
Fatal Case of Autochthonous Strongyloides stercoralis Hyperinfection in an Immunosuppressed Calabrian Patient

 , ,
, ,
Abstract
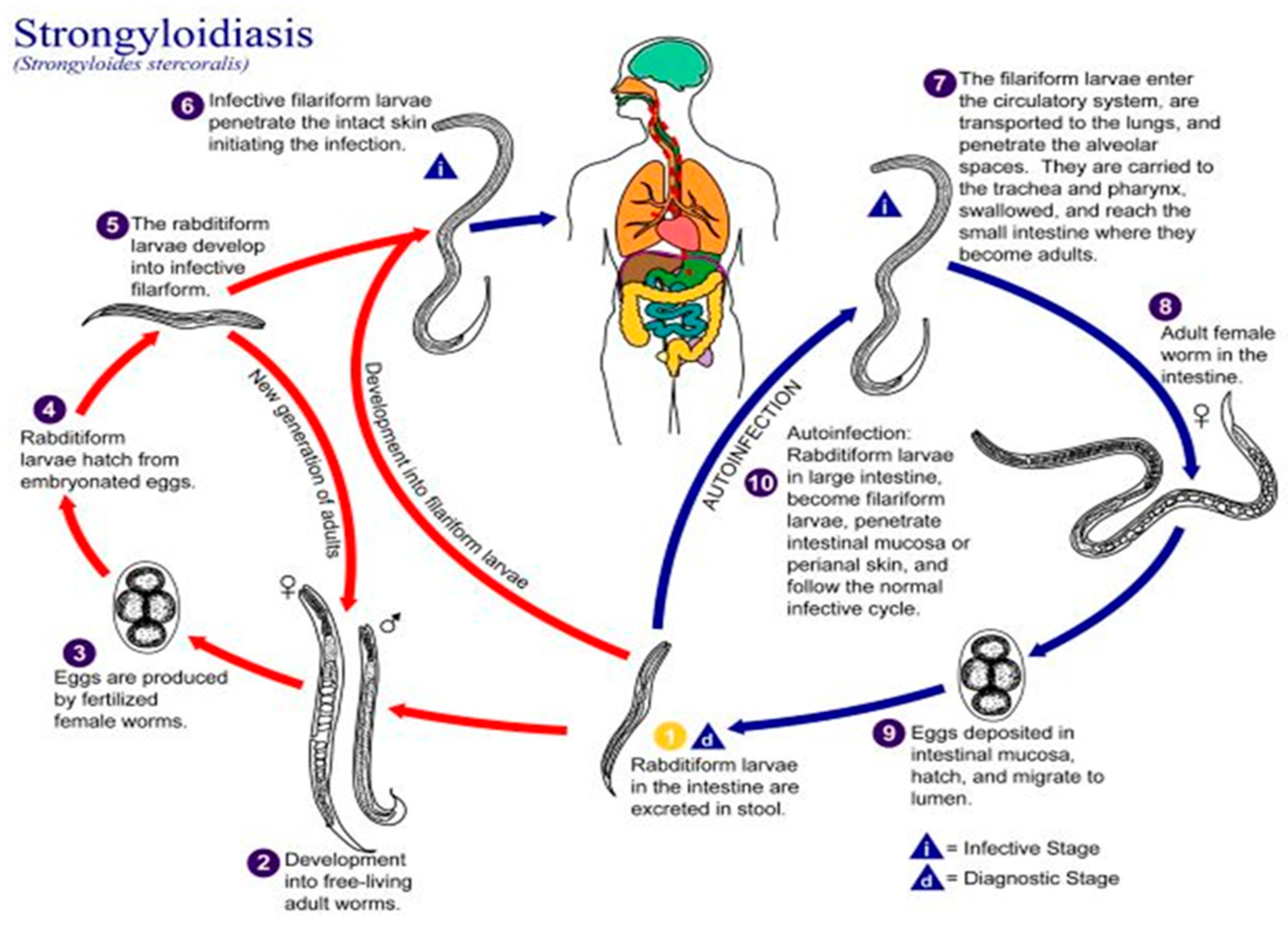
:1. Introduction
2. Case Presentation Section
2.1. Medical History
2.2. Physical Examination
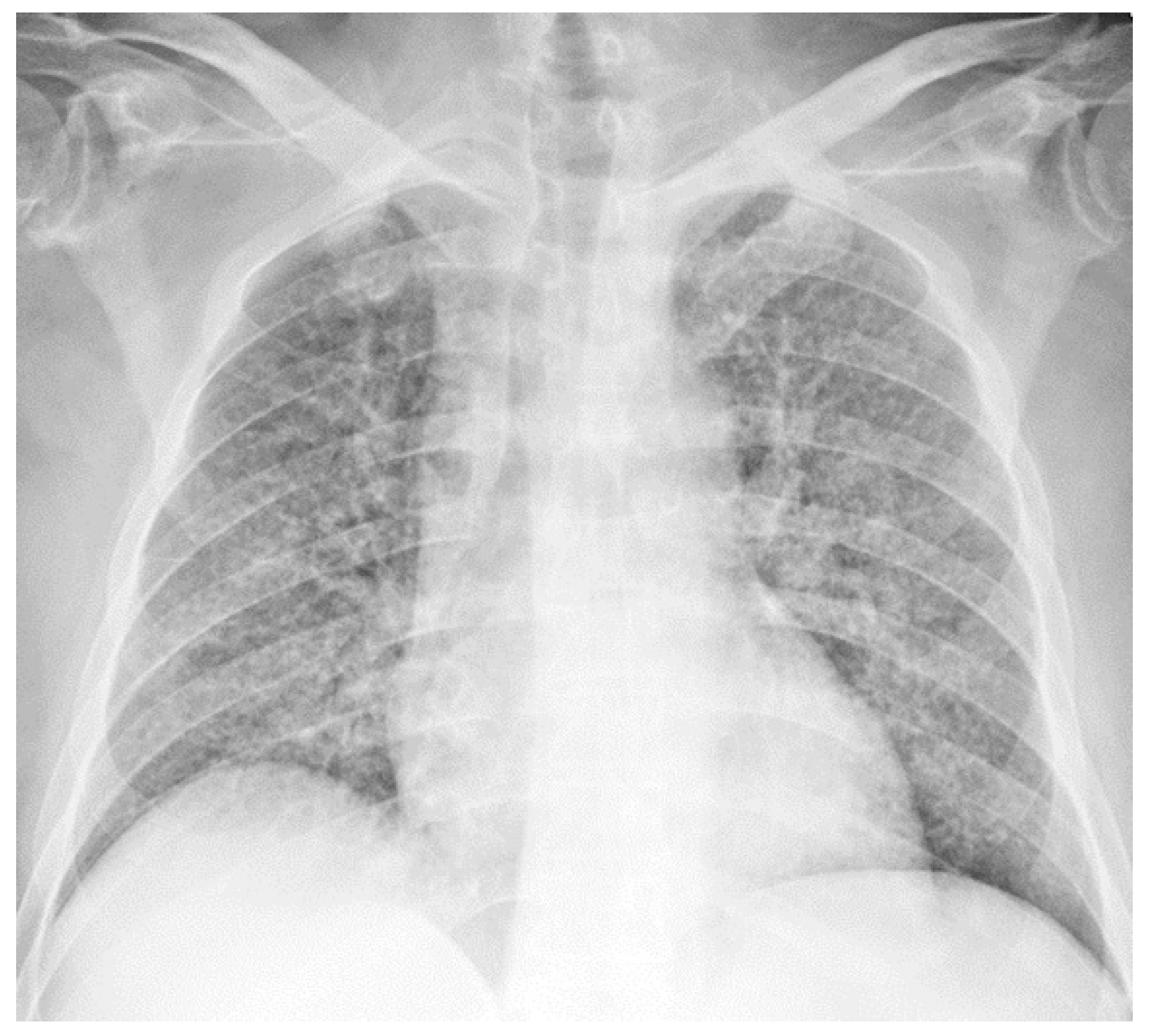
2.3. Chest Radiograph
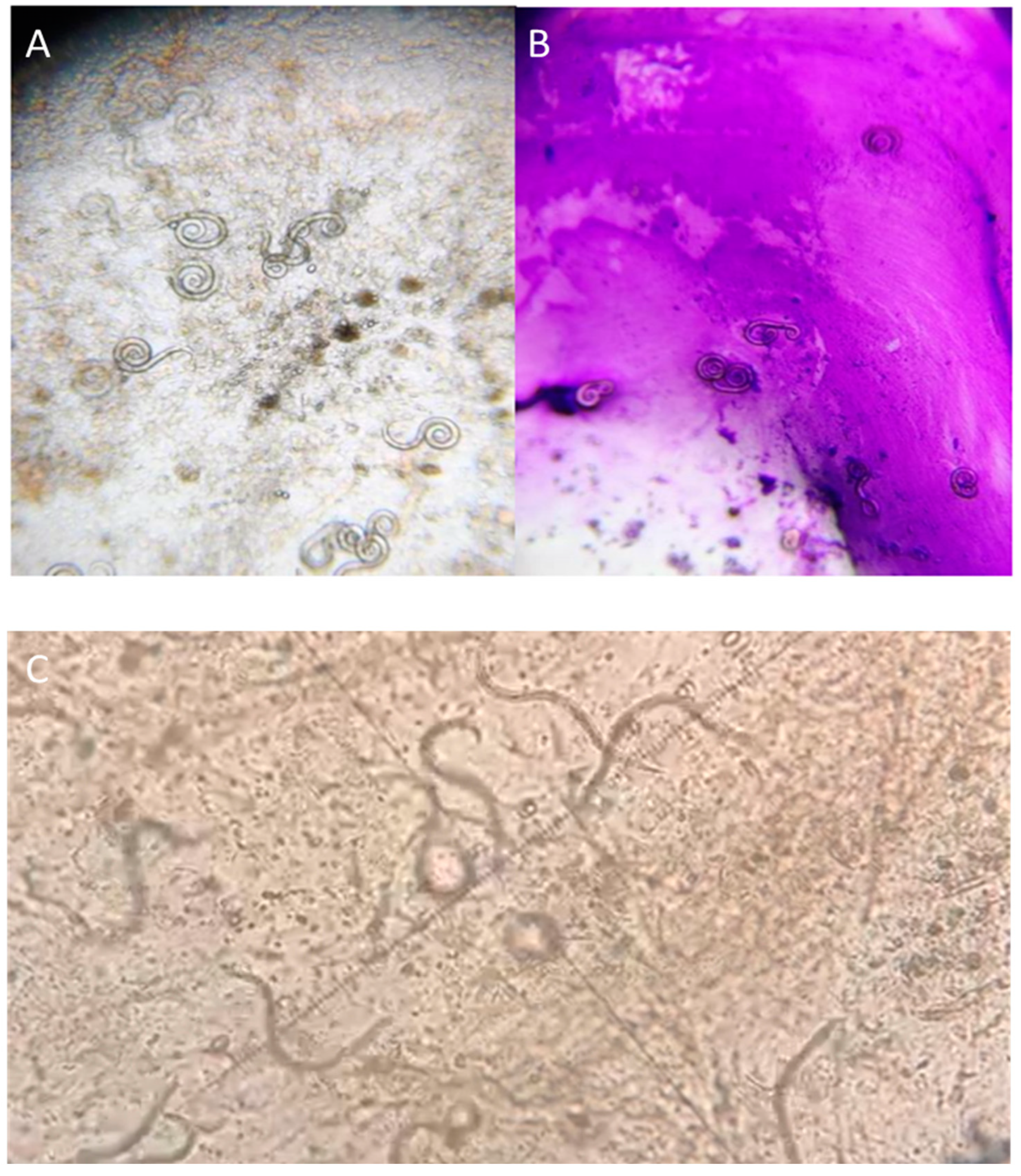
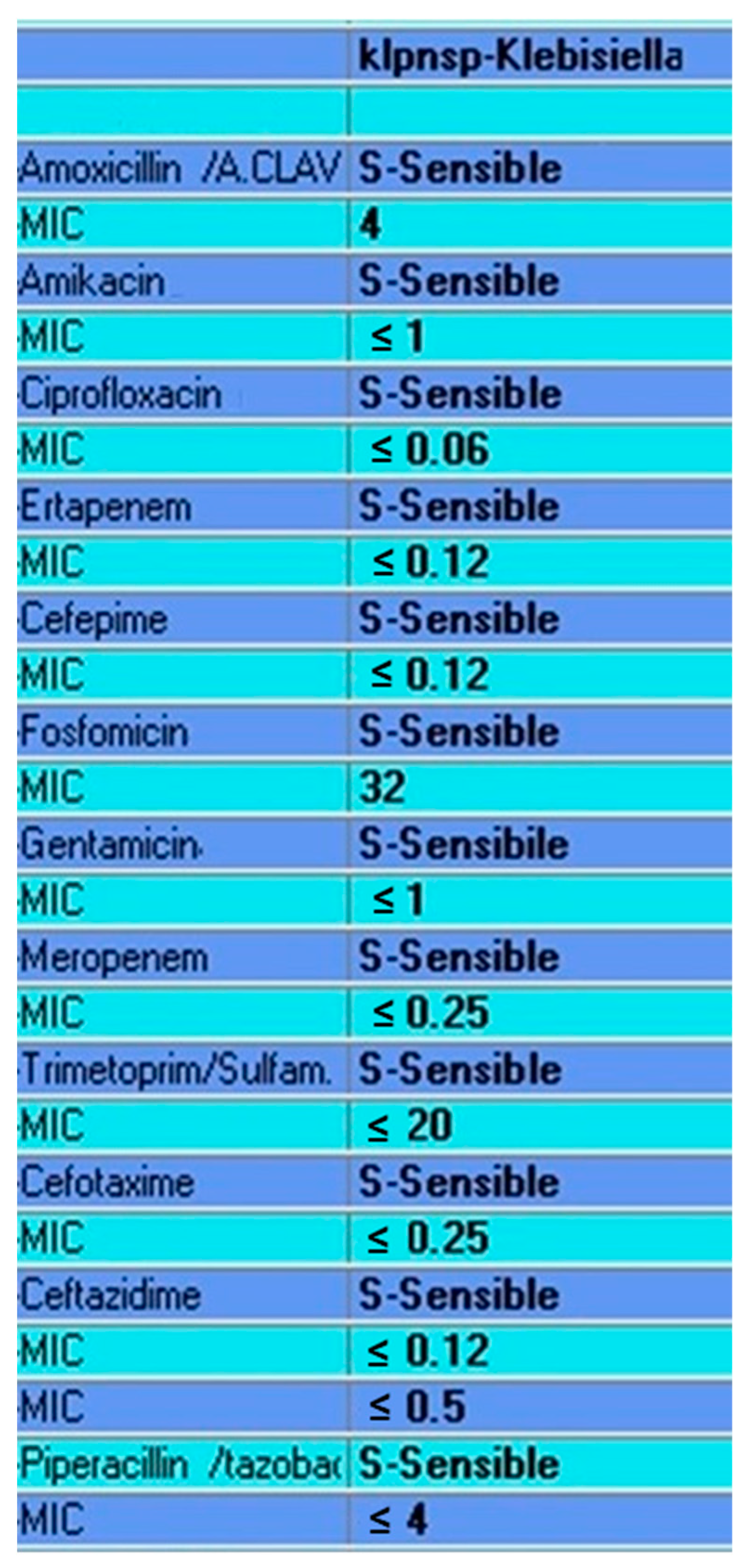
2.4. Laboratory Diagnosis and Therapy
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buonfrate, D.; Bisanzio, D.; Giorli, G.; Odermatt, P.; Fürst, T.; Greenaway, C.; French, M.; Reithinger, R.; Gobbi, F.; Montresor, A.; et al. The Global Prevalence of Strongyloides stercoralis Infection. Pathogens 2020, 9, 468. [Google Scholar] [CrossRef]
- Genta, R.M. Global prevalence of strongyloidiasis: Critical review with epidemiologic insights into the prevention of disseminated disease. Rev. Infect. Dis. 1989, 11, 755–767. [Google Scholar] [CrossRef] [PubMed]
- Al-Hasan, M.N.; McCormick, M.; Ribes, J.A. Invasive enteric infections in hospitalized patients with underlying strongyloidiasis. Am. J. Clin. Pathol. 2007, 128, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Schar, F.; Trostdorf, U.; Giardina, F.; Khieu, V.; Muth, S.; Marti, H.; Vounatsou, P.; Odermatt, P. Strongyloides stercoralis: Global Distribution and Risk Factors. PLoS Negl. Trop. Dis. 2013, 7, e2288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buonfrate, D.; Marrone, R.; Silva, R.; Mirisola, C.; Ragusa, A.; Mistretta, M.; Perandin, F.; Bisoffi, Z. Prevalence of Strongyloidiasis in a Cohort of Migrants in Italy and Accuracy of a Novel ELISA Assay for S. stercoralis Infection, a Cross-Sectional Study. Microorganisms 2021, 9, 401. [Google Scholar] [CrossRef] [PubMed]
- Walzer, P.D.; Milder, J.E.; Banwell, J.G.; Kilgore, G.; Klein, M.; Parker, R. Epidemiologic features of Strongyloides stercoralis infection in an endemic area of the United States. Am. J. Trop. Med. Hyg. 1982, 31, 313–319. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, L.C.; Ribeiro, C.T.; Mendes Dde, M.; Oliveira, T.C.; Costa-Cruz, J.M. Frequency of Strongyloides stercoralis infection in alcoholics. Memórias Do Inst. Oswaldo Cruz 2002, 97, 119–121. [Google Scholar] [CrossRef] [Green Version]
- Davidson, R.A.; Fletcher, R.H.; Chapman, L.E. Risk factors for strongyloidiasis. A case-control study. Arch. Intern. Med. 1984, 144, 321–324. [Google Scholar] [CrossRef]
- Marnell, F.; Guillet, A.; Holland, C. A survey of the intestinal helminths of refugees in Juba, Sudan. Ann. Trop. Med. Parasitol. 1992, 86, 387–393. [Google Scholar] [CrossRef]
- Sanchez, P.R.; Guzman, A.P.; Guillen, S.M.; Adell, R.I.; Estruch, A.M.; Gonzalo, I.N.; Olmos, C.R. Endemic strongyloidiasis on the Spanish Mediterranean coast. Q. J. Med. 2001, 94, 357–363. [Google Scholar] [CrossRef]
- Wagenvoort, J.H.; Houben, H.G.; Boonstra, G.L.; Scherpbier, J. Pulmonary superinfection with Strongyloides stercoralis in an immunocompromised retired coal miner. Eur. J. Clin. Microbiol. Infect. Dis. 1994, 13, 518–519. [Google Scholar] [CrossRef]
- Ottino, L.; Buonfrate, D.; Paradies, P.; Bisoffi, Z.; Antonelli, A.; Rossolini, G.M.; Gabrielli, S.; Bartoloni, A.; Zammarchi, L. Autochthonous Human and Canine Strongyloides stercoralis Infection in Europe: Report of a Human Case in An Italian Teen and Systematic Review of the Literature. Pathogens 2020, 9, 439. [Google Scholar] [CrossRef] [PubMed]
- Nagayasu, E.; Aung, M.P.P.T.H.H.; Hortiwakul, T.; Hino, A.; Tanaka, T.; Higashiarakawa, M.; Olia, A.; Taniguchi, T.; Win, S.M.T.; Ohashi, I.; et al. A possible origin population of pathogenic intestinal nematodes, Strongyloides stercoralis, unveiled by molecular phylogeny. Sci. Rep. 2017, 7, 4844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaleta, T.G.; Zhou, S.; Bemm, F.M.; Schär, F.; Khieu, V.; Muth, S.; Odermatt, P.; Lok, J.B.; Streit, A. Different but overlapping populations of Strongyloides stercoralis in dogs and humans-Dogs as a possible source for zoonotic strongyloidiasis. PLoS Negl. Trop. Dis. 2017, 11, e0005752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, L.X.; Weller, P.F. Strongyloidiasis and other intestinal nematode infections. Infect. Dis. Clin. N. Am. 1993, 7, 655–682. [Google Scholar] [CrossRef]
- Corti, M. Strongyloides stercoralis in Immunosuppressed Patients. Arch. Clin. Infect. Dis. 2016, 11, e27510. [Google Scholar] [CrossRef] [Green Version]
- Olsen, A.; van Lieshout, L.; Marti, H.; Polderman, T.; Polman, K.; Steinmann, P.; Stothard, R.; Thybo, S.; Verweij, J.J.; Magnussen, P. Strongyloidiasis—The most neglected of the neglected tropical diseases? Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 967–972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toledo, R.; Muñoz-Antoli, C.; José-Guillermo, E. Strongyloidiasis with Emphasis on Human Infections and Its Different Clinical Forms. Adv. Parasitol. 2015, 88, 165–241. [Google Scholar] [PubMed]
- Buonfrate, D.; Baldissera, M.; Abrescia, F.; Bassetti, M.; Caramaschi, G.; Giobbia, M.; Mascarello, M.; Rodari, P.; Scattolo, N.; Napoletano, G.; et al. Epidemiology of Strongyloides stercoralis in northern Italy: Results of a multicenter case–control study, February 2013 to July 2014. Eurosurveillance 2016, 21, 30310. [Google Scholar] [CrossRef] [Green Version]
- Abrescia, F.F.; Falda, A.; Caramaschi, G.; Scalzini, A.; Gobbi, F.; Angheben, A.; Gobbo, M.; Schiavon, R.; Rovere, P.; Bisoffi, Z. Reemergence of Strongyloidiasis, Northern Italy. Emerg. Infect. Dis. 2009, 15, 1531–1533. [Google Scholar] [CrossRef]
- Venturini, E.; Fusani, L.; Mantella, A.; Bianchi, L.; Antonelli, A.; Montagnani, C.; Chiappini, E.; Spinicci, M.; Bartoloni, A.; Rossolini, G.M.; et al. Strongyloidiasis in Children Outside the Tropics: Do We Need to Increase Awareness? Microorganisms 2021, 9, 1905. [Google Scholar] [CrossRef] [PubMed]
- Marchese, V.; Crosato, V.; Gulletta, M.; Castelnuovo, F.; Cristini, G.; Mattelli, A.; Castelli, F. Strongyloides infection manifested during immunosuppressive therapy for SARS-CoV-2 pneumonia. Infection 2021, 49, 539–542. [Google Scholar] [CrossRef] [PubMed]
- Beltrame, A.; Bortesi, L.; Benini, M.; Bisoffi, Z. A case of chronic strongyloidiasis diagnosed by histopathological study. Int. J. Infect. Dis. 2018, 77, 1–2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scaglia, M.; Brusita, R.; Gatti, S.; Bernuzzi, A.M.; Strosselli, M.; Malfitano, A.; Capelli, D. Autochtonous strongyloidiasis in Italy: An epidemiological and clinical review of 150 cases. Bull. Soc. Path. Ex. 1984, 77, 328–332. [Google Scholar]
- Angheben, A.; Mistretta, M.; Gobbo, M.; Bonafini, S.; Iacovazzi, T.; Sepe, A.; Gobbi, F.; Marocco, S.; Rossanese, A.; Bisoffi, Z. Acute strongyloidiasis in Italian tourists returning from Southeast Asia. J. Travel Med. 2011, 18, 138–140. [Google Scholar] [CrossRef] [Green Version]
- Montes, M.; Sanchez, C.; Verdonck, K.; Lake, J.E.; Gonzalez, E.; Lopez, G.; Terashima, A.; Nolan, T.; Lewis, D.E.; Gotuzzo, E.; et al. Regulatory T Cell Expansion in HTLV-1 and Strongyloidiasis Co-infection Is Associated with Reduced IL-5 Responses to Strongyloides stercoralis Antigen. PLoS Negl. Trop. Dis. 2009, 3, e456. [Google Scholar] [CrossRef] [Green Version]
- Pandiyan, P.; Zheng, L.; Ishihara, S.; Reed, J.; Lenardo, M.J. CD4+CD25+Foxp3+ regulatory T cells induce cytokine deprivation-mediated apoptosis of effector CD4+ T cells. Nat. Immunol. 2007, 8, 1353–1362. [Google Scholar] [CrossRef]
- Concha, R.; Harrington, W.J.; Rogers, A.I. Intestinal strongyloidiasis: Recognition, management, and determinants of outcome. J. Clin. Gastroenterol. 2005, 39, 203–211. [Google Scholar] [CrossRef]
- Suvajdzic, N.; Kranjcic-Zec, I.; Jovanovic, V.; Popovic, D.; Colovic, M. Fatal strongyloidosis following corticosteroid therapy in a patient with chronic idiopathic thrombocytopenia. Haematologia 1999, 29, 323–326. [Google Scholar]
- Kaslow, J.E.; Novey, H.S.; Zuch, R.H.; Spear, G.S. Disseminated strongyloidiasis: An unheralded risk of corticosteroid therapy. J. Allergy Clin. Immunol. 1990, 86, 138–142. [Google Scholar] [CrossRef]
- Thomas, M.C.; Costello, S.A. Disseminated strongyloidiasis arising from a single dose of dexamethasone before stereotactic radiosurgery. Int. J. Clin. Pract. 1998, 52, 520–521. [Google Scholar] [PubMed]
- Siddiqui, A.A.; Berk, S.L.; Genta, R.M. Strongyladiasis. In Tropical Infections Diseases; Elsevier: Philadelphia, PA, USA, 2005; pp. 1274–1285. [Google Scholar]
- Keiser, P.B.; Nutman, T.B. Strongyloides stercoralis in the Immunocompromised Population. Clin. Microbiol. Rev. 2004, 17, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Karachi, A.; Dastmalchi, F.; Mitchell, D.A.; Rahman, M. Temozolomide for immunomodulation in the treatment of glioblastoma. Neuro-Oncology 2018, 20, 1566–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janeway, C.A.; Negrao-Correa, D.; Taylor & Francis Group. Importance of immunoglobulin E (IgE) in the protective mechanism against gastrointestinal nematode infection: Looking at the intestinal mucosae. Rev. Inst. Med. Trop. Sao Paulo 2001, 43, 291–299. [Google Scholar]
- Siddiqui, A.A.; Berk, S.L. Diagnosis of Strongioloides stercoralis Infection. Clin. Infect. Dis. 2001, 33, 1040–1047. [Google Scholar] [CrossRef] [Green Version]
- Newnham, M.S. Manifestations, diagnosis, and treatment of Strongioloides stercoralis infection. Ann. Pharmacother. 2007, 41, 1992–2001. [Google Scholar] [CrossRef]
- Luvira, V.; Siripoon, T.; Phiboonbanakit, D.; Somsri, K.; Watthanakulpanich, D.; Dekumyoy, P. Strongyloides stercoralis: A Neglected but Fatal Parasite. Trop. Med. Infect. Dis. 2022, 7, 310. [Google Scholar] [CrossRef]
- Luvira, V.; Watthanakulpanich, D.; Pittisuttithum, P. Management of Strongyloides stercoralis: Puzzling parasite. Int. Health 2014, 6, 273–281. [Google Scholar] [CrossRef]
- Newberry, A.M.; Williams, D.N.; Stauffer, W.M.; Boulware, D.R.; Hendel-Paterson, B.R.; Walker, P.F. Strongyloides hyperinfection presenting as acute respiratory failure and gram-negative sepsis. Chest 2005, 128, 3681–3684. [Google Scholar] [CrossRef] [Green Version]
- Mendes, T.; Minori, K.; Ueta, M.; Miguel, D.C.; Allegretti, S.M. Strongyloidiasis Current Status with Emphasis in Diagnosis and Drug Research. J. Parasitol. Res. 2017, 2017, 5056314. [Google Scholar] [CrossRef] [Green Version]
- Santiago, M.; Leitao, B. Prevention of Strongyloides hyperinfection syndrome: A rheumatological point of view. Eur. J. Intern. Med. 2009, 20, 744–748. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.; Nellore, A. Management of Strongyloides in Solid Organ Transplant Recipients. Infect. Dis. Clin. N. Am. 2018, 32, 749–763. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bio-Parameters | 13th November | 14th November | 16th November | 17th November | 18th November | Normal Range | Range Reference |
|---|---|---|---|---|---|---|---|
| Total IgE | - | - | 361.3 | - | - | 0.5–158 | IU/mL |
| PCT | 1.00 mg/L | 15.92 mg/L | - | - | - | 0–0.05 | mg/L |
| Blood glucose | 253 mg/dL | - | - | - | - | 74–106 | mg/dL |
| White Blood Cell | 7.98 | 12.64 | 11.77 | 9.72 | 10.68 | 4.60–10.20 | ×103 μL |
| Red Blood Cell | 2.54 | 2.05 | 2.57 | 2.31 | 2.47 | 4.20–6.10 | ×106 μL |
| Hb | 8.7 | 7.3 | 8.5 | 7.6 | 8.1 | 12.0–18 | g/dL |
| HCT | 25.4 | 21.1 | 25.6 | 23.5 | 24.2 | 37–52 | % |
| MCV | 99.8 | 102.6 | 99.8 | 101.4 | 97.9 | 80–99 | fL |
| MCH | 34.4 | 35.3 | 33.3 | 33 | 32.5 | 27–32 | pg |
| MCHC | 34.4 | 34.4 | 33.4 | 32.5 | 33.2 | 32–37 | g/dL |
| RDW | 15.2 | 16 | 18.3 | 18.5 | 19.6 | 11.9–15 | % |
| Platelet | 186 | 190 | 162 | 116 | 94 | 130–400 | ×103 μL |
| MPV | 9.4 | 9.9 | 9.6 | 10.6 | 11.3 | 7.4–11 | fL |
| Plateletcrit | 0.18 | 0.2 | 0.15 | 0.123 | 0.11 | 0.18 | % |
| Differential White Blood Cell Count | 0.01–0.38 | ×103 μL | |||||
| Neutrophil | 86.8 | 90.4 | 90 | 90.5 | 93.5 | 40–74 | % |
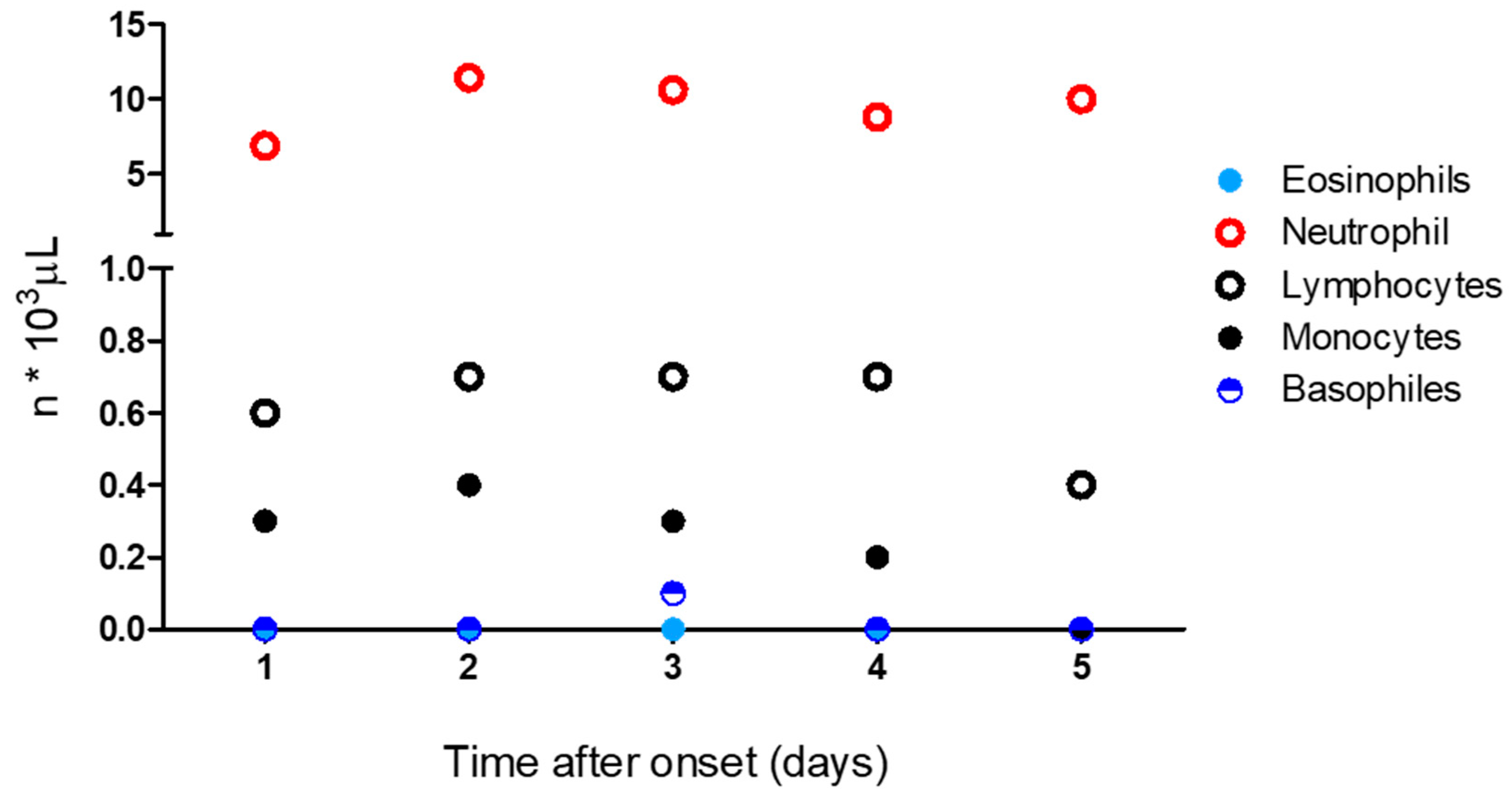
| 6.9 | 11.4 | 10.6 | 8.8 | 10 | 1.9–8 | ×103 μL | |
| Lymphocytes | 7.5 | 5.3 | 5.6 | 6.8 | 3.8 | 19–48 | % |
| 0.6 | 0.7 | 0.7 | 0.7 | 0.4 | 0.9–5.2 | ×103 μL | |
| Monocytes | 3.5 | 2.9 | 2.8 | 1.9 | 2 | 3.4–12 | % |
| 0.3 | 0.4 | 0.3 | 0.2 | 0.0 | 0.16–1 | ×103 μL | |
| Eosinophils | 0.2 | 0.1 | 0.1 | 0.1 | 0.0 | 0.0–7 | % |
| 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0–0.8 | ×103 μL | |
| Basophiles | 0.3 | 0.3 | 0.4 | 0.2 | 0.2 | 0.0–1.5 | % |
| 0.0 | 0.0 | 0.1 | 0.0 | 0.0 | 0.0–0.2 | ×103 μL | |
| Large Unstained Cell (LUC) | 16.1 | 1 | 1.0 | 0.5 | 0.5 | 0.15–6 | % |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colosimo, M.; Caroleo, M.C.; Caruso, A.; Luciani, F.; Cione, E.; Talarico, G.; Vescio, V.; De Sarro, G.; Minchella, P.; Nisticò, S. Fatal Case of Autochthonous Strongyloides stercoralis Hyperinfection in an Immunosuppressed Calabrian Patient. Reports 2022, 5, 47. https://doi.org/10.3390/reports5040047
Colosimo M, Caroleo MC, Caruso A, Luciani F, Cione E, Talarico G, Vescio V, De Sarro G, Minchella P, Nisticò S. Fatal Case of Autochthonous Strongyloides stercoralis Hyperinfection in an Immunosuppressed Calabrian Patient. Reports. 2022; 5(4):47. https://doi.org/10.3390/reports5040047
Chicago/Turabian StyleColosimo, Manuela, Maria Cristina Caroleo, Antonella Caruso, Filippo Luciani, Erika Cione, Giusy Talarico, Virginia Vescio, Giovambattista De Sarro, Pasquale Minchella, and Salvatore Nisticò. 2022. "Fatal Case of Autochthonous Strongyloides stercoralis Hyperinfection in an Immunosuppressed Calabrian Patient" Reports 5, no. 4: 47. https://doi.org/10.3390/reports5040047