
The Role of the Left Inferior Parietal Cortex in Gilles de la Tourette Syndrome—An rTMS Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Clinical Assessment
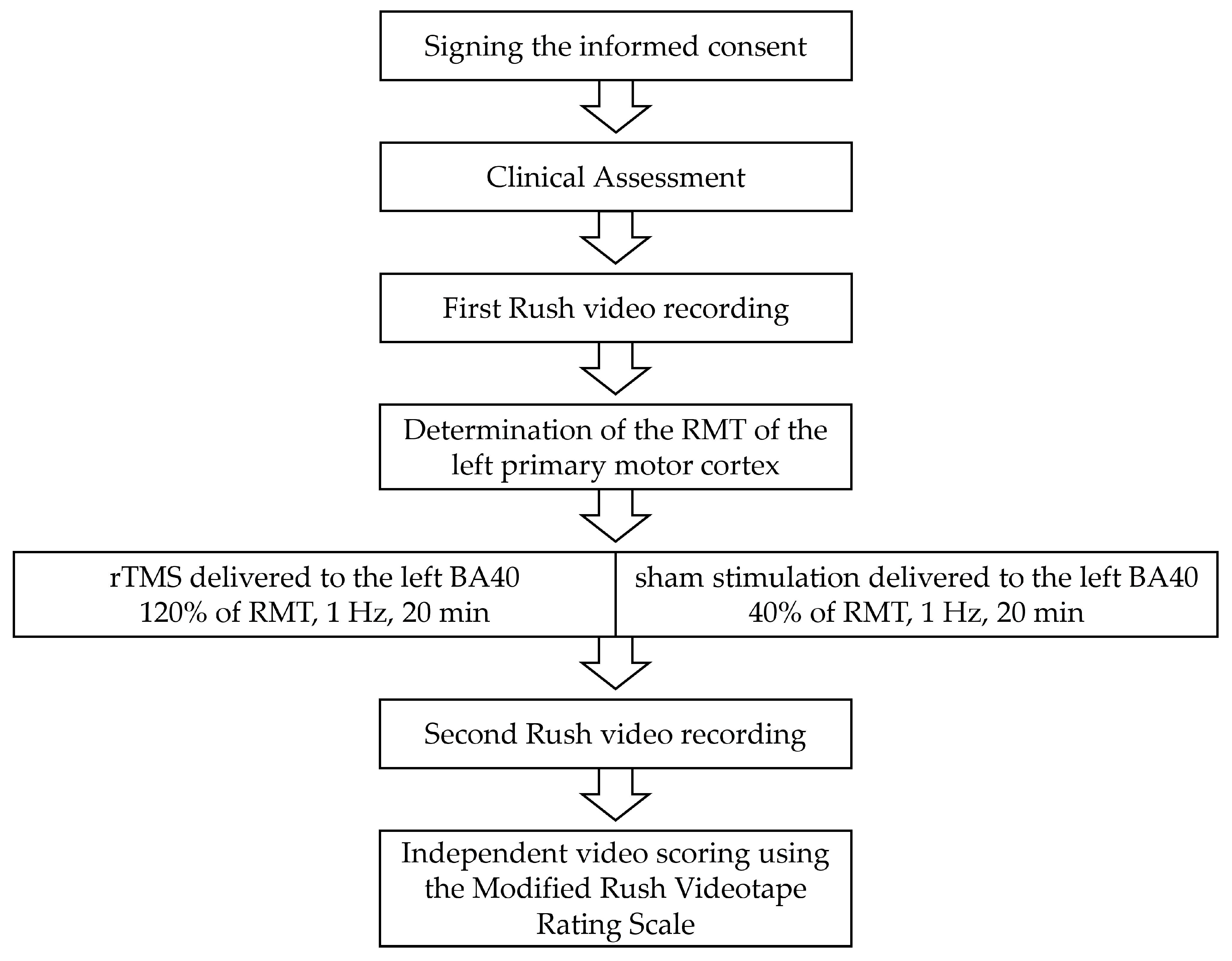
2.2. rTMS Protocol
2.3. Statistical Analysis
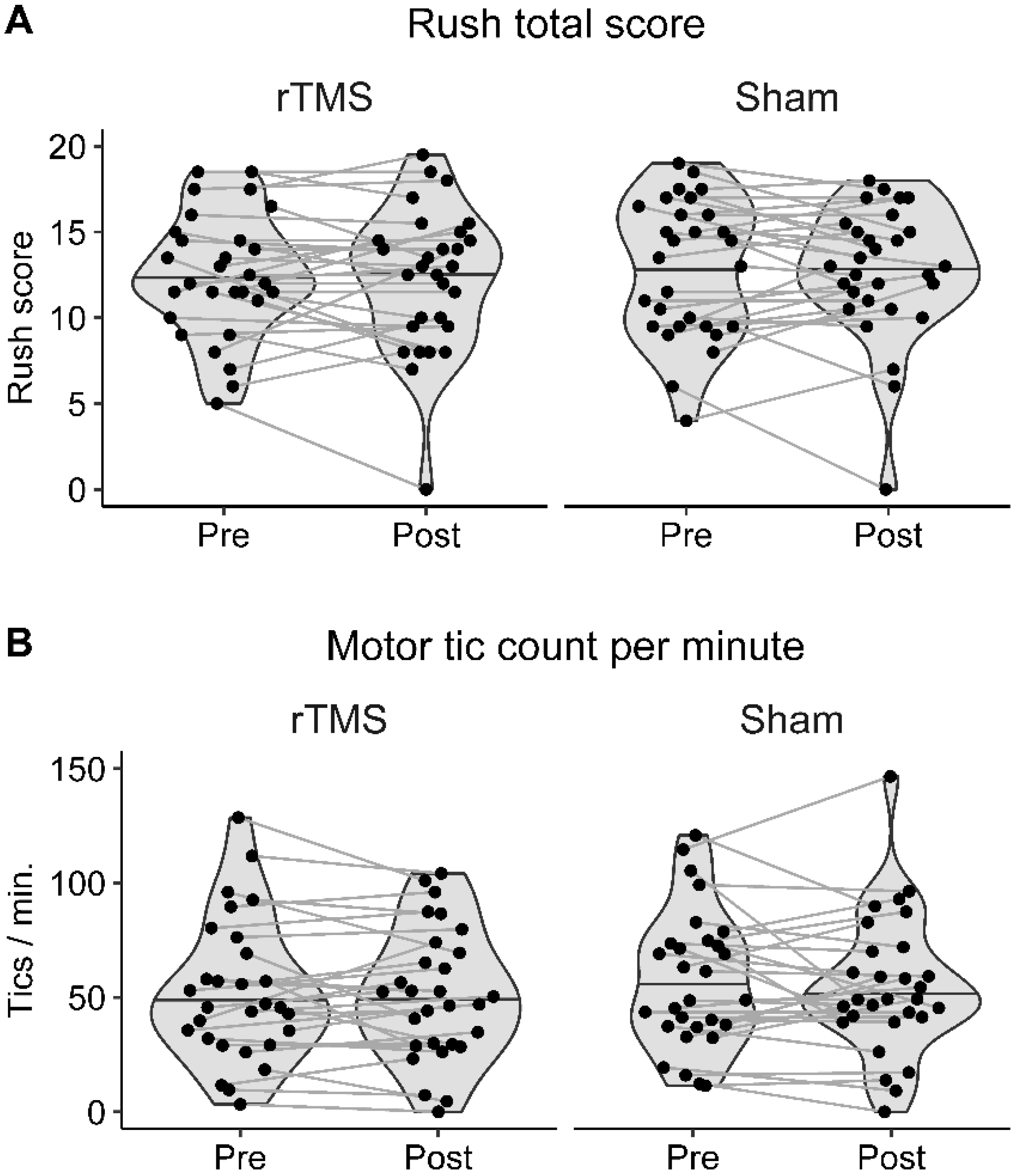
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Barker, A.T.; Jalinous, R.; Freeston, I.L. Non-invasive magnetic stimulation of human motor cortex. Lancet 1985, 1, 1106–1107. [Google Scholar] [CrossRef] [PubMed]
- Dyke, K.; Jackson, G.; Jackson, S. Non-invasive brain stimulation as therapy: Systematic review and recommendations with a focus on the treatment of Tourette syndrome. Exp. Brain Res. 2022, 240, 341–363. [Google Scholar] [CrossRef] [PubMed]
- Kleimaker, M.; Kleimaker, A.; Weissbach, A.; Colzato, L.S.; Beste, C.; Bäumer, T.; Münchau, A. Non-invasive brain stimulation for the treatment of Gilles de la Tourette Syndrome. Front. Neurol. 2020, 11, 592258. [Google Scholar] [CrossRef]
- Le, K.; Liu, L.; Sun, M.; Hu, L.; Xiao, N. Transcranial magnetic stimulation at 1 Hertz improves clinical symptoms in children with Tourette syndrome for at least 6 months. J. Clin. Neurosci. 2013, 20, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Kwon, H.J.; Lim, W.S.; Lim, M.H.; Lee, S.J.; Hyun, J.K.; Chae, J.H.; Paik, K.C. 1-Hz low frequency repetitive transcranial magnetic stimulation in children with Tourette’s syndrome. Neurosci. Lett. 2011, 492, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Lisanby, S.H.; Pieraccini, F.; Ulivelli, M.; Castrogiovanni, P.; Rossi, S. Repetitive transcranial magnetic stimulation (rTMS) in the treatment of obsessive-compulsive disorder (OCD) and Tourette’s syndrome (TS). Int. J. Neuropsychopharmacol. 2006, 9, 95–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mantovani, A.; Leckman, J.F.; Grantz, H.; King, R.A.; Sporn, A.L.; Lisanby, S.H. Repetitive Transcranial Magnetic Stimulation of the Supplementary Motor Area in the treatment of Tourette Syndrome: Report of two cases. Clin. Neurophysiol. 2007, 118, 2314–2315. [Google Scholar] [CrossRef]
- Münchau, A.; Bloem, B.R.; Thilo, K.V.; Trimble, M.R.; Rothwell, J.C.; Robertson, M.M. Repetitive transcranial magnetic stimulation for Tourette syndrome. Neurology 2002, 59, 1789–1791. [Google Scholar] [CrossRef]
- Landeros-Weisenberger, A.; Mantovani, A.; Motlagh, M.G.; de Alvarenga, P.G.; Katsovich, L.; Leckman, J.F.; Lisanby, S.H. Randomized sham controlled double-blind trial of repetitive transcranial magnetic stimulation for adults with severe Tourette syndrome. Brain Stimul. 2015, 8, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Wu, S.W.; Maloney, T.; Gilbert, D.L.; Dixon, S.G.; Horn, P.S.; Huddleston, D.A.; Eaton, K.; Vannest, J. Functional MRI-navigated repetitive transcranial magnetic stimulation over supplementary motor area in chronic tic disorders. Brain Stimul. 2014, 7, 212–218. [Google Scholar] [CrossRef]
- Orth, M.; Amann, B.; Robertson, M.M.; Rothwell, J.C. Excitability of motor cortex inhibitory circuits in Tourette syndrome before and after single dose nicotine. Brain 2005, 128, 1292–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, S.; Kumar, S.; Kumar, N.; Verma, R. Low-frequency repetitive transcranial magnetic stimulation for treatment of Tourette syndrome: A naturalistic study with 3 months of follow-up. Indian J. Psychol. Med. 2018, 40, 482–486. [Google Scholar] [CrossRef]
- Kahl, C.K.; Kirton, A.; Pringsheim, T.; Croarkin, P.E.; Zewdie, E.; Swansburg, R.; Wrightson, J.; Langevin, L.M.; Macmaster, F.P. Bilateral transcranial magnetic stimulation of the supplementary motor area in children with Tourette syndrome. Dev. Med. Child Neurol. 2021, 63, 808–815. [Google Scholar] [CrossRef] [PubMed]
- Fu, M.; Wei, H.; Meng, X.; Chen, H.; Shang, B.; Chen, F.; Huang, Z.; Sun, Y.; Wang, Y. Effects of low-frequency repetitive transcranial magnetic stimulation of the bilateral parietal cortex in patients with Tourette syndrome. Front. Neurol. 2021, 12, 602830. [Google Scholar] [CrossRef] [PubMed]
- Bohlhalter, S.; Goldfine, A.; Matteson, S.; Garraux, G.; Hanakawa, T.; Kansaku, K.; Wurzman, R.; Hallett, M. Neural correlates of tic generation in Tourette syndrome: An event-related functional MRI study. Brain 2006, 129, 2029–2037. [Google Scholar] [CrossRef] [Green Version]
- Kleimaker, M.; Takacs, A.; Conte, G.; Onken, R.; Verrel, J.; Bäumer, T.; Münchau, A.; Beste, C. Increased perception-action binding in Tourette syndrome. Brain 2020, 143, 1934–1945. [Google Scholar] [CrossRef]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I.): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. S20), 22–57. [Google Scholar]
- Goodman, W.K.; Price, L.H.; Rasmussen, S.A.; Mazure, C.; Fleischmann, R.L.; Hill, C.L.; Heninger, G.R.; Charney, D.S. The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Arch. Gen. Psychiatry 1989, 46, 1006–1011. [Google Scholar] [CrossRef]
- Christiansen, H.; Hirsch, O.; Philipsen, A.; Oades, R.D.; Matthies, S.; Hebebrand, J.; Ueckermann, J.; Abdel-Hamid, M.; Kraemer, M.; Wiltfang, J.; et al. German validation of the conners adult ADHD rating scale-self-report: Confirmation of factor structure in a large sample of participants with ADHD. J. Atten. Disord. 2013, 17, 690–698. [Google Scholar] [CrossRef]
- Donnell, A.J.; Pliskin, N.; Holdnack, J.; Axelrod, B.; Randolph, C. Rapidly-administered short forms of the Wechsler Adult Intelligence Scale-3rd edition. Arch. Clin. Neuropsychol. 2007, 22, 917–924. [Google Scholar] [CrossRef] [Green Version]
- Leckman, J.F.; Riddle, M.A.; Hardin, M.T.; Ort, S.I.; Swartz, K.L.; Stevenson, J.; Cohen, D.J. The Yale Global Tic Severity Scale: Initial testing of a clinician-rated scale of tic severity. J. Am. Acad. Child Adolesc. Psychiatry 1989, 28, 566–573. [Google Scholar] [CrossRef]
- Robertson, M.M.; Banerjee, S.; Kurlan, R.; Cohen, D.J.; Leckman, J.F.; McMahon, W.; Pauls, D.L.; Sandor, P.; van de Wetering, B.J. The Tourette syndrome diagnostic confidence index: Development and clinical associations. Neurology 1999, 53, 2108–2112. [Google Scholar] [CrossRef] [PubMed]
- Woods, D.W.; Piacentini, J.; Himle, M.B.; Chang, S. Premonitory Urge for Tics Scale (PUTS): Initial psychometric results and examination of the premonitory urge phenomenon in youths with Tic disorders. J. Dev. Behav. Pediatr. 2005, 26, 397–403. [Google Scholar] [CrossRef]
- Beste, C.; Münchau, A. Tics and Tourette syndrome—Surplus of actions rather than disorder? Mov. Disord. 2018, 33, 238–242. [Google Scholar] [CrossRef]
- Goetz, C.G.; Pappert, E.J.; Louis, E.D.; Raman, R.; Leurgans, S. Advantages of a modified scoring method for the Rush Video-Based Tic Rating Scale. Mov. Disord. 1999, 14, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Paulus, T.; Schappert, R.; Bluschke, A.; Alvarez-Fischer, D.; Naumann KE, R.; Roessner, V.; Bäumer, T.; Beste, C.; Münchau, A. Questioning the definition of Tourette syndrome-evidence from machine learning. Brain Commun. 2021, 3, fcab282. [Google Scholar] [CrossRef] [PubMed]
- Paulus, W.; Classen, J.; Cohen, L.G.; Large, C.H.; Di Lazzaro, V.; Nitsche, M.; Pascual-Leone, A.; Rosenow, F.; Rothwell, J.C.; Ziemann, U. State of the art: Pharmacologic effects on cortical excitability measures tested by transcranial magnetic stimulation. Brain Stimul. 2008, 1, 151–163. [Google Scholar] [CrossRef] [PubMed]
- Mazziotta, J.; Toga, A.; Evans, A.; Fox, P.; Lancaster, J.; Zilles, K.; Woods, R.; Paus, T.; Simpson, G.; Pike, B.; et al. A probabilistic atlas and reference system for the human brain: International Consortium for Brain Mapping (ICBM). Philos. Trans. R. Soc. Lond. B Biol. Sci. 2001, 356, 1293–1322. [Google Scholar] [CrossRef]
- Takacs, A.; Zink, N.; Wolff, N.; Münchau, A.; Mückschel, M.; Beste, C. Connecting EEG signal decomposition and response selection processes using the theory of event coding framework. Hum. Brain Mapp. 2020, 41, 2862–2877. [Google Scholar] [CrossRef]
- Lohse, A.; Meder, D.; Nielsen, S.; Lund, A.E.; Herz, D.M.; Løkkegaard, A.; Siebner, H.R. Low-frequency transcranial stimulation of pre-supplementary motor area alleviates levodopa-induced dyskinesia in Parkinson’s disease: A randomized cross-over trial. Brain Commun. 2020, 2, fcaa147. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, X.; Biurrun Manresa, J.; Zhang, L. What is a Bayes factor? Psychol. Methods 2021. [Google Scholar] [CrossRef] [PubMed]
- Dienes, Z. Using Bayes to get the most out of non-significant results. Front. Psychol. 2014, 5, 781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- JASP Team. JASP, Version 0.16.2; [Computer Software]. 2022. Available online: https://jasp-stats.org/ (accessed on 1 February 2023).
- Robertson, M.M. The prevalence and epidemiology of Gilles de la Tourette syndrome. Part 2: Tentative explanations for differing prevalence figures in GTS, including the possible effects of psychopathology, aetiology, cultural differences, and differing phenotypes. J. Psychosom. Res. 2008, 65, 473–486. [Google Scholar] [CrossRef] [PubMed]
- Hoogendam, J.M.; Ramakers, G.M.; Di Lazzaro, V. Physiology of repetitive transcranial magnetic stimulation of the human brain. Brain Stimul. 2010, 3, 95–118. [Google Scholar] [CrossRef]
- Chae, J.H.; Nahas, Z.; Wassermann, E.; Li, X.; Sethuraman, G.; Gilbert, D.; Sallee, F.R.; George, M.S. A pilot safety study of repetitive transcranial magnetic stimulation (rTMS) in Tourette’s syndrome. Cogn. Behav. Neurol. 2004, 17, 109–117. [Google Scholar] [CrossRef]
- Ganos, C.; Münchau, A.; Bhatia, K.P. The semiology of tics, Tourette’s, and their associations. Mov. Disord. Clin. Pract. 2014, 1, 145–153. [Google Scholar] [CrossRef]
- Conde, V.; Tomasevic, L.; Akopian, I.; Stanek, K.; Saturnino, G.B.; Thielscher, A.; Bergmann, T.O.; Siebner, H.R. The non-transcranial TMS-evoked potential is an inherent source of ambiguity in TMS-EEG studies. NeuroImage 2019, 185, 300–312. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Subject | Age | Sex 1 | IQ | Disease Duration (Years) | DCI 2 (0–100) | YGTSS 3 Total 120/40% RMT 4 (0–100) | PUTS 5 120/40% RMT 4 (10–40) | YBOCS 6 (0–40) | ADHD 7 T-Score | |
|---|---|---|---|---|---|---|---|---|---|---|
| IA 8 | HI 9 | |||||||||
| 1 | 23 | M | 104 | 16 | 54 | n.a./58 | n.a./21 | 0 | 50 | 49 |
| 2 | 21 | M | 106 | 7 | 39 | 54/40 | 20/18 | 0 | 47 | 35 |
| 3 | 25 | M | 119 | 9 | 42 | 38/29 | 20/22 | 11 | 50 | 45 |
| 4 | 46 | M | 111 | 41 | 76 | 25/12 | 14/14 | 7 | 51 | 45 |
| 5 | 25 | M | 112 | 19 | 46 | 15/18 | 9/9 | 0 | 33 | 47 |
| 6 | 44 | M | 115 | 39 | 100 | 60/44 | 24/26 | 25 | 79 | 70 |
| 7 | 28 | F | 111 | 14 | 36 | 53/58 | 22/23 | 0 | 55 | 38 |
| 8 | 47 | F | 123 | 41 | 48 | 52/29 | 20/19 | 25 | 79 | 88 |
| 9 | 27 | M | 102 | 11 | 70 | 41/36 | 26/23 | 20 | 54 | 54 |
| 10 | 20 | F | 117 | 16 | 78 | 39/47 | 30/30 | 4 | 43 | 43 |
| 11 | 28 | M | 104 | 22 | 78 | 60/45 | 20/19 | 10 | 36 | 42 |
| 12 | 39 | M | 121 | 33 | 76 | 30/53 | 20/23 | 36 | 56 | 56 |
| 13 | 19 | M | 94 | 16 | 58 | 61/59 | 16/19 | 17 | 69 | 38 |
| 14 | 32 | M | 117 | 24 | 59 | 50/47 | 25/21 | 14 | 42 | 71 |
| 15 | 20 | F | 102 | 12 | 44 | 29/38 | 23/23 | 21 | 55 | 38 |
| 16 | 24 | F | 96 | 20 | 72 | 52/44 | 18/19 | 14 | 43 | 43 |
| 17 | 26 | F | 115 | 21 | 53 | 60/67 | 30/28 | 20 | 60 | 56 |
| 18 | 20 | F | 112 | 13 | 58 | 27/48 | 23/22 | 17 | 53 | 46 |
| 19 | 46 | M | 121 | 35 | 100 | 36/39 | 19/14 | 12 | 54 | 55 |
| 20 | 50 | M | 89 | 37 | 36 | 51/28 | 29/26 | 11 | 58 | 62 |
| 21 | 28 | F | 123 | 25 | 67 | 48/40 | 14/17 | 8 | 60 | 46 |
| 22 | 49 | M | 110 | 43 | 27 | 50/53 | 16/15 | 0 | 42 | 40 |
| 23 | 25 | F | 102 | 23 | 47 | 31/55 | 19/15 | 0 | 48 | 46 |
| 24 | 18 | M | 110 | 11 | 35 | 18/21 | 16/21 | 10 | 57 | 58 |
| 25 | 30 | F | 112 | 24 | 58 | 75/85 | 23/24 | 23 | 53 | 59 |
| 26 | 27 | M | 89 | 20 | 91 | 24/20 | 24/14 | 10 | 36 | 49 |
| 27 | 33 | F | 119 | 27 | 74 | 47/57 | 27/23 | 15 | 46 | 45 |
| 28 | 28 | F | 108 | 23 | 80 | 51/50 | 20/18 | 24 | 88 | 88 |
| 29 | 30 | F | 110 | 25 | 98 | 66/63 | 32/30 | 19 | >90 | >90 |
| Mean | 30.3 | - | 109.4 | 23 | 62.1 | 44.4/44.2 | 21.4/20.6 | 12.9 | 54.8 | 53.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paulus, T.; Wernecke, L.; Lundie, A.; Friedrich, J.; Verrel, J.; Rawish, T.; Weissbach, A.; Frings, C.; Beste, C.; Bäumer, T.; et al. The Role of the Left Inferior Parietal Cortex in Gilles de la Tourette Syndrome—An rTMS Study. Biomedicines 2023, 11, 980. https://doi.org/10.3390/biomedicines11030980
Paulus T, Wernecke L, Lundie A, Friedrich J, Verrel J, Rawish T, Weissbach A, Frings C, Beste C, Bäumer T, et al. The Role of the Left Inferior Parietal Cortex in Gilles de la Tourette Syndrome—An rTMS Study. Biomedicines. 2023; 11(3):980. https://doi.org/10.3390/biomedicines11030980
Chicago/Turabian StylePaulus, Theresa, Lynn Wernecke, Annik Lundie, Julia Friedrich, Julius Verrel, Tina Rawish, Anne Weissbach, Christian Frings, Christian Beste, Tobias Bäumer, and et al. 2023. "The Role of the Left Inferior Parietal Cortex in Gilles de la Tourette Syndrome—An rTMS Study" Biomedicines 11, no. 3: 980. https://doi.org/10.3390/biomedicines11030980