
A Possible New Diagnostic Method for Early Diagnosis of Cryptococcus Infection in Lymphoma Patient Co-Infected with SARS-CoV-2
 and
and
Abstract
:1. Introduction
2. Case Presentation
3. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kozel, T.R.; Wickes, B. Fungal diagnostics. Cold Spring Harb. Perspect. Med. 2014, 4, a019299. [Google Scholar] [CrossRef] [PubMed]
- Srichatrapimuk, S.; Sungkanuparph, S. Integrated therapy for HIV and cryptococcosis. AIDS Res. Ther. 2016, 13, 42. [Google Scholar] [CrossRef] [Green Version]
- Negroni, R. Cryptococcosis. Clin. Regul. Dermatol. 2012, 30, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.; Idnurm, A.; Lin, X. Morphology and its underlying genetic regulation impact the interaction between Cryptococcus neoformans and its hosts. Med. Mycol. 2015, 53, 493–504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiertiburanakul, S.; Wirojtananugoon, S.; Pracharktam, R.; Sungkanuparph, S. Cryptococcosis in human immunodeficiency virus-negative patients. Int. J. Infect. Dis. 2006, 10, 72–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmalzle, S.A.; Buchwald, U.K.; Gilliam, B.L.; Riedel, D.J. Cryptococcus neoformansinfection in malignancy. Mycoses 2020, 63, 1033–1046. [Google Scholar] [CrossRef] [PubMed]
- Cunha Pereira, T.; Rb-Silva, R.; Félix Soares, R.; Domingues, N.; Mariz, J. Case Report: Cryptococcal meningitis in Hodgkin’s Lymphoma patient receiving brentuximab-vedotin therapy. F1000Research 2020, 9, 687. [Google Scholar] [CrossRef]
- Rhew, D.C.; Gaultier, C.R.; Daar, E.S.; Zakowski, P.C.; Said, J. Infections in Patients with Chronic Adult T-Cell Leukemia/Lymphoma: Case Report and Review. Clin. Infect. Dis. 1995, 21, 1014–1016. [Google Scholar] [CrossRef]
- Korfel, A.; Menssen, H.D.; Schwartz, S.; Thiel, E. Cryptococcosis in Hodgkin’s disease: Description of two cases and review of the literature. Ann. Hematol. 1998, 76, 283–286. [Google Scholar] [CrossRef]
- Dincol, G.; Kahraman, R. Cryptococcus neoformans meningitis in a patient with hairy cell Leukmia. Am. J. Hematol. 2006, 81, 387. [Google Scholar] [CrossRef]
- Reisfeld-Zadok, S.; Elis, A.; Szyper-Kravitz, M.; Chowers, M.; Lishner, M. Cryptococcal meningitis in chronic lymphocytic leukemia patients. Isr. Med. Assoc. J. IMAJ 2009, 11, 437–439. [Google Scholar] [PubMed]
- Pagano, L.; Fianchi, L.; Caramatti, C.; D’Antonio, D.; Melillo, L.; Caira, M.; Masini, L.; Todeschini, G.; Girmenia, C.; Martino, B.; et al. Cryptococcosis in patients with hematologic malignancies. A report from GIMEMA-infection. Haematologica 2004, 89, 852–856. [Google Scholar] [PubMed]
- Hirai, Y.; Ainoda, Y.; Shoji, T.; Fujita, T.; Yoshinaga, K.; Shiseki, M.; Mori, N.; Teramura, M.; Totsuka, K.; Motoji, T. Disseminated Cryptococcosis in a Non-Hodgkin’s Lymphoma Patient with Late-Onset Neutropenia Following Rituximab-CHOP Chemotherapy: A Case Report and Literature Review. Mycopathologia 2011, 172, 227–232. [Google Scholar] [CrossRef]
- Zhang, F.; Li, Y.; Shen, H.; Tao, J.; Wang, J. Case Report: Cryptococcal eosinophilic meningitis in a patient with Hodgkin lymphoma. Front. Neurol. 2022, 13, 898525. [Google Scholar] [CrossRef]
- A To, C.; Hsieh, R.W.; McClellan, J.S.; Howard, W.; Fischbein, N.J.; Brown, J.M.Y.; Felsher, D.W.; Fan, A.C. Cryptococcal osteomyelitis and meningitis in a patient with non-hodgkin’s lymphoma treated with PEP-C. BMJ Case Rep. 2012, 2012. [Google Scholar] [CrossRef]
- Chaaban, S.; Wheat, L.; Assi, M. Cryptococcal meningitis post autologous stem cell transplantation. Transpl. Infect. Dis. 2014, 16, 473–476. [Google Scholar] [CrossRef]
- Cruz, D.; Costa, P.; Sagüés, M. Meningeal cryptococcosis in a patient with angioimmunoblastic lymphoma treated with alemtuzumab. Med. Clin. 2019, 152, e19–e20. [Google Scholar] [CrossRef]
- Marcianò, G.; Roberti, R.; Palleria, C.; Mirra, D.; Rania, V.; Casarella, A.; De Sarro, G.; Gallelli, L. SARS-CoV-2 Treatment: Current Therapeutic Options and the Pursuit of Tailored Therapy. Appl. Sci. 2021, 11, 7457. [Google Scholar] [CrossRef]
- Kaplan, M.H.; Rosen, P.P.; Armstrong, D. Cryptococcosis in a cancer hospital.Clinical and pathological correlates in forty-six patients. Cancer 1977, 39, 2265–2274. [Google Scholar] [CrossRef]
- Kontoyiannis, D.P.; Peitsch, W.K.; Reddy, B.T.; Whimbey, E.E.; Han, X.Y.; Bodey, G.P.; Rolston, K.V.I. Cryptococcosis in Patients with Cancer. Clin. Infect. Dis. 2001, 32, e145–e150. [Google Scholar] [CrossRef] [Green Version]
- Bloomfield, N.; Gordon, M.A.; Elmendorf, D.F.; Elmendorf, J.D.F. Detection of Cryptococcus neoformans Antigen in Body Fluids by Latex Particle Agglutination. Exp. Biol. Med. 1963, 114, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Marcos, J.Y.; Pincus, D.H. Fungal diagnostics: Review of commercially available methods. In Fungal Diagnostics: Methods and Protocols; Springer: Berlin/Heidelberg, Germany, 2013; pp. 25–54. [Google Scholar]
- Tanner, D.C.; Weinstein, M.P.; Fedorciw, B.; Joho, K.L.; Thorpe, J.J.; Reller, L. Comparison of commercial kits for detection of cryptococcal antigen. J. Clin. Microbiol. 1994, 32, 1680–1684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gates-Hollingsworth, M.A.; Kozel, T.R. Serotype Sensitivity of a Lateral Flow Immunoassay for Cryptococcal Antigen. Clin. Vaccine Immunol. 2013, 20, 634–635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panackal, A.A.; Dekker, J.P.; Proschan, M.; Beri, A.; Williamsona, P.R. Enzyme Immunoassay versus Latex Agglutination Cryptococcal Antigen Assays in Adults with Non-HIV-Related Cryptococcosis. J. Clin. Microbiol. 2014, 52, 4356–4358. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Normal Range | 14 May | 20 May | 23 May | 30 May | 3 June | 6 June | 9 June | |
|---|---|---|---|---|---|---|---|---|
| Blood Cells | 3.92–5.13 million cells/µL | 4.8 | 4.9 | 4.9 | 6.5 | 4.3 | 3.9 | 4.5 |
| White Cells | 3.4–9.6 billion cells/L | 4.6 | 4.5 | 4.4 | 4.2 | 3.8 | 3.4 | 3.4 |
| Hemoglobin | 11.6–15 g/dL | 13.2 | 12.6 | 12.1 | 14.4 | 12.2 | 9.2 | 9.3 |
| Platelets | 157,000–371,000/mcL | 18,900 | 175,000 | 192,000 | 123,000 | 103,000 | 98,000 | 91,000 |
| Neutrophils | 40–60% | 78.1 | 77.5 | 77.1 | 82.5 | 77.5 | 78.6 | 75.4 |
| Lymphocytes | 20–40% | 14.1 | 14.1 | 13.9 | 9.9 | 9.8 | 13.0 | 17.5 |
| Monocytes | 2–8% | 5.2 | 6.0 | 6.6 | 4.5 | 5.4 | 4.8 | 3.2 |
| Eosinophils | 1–4% | 0.0 | 0.1 | 0.1 | 0.1 | 0.1 | 0.0 | 0.1 |
| Basophils | 0.5–1% | 0.1 | 0.2 | 0.3 | 0.2 | 0.9 | 0.2 | 0.2 |
| Large Unstained Cells | <4% | 2.4 | 2.0 | 2.0 | 2.9 | 6.4 | 3.3 | 3.6 |
| C Reactive protein | 5–10 mg/L | 19.1 | 6.79 | 10 | 10.8 | |||
| Pro calcitonin | <0.05 ng/mL | 0.06 | 0.05 | 0.10 | 0.10 | |||
| Erythro sedimentation rate | <28 mm/hours | 16 | 16 | |||||
| Β-d glucan | <3 | <3 | <3 |
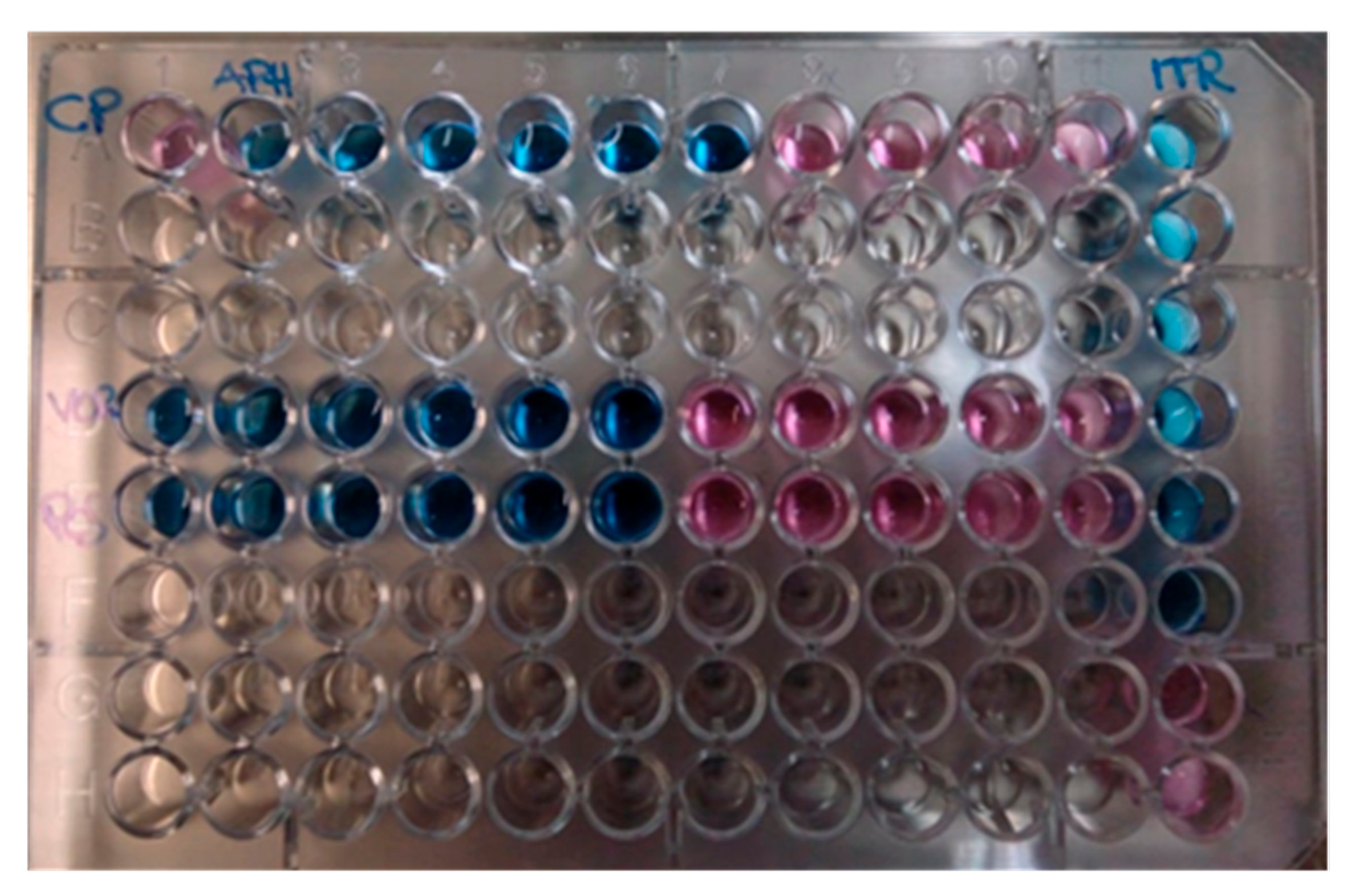
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| A | CP | APH:16 | 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.0625 | 0.031 | ITR 4 |
| B | 2 | |||||||||||
| C | 1 | |||||||||||
| D | VOR: 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.0625 | 0.031 | 0.015 | 0.0078 | 0.5 |
| E | POS: 8 | 4 | 2 | 1 | 0.5 | 0.25 | 0.125 | 0.0625 | 0.031 | 0.015 | 0.0078 | 0.25 |
| F | 0.125 | |||||||||||
| G | 0.0625 | |||||||||||
| H | 0.031 |
| Test | Type of Test | Sensitivity % | Sample | Drawbacks |
|---|---|---|---|---|
| India ink | Rapid test | 30–80 | CSF | low sensitivity, technical subjectivity |
| Culture | Bird seed agar | 50–80 | CSF, blood | requires extensive laboratory infrastructure; long incubation time (2 days); low sensitivity |
| Latex agglutination and ELISA Test (Serology) | Early diagnosis in asymptomatic HIV + patients (20–45 min) | 90 | CSF, serum | expensive, requires extensive laboratory infrastructure |
| Lateral flow assay (immuno- chromatography) | Early diagnosis in asymptomatic HIV + patients (10 min) | 95 | CSF, serum |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colosimo, M.; Nisticò, S.; Quintieri, F.; De Luca, A.; Minchella, P.; Gallelli, L. A Possible New Diagnostic Method for Early Diagnosis of Cryptococcus Infection in Lymphoma Patient Co-Infected with SARS-CoV-2. Reports 2023, 6, 11. https://doi.org/10.3390/reports6010011
Colosimo M, Nisticò S, Quintieri F, De Luca A, Minchella P, Gallelli L. A Possible New Diagnostic Method for Early Diagnosis of Cryptococcus Infection in Lymphoma Patient Co-Infected with SARS-CoV-2. Reports. 2023; 6(1):11. https://doi.org/10.3390/reports6010011
Chicago/Turabian StyleColosimo, Manuela, Salvatore Nisticò, Francesco Quintieri, Annamaria De Luca, Pasquale Minchella, and Luca Gallelli. 2023. "A Possible New Diagnostic Method for Early Diagnosis of Cryptococcus Infection in Lymphoma Patient Co-Infected with SARS-CoV-2" Reports 6, no. 1: 11. https://doi.org/10.3390/reports6010011