak, M.; Brugnera Junior, A.; Gruber, R.; Romanos, G.E.; Sculean, A. Er:YAG Laser for Metal and Ceramic Bracket Debonding: An In Vitro Study on Intrapulpal Temperature, SEM, and EDS Analysis. Photomed. Laser Surg. 2018, 36, 595–600. [Google Scholar] [CrossRef]
- Seghi, R.R.; Johnston, W.M.; O’Brien, W.J. Spectrophotometric analysis of color differences between porcelain systems. J. Prosthet. Dent. 1986, 56, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Sari, T.; Tuncel, İ.; Usumez, A.; Gutknecht, N. Transmission of Er:YAG Laser Through Different Dental Ceramics. Photomed. Laser Surg. 2014, 32, 37–41. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sample | ||||
|---|---|---|---|---|
| Group N | Aesthetic Bracket | Trade Name | Company | Sample Size |
| 1 | Monocrystalline Sapphire | Radiance | American Orthodontics, Sheboygan, WI, USA | 10 |
| 2 | Monocrystalline Sapphire | Absolute | Star Dentech, Seoul, South Korea | 10 |
| 3 | Polycrystalline | 20/40 | American Orthodontics, USA | 10 |
| 4 | Polycrystalline | Unitek Gemini Clear | 3M Unitek, Irwindale, CA, USA | 10 |
| 5 | Plastic (Silicon) | Silkon Plus | American Orthodontics, USA | 10 |
| 6 | Composite | Orthoflex | Ortho Technology, Tampa, FL, USA | 10 |
| Item | Description |
|---|---|
| Interferometer | Michelson interferometer (incident angle is 30 °C) |
| Optical system | Single beam |
| Beam splitter | Ge coated on KBr |
| Light source | Cooling-type ceramic |
| Detector | DLATGS detector with temperature control |
| Wavenumber range | 7500–400 cm−1 (±0.125 cm−1 accuracy) |
| Resolution | 0.5 cm−1, 1 cm−1, 2 cm−1, 4 cm−1, 8 cm−1, 16 cm−1 (Mid/Far IR); 2 cm−1, 4 cm−1, 8 cm−1, 16 cm−1 (NIR) |
| S/N ratio | 40,000:1 |
| Mirror speed | 2.8 mm/s, 5 mm/s, 9 mm/s, scanning at 4 cm−1 takes 2–3 s |
| Data sampling | He–Ne laser |
| Gain control | Automatic or manual (×1 to ×128) |
| Sample compartment | 200 (w) × 230 (L) × 170 (H) mm, center focus |
| Dimensions | 620 (w) × 680 (L) × 290 (H) mm |
| Weight | 54 kg |
| Studied Variable = Transmission Ratio | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Wavelength | Type of Bracket | N | Mean | Std. Deviation | Minimum | Maximum | F Value | p-Value | Significant Diff.? |
| 2940 nm | Radiance | 10 | 64.75 | 0.40 | 64.05 | 65.27 | 5562.186 | 0.000 | YES |
| Absolute | 10 | 56.16 | 0.55 | 55.54 | 56.72 | ||||
| 20/40 | 10 | 52.17 | 0.14 | 51.99 | 52.34 | ||||
| 3M | 10 | 40.48 | 0.31 | 39.97 | 40.82 | ||||
| Silkon Plus | 10 | 50.71 | 0.25 | 50.40 | 51.04 | ||||
| Composite Ortho Flex | 10 | 42.82 | 0.46 | 42.21 | 43.51 | ||||
| Studied Variable = Transmission Ratio | ||||||
|---|---|---|---|---|---|---|
| Wavelength | Type of Bracket (I) | Type of Bracket (J) | Mean Difference (I–J) | Std. Error | p-Value | Significant Diff.? |
| 2940 nm | Radiance | Absolute | 8.59 | 0.17 | 0.000 | YES |
| 20/40 | 12.58 | 0.17 | 0.000 | YES | ||
| 3M | 24.26 | 0.17 | 0.000 | YES | ||
| Silkon Plus | 14.04 | 0.17 | 0.000 | YES | ||
| Composite Ortho Flex | 21.93 | 0.17 | 0.000 | YES | ||
| Absolute | 20/40 | 3.99 | 0.17 | 0.000 | YES | |
| 3M | 15.68 | 0.17 | 0.000 | YES | ||
| Silkon Plus | 5.45 | 0.17 | 0.000 | YES | ||
| Composite Ortho Flex | 13.34 | 0.17 | 0.000 | YES | ||
| 20/40 | 3M | 11.68 | 0.17 | 0.000 | YES | |
| Silkon Plus | 1.46 | 0.17 | 0.000 | YES | ||
| Composite Ortho Flex | 9.35 | 0.17 | 0.000 | YES | ||
| 3M | Silkon Plus | −10.23 | 0.17 | 0.000 | YES | |
| Composite Ortho Flex | −2.33 | 0.17 | 0.000 | YES | ||
| Silkon Plus | Composite Ortho Flex | 7.89 | 0.17 | 0.000 | YES | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zamzam, M.K.; Hamadah, O.; Espana-Tost, T.; Arnabat-Dominguez, J. Comparative Study of Transmission of 2940 nm Wavelength in Six Different Aesthetic Orthodontic Brackets. Dent. J. 2023, 11, 67. https://doi.org/10.3390/dj11030067
Zamzam MK, Hamadah O, Espana-Tost T, Arnabat-Dominguez J. Comparative Study of Transmission of 2940 nm Wavelength in Six Different Aesthetic Orthodontic Brackets. Dentistry Journal. 2023; 11(3):67. https://doi.org/10.3390/dj11030067
Chicago/Turabian StyleZamzam, Mohammad Khare, Omar Hamadah, Toni Espana-Tost, and Josep Arnabat-Dominguez. 2023. "Comparative Study of Transmission of 2940 nm Wavelength in Six Different Aesthetic Orthodontic Brackets" Dentistry Journal 11, no. 3: 67. https://doi.org/10.3390/dj11030067