
Optimal Timing of Coronary Artery Bypass Grafting in Haemodynamically Stable Patients after Myocardial Infarction
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Statement
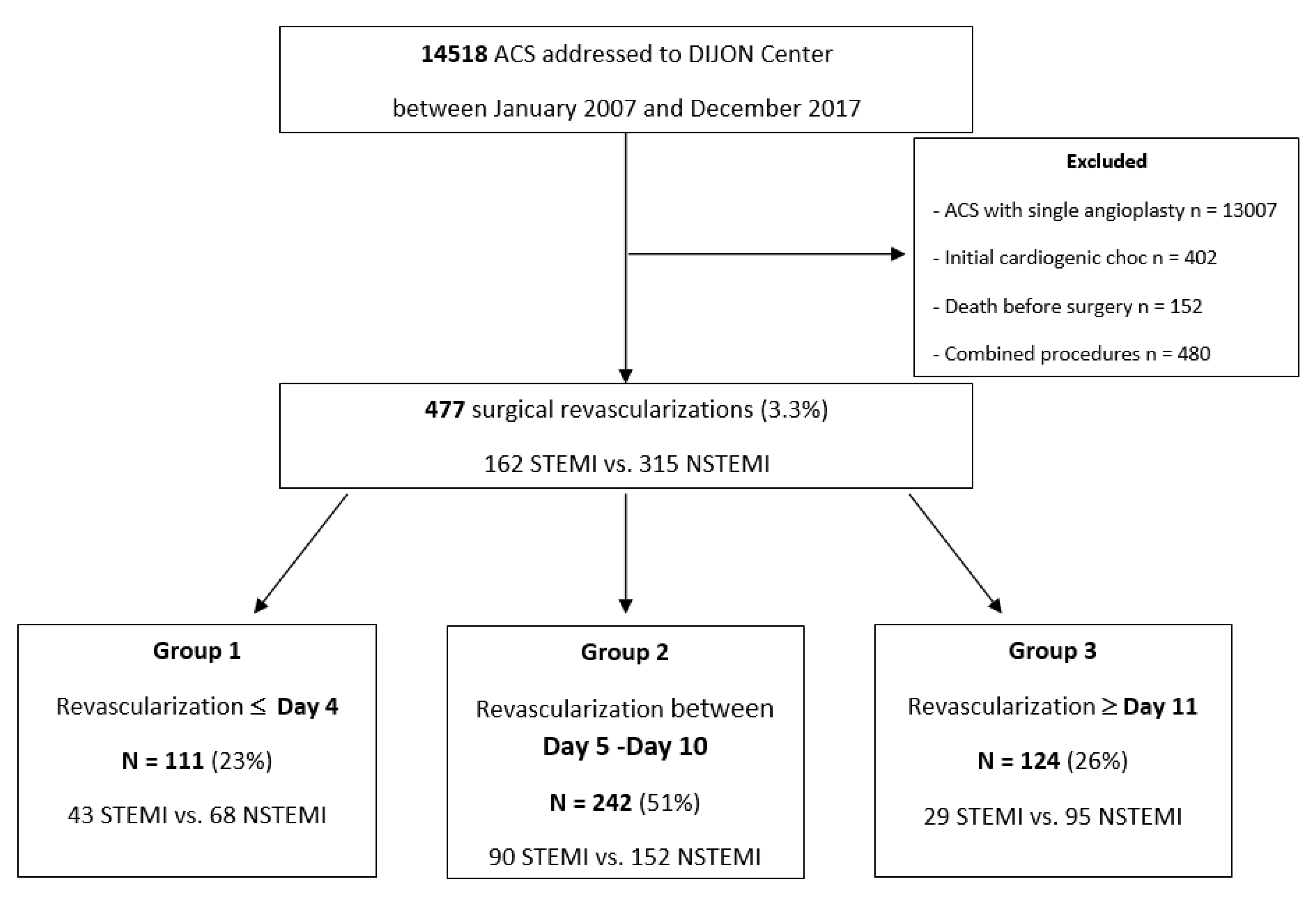
2.2. Study Population
2.3. Inclusion and Exclusion Criteria
2.4. Data Collection
2.5. Endpoint Definitions
2.6. Statistics
3. Results
3.1. Study Population
3.1.1. Preoperative State
3.1.2. Intraoperative Data
3.2. Mortality
3.3. In-Hospital Outcomes and Poor Prognosis Factors
3.3.1. Risk Factors
3.3.2. Postoperative Outcomes
3.4. Follow-Up
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Caceres, M.; Weiman, D.S. Optimal timing of coronary artery bypass grafting in acute myocardial infarction. Ann. Thorac. Surg. 2013, 95, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-L.; Liu, K. Timing of coronary artery bypass graft surgery for acute myocardial infarction patients: A meta-analysis. Int. J.Cardiol. 2014, 177, 53–56. [Google Scholar] [CrossRef] [PubMed]
- Weiss, E.S.; Chang, D.D.; Joyce, D.L.; Nwakanma, L.U.; Yuh, D.D. Optimal timing of coronary artery bypass after acute myocardial infarction: A review of California discharge data. J. Thorac. Cardiovasc. Surg. 2008, 135, 503–511.e3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biancari, F.; Onorati, F.; Rubino, A.S.; Mosorin, M.A.; Juvonen, T.; Ahmed, N.; Faggian, G.; Mariani, C.; Mignosa, C.; Cottini, M.; et al. Outcome of emergency coronary artery bypass grafting. J. Cardiothorac. Vasc. Anesth. 2015, 29, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.V.; de Lemos, J.A.; Jessen, M.E.; Brilakis, E.S.; Ohman, E.M.; Chen, A.Y.; Wang, T.Y.; Peterson, E.D.; Roe, M.T.; Hopler, E.M.; et al. Timing of in-hospital coronary artery bypass graft surgery for non-ST-segment elevation myocardial infarction patients results from the National Cardiovascular Data Registry ACTION Registry-GWTG. JACC Cardiovasc. Interv. 2010, 3, 419–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grothusen, C.; Friedrich, C.; Loehr, J.; Meinert, J.; Ohnewald, E.; Ulbricht, U.; Attmann, T.; Haneya, A.; Huenges, K.; Freitag-Wolf, S.; et al. Outcome of Stable Patients With Acute Myocardial Infarction and Coronary Artery Bypass Surgery Within 48 Hours: A Single-Center, Retrospective Experience. J. Am. Heart Assoc. 2017, 6, e005498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez, E.C.; Emmert, M.Y.; Thomas, G.N.; Emmert, L.S.; Lee, C.N.; Kofidis, T. Off-pump coronary artery bypass is a safe option in patients presenting as emergency. Ann. Acad. Med. Singap. 2010, 39, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Shroyer, A.L.; Grover, F.L.; Hattler, B.; Collins, J.F.; McDonald, G.O.; Kozora, E.; Lucke, J.C.; Baltz, J.H.; Novitzky, D.; Veterans Affairs Randomized On/Off Bypass (ROOBY) Study Group. On-pump versus off-pump coronary-artery bypass surgery. N. Engl. J. Med. 2009, 361, 1827–1837. [Google Scholar] [CrossRef] [PubMed]
- Klempfner, R.; Barac, Y.D.; Younis, A.; Kopel, E.; Younis, A.; Ronen, G.; Maor, E.; Arbel, Y.; Rott, D.; Goldenberg, I.; et al. Early Referral to Coronary Artery Bypass Grafting Following Acute Coronary Syndrome, Trends and Outcomes from the Acute Coronary Syndrome Israeli Survey (ACSIS) 2000–2010. Heart Lung Circ. 2018, 27, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. ESC/EACTS Guidelines on Myocardial Revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davierwala, P.M.; Verevkin, A.; Leontyev, S.; Misfeld, M.; Borger, M.A.; Mohr, F.W. Does Timing of Coronary Artery Bypass Surgery Affect Early and Long-Term Outcomes in Patients With Non-ST-Segment-Elevation Myocardial Infarction? Circulation 2015, 132, 731–740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assmann, A.; Boeken, U.; Akhyari, P.; Lichtenberg, A. Appropriate timing of coronary artery bypass grafting after acute myocardial infarction. Thorac. Cardiovasc. Surg. 2012, 60, 446–451. [Google Scholar] [CrossRef] [PubMed]
- Maganti, M.; Brister, S.J.; Yau, T.M.; Collins, S.; Badiwala, M.; Rao, V. Changing trends in emergency coronary bypass surgery. J. Thorac. Cardiovasc. Surg. 2011, 142, 816–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ebrahimi, R.; Dyke, C.; Mehran, R.; Manoukian, S.V.; Feit, F.; Cox, D.A.; Gersh, B.J.; Ohman, E.M.; White, H.D.; Moses, J.W.; et al. Outcomes following pre-operative clopidogrel administration in patients with acute coronary syndromes undergoing coronary artery bypass surgery: The ACUITY (Acute Catheterization and Urgent Intervention Triage strategY) trial. J. Am. Coll. Cardiol. 2009, 53, 1965–1972. [Google Scholar] [CrossRef] [Green Version]
- Grieshaber, P.; Roth, P.; Oster, L.; Schneider, T.M.; Görlach, G.; Nieman, B.; Böning, A. Is delayed surgical revascularization in acute myocardial infarction useful or dangerous? New insights into an old problem. Interact. Cardiovasc. Thorac. Surg. 2017, 25, 772–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thiele, R.H.; Hucklenbruch, C.; Ma, J.Z.; Colquhoun, D.; Zuo, Z.; Nemergut, E.C.; Raphael, J. Admission hyperglycemia is associated with poor outcome after emergent coronary bypass grafting surgery. J. Crit. Care 2015, 30, 1210–1216. [Google Scholar] [CrossRef] [PubMed]
- Sarembock, I.J.; Kereiakes, D.J. Risk stratification and timing of revascularization: Which patients benefit from early versus later revascularization? Curr. Cardiol. Rep. 2012, 14, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Harling, L.; Moscarelli, M.; Kidher, E.; Fattouch, K.; Ashrafian, H.; Athanasiou, T. The effect of off-pump coronary artery bypass on mortality after acute coronary syndrome: A meta-analysis. Int. J. Cardiol. 2013, 169, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Fattouch, K.; Guccione, F.; Dioguardi, P.; Sampognaro, R.; Corrado, E.; Caruso, M.; Ruvolo, G. Off-pump versus on-pump myocardial revascularization in patients with ST-segment elevation myocardial infarction: A randomized trial. J. Thorac. Cardiovasc. Surg. 2009, 137, 650–656. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variables | Group 1 n = 111 | Group 2 n = 242 | Group 3 n = 124 | p-Value |
|---|---|---|---|---|
| Age (years) | 65 ± 12 | 67 ± 12 | 67 ± 12 | 0.053 |
| Female sex, n (%) | 29 (26) | 53 (22) | 29 (23) | 0.57 |
| Comorbid disease | ||||
| Body mass index >30, n (%) | 25 (22) | 50 (21) | 28 (22) | 0.80 |
| Systemic hypertension, n (%) | 76 (68) | 162 (67) | 86 (69) | 0.89 |
| Hyperlipidaemia, n (%) | 80 (72) | 146 (60) | 88 (71) | 0.02 |
| Diabetes, n (%) | 27 (24) | 57 (23) | 41 (33) | 0.13 |
| Smoking, n (%) | 61 (55) | 137 (57) | 198 (56) | 0.74 |
| Peripheral vascular disease, n (%) | 12 (11) | 20 (8) | 11 (9) | 0.50 |
| Heredity, n (%) | 31 (28) | 68 (28) | 99 (28) | 0.93 |
| Renal failure, n (%) | 5 (4) | 20 (8) | 8 (6) | 0.42 |
| Mean maximal troponin level (ng/mL) | 24.8 ± 54 | 22.9 ± 55 | 24.6 ± 53 | 0.32 |
| Mean lactate level (mmol/L) | 1.8 ± 1.8 | 1.5 ± 1.9 | 1.9 ± 2.2 | 0.54 |
| Coronary history, n (%) | 18 (16) | 36 (15) | 27 (22) | 0.29 |
| LVEF (%) | 52.8 ± 11.8 | 52.9 ± 11.3 | 54.8 ± 11.2 | 0.3 |
| EuroSCORE II (%) | 3.25 ± 1.8 | 3.0 ± 1.8 | 3.1 ± 2.7 | 0.8 |
| STEMI, n (%) | 43 (39) | 90 (37) | 29 (23) | 0.015 |
| Left main disease, n (%) | 52 (47) | 123 (51) | 55 (44) | 0.48 |
| Number of diseased coronary arteries | ||||
| One, n (%) | 3 (3) | 5 (2) | 3 (2) | 0.47 |
| Two, n (%) | 24 (21) | 58 (24) | 23 (19) | 0.52 |
| Three, n (%) | 84 (76) | 179 (74) | 98 (79) | 0.38 |
| Ischemic recurrence, n (%) | 25 (22) | 37 (15) | 30 (24) | 0.20 |
| Variable | Group 1 n = 111 | Group 2 n = 242 | Group 3 n = 124 | p-Value |
|---|---|---|---|---|
| Angioplasty failure, n (%) | 17 (15) | 10 (4) | 14 (11) | <0.01 |
| Overall antiplatelet use, n (%) | 104 (94) | 207 (85) | 116 (93) | 0.01 |
| Aspirin, n (%) | 99 (89) | 205 (85) | 116 (94) | 0.01 |
| Plavix, n (%) | 55 (50) | 103 (43) | 47 (38) | 0.15 |
| Other antiplatelet agent, n (%) | 23 (21) | 49 (20) | 18 (15) | 0.35 |
| VKA, n (%) | 3 (3) | 6 (2) | 2 (2) | 0.85 |
| Fibrinolysis, n (%) | 12 (11) | 26 (11) | 10 (8) | 0.69 |
| Events | Group 1 n = 111 | Group 2 n = 242 | Group 3 n = 124 | p-Value |
|---|---|---|---|---|
| None, n (%) | 86 (77) | 206 (85) | 94 (76) | 0.13 |
| Ischemic recurrency, n (%) | 18 (16) | 28 (12) | 25 (20) | 0.13 |
| Cardiorespiratory arrest, n (%) | 0 (0) | 3 (1) | 1 (0.8) | |
| IABP, n (%) | 53 (48) | 42 (17) | 6 (5) | <0.001 |
| Cardiogenic shock, n (%) | 2 (2) | 1 (0.4) | 1 (1) | |
| Intra-aortic balloon pump after ischemic recurrence, n (%) | 16 (14) | 16 (6) | 2 (2) | <0.001 |
| Outcomes | Group 1 n = 111 | Group 2 n = 242 | Group 3 n = 124 | Total | p-Value |
|---|---|---|---|---|---|
| Thirty-day mortality, n (%) | 16 (14) | 10 (4) | 8 (6) | 34 (7) | <0.01 |
| Causes of death | |||||
| Multiorgan failure, n (%) | 3 | 1 | 5 | 9 | 0.023 |
| Cardiorespiratory arrest or cardiogenic shock, n (%) | 7 | 2 | 2 | 11 | <0.01 |
| Stroke, n (%) | 0 | 1 | 0 | 1 | 1 |
| Mesenteric ischemia, n (%) | 0 | 2 | 0 | 2 | 0.74 |
| Others, n (%) | 6 | 4 | 1 | 11 | 0.054 |
| Variables | Odds Ratio | 95% Confidence Interval | p > |z| |
|---|---|---|---|
| Age | 1.08 | (1.04; 1.12) | <0.001 |
| Renal failure, n (%) | 6.39 | (2.49; 15.6) | <0.001 |
| Peripheral vascular disease, n (%) | 3.31 | (1.16; 9.43) | 0.024 |
| LVEF (%) | 0.975 | (0.945; 1.01) | 0.12 |
| STEMI, n (%) | 0.701 | (0.306; 1.50) | 0.38 |
| Left main disease, n (%) | 1.02 | (0.495; 2.07) | 0.96 |
| Aspirin, n (%) | 0.637 | (0.260; 1.81) | 0.35 |
| Angioplasty failure, n (%) | 0.227 | (0.0968; 0.507) | <0.001 |
| Preoperative intra-aortic balloon pump, n (%) | 3.26 | (1.55; 6.74) | <0.01 |
| Ischemic recurrence, n (%) | 3.47 | (1.59; 7.48) | <0.01 |
| Revascularization timing | 3.69 | (1.77; 7.57) | <0.001 |
| Postoperative bleeding | 0.276 | (0.116; 0.630) | <0.01 |
| Postoperative Outcomes | Group 1 n = 111 | Group 2 n = 242 | Group 3 n = 124 | Total | p-Value |
|---|---|---|---|---|---|
| Redo for bleeding, n (%) | 6 (5.4) | 9 (3.7) | 3 (2.4) | 18 (3.7) | 0.54 |
| Early ischemic recurrence <D3, n (%) | 0 (0) | 3 (1.2) | 3 (2.4) | 6 (1.2) | 0.6 |
| Delayed ischemic recurrence, n (%) | 8 (7) | 11 (4.5) | 7 (5.6) | 26 (5.2) | 0.59 |
| Cardiac failure, n (%) | 3 (2.7) | 6 (2.5) | 2 (1.6) | 11 (2.3) | 0.85 |
| Stroke, n (%) | 3 (2.7) | 4 (1.6) | 0 (0) | 7 (1.4) | 0.52 |
| Cardiorespiratory arrest or cardiogenic shock, n (%) | 5 (4.5) | 7 (2.8) | 3 (2.4) | 15 (3.1) | 0.62 |
| Acute pulmonary oedema, n (%) | 2 (1.8) | 0 (0) | 0 (0) | 2 (0.4) | 0.054 |
| Wound surgery for infection, n (%) | 4 (3.6) | 10 (4.1) | 4 (3.2) | 18 (3.7) | 0.92 |
| Septic shock, n (%) | 4 (3.6) | 0 (0) | 0 (0) | 4 (0.8) | 0.042 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernard, C.; Morgant, M.C.; Jazayeri, A.; Perrin, T.; Malapert, G.; Jazayeri, S.; Bernard, A.; Bouchot, O. Optimal Timing of Coronary Artery Bypass Grafting in Haemodynamically Stable Patients after Myocardial Infarction. Biomedicines 2023, 11, 979. https://doi.org/10.3390/biomedicines11030979
Bernard C, Morgant MC, Jazayeri A, Perrin T, Malapert G, Jazayeri S, Bernard A, Bouchot O. Optimal Timing of Coronary Artery Bypass Grafting in Haemodynamically Stable Patients after Myocardial Infarction. Biomedicines. 2023; 11(3):979. https://doi.org/10.3390/biomedicines11030979
Chicago/Turabian StyleBernard, Chloé, Marie Catherine Morgant, Aline Jazayeri, Thomas Perrin, Ghislain Malapert, Saed Jazayeri, Alain Bernard, and Olivier Bouchot. 2023. "Optimal Timing of Coronary Artery Bypass Grafting in Haemodynamically Stable Patients after Myocardial Infarction" Biomedicines 11, no. 3: 979. https://doi.org/10.3390/biomedicines11030979