

Assessment of Selected Immune Parameters in Patients Undergoing Cardiac Surgery with the Use of Cardiopulmonary Bypass: Aspects of Age and Sex—A Pilot Study

Abstract
:
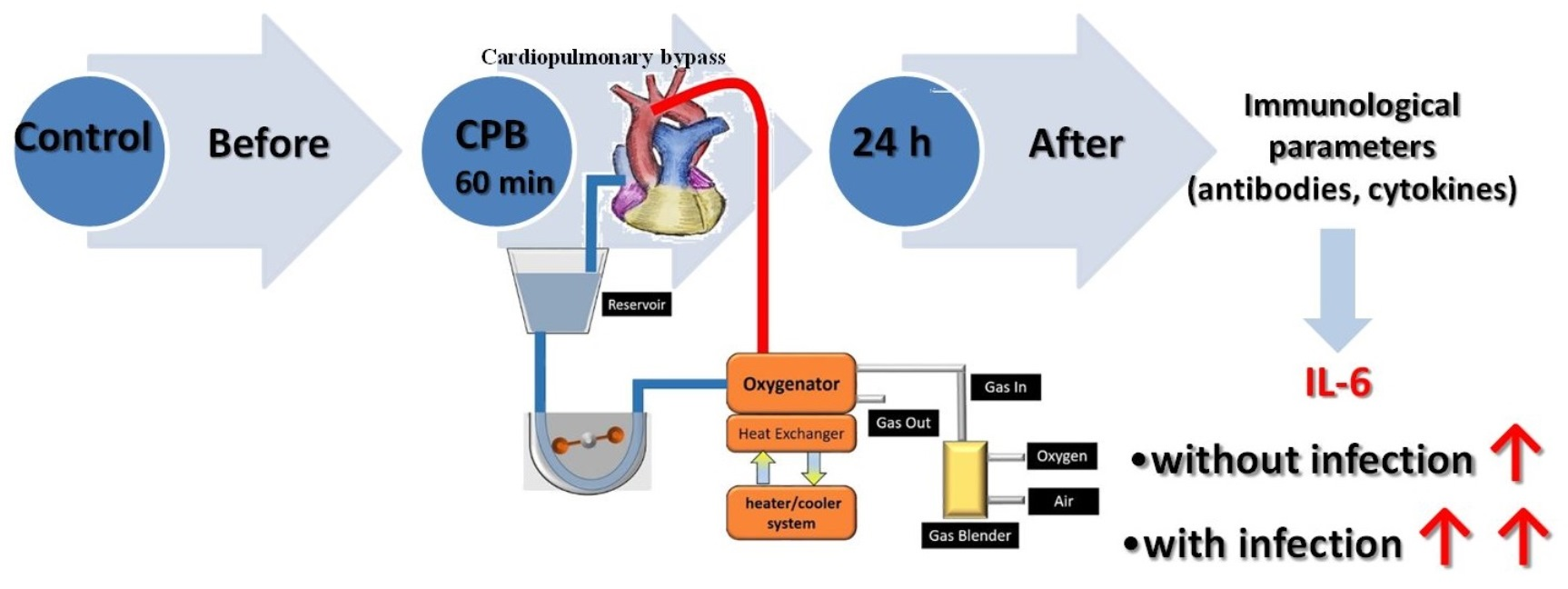
1. Introduction
2. Materials and Methods
2.1. Legal Aspects
2.2. Inclusion and Exclusion Criteria
2.3. Characteristics of Surgery Conditions
2.4. Collection and Preparation of Samples
2.5. Statistical Analyses
3. Results
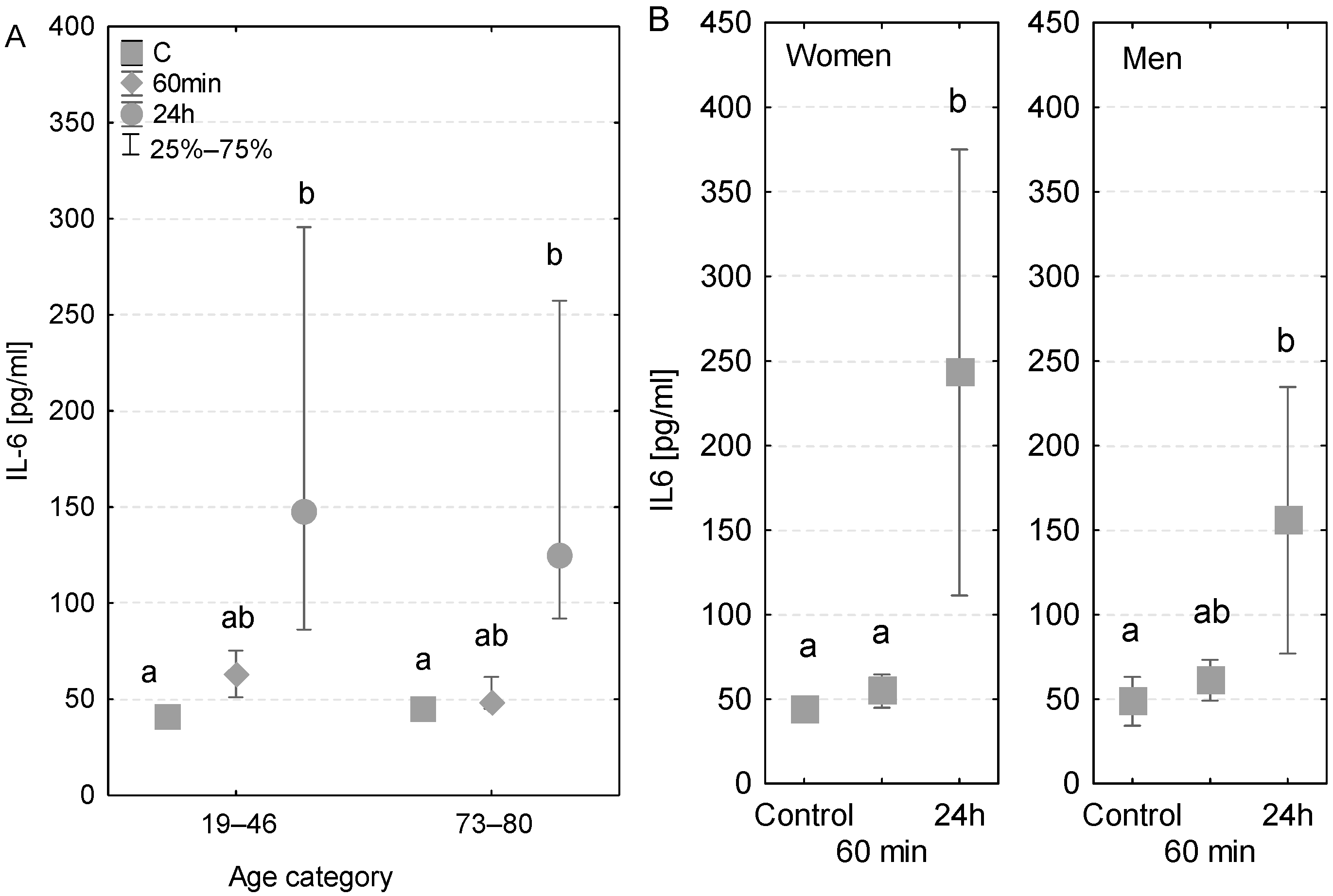
3.1. IL-6
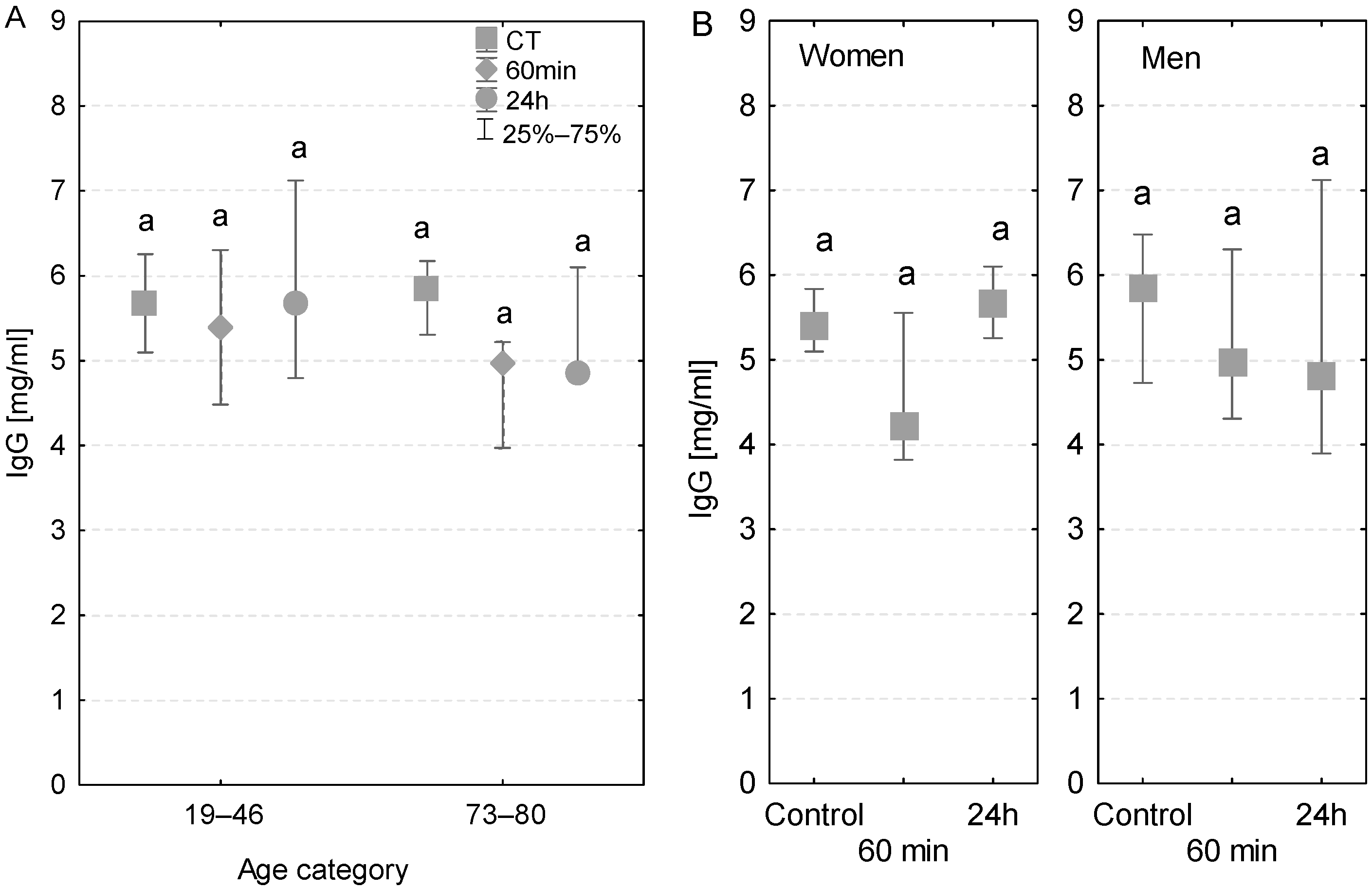
3.2. IgG
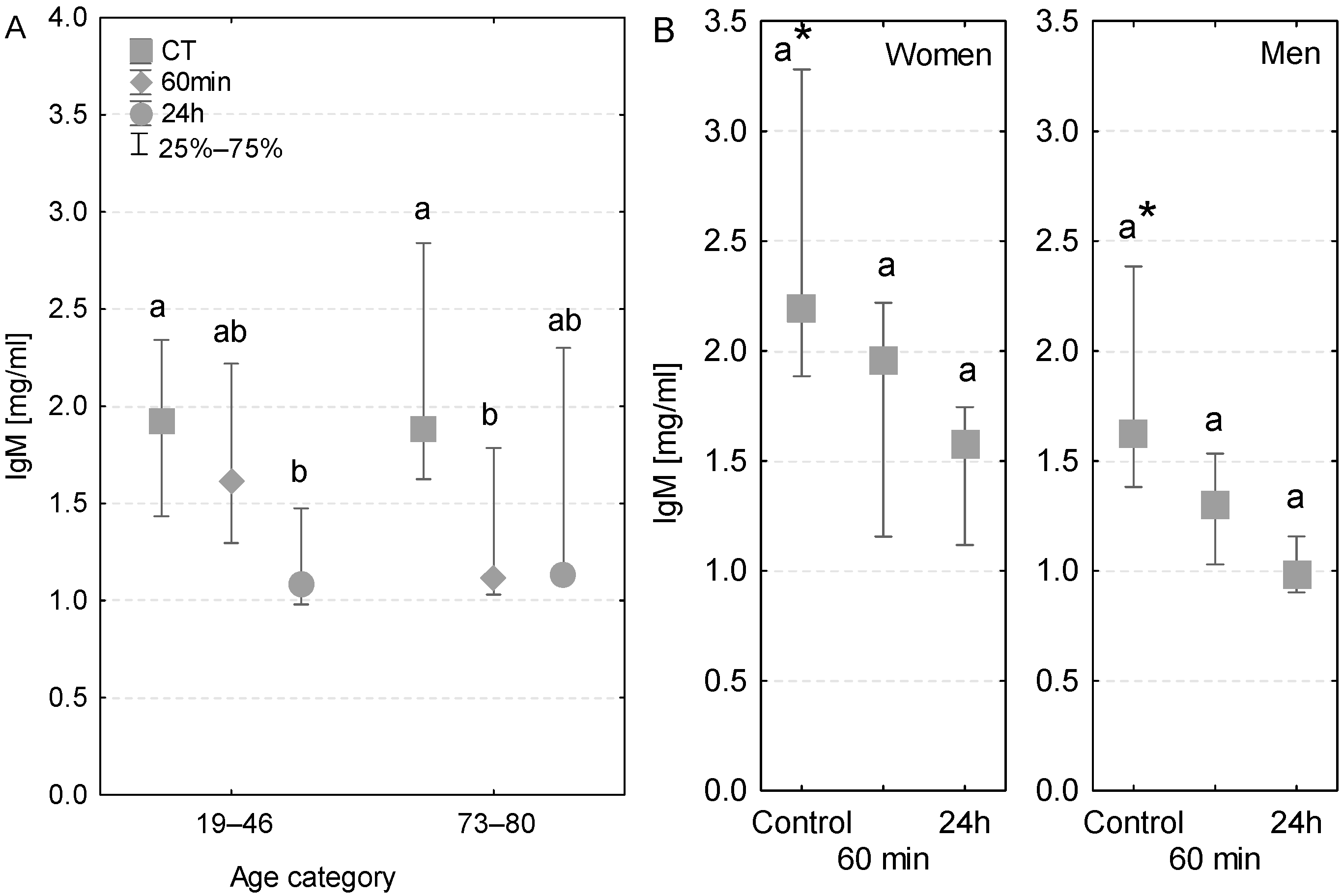
3.3. IgM
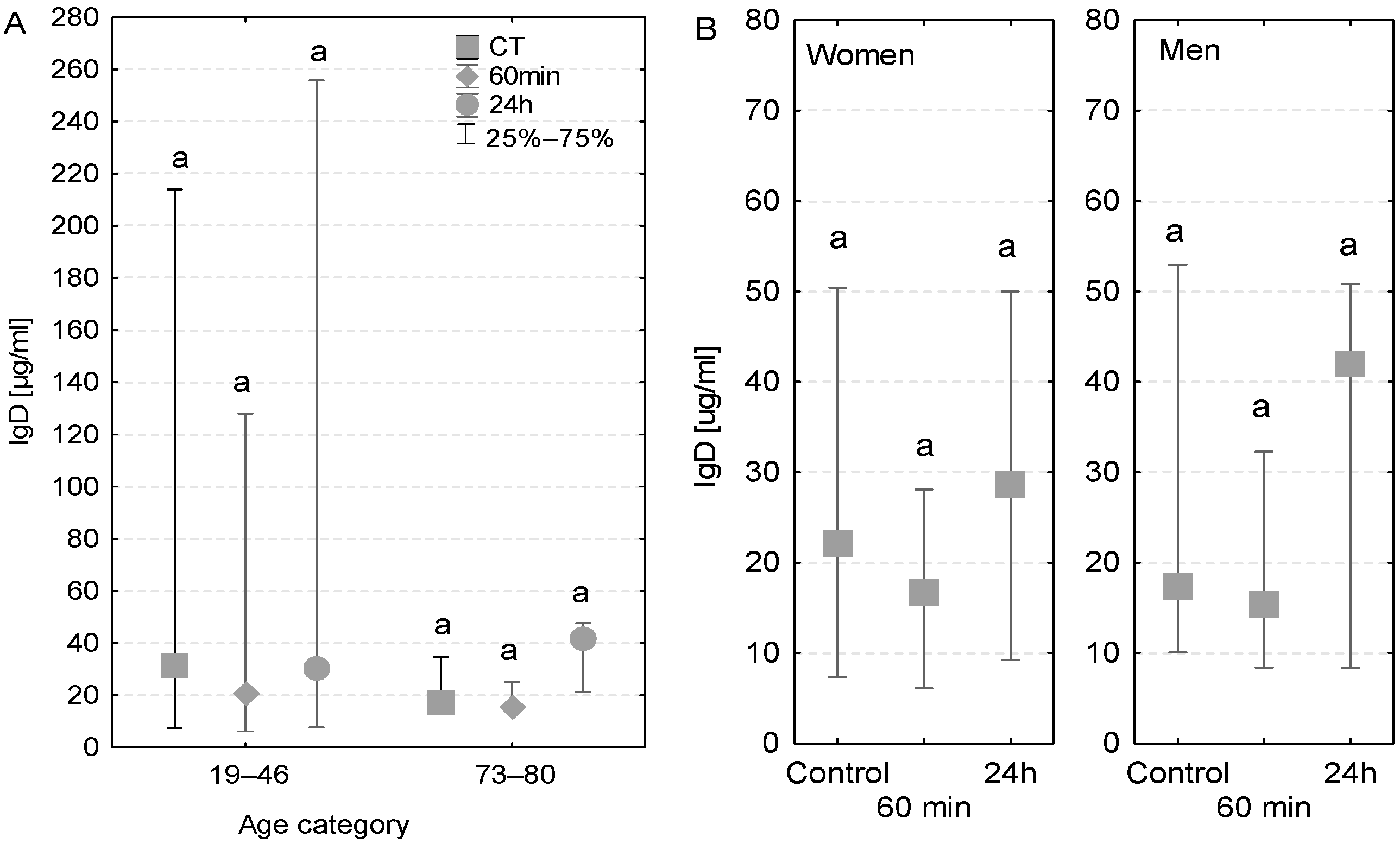
3.4. IgD
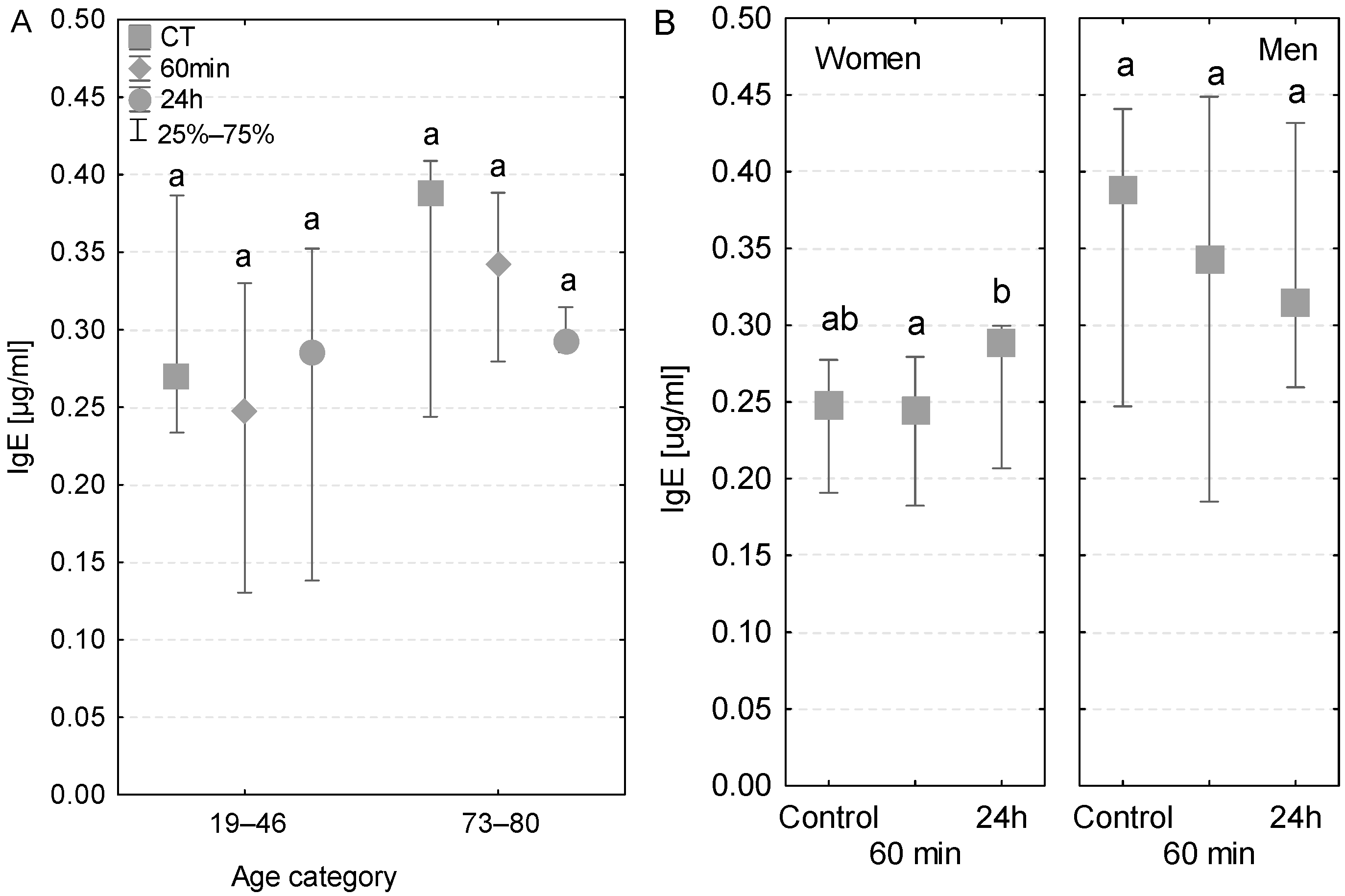
3.5. IgE
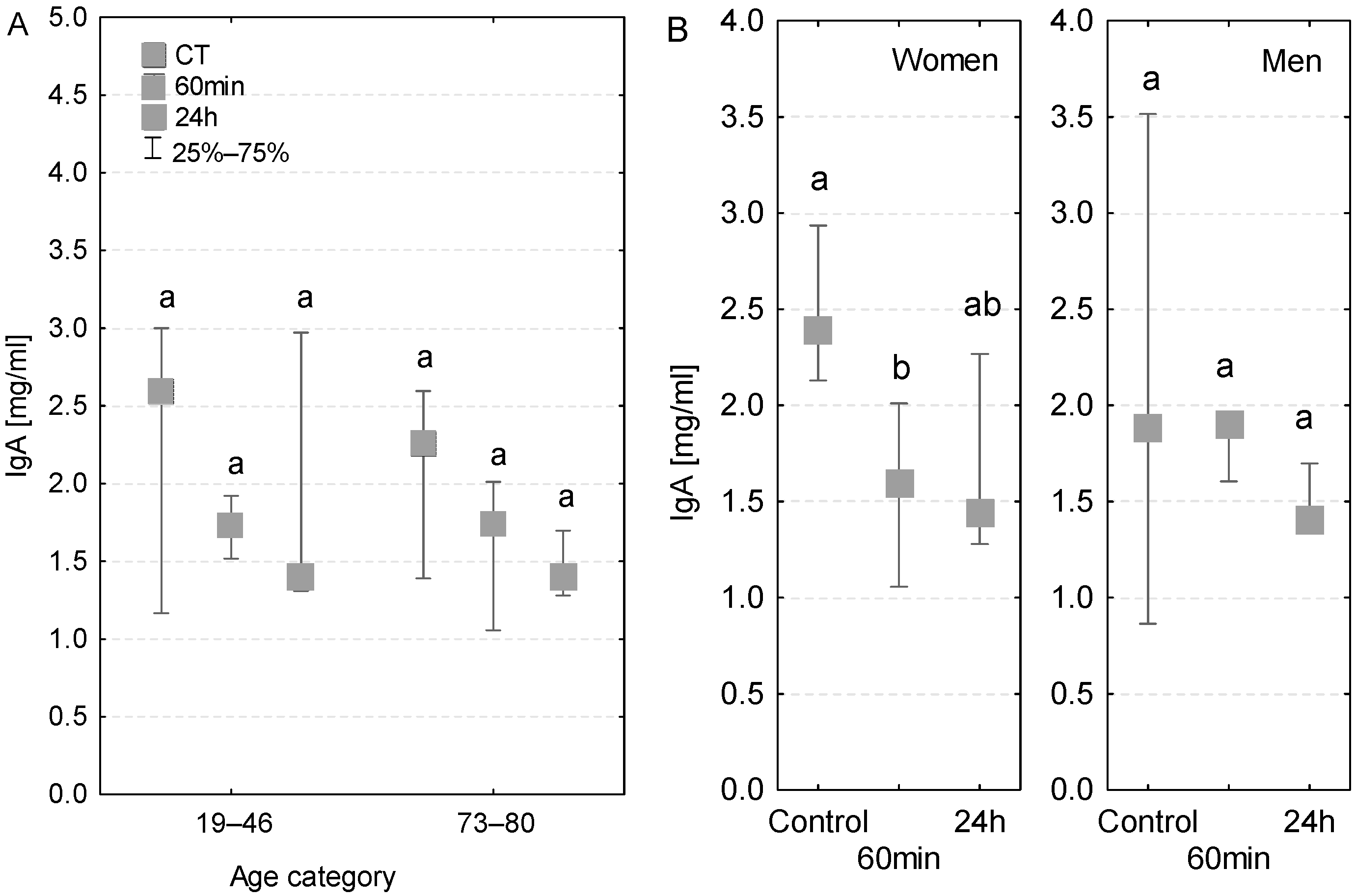
3.6. IgA
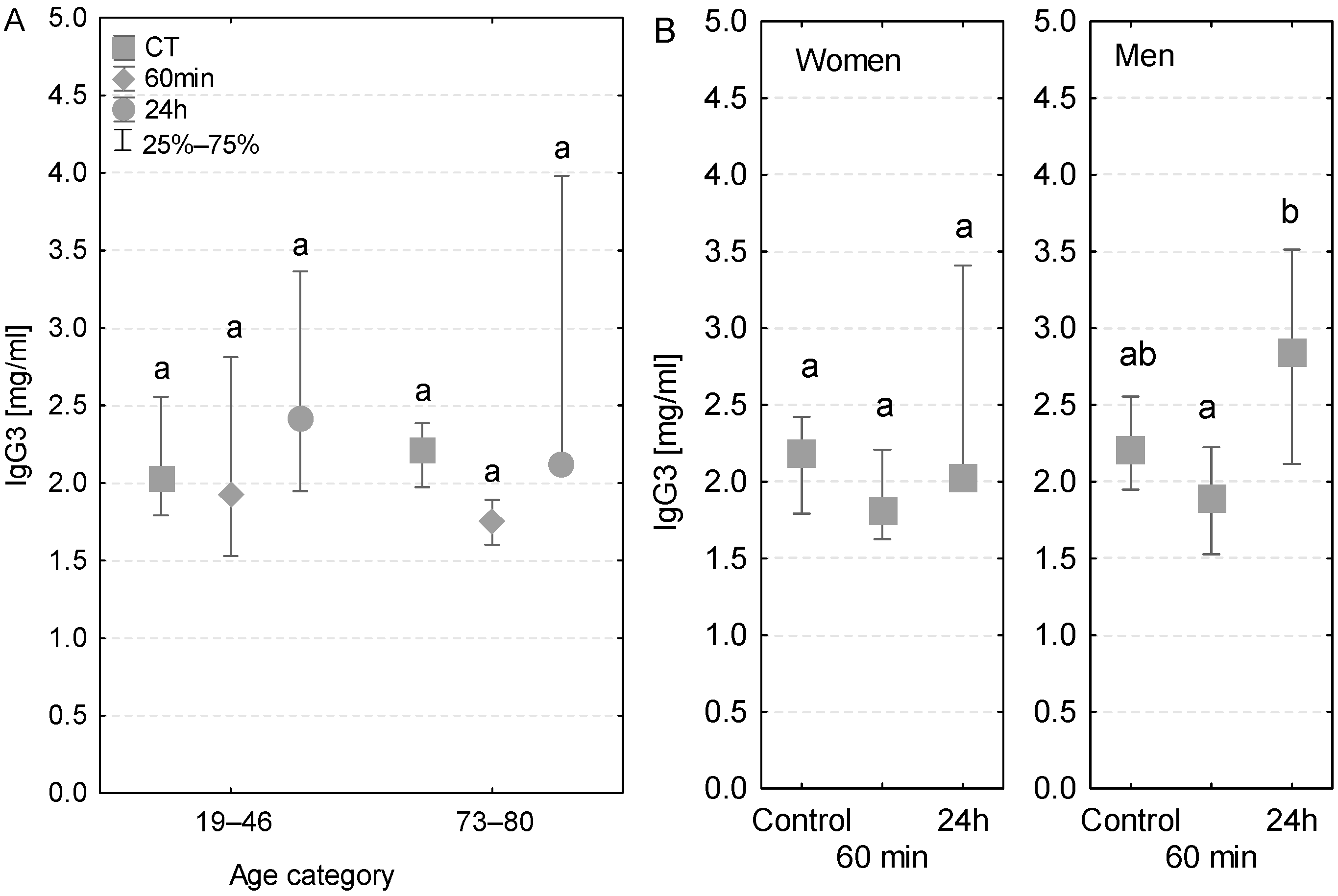
3.7. IgG3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gravlee, G.P.; Davis, F.R.; Kursz, M.; Utley, J.R. Cardiopulmonary Bypass: Principles and Practice, 2nd ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2002. [Google Scholar]
- Scott, B.H.; Seifert, F.C.; Glass, P.S.; Grimson, R. Blood use in patients undergoing coronary artery bypass surgery: Impact of cardiopulmonary bypass pump, hematocrit, gender, age, and body weight. Anesth. Analg. 2003, 97, 958–963. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Z.; Theroux, P. Platelet activation with unfractionated heparin at therapeutic concentrations and comparisons with a low–molecular–weight heparin and with a direct thrombin inhibitor. Circulation 1998, 97, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Tajima, K.; Yamamoto, F.; Kawazoe, K.; Nakatani, I.; Sakai, H.; Abe, T.; Kawashima, Y. Cardiopulmonary bypass and cellular immunity: Changes in lymphocyte subsets and natural killer cell activity. Ann. Thorac. Surg. 1993, 55, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Fillinger, M.P.; Rassias, A.J.; Guyre, P.M.; Sanders, J.H.; Beach, M.; Pahl, J.; Watson, R.B.; Whalen, P.K.; Yeo, K.-T.J.; Yeager, M.P. Glucocorticoid effects on the inflammatory and clinical responses to cardiac surgery. J. Cardiothorac. Vasc. Anesth. 2002, 16, 163–169. [Google Scholar] [CrossRef]
- Teoh, K.H.; Bradley, C.A.; Gauldie, J.; Burrows, H. Steroid inhibition of cytokine–mediated vasodilation after warm heart surgery. Circulation 1995, 92, 347–353. [Google Scholar] [CrossRef]
- Kirklin, J.K.; Westaby, S.; Blackstone, E.H.; Kirklin, J.W.; Chenoweth, D.E.; Pacifico, A.D. Complement and the damaging effects of cardiopulmonary bypass. J. Thorac. Cardiovasc. Surg. 1983, 86, 845–857. [Google Scholar] [CrossRef]
- Chenoweth, D.E.; Cooper, S.W.; Hugli, T.E.; Stewart, R.W.; Blackstone, E.H.; Kirklin, J.W. Complement activation during cardiopulmonary bypass: Evidence for generation of C3a and C5a anaphylatoxins. N. Engl. J. Med. 1981, 304, 497–503. [Google Scholar] [CrossRef]
- Hammerschmidt, D.E.; Stroncek, D.F.; Bowers, T.K.; Lammi-Keefe, C.J.; Kurth, D.M.; Ozalins, A.; Nicoloff, D.M.; Lillehei, R.C.; Craddock, P.R.; Jacob, H.S. Complement activation and neutropenia occurring during cardiopulmonary bypass. J. Thorac. Cardiovasc. Surg. 1981, 81, 370–377. [Google Scholar] [CrossRef]
- Utley, J.R. Pathophysiology of cardiopulmonary bypass: A current review. Aust. J. Cardiac. Thorac. Surg. 1992, 1, 46–52. [Google Scholar] [CrossRef]
- Kirklin, J.; McGriffin, D. Early complications following cardiac surgery. Cardiovasc. Clin. 1987, 17, 321–343. [Google Scholar]
- Miedzinsky, L.; Karen, G. Serious infectious complications of open heart surgery. Can. J. Surg. 1987, 30, 103–107. [Google Scholar]
- Cremer, J.; Martin, M.; Redl, H. Systemic inflammatory response after cardiac operations. Ann. Thorac. Surg. 1996, 61, 1714–1720. [Google Scholar] [CrossRef]
- Martin, G.R.; Short, B.L.; Abbot, C.; O’Brien, A.M. Cardiac stun in infants undergoing extracorporeal membrane oxygenation. J. Thorac. Cardiovasc. Surg. 1991, 101, 607–611. [Google Scholar] [CrossRef]
- Gaudino, M.; Chadow, D.; Rahouma, M.; Soletti, G.J.; Sandner, S.; Perezgrovas-Olaria, R.; Audisio, K.; Cancelli, G.; Bratton, B.A.; Fremes, S.; et al. Operative Outcomes of Women Undergoing Coronary Artery Bypass Surgery in the US, 2011 to 2020. JAMA Surg. 2023, 1, e228156. [Google Scholar] [CrossRef]
- Greenberg, J.H.; Whitlock, R.; Zhang, W.R.; Thiessen-Philbrook, H.R.; Zappitelli, M.; Devarajan PEikelboom, J.; Kavsak, P.A.; Devereaux, P.J.; Shortt, C.; Garg, A.X.; et al. Interleukin–6 and interleukin–10 as acute kidney injury biomarkers in pediatric cardiac surgery. Pediatr. Nephrol. 2015, 30, 1519–1527. [Google Scholar] [CrossRef]
- Lante, W.; Franke, A.; Weinhold, C.; Markewitz, A. Immunoglobulin levels and lymphocyte subsets following cardiac operations: Further evidence for a T–helper cell shifting. Thorac. Cardiovasc. Surg. 2005, 53, 16–22. [Google Scholar] [CrossRef]
- Brix-Christensen, V. The systemic inflammatory response after cardiac surgery with cardiopulmonary bypass in children. Acta Anaesthesiol. Scand. 2001, 45, 671–679. [Google Scholar] [CrossRef]
- Butler, J.; Chong, G.L.; Baigrie, R.J.; Pillai, R.; Westaby, S.; Rocker, G.M. Cytokine responses to cardiopulmonary bypass with membrane and bubble oxygenation. Ann. Thorac. Surg. 1992, 61, 1724–1821. [Google Scholar] [CrossRef]
- Steinberg, J.B.; Kapelanski, D.P.; Olson, J.D.; Weiler, J.M. Cytokine and complement levels in patients undergoing cardiopulmonary bypass. Ann. Thorac. Surg. 1993, 106, 1008–1016. [Google Scholar] [CrossRef]
- Gaini, S.; Koldkjaer, O.G.; Pedersen, C. Procalcitonin, lipopolysaccharide–binding protein, interleukin–6 and C–reactive protein in community–acquired infections and sepsis: A prospective study. Crit. Care 2006, 10, R53. [Google Scholar] [CrossRef]
- Van Velzen–Blad, H.; Dijkstra, Y.J.; Schurink, G.A.; Verbrugh, H.A.; Verhoef, J.; Zegers, B.J.; Ballieux, R.E. Cardiopulmonary bypass and host defense functions in human beings: Serum levels and the role of immunoglobulins and complement in phagocytosis. Ann. Thorac. Surg. 1985, 39, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Castle, S.; Uyemura, K.; Crawford, W.; Wong, W.; Makinodan, T. Antigen presenting cell function is enhanced in healthy elderly. Mech. Ageing Dev. 1999, 107, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Fulop, T.; Larbi, A.; Wikby, A.; Mocchegiani, E.; Hirokawa, K.; Pawelec, G. Dysregulation of T–cell function in the elderly: Scientific basis and clinical implications. Drugs Aging 2005, 22, 589–603. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M. A comparison of alternative tests of significance for the problem of m rankings. Ann. Math. Stat. 1940, 11, 86–92. [Google Scholar] [CrossRef]
- Gozdzik, W.; Adamik, B.; Gozdzik, A.; Rachwalik, M.; Kustrzycki, W.; Kübler, A. Unchanged plasma levels of the soluble urokinase plasminogen activator receptor in elective coronary artery bypass graft surgery patients and cardiopulmonary bypass use. PLoS ONE 2014, 9, e98923. [Google Scholar] [CrossRef]
- Diegeler, A.; Doll, N.; Rauch, T.; Haberer, D.; Walther, T.; Falk, V.; Mohr, F.W. Humoral immune response during coronary artery bypass grafting: A comparison of limited approach, “off–pump” technique, and conventional cardiopulmonary bypass. Circulation 2000, 102, 95–100. [Google Scholar] [CrossRef]
- Vertrees, R.; Tao, W.; Kramer, G.C. Tumor necrosis factor monoclonal antibody prevents alteration in leucocyte population during cardiopulmonary bypass. ASAIO J. 1994, 40, 554–559. [Google Scholar] [CrossRef]
- He, S.; Lin, K.; Ma, R.; Xu, R.; Xiao, Y. Effect of the urinary tryptin inhibitor ulinastatin on cardiopulmonary bypass–related inflammatory response and clinical outcomes: A meta–analysis of randomized controlled trials. Clin. Ther. 2015, 37, 643–653. [Google Scholar] [CrossRef]
- Hirokawa, K.; Utsuyama, M.; Hayashi, Y.; Kitagawa, M.; Makinodan, T.; Fulop, T. Slower immune system aging in women versus men in the Japanese population. Immun. Ageing 2013, 15, 10–19. [Google Scholar] [CrossRef]
- Oertelt–Prigione, S. The influence of sex and gender on the immune response. Autoimmun. Rev. 2012, 11, 479–485. [Google Scholar] [CrossRef]
- Vina, J.; Borras, C.; Gambini, J.; Sastre, J.; Pallardo, V.V. Why females live longer than males? Importance of the upregulation of longevity–associated genes by estrogenic compounds. FEBS Lett. 2005, 579, 2541–2545. [Google Scholar] [CrossRef]
- Caruso, C.; Accardi, G.; Virruso, C.; Candore, G. Sex, gender and immunosenescence: A key to understand the different lifespan between men and women. Immun. Ageing 2013, 16, 20. [Google Scholar] [CrossRef]
- Fernandez, J.; Laub, G.W.; Adkins, M.S.; Anderson, W.A.; Chen, C.; Bailey, B.M.; Nealon, L.M.; McGrath, L.B. Early and late–phase events after valve replacement with the St. Jude Medical prosthesis in 1200 patients. J. Thorac. Cardiovasc. Surg. 1994, 107, 394–406. [Google Scholar] [CrossRef]
- Rinder, C.S.; Mathew, J.P.; Rinder, H.M.; Tracey, J.B.; Davis, E.; Smith, B.R. Lymphocyte and monocyte subsets changes during cardiopulmonary bypass: Effects of aging and gender. J. Lab. Clin. Med. 1997, 129, 592–602. [Google Scholar] [CrossRef]
- DiPiro, J.T.; Howdieshell, T.R.; Hamilton, R.G.; Mansberger, A.R., Jr. Immunoglobulin E and eosinophil counts are increased after sepsis in trauma patients. Crit. Care Med. 1998, 26, 465–469. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| IL-6 and IgA Concentration Analyses | ||||||
|---|---|---|---|---|---|---|
| Group of Patients | Parameter | Age (Years) | EuroSCORE | BMI | Circulation Duration (min) | Aortic Cross-Clamping Duration (min) |
| Women | Average | 61 | 7 | 26.8 | 132 | 82 |
| Min | 19 | 5 | 20 | 95 | 58 | |
| Max | 83 | 12 | 33 | 171 | 120 | |
| Number of patients | 6 | |||||
| Men | Average | 55 | 6 | 25.2 | 98 | 67 |
| Min | 26 | 3 | 20 | 59 | 34 | |
| Max | 83 | 8 | 32 | 157 | 124 | |
| Number of patients | 6 | |||||
| Patients at the age of 18–69 | Average | 39 | 7 | 23.3 | 121 | 74 |
| Min | 19 | 3 | 20 | 59 | 34 | |
| Max | 61 | 12 | 30 | 157 | 124 | |
| Number of patients | 6 | |||||
| Patients at the age of 70 and above | Average | 77 | 7 | 28.7 | 112 | 76 |
| Min | 72 | 5 | 24 | 71 | 39 | |
| Max | 83 | 8 | 33 | 171 | 120 | |
| Number of patients | 6 | |||||
| IgG, IgM, IgD, IgE, and IgG3 concentration analyses | ||||||
| Women | Average | 51 | 6 | 30.2 | 104 | 62 |
| Min | 21 | 3 | 24 | 80 | 44 | |
| Max | 76 | 9 | 39 | 121 | 80 | |
| Number of patients | 5 | |||||
| Men | Average | 49 | 4 | 25.7 | 154 | 100 |
| Min | 19 | 2 | 19 | 104 | 64 | |
| Max | 76 | 6 | 33 | 307 | 235 | |
| Number of patients | 6 | |||||
| Patients at the age of 18–69 | Average | 30 | 4 | 28.5 | 139 | 96 |
| Min | 19 | 2 | 19 | 80 | 57 | |
| Max | 46 | 6 | 39 | 307 | 235 | |
| Number of patients | 6 | |||||
| Patients at the age of 70 and above | Average | 75 | 7 | 26.8 | 114 | 66 |
| Min | 73 | 5 | 22 | 104 | 44 | |
| Max | 76 | 9 | 33 | 123 | 76 | |
| Number of patients | 5 | |||||
| Characteristic | P1 | P2 | P3 |
|---|---|---|---|
| Sex | Man | Woman | Woman |
| Age (years) | 73 | 80 | 77 |
| EuroSCORE | 12 | 7 | 8 |
| BMI | 28 | 23 | 22 |
| Circulation duration (min) | 368 | 100 | 147 |
| Aortic cross-clamping duration (min) | 207 | 62 | 105 |
| Time Point | IgG (mg/mL) | IgG3 (mg/mL) | IgM (mg/mL) | IgD (µg/mL) | IgE (µg/mL) | IgA (mg/mL) | IL6 (pg/mL) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient | ||||||||||||
| P1 | P2 | P1 | P2 | P1 | P2 | P1 | P2 | P1 | P2 | P3 | P3 | |
| CT | 5.02 | 4.39 | 3.09 | 2.42 | 2.38 | 1.83 | 26 | 9.38 | 0.25 | 0.25 | 2.87 | 49.01 |
| 60 min | 4.31 | 3.75 | 1.96 | 1.86 | 1.53 | 1.16 | 15.9 | 8.2 | 0.19 | 0.23 | 2.05 | 52.26 |
| 24 h | 3.89 | 5.25 | 2.29 | 3.41 | 0.98 | 1.75 | 44.68 | 9.25 | 0.35 | 0.21 | 1.89 | 318.29 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sindera, P.; Kucewicz-Czech, E.; Wilczek, G. Assessment of Selected Immune Parameters in Patients Undergoing Cardiac Surgery with the Use of Cardiopulmonary Bypass: Aspects of Age and Sex—A Pilot Study. Biomedicines 2023, 11, 1224. https://doi.org/10.3390/biomedicines11041224
Sindera P, Kucewicz-Czech E, Wilczek G. Assessment of Selected Immune Parameters in Patients Undergoing Cardiac Surgery with the Use of Cardiopulmonary Bypass: Aspects of Age and Sex—A Pilot Study. Biomedicines. 2023; 11(4):1224. https://doi.org/10.3390/biomedicines11041224
Chicago/Turabian StyleSindera, Piotr, Ewa Kucewicz-Czech, and Grażyna Wilczek. 2023. "Assessment of Selected Immune Parameters in Patients Undergoing Cardiac Surgery with the Use of Cardiopulmonary Bypass: Aspects of Age and Sex—A Pilot Study" Biomedicines 11, no. 4: 1224. https://doi.org/10.3390/biomedicines11041224