1. Introduction
Healthcare workers (HCWs) are at high risk of contracting Coronavirus disease 2019 (COVID-19) due to occupational exposure to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [
1]. In the first quarter of 2021, the Japanese government launched a mass COVID-19 vaccination campaign using the BNT162b2 (Comirnaty, Pfizer-BioNTech, NY, USA) vaccine. The mRNA-1273 (Spikevax, Moderna, Cambridge, MA, USA) and ChAdOx1-S (Vaxzevria AstraZeneca, Cambridge, UK) vaccines were added subsequently [
2].
BNT162b2 is an mRNA vaccine encoding a full-length spike protein of SARS-CoV-2 (SARS-CoV-2 S) [
3]. Its efficacy against severe COVID-19 was reported to be >90%; however, it has been found that the efficacy peaks within two months after the administration of a second dose and then declines [
4]. Despite its high efficacy, breakthrough infections have been reported among HCWs who received two or more doses of the BNT162b2 vaccine [
5], thereby making it necessary to administer booster doses to sustain protection. Individuals who experienced acute allergic-like reactions (AALR) to vaccines are often hesitant to receive further doses, and healthcare providers are cautious about vaccinating such individuals.
This study compared the immune response to the second vaccination in four HCWs who received the first two doses six months apart (due to acute allergic-like adverse events after the first dose), with that of six HCWs who received the first two doses three weeks apart according to the standard schedule.
2. Materials and Methods
Before introducing the BNT162b2 vaccine, HCWs at the Gunma Prefectural Cancer Center (GPCC) in Ota City, Gunma, Japan, were invited to participate in a prospective cohort study to monitor their immunological status against SARS-CoV-2. Six HCWs enrolled in the study. They subsequently received three doses of the BNT162b2 vaccine. The first two doses were administered three weeks apart and a third dose was administered six months after the second dose.
An additional four HCWs who had experienced AALR after receiving the first dose of the vaccine subsequently joined the study prior to receiving the second dose. AALR was defined according to the World Allergy Organization criteria [
6]. The clinical criteria for diagnosing AALR were illness with involvement of skin, mucosal tissue, respiratory compromise, change in blood pressure, associated symptoms of end-organ dysfunction, or persistent gastrointestinal symptoms. These four participants were administered a second dose of vaccine six months after the first dose, with 50 mg oral diphenhydramine administered 30 min before vaccination to prevent AALR [
7].
Serum was collected from the study participants at four distinct time points: (1) at the time of enrollment, (2) every 3 months after enrollment, (3) a week before, and (4) 2–3 weeks after each vaccination. The serum samples were stored at −35 °C and tested for SARS-CoV-2 anti-spike (S) IgG using a commercial chemiluminescence enzyme immunoassay (SARS-CoV-2 S-IgG reagents, Fujirebio, Tokyo, Japan). This test had a specificity of 100 and a 98.7% concordance with the Abbott SARS-CoV-2 S-IgG assay (Abbott Japan LLC, Tokyo, Japan) [
8]. If COVID-19 infection was suspected during the study period, participants were tested for SARS-CoV-2 via nasopharyngeal swab samples using a polymerase chain reaction test (ID NOW COVID-19, Abbott Japan LLC) [
8]. We did not evaluate cellular immunogenicity and cytokines other than SARS-CoV-2 anti-spike immunoglobulin G in this study.
This study was registered in the University Hospital Medical Information Network Center Clinical Trials Registry (UMIN000040679) and was approved by the GPCC Institutional Review Board (IRB# 405-03030). The study was conducted according to the guidelines of the Declaration of Helsinki. Written informed consent was obtained from all the participants prior to the commencement of the study.
Geometric mean titer (GMT) and geometric mean fold rise (GMFR) after the second dose of vaccine were the primary outcomes. Statistical analysis was performed using EZR software (EZR) [
9]. Mann-Whitney U test was used to assess the statistical significance of differences in the mean and median antibody titers, according to the group. Two-sided
p values < 0.05 were considered statistically significant.
3. Results
The characteristics of the four HCWs who experienced AALR to the first dose of the vaccine are presented in
Table 1. These four participants experienced grade 1 adverse events (AEs) according to the World Allergy Organization Anaphylaxis Guidance 2020 [
6].
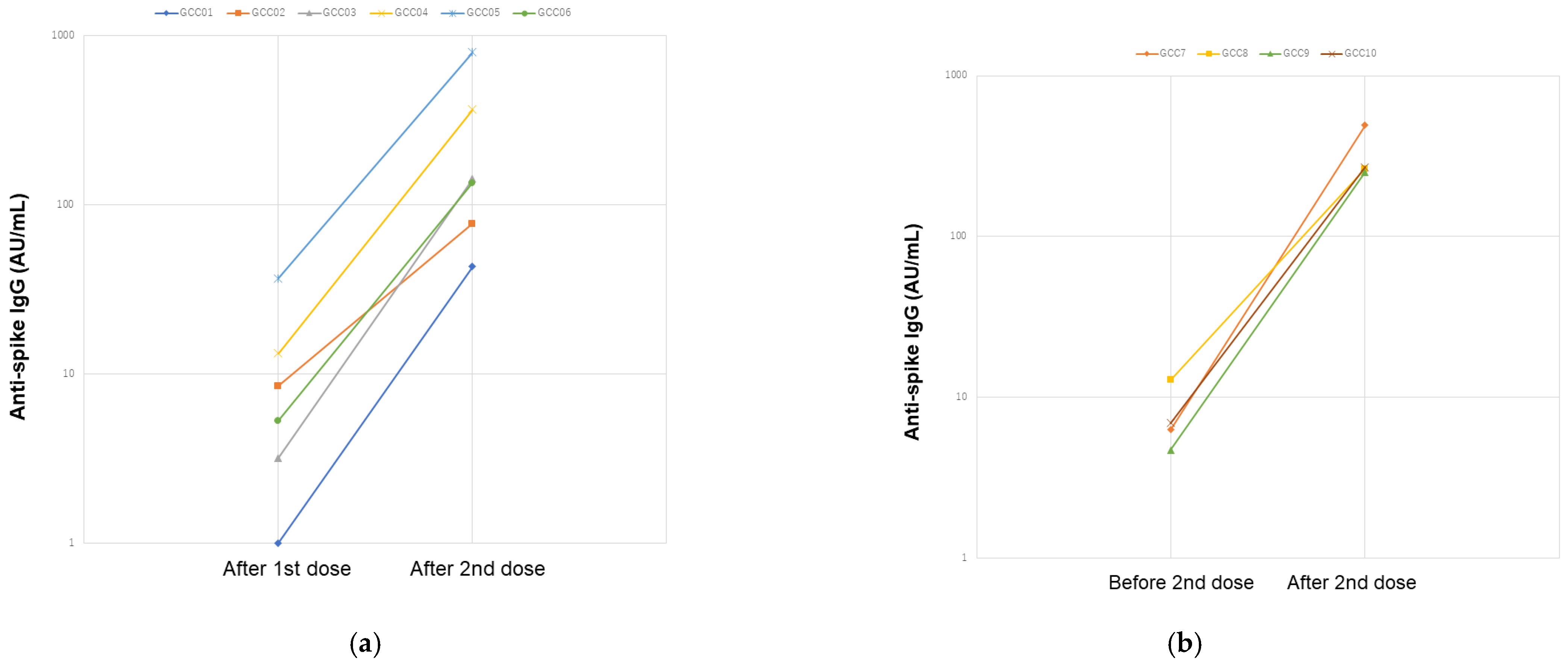
None of the initial six participants showed detectable levels of anti-S-IgG antibodies before the administration of the first dose of the vaccine (
Supplemental Table S1). Changes in anti-S-IgG titers after the administration of the second dose are shown in
Table 2 and
Table 3 and
Figure 1. In individuals who received the second dose of the vaccine three weeks and six months after the first dose, GMT values recorded 1–3 weeks after the administration of the second dose were 7.22 arbitrary units (AU) and 8.26 AU, respectively. Similarly, the GMFR values were 2.89 log and 2.91 log, respectively, relative to the titer 1–2 weeks before the administration of the second dose (
Table 2). The median anti-S-IgG titer of the four additional participants was similar to that of the initial six participants before and after the second dose of vaccination (
p > 0.999 and
p = 0.325, respectively,
Table 3). These data might indicate that the second dose vaccination had a similar boosting effect in the initial six and additional four participants.
None of the four participants who had AALR after the first dose experienced any acute or delayed allergic-like reaction after the administration of a second dose. None of the participants were diagnosed with SARS-CoV-2-infection during the study period.
4. Discussion
This study found two important implications regarding BNT162b2 immunogenicity. First, the second vaccine dose administered six months after the first dose had a boosting effect on anti-S-IgG titers similar to that of a second dose administered three weeks after the first dose. This can be explained by the fact that a similar immune response was obtained in both groups, which could be due to booster vaccines and repetitive immunogenic stimulations providing long-lasting protective immunity due to adaptive immunity provided by the memory cells, and not the duration of the vaccine [
10]. Second, it demonstrated that premedication with diphenhydramine can protect recipients against vaccine-induced AALR without affecting the immunogenicity of the vaccine.
The BNT162b2 vaccine consists of mRNA encased in a lipid membrane [
3]. Allergen-induced basophil reactivity against the BNT162b2 vaccine may be mediated by polyethylene glycosylated (PEGylated) lipid nanoparticles present on the lipid membrane [
11]. This can be prevented by administering antihistamines prior to vaccination [
7]. In addition, mRNA vaccines could elicit immunity through transfection of antigen-presenting cells, which is different from live attenuated vaccines [
2]; we considered that diphenhydramine could not affect the levels of SARS-CoV-2 anti-spike immunoglobulin G.
Unfortunately, this study did not evaluate cellular immunogenicity and cytokines other than SARS-CoV-2 anti-spike immunoglobulin G. T cell immunity and cytokines might not only play significant roles in controlling SARS-CoV-2 replication [
12] but could also affect immediate hypersensitivity response in the participants [
13]. Gamma-globulin titer of the additional four-group was higher than the initial six-groups; however, no significant differences were observed between the two groups. There might be a possibility that gammaglobulinemia could induce the formation of immune complexes, similar to type III hypersensitivity reaction, which might induce AALR [
14]. If we could evaluate cellular immunogenicity along with pre- and post- vaccination cytokine levels, it would have helped devise a useful strategy for treating mRNA vaccine-induced allergic reactions with antihistamine agents.
This study is limited by its small sample size. Further extensive studies are required to confirm the safety of using antihistamines to prevent AALR following vaccination with mRNA vaccines and the immunogenicity of a delayed second dose.
5. Conclusions
Our study may show that delayed administration of a second vaccine dose does not adversely affect its immunogenicity and supports the findings of previous reports that antihistamines can be used to prevent AALR to the BNT162b2 vaccine in at-risk individuals. Since HCWs have a high risk of occupational exposure to SARS-CoV-2, previous AALR following vaccination is not a contraindication for further vaccination.
Author Contributions
Conceptualization, K.A. and Y.Y.; methodology, K.A. and Y.Y.; formal analysis, K.A. and Y.Y.; investigation, all authors; visualization, K.A.; writing—original draft preparation, K.A.; writing—review and editing, K.A., N.S., M.I., H.H. and Y.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the GPCC institutional review board (IRB#405-03030) and conducted according to the guidelines of the Declaration of Helsinki. Written informed consent was obtained from all the study participants prior to the commencement of the study. The study was registered in the University Hospital Medical Information Network Center Clinical Trials Registry on 9 June 2020 (UMIN000040679).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the participants to publish this paper.
Data Availability Statement
The data are available from the corresponding author on reasonable request.
Acknowledgments
The authors thank the staff at the Central Clinical Laboratory for their technical assistance with serum preparation. Additionally, we thank Keiko Yanai, Kazuko Komiya, Kazumi Ono, Hiroko Ogiwara, Kyoko Tsuchiya, Sachiko Ogura, and Hiroko Hosokawa for their help with sample collection. All individuals included in this section have consented to the acknowledgement.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, N.; Weissman, D.; Whitehead, K.A. mRNA vaccines for infectious diseases: Principles, delivery and clinical translation. Nat. Rev. Drug Discov. 2021, 20, 817–838. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D., Jr.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.J.; Moreira, E.D.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef] [PubMed]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. Covid-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Cardona, V.; Ansotegui, I.J.; Ebisawa, M.; El-Gamal, Y.; Rivas, M.F.; Fineman, S.; Geller, M.; Gonzalez-Estrada, A.; Greenberger, P.A.; Borges, M.S.; et al. World allergy organization anaphylaxis guidance 2020. World Allergy Organ. J. 2020, 13, 100472. [Google Scholar] [CrossRef]
- Grabowski, J.; Wolff, M.; Pettersson, S.D.; Brancewicz, T.; Bidzan, L. Use of antihistamines for COVID-19 vaccine recipients with risk of anaphylaxis. Eur. J. Transl. Clin. Med. 2022, 5, 8–11. [Google Scholar] [CrossRef]
- Hibino, M.; Watanabe, S.; Kamada, R.; Tobe, S.; Maeda, K.; Horiuchi, S.; Kondo, T. Antibody Responses to the BNT162b2 mRNA Vaccine in Healthcare Workers in a General Hospital in Japan: A Comparison of Two Assays for Anti-spike Protein Immunoglobulin G. Intern. Med. 2022, 61, 811–819. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallusto, F.; Lanzavecchia, A.; Araki, K.; Ahmed, R. From vaccines to memory and back. Immunity 2010, 33, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Troelnikov, A.; Perkins, G.; Yuson, C.; Ahamdie, A.; Balouch, S.; Hurtado, P.R.; Hissaria, P. Basophil reactivity to BNT162b2 is mediated by PEGylated lipid nanoparticles in patients with PEG allergy. J. Allergy Clin. Immunol. 2021, 148, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Moss, P. The T cell immune response against SARS-CoV-2. Nat. Immunol. 2022, 23, 186–193. [Google Scholar] [CrossRef] [PubMed]
- Rivas, M.N.; Chatila, T.A. Regulatory T cells in allergic diseases. J. Allergy Clin. Immunol. 2016, 138, 639–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solomon, S.; Kassahn, D.; Illges, H. The role of the complement and the Fc gamma R system in the pathogenesis of arthritis. Arthritis Res. Ther. 2005, 7, 129–135. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).




{kind=link}