

Unusual Case of Biliary Peritonitis in a Dog Secondary to a Gastric Perforation

 , ,
, , {kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
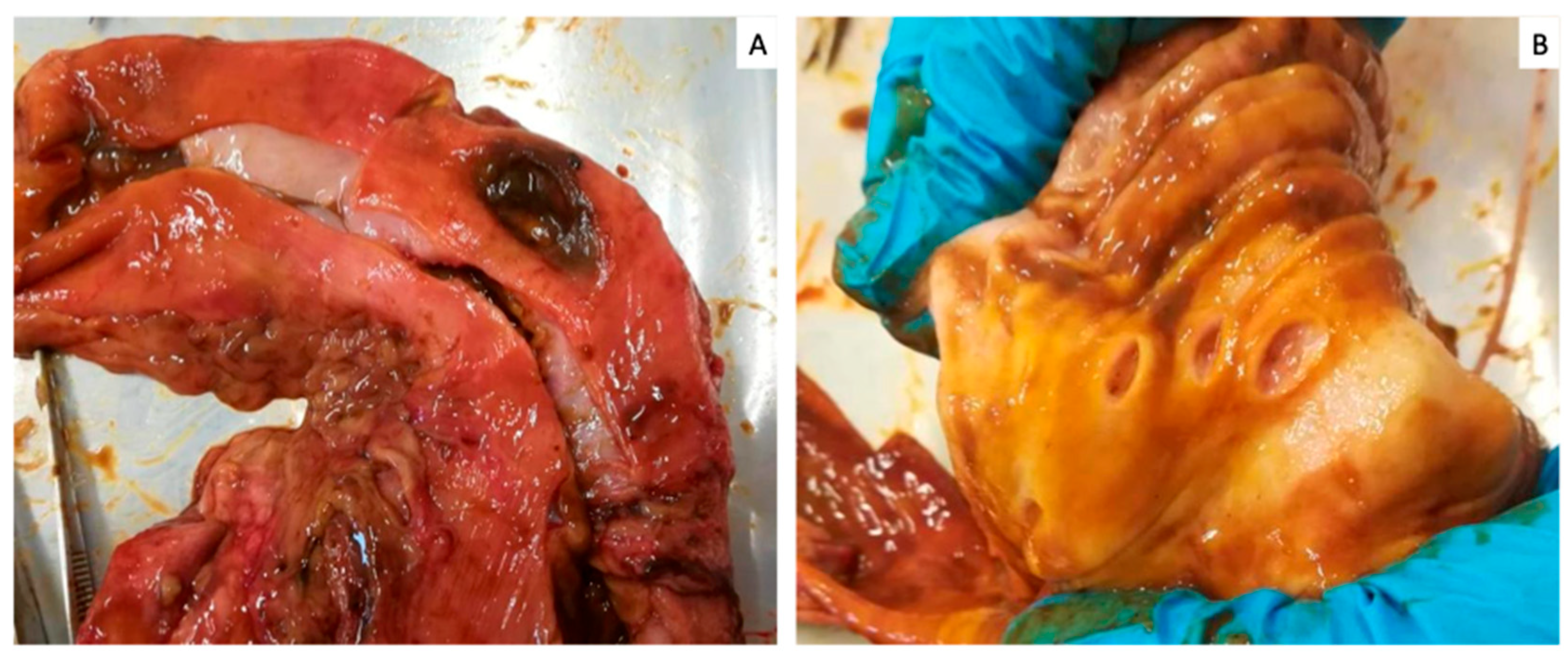
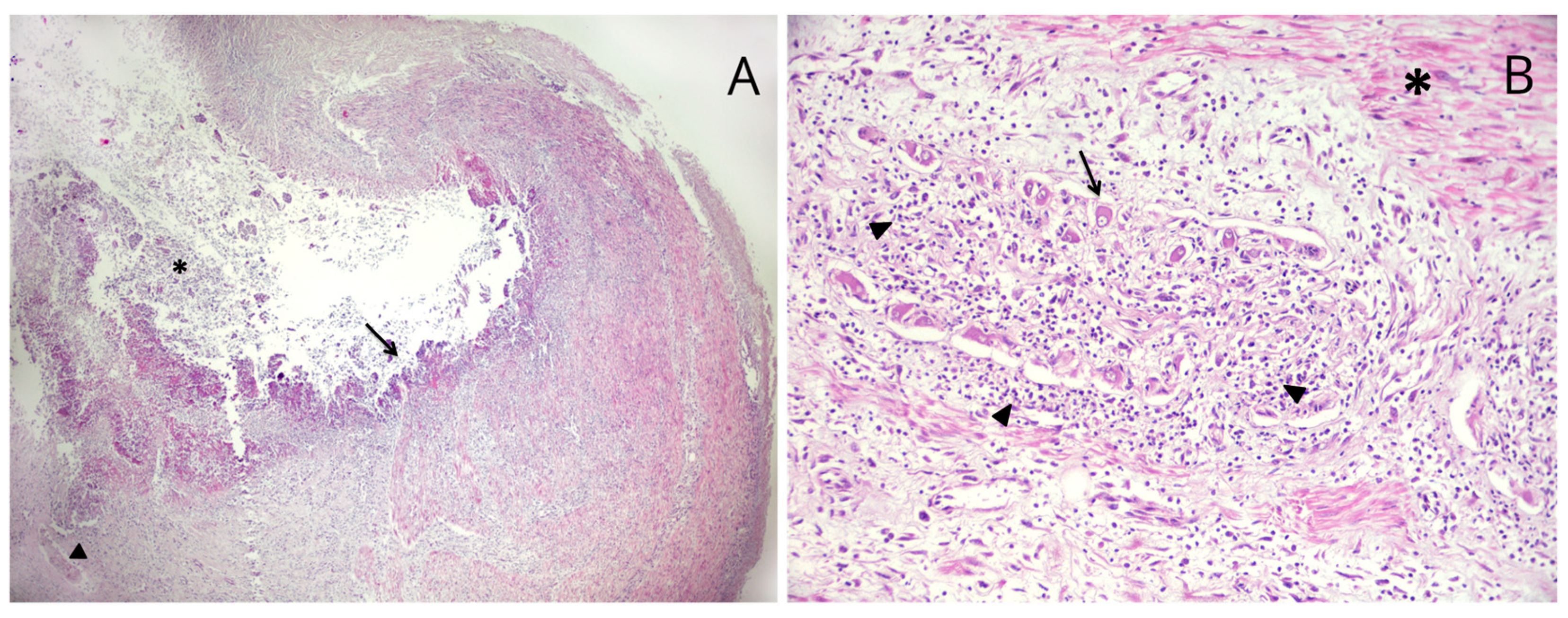
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thompson, B.J.; Sherman, R.A. Comprehensive Review of Biliary Peritonitis. Top. Companion Anim. Med. 2021, 44, 100532. [Google Scholar] [CrossRef]
- Mehler, S.J. Complications of the extra hepatic biliary surgery in companion animals. Vet. Clin. N. Am. Small Anim. Pract. 2011, 41, 949–967. [Google Scholar] [CrossRef]
- Crews, L.J.; Feeney, D.A.; Jessen, C.R.; Rose, N.D.; Matise, I. Clinical, ultrasonographic, and laboratory findings associated with gallbladder disease and rupture findings: 45 cases (1997–2007). J. Am. Vet. Med. Assoc. 2009, 234, 359–366. [Google Scholar] [CrossRef]
- Church, E.M.; Matthiesen, D.T. Surgical treatment of 23 dogs with necrotizing cholecystitis. J. Am. Anim. Hosp. Assoc. 1988, 24, 305–310. [Google Scholar]
- Mutsaers, S.E. The mesothelial cell. Int. J. Biochem. Cell Biol. 2004, 36, 9–16. [Google Scholar] [CrossRef]
- Ludwig, L.L.; McLoughlin, M.A.; Graves, T.K.; Crisp, M.S. Surgical treatment of bile peritonitis in 24 dogs and 2 cats: A retrospective study (1987–1994). Vet. Surg. 1997, 26, 90–98. [Google Scholar] [CrossRef]
- MacLeod, A.N.; Reichle, J.K.; Szabo, D.; Cohen, E.B.; Artiles, C.; Fulkerson, C.V.; Kurihara, M.; Mattoon, J. Ultrasonographic Appearance of Gallbladder Neoplasia in 14 Dogs and 1 Cat. Vet. Radiol. Ultrasound, 2023; ahead of print. [Google Scholar] [CrossRef]
- Harrison, J.; Turek, B.; Brown, D.; Bradley, C.; Clark, J.C. Cholangitis and Cholangiohepatitis in Dogs: A Descriptive Study of 54 Cases Based on Histopathologic Diagnosis (2004–2014). J. Vet. Intern. Med. 2018, 32, 172–180. [Google Scholar] [CrossRef]
- Wilkinson, A.R.; DeMonaco, S.M.; Panciera, D.L.; Otoni, C.C.; Leib, M.S.; Larson, M.M. Bile duct obstruction associated with pancreatitis in 46 dogs. J. Vet. Intern. Med. 2020, 34, 1794–1800. [Google Scholar] [CrossRef]
- Hamura, R.; Haruki, K.; Tsutsumi, J.; Takayama, S.; Shiba, H.; Yanaga, K. Spontaneous biliary peritonitis with common bile duct stones: Report of a case. Surg. Case Rep. 2016, 2, 103. [Google Scholar] [CrossRef] [PubMed]
- Shukla, R.M.; Roy, D.; Mukherjee, P.P.; Saha, K.; Mukhopadhyay, B.; Mandal, K.C.; SahaBasu, K.; Barman, S.S. Spontaneous gall bladder perforation: A rare condition in the differential diagnosis of acute abdomen in children. J. Pediatr. Surg. 2011, 46, 241–243. [Google Scholar] [CrossRef]
- Andersson, R.; Tranberg, K.G.; Bengmark, S. Roles of bile and bacteria in biliary peritonitis. Br. J. Surg. 1990, 77, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Jaffey, J.A.; Graham, A.; VanEerde, E.; Hostnik, E.; Alvarez, W.; Arango, J.; Jacobs, C.; DeClue, A.E. Gallbladder mucocele: Variables associated with outcome and the utility of ultrasonography to identify gallbladder rupture in 219 dogs (2007–2016). J. Vet. Intern. Med. 2018, 32, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Besso, J.G.; Wrigley, R.H.; Gliatto, J.M.; Webster, C.R. Ultrasonographic appearance and clinical findings in 14 dogs with gallbladder mucocele. Vet. Radiol. Ultrasound 2000, 41, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kim, A.; Keh, S.; Oh, J.; Kim, H.; Yoon, J. Comparison between ultrasonographic and clinical findings in 43 dogs with gallbladder mucoceles. Vet. Radiol. Ultrasound 2014, 55, 202–207. [Google Scholar] [CrossRef]
- Escobar, M.C.; Neel, J.A. Pathology in practice. J. Am. Vet. Med. Assoc. 2011, 239, 65–67. [Google Scholar] [CrossRef]
- Amsellem, P.M.; Seim, H.B., 3rd; MacPhail, C.M.; Bright, R.M.; Twedt, D.C.; Wrigley, R.H.; Monnet, E. Long-term survival and risk factors associated with biliary surgery in dogs: 34 cases. J. Am. Vet. Med. Assoc. 2006, 229, 1451–1457. [Google Scholar] [CrossRef]
- Norwich, A. Gallbladder mucocele in a 12 year-old cocker spaniel. Can. Vet. J. 2011, 52, 319–321. [Google Scholar]
- O’Brien, P.J.; Lumsden, J.H. The cytologic examination of body cavity fluids. Semin. Vet. Med. Surg. (Small Anim.) 1988, 3, 140–156. [Google Scholar]
- Bonczynski, J.J.; Ludwig, L.L.; Barton, L.J.; Loar, A.; Peterson, M.E. Comparison of peritoneal fluid and peripheral blood pH, bicarbonate, glucose, and lactate concentration as a diagnostic tool for septic peritonitis in dogs and cats. Vet. Surg. 2003, 32, 161–166. [Google Scholar] [CrossRef]
- Levin, G.M.; Bonczynski, J.J.; Ludwig, L.L.; Barton, L.J.; Loar, A.S. Lactate as a diagnostic test for septic peritoneal effusions in dogs and cats. J. Am. Anim. Hosp. Assoc. 2004, 40, 364–371. [Google Scholar] [CrossRef]
- Dempsey, S.M.; Ewing, P.J. A review of the pathophysiology, classification, and analysis of canine and feline cavitary effusions. J. Am. Anim. Hosp. Assoc. 2011, 47, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Fry, M.M. Diagnosis of uroabdomen. In Nephrology and Urology of Small Animals; Bartges, J., Polzin, D.J., Eds.; Wiley-Blackwell: Ames, IA, USA, 2011; pp. 73–74. [Google Scholar]
- Schmiedt, C.; Tobias, K.M.; Otto, C.M. Evaluation of abdominal fluid: Peripheral blood creatinine and potassium ratios for diagnosis of uroperitoneum in dogs. J. Vet. Emerg. Crit. Care 2011, 11, 275–280. [Google Scholar] [CrossRef]
- Gupta, R.K.; Johnston, P.S.; Naran, S.; Lallu, S.; Fauck, R. Cytological findings in a sample of peritoneal aspirate from a case of bile peritonitis. Diagn. Cytopathol. 2005, 32, 35–37. [Google Scholar] [CrossRef] [PubMed]
- Aumann, M.; Worth, L.T.; Drobatz, K.J. Uroperitoneum in cats: 26 cases (1986–1995). J. Am. Anim. Hosp. Assoc. 1998, 34, 315–324. [Google Scholar] [CrossRef]
- Webb, C.B.; Twedt, D.C. Canine gastritis. Vet. Clin. N. Am. Small Anim. 2003, 33, 969–985. [Google Scholar] [CrossRef]
- Eagon, J.C.; Miedema, B.W.; Kelly, K.A. Postgastrectomy syndromes. Surg. Clin. N. Am. 1992, 72, 445–465. [Google Scholar] [CrossRef]
- Camilleri, M. Gastrointestinal hormones and regulation of gastric emptying. Curr. Opin. Endocrinol. Diabetes Obes. 2019, 26, 3–10. [Google Scholar] [CrossRef]
- Duane, W.C.; Wiegand, D.M. Mechanism by which bile salt disrupts the gastric mucosal barrier in the dog. J. Clin. Investig. 1980, 203, 537–544. [Google Scholar] [CrossRef]
- Ritchie, W.P. Alkaline reflux gastritis. Late results on a controlled trial of diagnosis and treatment. Ann. Surg. 1986, 203, 537–544. [Google Scholar] [CrossRef]
- Naylor, A.; Axon, A. Role of bacterial overgrowth in the stomach as an additional risk factor for gastritis. Can. J. Gastroenterol. 2003, 17 (Suppl. b), 13B–17B. [Google Scholar] [CrossRef]
- Shi, X.; Chen, Z.; Yang, Y.; Yan, S. Bile Reflux Gastritis: Insights into Pathogenesis, Relevant Factors, Carcinomatous Risk, Diagnosis, and Management. Gastroenterol. Res. Pract. 2022, 2022, 2642551. [Google Scholar] [CrossRef] [PubMed]
- Henderson, A.K.; Webster, C.R.L. An in-depth look: Disruption of the gastric mucosal barrier in dogs. Compendium 2006, 28, 340–357. [Google Scholar]
- Bertolini, A.; Ottani, A.; Sandrini, M. Dual acting anti-inflammatory drugs: A reappraisal. Pharmacol. Res. 2001, 44, 437–450. [Google Scholar] [CrossRef] [PubMed]
- Cariou, M.P.; Halfacree, Z.J.; Lee, K.C.; Baines, S.J. Successful surgical management of spontaneous gastric perforations in three cats. J. Feline Med. Surg. 2010, 12, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Bernardin, F.; Martinez Rivera, L.; Ragetly, G.; Gomes, E.; Hernandez, J. Spontaneous gastrointestinal perforation in cats: A retrospective study of 13 cases. J. Feline Med. Surg. 2015, 17, 873–879. [Google Scholar] [CrossRef]
- Prabhu, V.; Shivani, A. An overview of history, pathogenesis and treatment of perforated peptic ulcer disease with evaluation of prognostic scoring in adults. Ann. Med. Health Sci. Res. 2014, 39, 421–424. [Google Scholar] [CrossRef]
- Forsyt, S.F.; Guilford, W.G.; Haslett, S.J.; Godfrey, J. Endoscopy of the gastroduodenal mucosa after carprofen, meloxicam and ketoprofen administration in dogs. J. Small Anim. Pract. 1998, 39, 421–424. [Google Scholar] [CrossRef]
- Lascelles, B.D.; Blikslager, A.T.; Fox, S.M.; Reece, D. Gastrointestinal tract perforation in dogs treated with a selective cycloxygenase-2 inhibitor: 29 cases (2002–2003). J. Am. Vet. Med. Assoc. 2005, 227, 1112–1117. [Google Scholar] [CrossRef]
- Runk, A.; Kyles, A.E.; Downs, M.O. Duodenal perforation in a cat following the administration of nonsteroidal anti-inflammatory medication. J. Am. Anim. Hosp. Assoc. 1999, 35, 52–55. [Google Scholar] [CrossRef]
- Sostres, C.; Gargano, C.J.; Lanas, A. Nonsteroidal anti-inflammatory drugs and upper and lower gastrointestinal mucosal damage. Arthritis Res. Ther. 2013, 15 (Suppl. S3), S3. [Google Scholar] [CrossRef]
- Luna, S.P.; Basilio, A.C.; Steagall, P.V.; Machado, L.P.; Moutinho, F.Q.; Takahira, R.K.; Brandão, C.V. Evaluation of adverse effects of long-term oral administration of carprofen, etodolac, flunixin meglumine, ketoprofen, and meloxicam in dogs. Am. J. Vet. Res. 2007, 68, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Trevor, B.E.; Braun, L.D.; Kuzma, A.B. Gastrointestinal perforation in five dogs associated with the administration of meloxicam. J. Vet. Emerg. Crit. Care 2006, 16, 34–43. [Google Scholar]
- Wallace, J.L.; Vong, L. NSAID-induced gastrointestinal damage and the design of GI-sparing NSAIDs. Curr. Opin. Investig. Drugs 2008, 9, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Senello, K.A.; Leib, M.S. Effects of deracoxib or buffered aspirin on the gastric mucosa of healthy dogs. J. Vet. Intern. Med. 2006, 20, 1291–1296. [Google Scholar] [CrossRef]
- Goodman, L.; Torres, B.; Punke, J.; Reynolds, L.; Speas, A.; Ellis, A.; Budsberg, S. Effects of firocoxib and tepoxalin on healing in a canine gastric mucosal injury model. J. Vet. Intern. Med. 2009, 23, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Wooten, J.G.; Blikslager, A.T.; Marks, S.L.; Law, J.M.; Graeber, E.C.; Lascelles, B.D. Effect of nonsteroidal anti-inflammatory drugs with varied cycloxygenase-2 selectivity on cycloxygenase protein and prostanoid concentrations in pyloric and duodenal, mucosa of dogs. Am. J. Vet. Res. 2009, 70, 1243–1249. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pavone, G.; Castellucci, B.; Pavone, S.; Stefanetti, V.; Vitolo, C.; Mangiaterra, S. Unusual Case of Biliary Peritonitis in a Dog Secondary to a Gastric Perforation. Vet. Sci. 2023, 10, 384. https://doi.org/10.3390/vetsci10060384
Pavone G, Castellucci B, Pavone S, Stefanetti V, Vitolo C, Mangiaterra S. Unusual Case of Biliary Peritonitis in a Dog Secondary to a Gastric Perforation. Veterinary Sciences. 2023; 10(6):384. https://doi.org/10.3390/vetsci10060384
Chicago/Turabian StylePavone, Giovanni, Barbara Castellucci, Silvia Pavone, Valentina Stefanetti, Chiara Vitolo, and Sara Mangiaterra. 2023. "Unusual Case of Biliary Peritonitis in a Dog Secondary to a Gastric Perforation" Veterinary Sciences 10, no. 6: 384. https://doi.org/10.3390/vetsci10060384