

Clinical Application of Pediatric Sleep Endoscopy: An International Survey

 , , ,
, , ,  , , , , ,
, , , , ,  ,
,
Abstract
:1. Introduction
- –
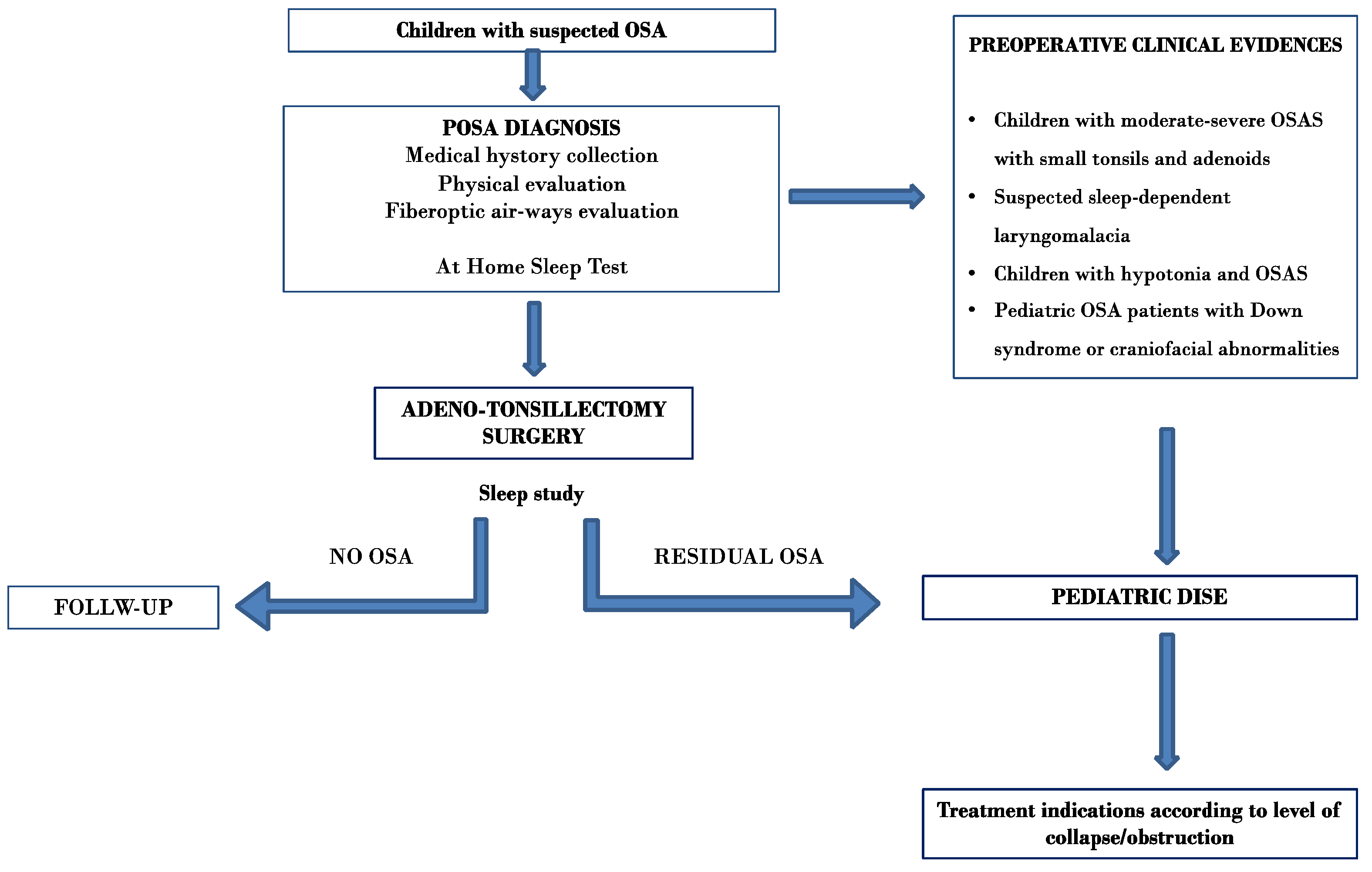
- Use and application of pediatric DISE (primary outcome);
- –
- Clinical indications for its use;
- –
- How the DISE procedure is performed in children;
- –
- Treatment choices for residual pediatric OSA according to the DISE outcomes.
2. Materials and Methods
2.1. Study Design and Setting
2.2. Survey
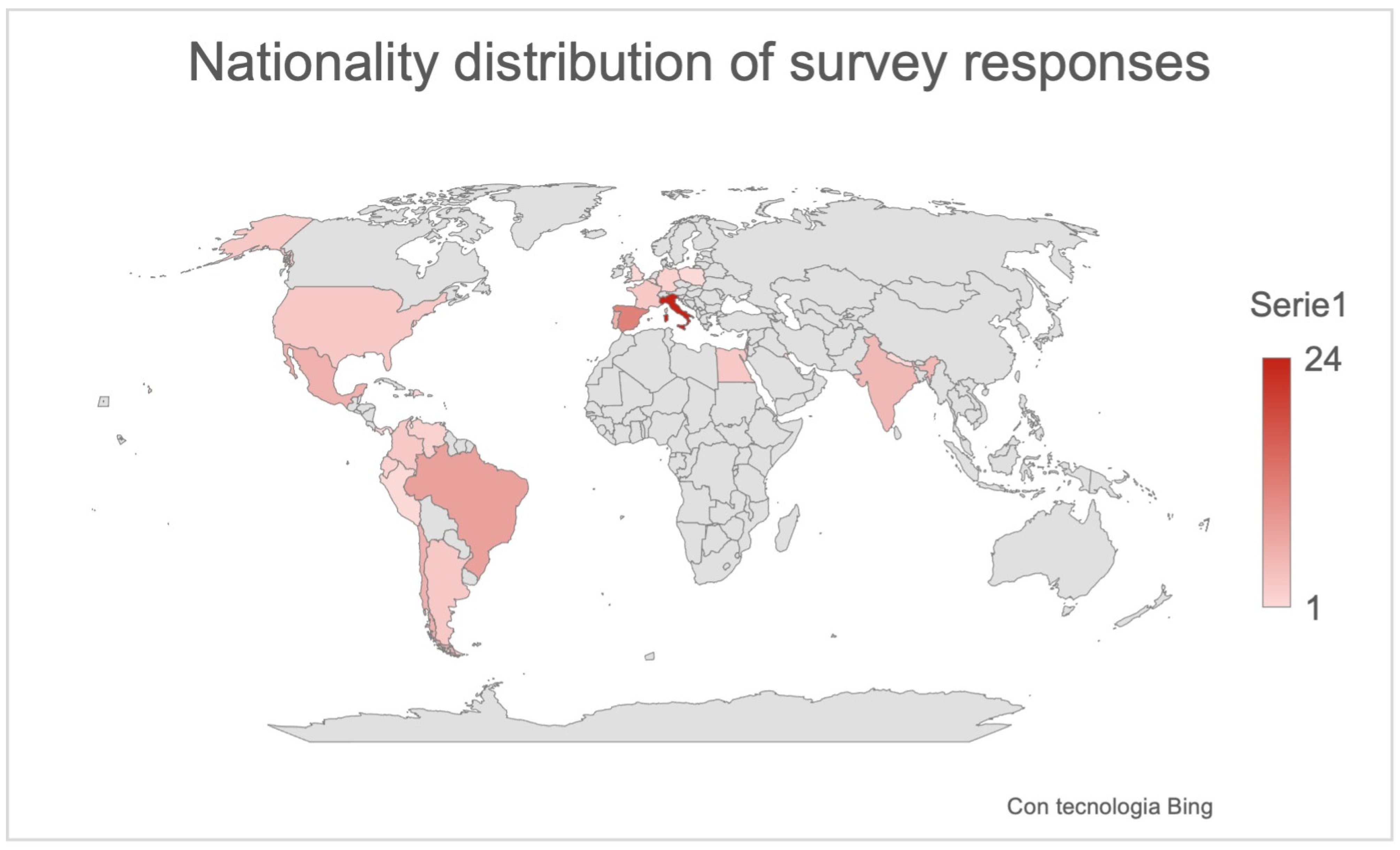
2.3. Participants of the Survey
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. General Information
3.2. Indication to the Pediatric DISE
3.3. DISE Protocol
3.4. Patient’s Indications According to Pediatric DISE Outcomes
4. Discussion
4.1. Indication to the Pediatric DISE
4.2. DISE Protocol
Patient’s Indications According to Pediatric DISE Outcomes
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parikh, S.R.; Boudewyns, A.; Friedman, N.R.; Schwartz, S.R.; Baldassari, C.M.; Benedek, P.; Carr, M.M.; Chan, D.K.; Chan, K.C.; Cheng, A.T.; et al. International Pediatric Otolaryngology Group (IPOG) consensus on scoring of pediatric Drug Induced Sleep Endoscopy (DISE). Int. J. Pediatr. Otorhinolaryngol. 2023, 171, 111627. [Google Scholar] [CrossRef] [PubMed]
- Cielo, C.M.; Tapia, I.E. What’s New in Pediatric Obstructive Sleep Apnea? Sleep Med. Clin. 2023, 18, 173–181. [Google Scholar] [CrossRef] [PubMed]
- Mussi, N.; Forestiero, R.; Zambelli, G.; Rossi, L.; Caramia, M.R.; Fainardi, V.; Esposito, S. The First-Line Approach in Children with Obstructive Sleep Apnea Syndrome (OSA). J. Clin. Med. 2023, 12, 7092. [Google Scholar] [CrossRef] [PubMed]
- Qarbal, J.; Le Treut-Gay, C.; Allali, L.; Rossi, M.E.; Nicollas, R.; Moreddu, E. Drug-Induced sleep endoscopy in children: NAVOTEL scoring system development. Pediatr. Pulmonol. 2023, 58, 1889–1895. [Google Scholar] [CrossRef]
- Mendes, N.; Antunes, J.; Guimarães, A.; Adónis, C.; Freire, F. Severe Pediatric Sleep Apnea: Drug-Induced Sleep Endoscopy Based Surgery. Indian. J. Otolaryngol. Head Neck Surg. 2023, 75, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Shman, S.L.; Maturo, S.; Schwartz, S.; McKenna, M.; Baldassari, C.M.; Bergeron, M.; Chernobilsky, B.; Ehsan, Z.; Gagnon, L.; Liu, Y.C.; et al. Expert Consensus Statement: Management of Pediatric Persistent Obstructive Sleep Apnea After Adenotonsillectomy. Otolaryngol. Head Neck Surg. 2023, 168, 115–130. [Google Scholar] [CrossRef]
- Iannella, G.; Magliulo, G.; Cammaroto, G.; Meccariello, G.; De Vito, A.; Pelucchi, S.; Ciorba, A.; Maniaci, A.; Cocuzza, S.; Gulotta, G.; et al. Effectiveness of drug-induced sleep endoscopy in improving outcomes of barbed pharyngoplasty for obstructive sleep apnea surgery: A prospective randomized trial. Sleep Breath. 2022, 26, 1621–1632. [Google Scholar] [CrossRef] [PubMed]
- Borrelli, M.; Corcione, A.; Rongo, R.; Cantone, E.; Scala, I.; Bruzzese, D.; Martina, S.; Strisciuglio, P.; Michelotti, A.; Santamaria, F. Obstructive Sleep Apnoea in Children with Down Syndrome: A Multidisciplinary Approach. J. Pers. Med. 2022, 13, 71. [Google Scholar] [CrossRef]
- Castillo-García, M.; Solano-Pérez, E.; Coso, C.; Romero-Peralta, S.; García-Borreguero, D.; Izquierdo, J.L.; Mediano, O. Impact of obstructive sleep apnea in cardiovascular risk in the pediatric population: A systematic review. Sleep Med. Rev. 2023, 71, 101818. [Google Scholar] [CrossRef]
- Frederick, R.M., 2nd; Brandt, J.; Sheyn, A. Drug-induced sleep endoscopy effect on intraoperative decision making in pediatric sleep surgery: A 2-year follow up. Laryngoscope Investig. Otolaryngol. 2022, 7, 2112–2118. [Google Scholar] [CrossRef]
- Kirkham, E.M. Pediatric Drug-Induced Sleep Endoscopy. Otolaryngol. Clin. N. Am. 2022, 55, 1165–1180. [Google Scholar] [CrossRef] [PubMed]
- Esteller Moré, E.; Navazo Egía, A.I.; Carrasco Llatas, M. Drug-induced sleep endoscopy in children. Acta Otorrinolaringol. (Engl. Ed.) 2020, 71, 309–315. [Google Scholar] [CrossRef]
- Sharma, A.V.; Padhya, T.; Nallu, S. Management of Pediatric Obstructive Sleep Apnea After Failed Tonsillectomy and Adenoidectomy. Adv. Pediatr. 2022, 69, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Kou, Y.F.; DeMarcantonio, M.A.; Heubi, C.H.; Fleck, R.; Kandil, A.; Smith, D.F.; Ishman, S.L. Sleep Endoscopy and Cine Magnetic Resonance Imaging Evaluation of Children with Persistent Obstructive Sleep Apnea. Otolaryngol. Head Neck Surg. 2023, 168, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.; McArdle, E.H.; Morrow, V.R.; Zalzal, H.G.; Carr, M.M.; Coutras, S.W. Base of Tongue Surgery and Pediatric Obstructive Sleep Apnea. Otolaryngol. Head Neck Surg. 2023, 168, 839–847. [Google Scholar] [CrossRef] [PubMed]
- Williamson, A.; Coutras, S.W.; Carr, M.M. Sleep Endoscopy Findings in Children with Obstructive Sleep Apnea and Small Tonsils. Ann. Otol. Rhinol. Laryngol. 2022, 131, 851–858. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.T.; Hsu, W.C. Efficacy of adenotonsillectomy on pediatric obstructive sleep apnea and related outcomes: A narrative review of current evidence. J. Formos. Med. Assoc. 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Cousineau, J.; Prévost, A.S.; Battista, M.C.; Gervais, M. Management of obstructive sleep apnea in children: A Canada-wide survey. J. Otolaryngol. Head Neck Surg. 2021, 50, 53. [Google Scholar] [CrossRef]
- Arganbright, J.M.; Lee, J.C.; Weatherly, R.A. Pediatric drug-induced sleep endoscopy: An updated review of the literature. World J. Otorhinolaryngol. Head Neck Surg. 2021, 7, 221–227. [Google Scholar] [CrossRef]
- Baldassari, C.M.; Lam, D.J.; Ishman, S.L.; Chernobilsky, B.; Friedman, N.R.; Giordano, T.; Lawlor, C.; Mitchell, R.B.; Nardone, H.; Ruda, J.; et al. Expert Consensus Statement: Pediatric Drug-Induced Sleep Endoscopy. Otolaryngol. Head Neck Surg. 2021, 165, 578–591. [Google Scholar] [CrossRef]
- Ergenekon, A.P.; Gokdemir, Y.; Ersu, R. Medical Treatment of Obstructive Sleep Apnea in Children. J. Clin. Med. 2023, 12, 5022. [Google Scholar] [CrossRef] [PubMed]
- Hyzer, J.M.; Milczuk, H.A.; Macarthur, C.J.; King, E.F.; Quintanilla-Dieck, L.; Lam, D.J. Drug-Induced Sleep Endoscopy Findings in Children with Obstructive Sleep Apnea with vs without Obesity or Down Syndrome. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.A.; Liu, C.C.; Alex, G.; Szmuk, P.; Mitchell, R.B. Anesthetic management of children undergoing drug-induced sleep endoscopy: A retrospective review. Int. J. Pediatr. Otorhinolaryngol. 2020, 139, 110440. [Google Scholar] [CrossRef] [PubMed]
- Love, H.; Slaven, J.E.; Mitchell, R.M.; Bandyopadhyay, A. Outcomes of OSA in surgically naïve young children with and without DISE identified laryngomalacia. Int. J. Pediatr. Otorhinolaryngol. 2020, 138, 110351. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, E.M.; Hoi, K.; Melendez, J.B.; Henderson, L.M.; Leis, A.M.; Puglia, M.P., 2nd; Chervin, R.D. Propofol versus dexmedetomidine during drug-induced sleep endoscopy (DISE) for pediatric obstructive sleep apnea. Sleep Breath. 2021, 25, 757–765. [Google Scholar] [CrossRef] [PubMed]
- Raposo, D.; Menezes, M.; Rito, J.; Trindade-Soares, M.; Adónis, C.; Loureiro, H.C.; Freire, F. Drug-Induced Sleep Endoscopy in Pediatric Obstructive Sleep Apnea. Otolaryngol. Head Neck Surg. 2021, 164, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Kirkham, E.M.; Melendez, J.B.; Hoi, K.; Chervin, R.D. Drug-Induced Sleep Endoscopy in Children with Positional Obstructive Sleep Apnea. Otolaryngol. Head Neck Surg. 2021, 164, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.F.; He, S.; Peddireddy, N.S.; Vairavan Manickam, P.; Heubi, C.H.; Shott, S.R.; Cohen, A.P.; Ishman, S.L. Effectiveness of pediatric drug-induced sleep endoscopy for REM-predominant obstructive sleep apnea. Sleep Breath. 2020, 24, 1705–1713. [Google Scholar] [CrossRef]
- Venekamp, R.P.; Hearne, B.J.; Chandrasekharan, D.; Blackshaw, H.; Lim, J.; Schilder, A.G. Tonsillectomy or adenotonsillectomy versus non-surgical management for obstructive sleep-disordered breathing in children. Cochrane Database Syst. Rev. 2015, 2015, CD011165. [Google Scholar] [CrossRef]
- Amos, J.M.; Durr, M.L.; Nardone, H.C.; Baldassari, C.M.; Duggins, A.; Ishman, S.L. Systematic Review of Drug-Induced Sleep Endoscopy Scoring Systems. Otolaryngol. Head Neck Surg. 2018, 158, 240–248. [Google Scholar] [CrossRef]
- Camacho, M.; Noller, M.W.; Zaghi, S.; Reckley, L.K.; Fernandez-Salvador, C.; Ho, E.; Dunn, B.; Chan, D. Tongue surgeries for pediatric obstructive sleep apnea: A systematic review and meta-analysis. Eur. Arch. Otorhinolaryngol. 2017, 274, 2981–2990. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.F.; Hsu, W.C.; Lee, C.H.; Lin, M.T.; Kang, K.T. Treatment outcomes of supraglottoplasty for pediatric obstructive sleep apnea: A meta-analysis. Int. J. Pediatr. Otorhinolaryngol. 2016, 87, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Iannella, G.; Cammaroto, G.; Meccariello, G.; Cannavicci, A.; Gobbi, R.; Lechien, J.R.; Calvo-Henríquez, C.; Bahgat, A.; Di Prinzio, G.; Cerritelli, L.; et al. Head-of-Bed Elevation (HOBE) for Improving Positional Obstructive Sleep Apnea (POSA): An Experimental Study. J. Clin. Med. 2022, 11, 5620. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Advocated Reasons against the Use of the Pediatric DISE in OSA Children of 37 Participants to the Survey | Number | Percentage |
|---|---|---|
| Lack of pediatric DISE experience at the sleep center | 10 | 27% |
| Absence of an anesthesiologic pediatric team with expertise in children’s sedation—Anesthesia Risks | 7 | 18.9% |
| Not useful procedures | 9 | 24.3% |
| Procedure useful in very selected cases (neurological cases—craniofacial deformities children) | 5 | 13.5% |
| Not favorable risk/benefit ratio | 5 | 13.5% |
| Expensive | 1 | 2.7% |
| PEDIATRIC DISE INDICATIONS—83 Participants | Disagree | Neutral | Agree |
|---|---|---|---|
| In cases of healthy pediatric patients with a new diagnosis of OSA (At-Home Sleep Test), do you consider DISE as the first test before adenotonsillectomy surgery in order to identify sites of collapse? | 59 (71%) | 15 (18.1%) | 9 (10.8%) |
| In cases of healthy pediatric patients with a new diagnosis of OSA (At-Home Sleep Test), do you consider DISE at the same time as scheduling adenotonsillectomy surgery to identify other possible sites of collapse? | 46 (55.4%) | 10 (12%) | 27 (32.5%) |
| In the case of children with moderate–severe OSAS with small tonsils and adenoids (disproportion), do you consider DISE indicated before surgery? | 11 (13.2%) | 2 (2.4%) | 70 (84.3%) |
| Do you consider a DISE as a first-line test in cases of suspected sleep-dependent laryngomalacia? | 15 (18%) | 6 (7.2%) | 62 (74.6%) |
| In children with hypotonia and OSAS, do you consider DISE in the diagnostic management? | 7 (8.4%) | 13 (16.9%) | 63 (75.9%) |
| In cases of patients with Down syndrome or craniofacial abnormalities and OSA, do you consider DISE before surgery? | 11 (13.3%) | 18 (21.7%) | 54 (65%) |
| In cases of persistent OSA in children after adenotonsillectomy, do you suggest DISE as the first diagnostic step? | 10 (12%) | 5 (6%) | 68 (81.9%) |
| In cases of persistent OSA in children after adenotonsillectomy, do you consider CPAP or other treatments as a first line treatment avoiding DISE? | 65 (78.3%) | 12 (14.6%) | 5 (6%) |
| PEDIATRIC DISE PROTOCOL—83 Participants | Disagree | Neutral | Agree |
|---|---|---|---|
| Do you consider maneuvers such as jaw thrusts useful during pediatric DISE? | 7 (8.4%) | 19 (22.9%) | 57 (68.6%) |
| Do you consider maneuvers such as chin lifts useful during pediatric DISE? | 4 (6.8%) | 21 (25.3%) | 58 (69.8%) |
| Do you consider testing the lateral position during the pediatric DISE? | 6 (7.2%) | 16 (19.3%) | 61 (73.4%) |
| Do you consider testing the Head-Of-Bed Elevation (HOBE) during the pediatric DISE? | 8 (9.6%) | 39 (46.9%) | 36 (43.3%) |
| Do you consider the use of topical nasal decongestants in order to facilitate the advancement of the endoscope? | 51 (61.4%) | 15 (18.1%) | 17 (20.4%) |
| TREATMENT INDICATIONS ACCORDING TO PEDIATRIC DISE OUTCOMES—83 Participants | Disagree | Neutral | Agree |
|---|---|---|---|
| In cases of base-of-tongue anteroposterior collapse during DISE in children with previous adenotonsillectomy surgery, do you consider base-of-tongue surgery? | 19 (22.8%) | 16 (19.3%) | 48 (57.8%) |
| In cases of children with severe OSA, comorbidities or craniofacial malformations and only the collapse of big tonsils during DISE, do you consider only the tonsillectomy? | 6 (7.2%) | 4 (5.8%) | 73 (87.9%) |
| In cases of young patients with severe OSA and only epiglottis collapses during DISE, do you consider epiglottis surgery? | 10 (12%) | 15 (17.9%) | 59 (71%) |
| In cases of young patients with residual OSA and only pharyngeal collapse during DISE, do you consider velopharyngeal surgery? | 23 (27.7%) | 18 (21.4%) | 43 (51.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iannella, G.; Magliulo, G.; Greco, A.; De Virgilio, A.; Maniaci, A.; Lechien, J.R.; Calvo-Henriquez, C.; Bahgat, A.Y.; Casale, M.; Lugo, R.; et al. Clinical Application of Pediatric Sleep Endoscopy: An International Survey. Children 2024, 11, 94. https://doi.org/10.3390/children11010094
Iannella G, Magliulo G, Greco A, De Virgilio A, Maniaci A, Lechien JR, Calvo-Henriquez C, Bahgat AY, Casale M, Lugo R, et al. Clinical Application of Pediatric Sleep Endoscopy: An International Survey. Children. 2024; 11(1):94. https://doi.org/10.3390/children11010094
Chicago/Turabian StyleIannella, Giannicola, Giuseppe Magliulo, Antonio Greco, Armando De Virgilio, Antonino Maniaci, Jerome R. Lechien, Christian Calvo-Henriquez, Ahmed Yassin Bahgat, Manuele Casale, Rodolfo Lugo, and et al. 2024. "Clinical Application of Pediatric Sleep Endoscopy: An International Survey" Children 11, no. 1: 94. https://doi.org/10.3390/children11010094