
Whole-Slide Images and Patches of Clear Cell Renal Cell Carcinoma Tissue Sections Counterstained with Hoechst 33342, CD3, and CD8 Using Multiple Immunofluorescence



Abstract
:1. Summary
2. Data Description
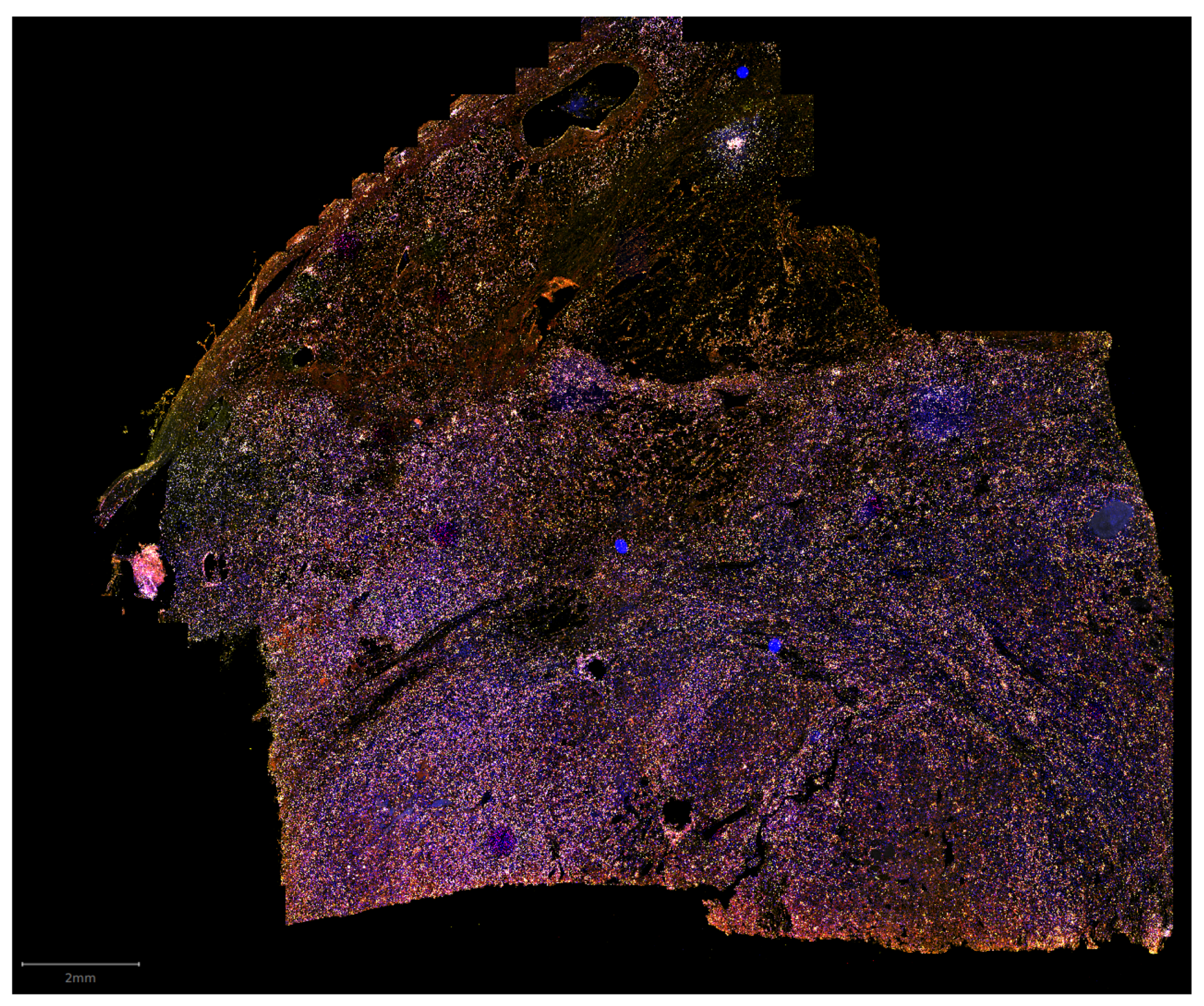
2.1. Raw Whole-Slide Images
2.2. Preprocessed Image Patches
| Listing 1. Structure of the JSON file accompanying each patch. |
{
"original_file": "ICAIRD1007_MCM2FITC_CD3CY3_CD8CY5_MCK750.czi",
"x": 51712,
"y": 51968,
"w": 256,
"h": 256,
"images": [
{
"file": "ICAIRD1007_MCM2FITC_CD3CY3_CD8CY5_MCK750 […].png",
"mode": "mask",
"channel": "CD3"
},
// …
]
}
2.3. Clinical Data
3. Methods
3.1. Multiplex Immunofluorescence Protocol
3.2. Whole-Slide Image Acquisition
3.3. Patch Processing
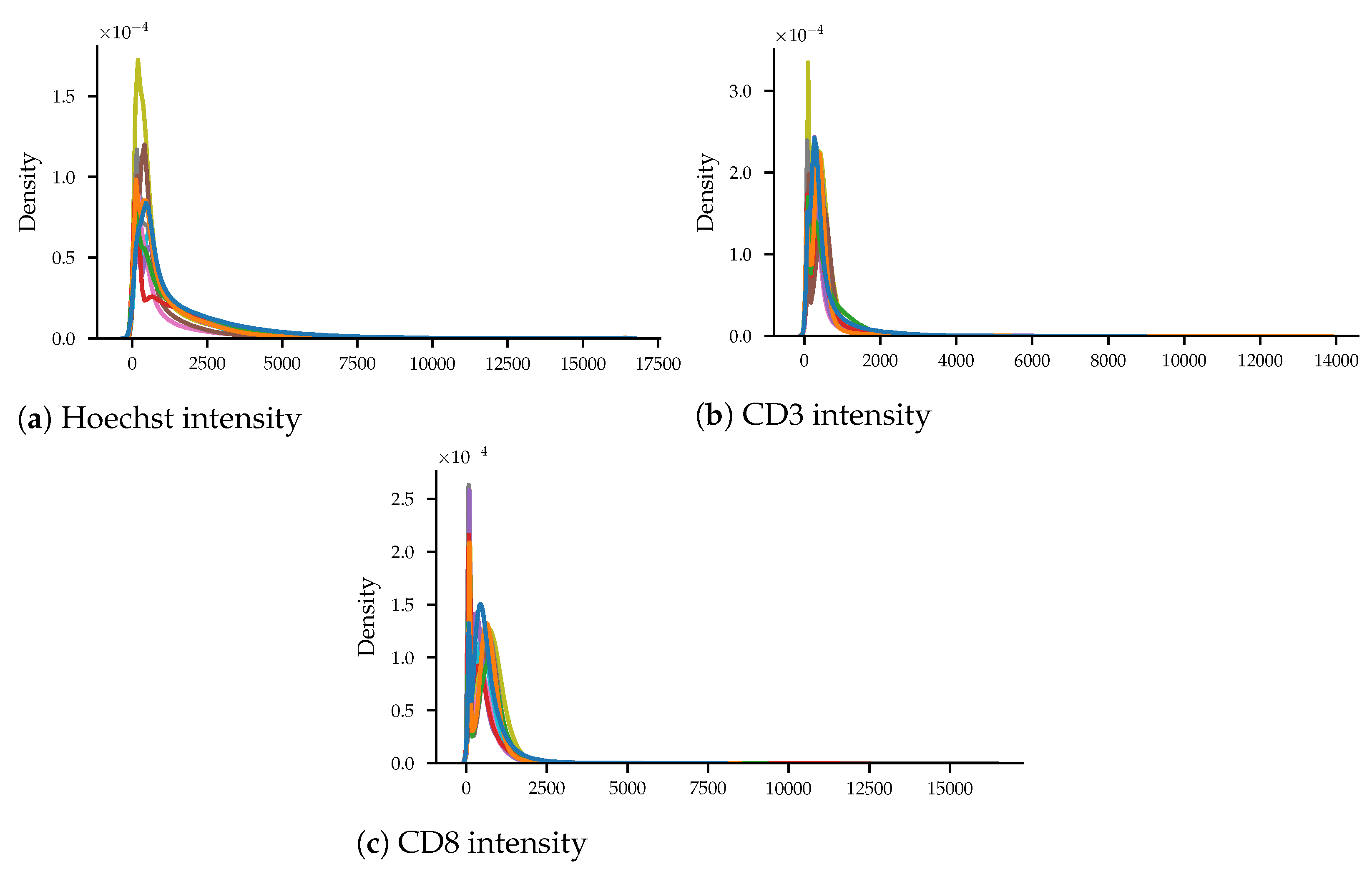
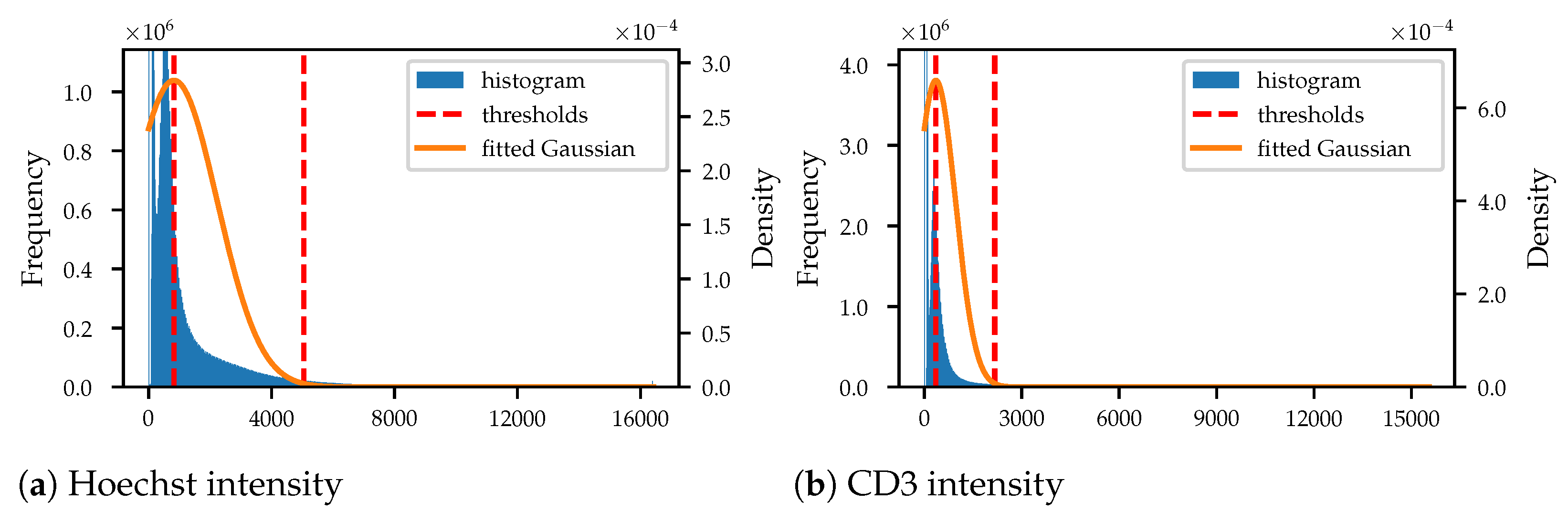
3.3.1. Intensity Normalisation
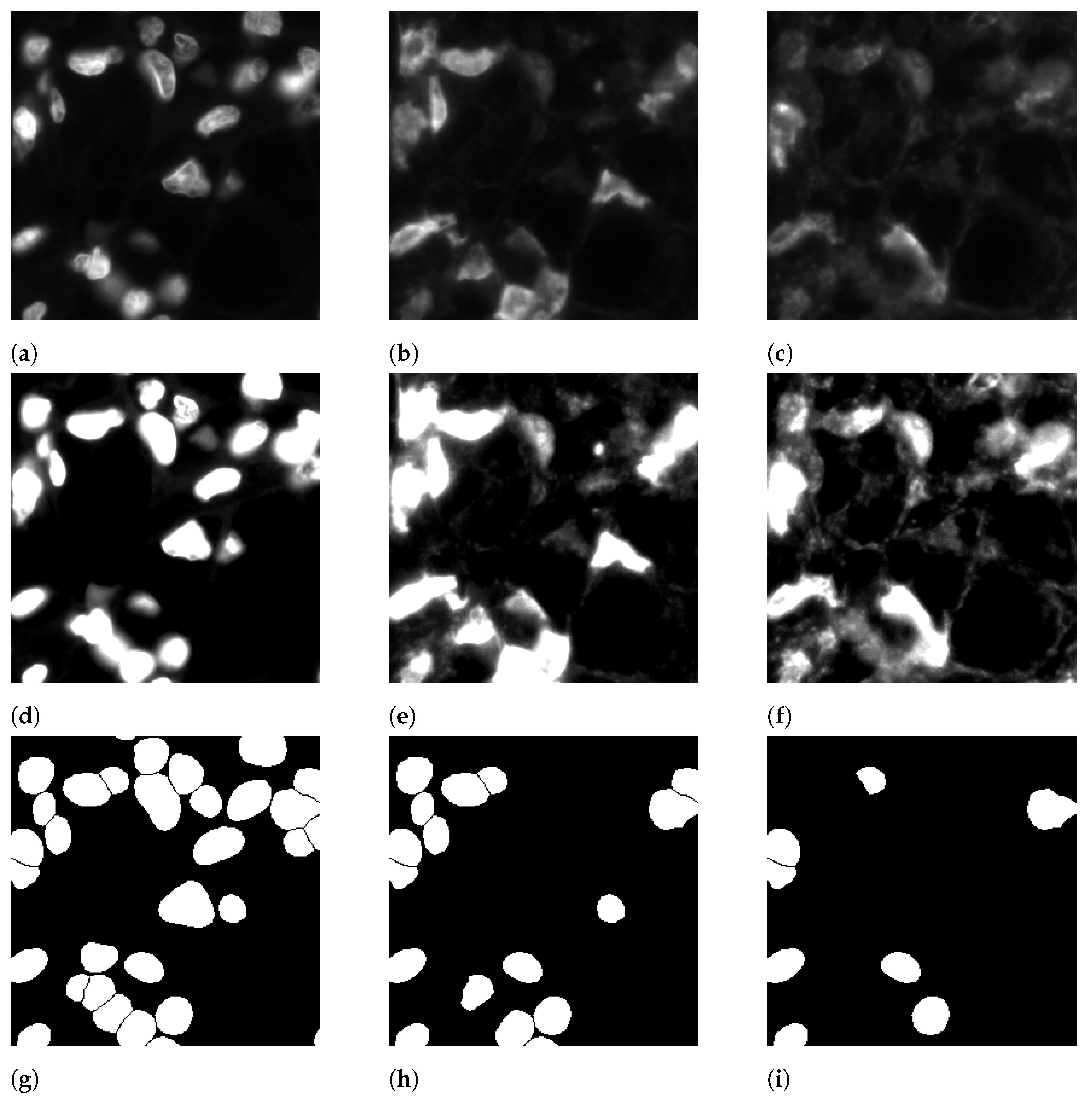
3.3.2. Nucleus Segmentation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ccRCC | clear cell renal cell carcinoma |
| TME | tumour microenvironment |
| mIF | multiplex immunofluorescence |
| IHC | immunohistochemistry |
| WSI | whole-slide image |
| GAN | generative adversarial network |
| CD3 | cluster of differentiation 3 |
| CD8 | cluster of differentiation 8 |
| TSA | tyramide signal amplification |
| HRP | horseradish peroxidase |
| JSON | JavaScript object notation |
| PNG | portable network graphics |
| CSV | comma-separated values |
References
- Cancer Research UK. Kidney Cancer Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/kidney-cancer (accessed on 30 September 2022).
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef]
- De Filippis, R.; Wölflein, G.; Um, I.H.; Caie, P.D.; Warren, S.; White, A.; Suen, E.; To, E.; Arandjelović, O.; Harrison, D.J. Use of high-plex data reveals novel insights into the tumour microenvironment of clear cell renal cell carcinoma. Cancers 2022, 14, 5387. [Google Scholar] [CrossRef] [PubMed]
- Coons, A.H.; Creech, H.J.; Jones, R.N.; Berliner, E. The Demonstration of Pneumococcal Antigen in Tissues by the Use of Fluorescent Antibody. J. Immunol. 1942, 45, 159–170. [Google Scholar] [CrossRef]
- Kalyuzhny, A.E. Immunohistochemistry—Essential Elements and Beyond; Springer: Berlin/Heidelberg, Germany, 2016. [Google Scholar]
- Goldstein, N.S.; Hewitt, S.M.; Taylor, C.R.; Yaziji, H.; Hicks, D.G.; Members of Ad-Hoc Committee on Immunohistochemistry Standardization. Recommendations for Improved Standardization of Immunohistochemistry. Appl. Immunohistochem. Mol. Morphol. 2007, 15, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, J.G. Immunofluorescence Staining. Curr. Protoc. Cell Biol. 2015, 69, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.U.; Enomoto, H.; Milbrandt, J.; Roth, K.A. Dual Fluorescent in Situ Hybridization and Immunohistochemical Detection with Tyramide Signal Amplification. J. Histochem. Cytochem. 2000, 48, 1369–1375. [Google Scholar] [CrossRef] [Green Version]
- Buchwalow, I.B.; Böcker, W. Immunohistochemistry: Basics and Methods; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2010. [Google Scholar]
- Chazotte, B. Labeling Nuclear DNA with Hoechst 33342. Cold Spring Harb. Protoc. 2011, 2011, pdb-prot5557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caie, P.D.; Dimitriou, N.; Arandjelović, O. Precision Medicine in Digital Pathology via Image Analysis and Machine Learning. In Artificial Intelligence and Deep Learning in Pathology; Elsevier: Amsterdam, The Netherlands, 2021; pp. 149–173. [Google Scholar]
- Kather, J.N.; Krisam, J.; Charoentong, P.; Luedde, T.; Herpel, E.; Weis, C.A.; Gaiser, T.; Marx, A.; Valous, N.A.; Ferber, D.; et al. Predicting survival from colorectal cancer histology slides using deep learning: A retrospective multicenter study. PLoS Med. 2019, 16, e1002730. [Google Scholar] [CrossRef] [PubMed]
- Yao, J.; Zhu, X.; Huang, J. Deep multi-instance learning for survival prediction from whole-slide images. In Proceedings of the Medical Image Computing and Computer Assisted Intervention–MICCAI 2019: 22nd International Conference, Shenzhen, China, 13–17 October 2019; Springer: Berlin/Heidelberg, Germany, 2019; pp. 496–504. [Google Scholar]
- Abousamra, S.; Gupta, R.; Hou, L.; Batiste, R.; Zhao, T.; Shankar, A.; Rao, A.; Chen, C.; Samaras, D.; Kurc, T.; et al. Deep learning-based mapping of tumor infiltrating lymphocytes in whole-slide images of 23 types of cancer. Front. Oncol. 2022, 11, 5971. [Google Scholar] [CrossRef] [PubMed]
- Cooper, J.; Um, I.H.; Arandjelović, O.; Harrison, D.J. Lymphocyte Classification from Hoechst Stained Slides with Deep Learning. Cancers 2022, 14, 5957. [Google Scholar] [CrossRef] [PubMed]
- Wölflein, G.; Um, I.H.; Harrison, D.J.; Arandjelović, O. HoechstGAN: Virtual Lymphocyte Staining Using Generative Adversarial Networks. In Proceedings of the IEEE/CVF Winter Conference on Applications of Computer Vision (WACV), Waikoloa, HI, USA, 2–8 January 2023; pp. 4997–5007. [Google Scholar]
- Warren, A.Y.; Harrison, D. WHO/ISUP classification, grading and pathological staging of renal cell carcinoma: Standards and controversies. World J. Urol. 2018, 36, 1913–1926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bektas, S.; Bahadir, B.; Kandemir, N.O.; Barut, F.; Gul, A.E.; Ozdamar, S.O. Intraobserver and interobserver variability of Fuhrman and modified Fuhrman grading systems for conventional renal cell carcinoma. Kaohsiung J. Med Sci. 2009, 25, 596–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulrane, L.; Rexhepaj, E.; Penney, S.; Callanan, J.J.; Gallagher, W.M. Automated image analysis in histopathology: A valuable tool in medical diagnostics. Expert Rev. Mol. Diagn. 2008, 8, 707–725. [Google Scholar] [CrossRef] [PubMed]
- Wölflein, G.; Um, I.H.; Harrison, D.J.; Arandjelović, O. Whole Slide Images and Patches of Clear Cell Renal Cell Carcinoma Counterstained with Multiple Immunofluorescence for Hoechst, CD3, and CD8. 2022. Available online: https://www.ebi.ac.uk/biostudies/bioimages/studies/S-BIAD605 (accessed on 6 February 2023).
- Goodfellow, I.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative Adversarial Nets. In Proceedings of the Advances in Neural Information Processing Systems; Ghahramani, Z., Welling, M., Cortes, C., Lawrence, N., Weinberger, K., Eds.; Curran Associates, Inc.: New York, NY, USA, 2014; Volume 27. [Google Scholar]
- Isola, P.; Zhu, J.Y.; Zhou, T.; Efros, A.A. Image-to-image translation with conditional adversarial networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1125–1134. [Google Scholar]
- Fuhrman, S.A.; Lasky, L.C.; Limas, C. Prognostic significance of morphologic parameters in renal cell carcinoma. Am. J. Surg. Pathol. 1982, 6, 655–663. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The eighth edition AJCC cancer staging manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Leibovich, B.C.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Frank, I.; Kwon, E.D.; Weaver, A.L.; Parker, A.S.; Zincke, H. Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: A stratification tool for prospective clinical trials. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2003, 97, 1663–1671. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, U.; Weigert, M.; Broaddus, C.; Myers, G. Cell Detection with Star-Convex Polygons. In Proceedings of the Medical Image Computing and Computer Assisted Intervention—MICCAI 2018—21st International Conference, Granada, Spain, 6–20 September 2018; pp. 265–273. [Google Scholar]
- He, K.; Gkioxari, G.; Dollár, P.; Girshick, R. Mask r-cnn. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 2961–2969. [Google Scholar]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mode | Channel | Description |
|---|---|---|
| raw | H3342 | normalised Hoechst patch |
| raw | Cy3 | normalised CD3 patch |
| raw | Cy5 | normalised CD8 patch |
| mask | Hoechst | segmentation mask of all detected cells |
| mask | CD3 | segmentation mask of CD3+ cells (subset of Hoechst cells) |
| mask | CD8 | segmentation mask of CD8+ cells (subset of CD3+ cells) |
| mask | unclassified | segmentation mask of CD3- cells (subset of Hoechst cells) |
| Hoechst | CD3 | CD8 | |
|---|---|---|---|
| Total cells | 15,956,049 | 3,390,533 | 1,894,016 |
| Cells per patch | 25.42 | 5.40 | 3.02 |
| Presence | 99.95% | 93.08% | 71.61% |
| Area coverage | 26.48% | 05.01% | 03.02% |
| Column Name | Format | Description |
|---|---|---|
| ICAIRD number | ICAIRD_XXX | patient ID |
| Gender | M or F | gender |
| Response | 0 or 1 | recurrence within 5 years after surgery |
| Age at surgery | whole number | age at surgery in years |
| Disease-free months | float | number of months with no recurrence |
| Fuhrman nuclear grade | 1 – 4 | Fuhrman grade [24] |
| ISUP nuclear grade | 1 – 4 | ISUP grade [3] |
| Tumour stage | 1a, 1b, 2a, 2b, 3a, 3b, 3c, or 4 | tumour size according to TNM system [25] |
| Tumour size | float | tumour size in cm |
| Node status | 0 or 1 | lymph node status according to TNM system [25] |
| Necrosis | 0 or 1 | whether necrosis is detected |
| Leibovich score (Fuhrman) | 0 – 11 | Leibovich score [26] using Fuhrman nuclear grade [24] |
| Leibovich score (ISUP) | 0 – 11 | Leibovich score [26] using ISUP nuclear grade [3] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wölflein, G.; Um, I.H.; Harrison, D.J.; Arandjelović, O. Whole-Slide Images and Patches of Clear Cell Renal Cell Carcinoma Tissue Sections Counterstained with Hoechst 33342, CD3, and CD8 Using Multiple Immunofluorescence. Data 2023, 8, 40. https://doi.org/10.3390/data8020040
Wölflein G, Um IH, Harrison DJ, Arandjelović O. Whole-Slide Images and Patches of Clear Cell Renal Cell Carcinoma Tissue Sections Counterstained with Hoechst 33342, CD3, and CD8 Using Multiple Immunofluorescence. Data. 2023; 8(2):40. https://doi.org/10.3390/data8020040
Chicago/Turabian StyleWölflein, Georg, In Hwa Um, David J. Harrison, and Ognjen Arandjelović. 2023. "Whole-Slide Images and Patches of Clear Cell Renal Cell Carcinoma Tissue Sections Counterstained with Hoechst 33342, CD3, and CD8 Using Multiple Immunofluorescence" Data 8, no. 2: 40. https://doi.org/10.3390/data8020040