


Sleep-Disordered Breathing and Its Association with Nocturnal Enuresis at the Primary Schools in Saudi Arabia: A Cross-Sectional Study

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Setting and Participants
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Sample Size and Sampling
2.6. Data Collection Tools and Processes
2.7. Statistical Analysis
2.8. Ethical Consideration
3. Results
4. Discussion
4.1. Association between NE and SDB
4.2. Prevalence of NE
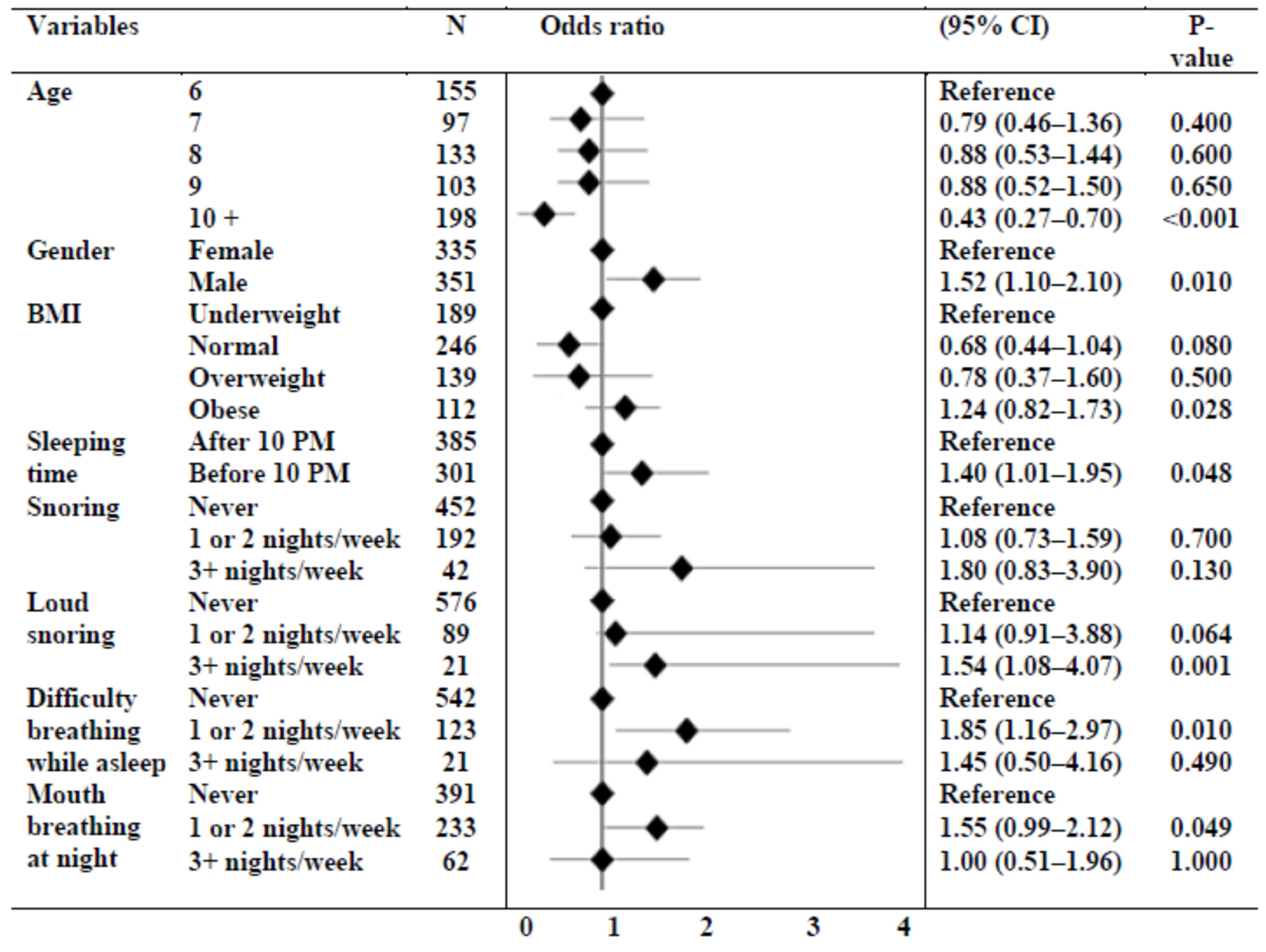
4.3. Risk Factors for NE
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADH | Antidiuretic hormone |
| AHI | Apnea hypopnea index |
| ANP | Atrial natriuretic peptide |
| BMI | Body mass index |
| CI | Confidence interval |
| DSM | Diagnostic and Statistical Manual |
| ICD | International Classification of Diseases |
| NE | Nocturnal enuresis |
| OR | Odds ratio |
| OSA | Obstructive sleep apnea |
| OSAHS | Obstructive sleep apnea–hypopnea syndrome |
| SDB | Sleep-disordered breathing |
| SRBD | Sleep-related breathing disorder |
References
- Gallai, B.; Esposito, M.; Parisi, L.; Roccella, M.; Marotta, R.; Lavano, S.M.; Mazzotta, G.; Carotenuto, M. Primary nocturnal enuresis as a risk factor for sleep disorders: An observational questionnaire-based multicenter study. Neuropsychiatr. Dis. Treat. 2013, 9, 437–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alhifthy, E.; Alghadeer, H.; Aljubran, T.; Alsahaf, H.; Alherz, S.; Ali, M.; Hewishel, A. Prevalence of nocturnal enuresis among children in eastern region in Saudi Arabia. Med. Sci. 2021, 25, 67–75. Available online: https://www.discoveryjournals.org/medicalscience/current_issue/v25/n107/A8.pdf (accessed on 30 April 2023).
- Tsuji, S.; Takewa, R.; Ohnuma, C.; Kimata, T.; Yamanouchi, S.; Kaneko, K. Nocturnal enuresis and poor sleep quality. Pediatr. Int. 2018, 60, 1020–1023. [Google Scholar] [CrossRef] [Green Version]
- Li, H.Y.; Lee, L.A. Sleep-disordered breathing in children. Chang Gung Med. J. 2009, 32, 247–257. [Google Scholar]
- Kaditis, A.; Kheirandish-Gozal, L.; Gozal, D. Algorithm for the diagnosis and treatment of pediatric OSA: A proposal of two pediatric sleep centers. Sleep Med. 2012, 13, 217–227. [Google Scholar] [CrossRef]
- Alexopoulos, E.; Malakasioti, G.; Varlami, V.; Miligkos, M.; Gourgoulianis, K.; Kaditis, A.G. Nocturnal enuresis is associated with moderate-to-severe obstructive sleep apnea in children with snoring. Pediatr. Res. 2014, 76, 555–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gu, Y.-M.; Kwon, J.E.; Lee, G.; Lee, S.J.; Suh, H.R.; Min, S.; Roh, D.E.; Jo, T.K.; Baek, H.S.; Hong, S.J.; et al. Sleep Problems and Daytime Sleepiness in Children with Nocturnal Enuresis. Child. Kidney Dis. 2016, 20, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Berry, R.B.; Kouchi, K.G.; Der, D.E.; Dickel, M.J.; Light, R.W. Sleep Apnea Impairs the Arousal Response to Airway Occlusion. Chest 1996, 109, 1490–1496. [Google Scholar] [CrossRef]
- Brooks, L.J.; Topol, H.I. Enuresis in children with sleep apnea. J. Pediatr. 2003, 142, 515–518. [Google Scholar] [CrossRef] [Green Version]
- Su, M.S.; Li, A.M.; So, H.K.; Au, C.T.; Ho, C.; Wing, Y.K. Nocturnal Enuresis in Children: Prevalence, Correlates, and Relationship with Obstructive Sleep Apnea. J. Pediatr. 2011, 159, 238–242.e1. [Google Scholar] [CrossRef]
- Zaffanello, M.; Piacentini, G.; Lippi, G.; Fanos, V.; Gasperi, E.; Nosetti, L. Obstructive sleep-disordered breathing, enuresis and combined disorders in children: Chance or related association? Swiss Med. Wkly. 2017, 147, w14400. [Google Scholar] [CrossRef]
- Gomez Rincon, M.; Leslie, S.W.; Lotfollahzadeh, S. Nocturnal Enuresis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK545181/ (accessed on 3 June 2023).
- Csábi, E.; Gaál, V.; Hallgató, E.; Schulcz, R.A.; Katona, G.; Benedek, P. Increased behavioral problems in children with sleep-disordered breathing. Ital. J. Pediatr. 2022, 48, 173. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Pakhare, A.; Bhatt, G.; Choudhary, B.; Patil, R. Association of pediatric obstructive sleep apnea with poor academic performance: A school-based study from India. Lung India 2018, 35, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Sakellaropoulou, A.V.; Hatzistilianou, M.N.; Emporiadou, M.N.; Aivazis, V.T.; Goudakos, J.; Markou, K.; Athanasiadou-Piperopoulou, F. Association between primary nocturnal enuresis and habitual snoring in children with obstructive sleep apnoea-hypopnoea syndrome. Arch. Med. Sci. 2012, 3, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Alexopoulos, E.I.; Kostadima, E.; Pagonari, I.; Zintzaras, E.; Gourgoulianis, K.; Kaditis, A.G. Association between primary nocturnal enuresis and habitual snoring in children. Urology 2006, 68, 406–409. [Google Scholar] [CrossRef]
- Goodwin, J.L.; Kaemingk, K.L.; Fregosi, R.F.; Rosen, G.M.; Morgan, W.J.; Smith, T.; Quan, S.F. Parasomnias and sleep disordered breathing in Caucasian and Hispanic children—The Tucson children’s assessment of sleep apnea study. BMC Med. 2004, 2, 14. [Google Scholar] [CrossRef] [Green Version]
- Ezzat, W.; Fawaz, S.; Farid, S. Impact of sleep-disordered breathing and its treatment on children with primary nocturnal enuresis. Swiss Med. Wkly. 2011, 141, w13216. [Google Scholar] [CrossRef]
- Shafiek, H.; Evangelisti, M.; Abd-Elwahab, N.H.; Barreto, M.; Villa, M.P.; Mahmoud, M.I. Obstructive Sleep Apnea in School-Aged Children Presented with Nocturnal Enuresis. Lung 2020, 198, 187–194. [Google Scholar] [CrossRef]
- Kalo, B.B.; Bella, H. Enuresis: Prevalence and associated factors among primary school children in Saudi Arabia. Acta Paediatr. 1996, 85, 1217–1222. [Google Scholar] [CrossRef]
- Alwadei, S.H.; Alsaeed, S.; Masoud, A.I.; Alwadei, F.; Gufran, K.; Alwadei, A. Sleep-Disordered Breathing among Saudi Primary School Children: Incidence and Risk Factors. Healthcare 2023, 11, 747. [Google Scholar] [CrossRef]
- Wada, H.; Kimura, M.; Tajima, T.; Shirahama, R.; Suzuki, Y.; Suzuki, Y.; Hayashi, T.; Maruyama, K.; Endo, M.; Sakamoto, N.; et al. Nocturnal enuresis and sleep disordered breathing in primary school children: Potential implications. Pediatr. Pulmonol. 2018, 53, 1541–1548. [Google Scholar] [CrossRef] [PubMed]
- Ersu, R.; Arman, A.R.; Save, D.; Karadag, B.; Karakoc, F.; Berkem, M.; Dagli, E. Prevalence of Snoring and Symptoms of Sleep-Disordered Breathing in Primary School Children in Istanbul. Chest 2004, 126, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Zrubavel, V.; Kushnir, B.; Kushnir, J.; Sadeh, A. Sleep and Sleepiness in Children with Nocturnal Enuresis. Sleep 2011, 34, 191–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherah, K.; ElSharief, M.; Barkat, N.; Jafery, A. Prevalence of Nocturnal Enuresis in school-age children in Saudi Arabia. Int. J. Med. Dev. Ctries. 2019, 3, 669–675. [Google Scholar] [CrossRef]
- Alshahrani, A.; Selim, M.; Abbas, M. Prevalence of nocturnal enuresis among children in Primary Health Care Centers of Family and Community Medicine, PSMMC, Riyadh City, KSA. J. Fam. Med. Prim. Care 2018, 7, 937–941. [Google Scholar] [CrossRef]
- Gümüs, B.; Vurgun, N.; Lekili, M.; Iscan, A.; Müezzinoğlu, T.; Büyüksu, C. Prevalence of nocturnal enuresis and accompanying factors in children aged 7-11 years in Turkey. Acta Paediatr. 1999, 88, 1369–1372. [Google Scholar] [CrossRef]
- Ferrara, P.; Franceschini, G.; Di Castelbianco, F.B.; Bombace, R.; Villani, A.; Corsello, G. Epidemiology of enuresis: A large number of children at risk of low regard. Ital. J. Pediatr. 2020, 46, 128. [Google Scholar] [CrossRef]
- Hansakunachai, T.; Ruangdaraganon, N.; Udomsubpayakul, U.; Sombuntham, T.; Kotchabhakdi, N. Epidemiology of Enuresis Among School-Age Children in Thailand. J. Dev. Behav. Pediatr. 2005, 26, 356–360. [Google Scholar] [CrossRef]
- Makrani, A.H.; Moosazadeh, M.; Nasehi, M.; Abedi, G.; Afshari, M.; Farshidi, F.; Aghaei, S. Prevalence of Enuresis and its related factors among children in Iran: A systematic review and meta-analysis. Int. J. Pediatr. 2015, 3, 995–1004. [Google Scholar] [CrossRef]
- Birdal, S.; Dogangun, B. Behavioural problems in children with enuresis. Turk. Pediatri. Ars. 2016, 51, 142–147. [Google Scholar] [CrossRef] [Green Version]
- Bakhtiar, K.; Pournia, Y.; Ebrahimzadeh, F.; Farhadi, A.; Shafizadeh, F.; Hosseinabadi, R. Prevalence of Nocturnal Enuresis and Its Associated Factors in Primary School and Preschool Children of Khorramabad in 2013. Int. J. Pediatr. 2014, 2014, 120686. [Google Scholar] [CrossRef] [Green Version]
- Mohammed, A.H.; Saleh, A.G.; Al Zoheiry, I. Frequency of bedwetting among primary school children in Benha city, Egypt. Egypt. J. Med. Hum. Genet. 2014, 15, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Alhifthy, E.H.; Habib, L.; Abu Al-Makarem, A.; AlGhamdi, M.; Alsultan, D.; Aldhamer, F.; Buhlagah, R.; Almubarak, F.M.; Almufadhi, E.; Bukhamsin, G.M.; et al. Prevalence of Nocturnal Enuresis among Saudi Children Population. Cureus 2020, 12, e6662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nørgaard, J.P. Pathophysiology of nocturnal enuresis. Scand. J. Urol. Nephrol. Suppl. 1991, 140, 1–35. [Google Scholar] [PubMed]
- von Gontard, A.; Schaumburg, H.; Hollmann, E.; Eiberg, H.; Rittig, S. The genetics of enuresis: A review. J. Urol. 2001, 166, 2438–2443. [Google Scholar] [CrossRef] [PubMed]
- Mammen, A.A.; Ferrer, A.F. Nocturnal enuresis: Medical management. Urol. Clin. N. Am. 2004, 31, 491–498. [Google Scholar] [CrossRef]
- Dang, J.; Tang, Z. Pathogenesis and brain functional imaging in nocturnal enuresis: A review. Exp. Biol. Med. 2021, 246, 1483–1490. [Google Scholar] [CrossRef]
- Lei, D.; Ma, J.; Shen, X.; Du, X.; Shen, G.; Liu, W.; Yan, X.; Li, G. Changes in the Brain Microstructure of Children with Primary Monosymptomatic Nocturnal Enuresis: A Diffusion Tensor Imaging Study. PLoS ONE 2012, 7, e31023. [Google Scholar] [CrossRef] [Green Version]
- Altunoluk, B.; Davutoglu, M.; Garipardic, M.; Bakan, V. Decreased Vitamin B12Levels in Children with Nocturnal Enuresis. ISRN Urol. 2012, 2012, 789706. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.; Masruha, M.R.; Peres, M.F.P.; Minett, T.S.C.; Vitalle, M.S.D.S.; Scerni, D.A.; Vilanova, L.C.P. Nocturnal Enuresis Antecedent Is Common in Adolescents with Migraine. Eur. Neurol. 2012, 67, 354–359. [Google Scholar] [CrossRef]
- Nikibakhsh, A.; Mahmoodzadeh, H.; Ghareaghaji, R.R.; Poostindooz, H.; Karamyyar, M.; Sepehrvand, N. Is there any correlation between hypercalciuria and nocturnal enuresis? Indian J. Nephrol. 2012, 22, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Backhaus, M.; Agulló, E.M.; Guzmán, S.A.; Pérez, L.G.; Oliva, F.D.; García, R.M.; Cruz, J.F.J. Prevalence of nocturnal enuresis in the Valencian Community. Pediatric section of the National Incontinence Survey. The EPICC Study. Acta Urol. Esp. 2009, 33, 1011–1018. [Google Scholar] [CrossRef] [Green Version]
- Tai, H.-L.; Chang, Y.-J.; Chang, S.C.-C.; Chen, G.-D.; Chang, C.-P.; Chou, M.-C. The epidemiology and factors associated with nocturnal enuresis and its severity in primary school children in Taiwan. Acta Paediatr. 2007, 96, 242–245. [Google Scholar] [CrossRef]
- Schroeder, M.K.; Juul, K.V.; Mahler, B.; Nørgaard, J.P.; Rittig, S. Desmopressin use in pediatric nocturnal enuresis patients: Is there a sex difference in prescription patterns? Eur. J. Pediatr. 2017, 177, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Molinari, L.; von Siebenthal, K.; Wolfensberger, U.; Largo, R.H. Development of bladder and bowel control: Significance of prematurity, perinatal risk factors, psychomotor development and gender. Eur. J. Pediatr. 1999, 158, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Sun, Z.; Uchiyama, M.; Li, Y.; Okawa, M. Attaining Nocturnal Urinary Control, Nocturnal Enuresis, and Behavioral Problems in Chinese Children Aged 6 Through 16 Years. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 1557–1564. [Google Scholar] [CrossRef] [PubMed]
- Piyasil, V.; Udomsup, J. Enuresis in children 5-15 years at Queen Sirikit National Institute of Child Health. J. Med. Assoc. Thail. 2002, 85, 11–16. [Google Scholar]
- Serel, T.A.; Akhan, G.; Koyuncuoğlu, H.R.; Öztürk, A.; Doğruer, K.; Ünal, S.; Çelik, K. Epidemiology of Enuresis in Turkish Children. Scand. J. Urol. Nephrol. 1997, 31, 537–539. [Google Scholar] [CrossRef]
- Ghotbi, N.; Kheirabadi, G. Prevalence of nocturia and its associated factors in primary school children in Sanandaj in 2002. J. Kurd. Univ. Med. Sci. 2001, 5, 30–33. [Google Scholar]
- Yousef, K.A.; Basaleem, H.O.; Bin Yahiya, M.T. Epidemiology of nocturnal enuresis in basic schoolchildren in Aden Governorate, Yemen. Saudi J. Kidney Dis. Transplant. 2011, 22, 167–173. [Google Scholar]
- Gunes, A.; Gunes, G.; Acik, Y.; Akilli, A. The epidemiology and factors associated with nocturnal enuresis among boarding and daytime school children in southeast of Turkey: A cross sectional study. BMC Public Health 2009, 9, 357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cher, T.-W.; Lin, G.-J.; Hsu, K.-H. Prevalence of Nocturnal Enuresis and Associated Familial Factors in Primary School Children in Taiwan. J. Urol. 2002, 168, 1142–1146. [Google Scholar] [CrossRef] [PubMed]
- van Hoecke, E.; Baeyens, D.; Walle, J.V.; Hoebeke, P.; Roeyers, H. Socioeconomic Status as a Common Factor Underlying the Association Between Enuresis and Psychopathology. J. Dev. Behav. Pediatr. 2003, 24, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Weintraub, Y.; Singer, S.; Alexander, D.; Hacham, S.; Menuchin, G.; Lubetzky, R.; Steinberg, D.M.; Pinhas-Hamiel, O. Enuresis—An unattended comorbidity of childhood obesity. Int. J. Obes. 2012, 37, 75–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erdem, E.; Lin, A.; Kogan, B.A.; Feustel, P. Association of elimination dysfunction and body mass index. J. Pediatr. Urol. 2006, 2, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Shen, Y.; Liu, X. Association between enuresis and obesity in children with primary monosymptomatic nocturnal enuresis. Int. Braz. J. Urol. 2019, 45, 790–797. [Google Scholar] [CrossRef]
- Chang, S.-J.; Chiang, I.-N.; Lin, C.-D.; Hsieh, C.-H.; Yang, S.S.-D. Obese children at higher risk for having overactive bladder symptoms: A community-based study. Neurourol. Urodyn. 2015, 34, 123–127. [Google Scholar] [CrossRef]
- Zahra, S.S. A prospective longitudinal study to estimate the prevalence of obesity in Egyptian children with nocturnal enuresis and the association between body mass index and response to therapy. Egypt. J. Med. Hum. Genet. 2017, 18, 211–218. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Variables | n = 686 (%) | |
|---|---|---|
| Age (years) | 6 | 155 (22.6) |
| 7 | 97 (14.1) | |
| 8 | 133 (19.4) | |
| 9 | 103 (15.0) | |
| 10+ | 198 (28.9) | |
| Gender | Female | 335 (48.8) |
| Male | 351 (51.2) | |
| Relation | Mother | 519 (75.7) |
| Father | 151 (22.0) | |
| Guardian | 16 (2.3) | |
| Region | Western | 226 (32.9) |
| Central | 205 (29.9) | |
| Eastern | 103 (15.0) | |
| Southern | 99 (14.4) | |
| Northern | 53 (7.7) | |
| Average parental education level | Illiterate | 7 (1.0) |
| Primary school | 40 (5.8) | |
| High school | 198 (28.9) | |
| Bachelor’s degree | 396 (57.7) | |
| Postgraduate degree | 45 (6.6) | |
| Weight (kg) | 28.5 ± 14.6 | |
| Height (cm) | 122.0 ± 24.0 | |
| BMI (kg/m2) | 20.0 ± 8.2 | |
| BMI category | Underweight (<18.5) | 189 (27.6) |
| Normal (18.5–24.9) | 246 (35.9) | |
| Overweight (25–29.9) | 139 (20.2) | |
| Obese (>30) | 112 (16.3) | |
| Comorbidities 1 | None | 529 (77.1) |
| Asthma | 111 (16.2) | |
| Adenotonsillar hypertrophy | 107 (15.6) | |
| Other pulmonary disorders | 55 (8.0) | |
| Psychological disorders | 33 (4.8) | |
| Cardiac disorders | 24 (3.5) | |
| Other | 13 (1.9) | |
| Nocturnal enuresis | 153 (22.3) | |
| Frequency of nocturnal enuresis | <2 times/week | 97 (63.4) |
| 2+ times/week | 56 (36.6) | |
| Duration of nocturnal enuresis | <3 months | 82 (53.6) |
| 3+ months | 71 (46.4) | |
| Sociodemographic Characteristics | Nocturnal Enuresis | p-Value | ||
|---|---|---|---|---|
| Yes n = 153 (%) | No n = 533 (%) | |||
| Age (years) | 6 | 39 (25.2) | 116 (74.8) | 0.020 * |
| 7 | 22 (22.7) | 75 (77.3) | ||
| 8 | 35 (26.3) | 98 (73.7) | ||
| 9 | 29 (28.2) | 74 (71.8) | ||
| 10+ | 28 (14.1) | 170 (85.9) | ||
| Gender | Female | 63 (18.8) | 272 (81.2) | 0.035 * |
| Male | 90 (25.6) | 261 (74.4) | ||
| Region | Western | 51 (22.6) | 175 (77.4) | 0.097 |
| Central | 45 (22.0) | 160 (78.0) | ||
| Eastern | 30 (29.1) | 73 (70.9) | ||
| Southern | 22 (22.2) | 77 (77.8) | ||
| Northern | 5 (9.4) | 48 (90.6) | ||
| Average parental education level | Illiterate | 2 (28.6) | 5 (71.4) | 0.414 |
| Primary school | 10 (25.0) | 30 (75.0) | ||
| High school | 41 (20.7) | 157 (79.3) | ||
| Bachelor’s degree | 85 (21.5) | 311 (78.5) | ||
| Postgraduate degree | 15 (33.3) | 30 (66.7) | ||
| Weight (kg) | 26.4 ± 13.2 | 30.2 ± 15.5 | 0.006 * | |
| Height (cm) | 121.0 ± 22.1 | 124.0 ± 25.3 | 0.184 | |
| BMI (kg/m2) | 19.2 ± 8.0 | 20.8 ± 8.2 | 0.033 * | |
| BMI category | Underweight | 31 (16.4) | 158 (83.6) | <0.001 * |
| Normal | 48 (19.5) | 198 (80.5) | ||
| Overweight | 29 (20.9) | 110 (79.1) | ||
| Obese | 45 (40.2) | 67 (59.8) | ||
| Sleep-Related Characteristics | Total n = 686 (%) | Nocturnal Enuresis | p-Value | ||
|---|---|---|---|---|---|
| Yes n = 153 (%) | No n = 533 (%) | ||||
| Sleep duration | >9 h | 276 (40.2) | 64 (44.6) | 212 (55.4) | 0.708 |
| 9 h or less | 410 (59.8) | 89 (41.7) | 321 (58.3) | ||
| Sleeping time | After 10 PM | 385 (56.1) | 73 (19.0) | 312 (81.0) | 0.021 * |
| Before 10 PM | 301 (43.9) | 80 (26.6) | 221(73.4) | ||
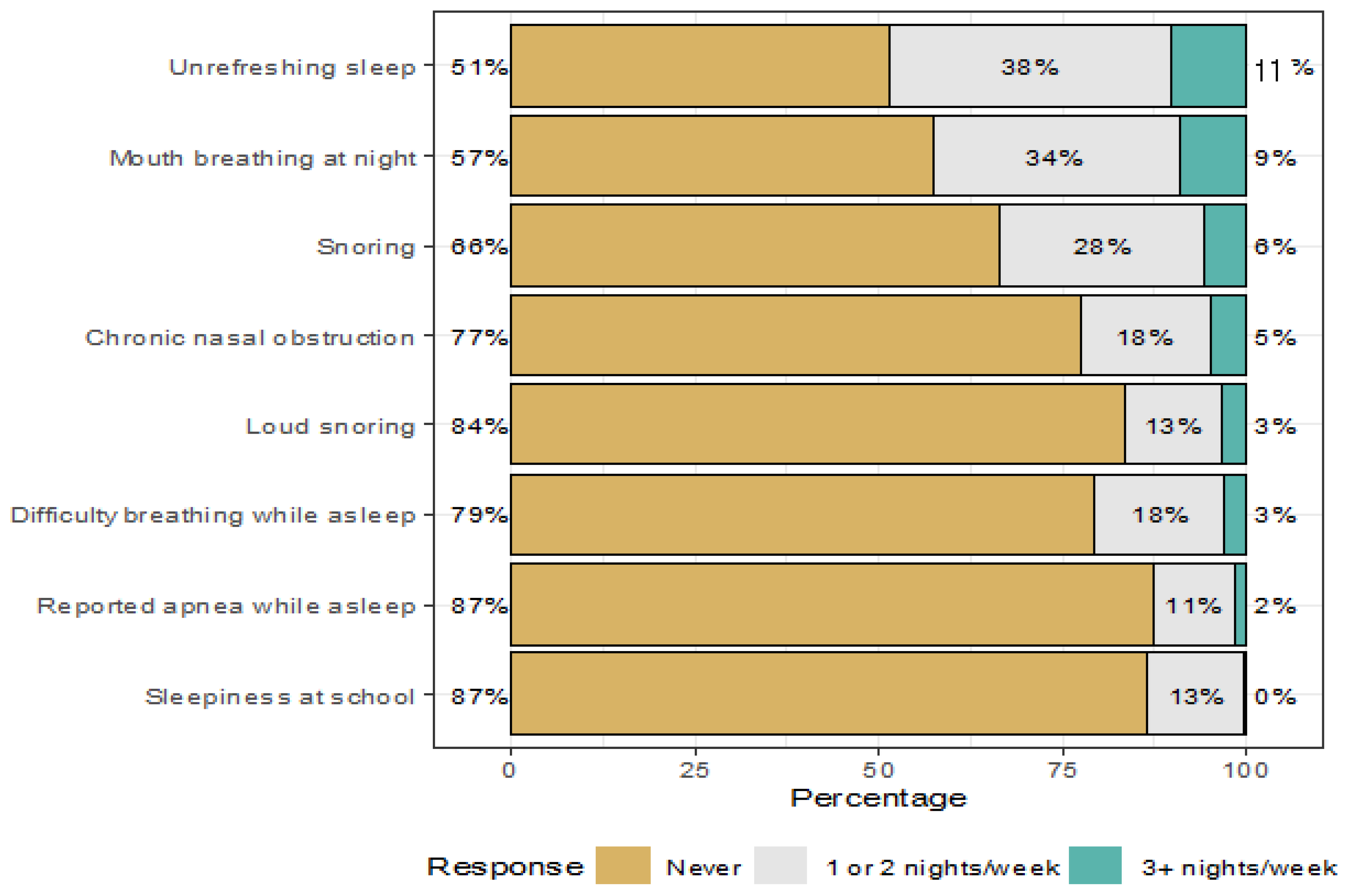
| Snoring | Never | 452 (66.0) | 117 (25.9) | 335 (74.1) | 0.001 * |
| 1 or 2 nights/week | 192 (28.0) | 24 (12.5) | 168 (87.5) | ||
| 3+ nights/week | 42 (6.0) | 12 (28.6) | 30 (71.4) | ||
| Loud snoring | Never | 576 (84.0) | 89 (15.5) | 487 (84.5) | <0.001 * |
| 1 or 2 nights/week | 89 (13.0) | 52 (58.4) | 37 (41.6) | ||
| 3+ nights/week | 21 (3.0) | 12 (57.1) | 9 (42.9) | ||
| Unrefreshing sleep | Never | 350 (51.0) | 75 (21.4) | 275 (78.6) | 0.780 |
| 1 or 2 nights/week | 260 (38.0) | 59 (22.7) | 201 (77.3) | ||
| 3+ nights/week | 76 (11.0) | 19 (25.0) | 57 (75.0) | ||
| Reported apnea while asleep | Never | 597 (87.0) | 128 (21.4) | 469 (78.6) | 0.372 |
| 1 or 2 nights/week | 75 (11.0) | 21 (28.0) | 54 (72.0) | ||
| 3+ nights/week | 14 (2.0) | 4 (28.6) | 10 (71.4) | ||
| Difficulty breathing while asleep | Never | 542 (79.0) | 83 (15.3) | 459 (84.7) | <0.001 * |
| 1 or 2 nights/week | 123 (18.0) | 63 (51.2) | 60 (48.8) | ||
| 3+ nights/week | 21 (3.0) | 7 (33.3) | 14 (66.7) | ||
| Sleepiness at school | Never | 597 (87.0) | 129 (21.6) | 468 (78.4) | 0.275 |
| 1 or 2 nights/week | 89 (13.0) | 24 (27.0) | 65 (73.0) | ||
| 3+ nights/week | 0 (0.0) | 0 (0.0) | 0 (0.0) | ||
| Mouth breathing at night | Never | 391 (57.0) | 70 (17.9) | 321 (82.1) | 0.005 * |
| 1 or 2 nights/week | 233 (34.0) | 64 (27.5) | 169 (72.5) | ||
| 3+ nights/week | 62 (9.0) | 19 (30.6) | 43 (69.4) | ||
| Chronic nasal obstruction | Never | 528 (77.0) | 113 (21.4) | 415 (78.6) | 0.540 |
| 1 or 2 nights/week | 123 (18.0) | 32 (26.0) | 91 (74.0) | ||
| 3+ nights/week | 35 (5.0) | 8 (22.9) | 27 (77.1) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshehri, A.A.; Zaki, M.S.H.; Nour, S.O.; Gadi, W.H.; Zogel, B.A.; Alfaifi, S.M.; Masmali, E.M.; Aburasain, A.B.; Nour, M.O. Sleep-Disordered Breathing and Its Association with Nocturnal Enuresis at the Primary Schools in Saudi Arabia: A Cross-Sectional Study. Children 2023, 10, 1074. https://doi.org/10.3390/children10061074
Alshehri AA, Zaki MSH, Nour SO, Gadi WH, Zogel BA, Alfaifi SM, Masmali EM, Aburasain AB, Nour MO. Sleep-Disordered Breathing and Its Association with Nocturnal Enuresis at the Primary Schools in Saudi Arabia: A Cross-Sectional Study. Children. 2023; 10(6):1074. https://doi.org/10.3390/children10061074
Chicago/Turabian StyleAlshehri, Ali Abdullah, Mohamed Soliman Hassan Zaki, Sameh Osama Nour, Wala H. Gadi, Basem A. Zogel, Samar M. Alfaifi, Enas M. Masmali, Amani B. Aburasain, and Mohamed Osama Nour. 2023. "Sleep-Disordered Breathing and Its Association with Nocturnal Enuresis at the Primary Schools in Saudi Arabia: A Cross-Sectional Study" Children 10, no. 6: 1074. https://doi.org/10.3390/children10061074