
Countermovement Jumps Detect Subtle Motor Deficits in People with Multiple Sclerosis below the Clinical Threshold



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessments
2.2.1. Expanded Disability Status Scale (EDSS)
- (a)
- No disability in pyramidal FSS: pyramidal ≤ 1.
- (b)
- Normal sensory and cerebellar function: sensory FSS = 0 and cerebellar FSS = 0.
- (a)
- Participants with normal muscle strength: full strength in all assessed muscle groups of the lower extremity.
- (b)
- Participants with reduced muscle strength: not full strength in one or more muscle groups of the lower extremity.
- (a)
- Participants with monopedal hopping unimpaired: normal, 10 jumps performed on one leg right and left.
- (b)
- Participants with monopedal hopping impaired: less than 10 jumps on one or both legs.
2.2.2. Godin Leisure Time Exercise Questionnaire (GLTEQ)
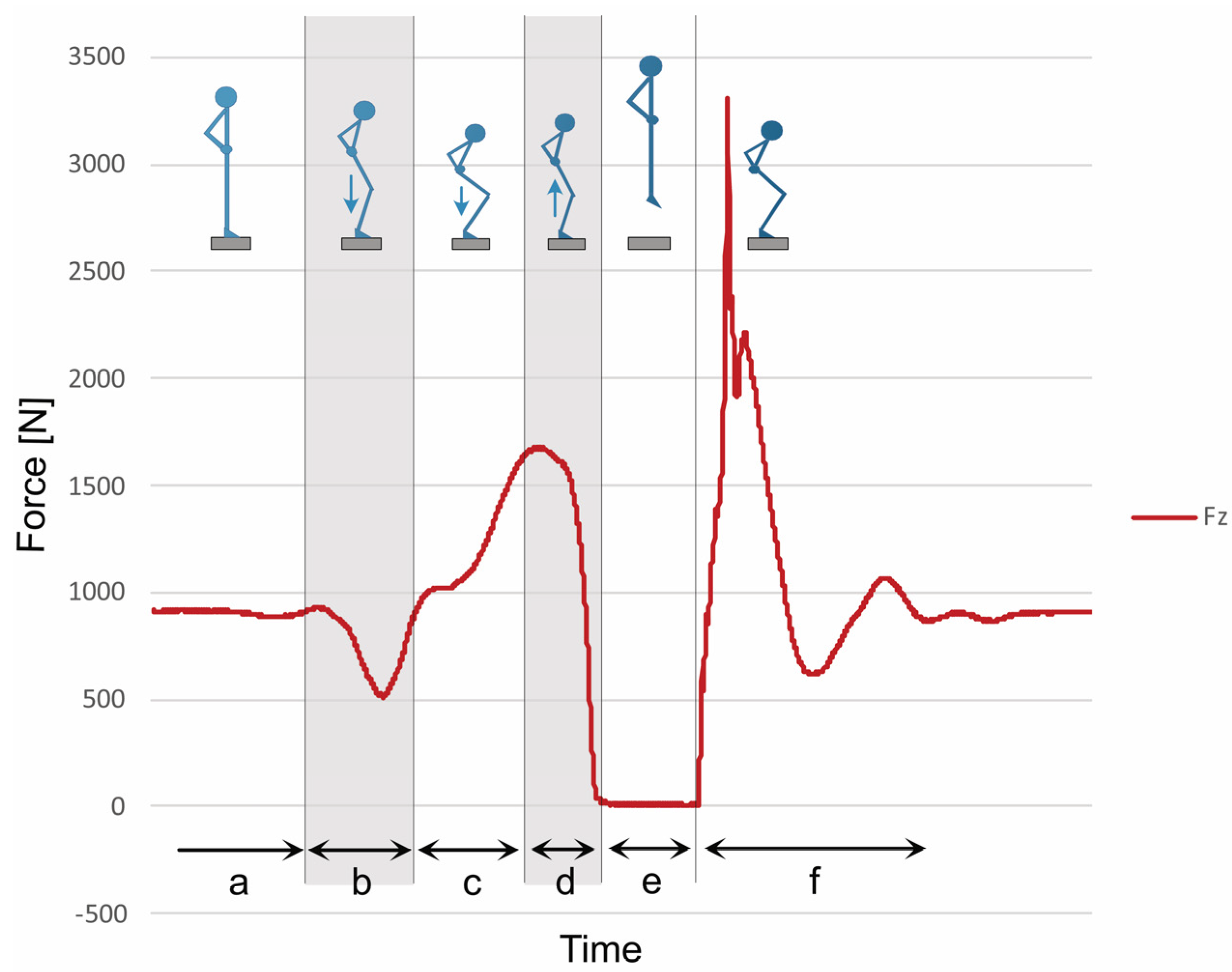
2.2.3. Countermovement Jump (CMJ)
2.3. Data Collection
2.4. Statistical Analysis
3. Results
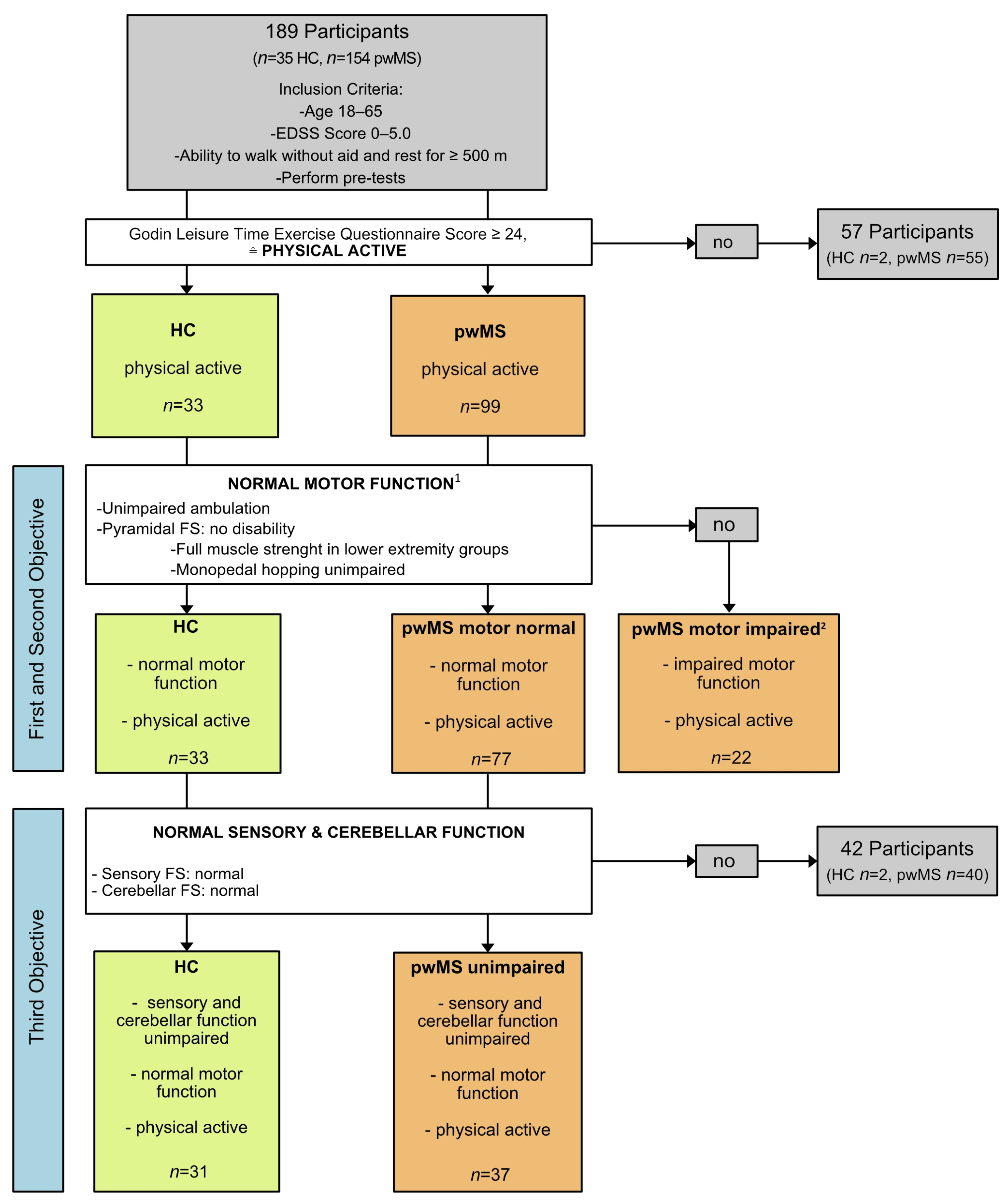
3.1. Participants
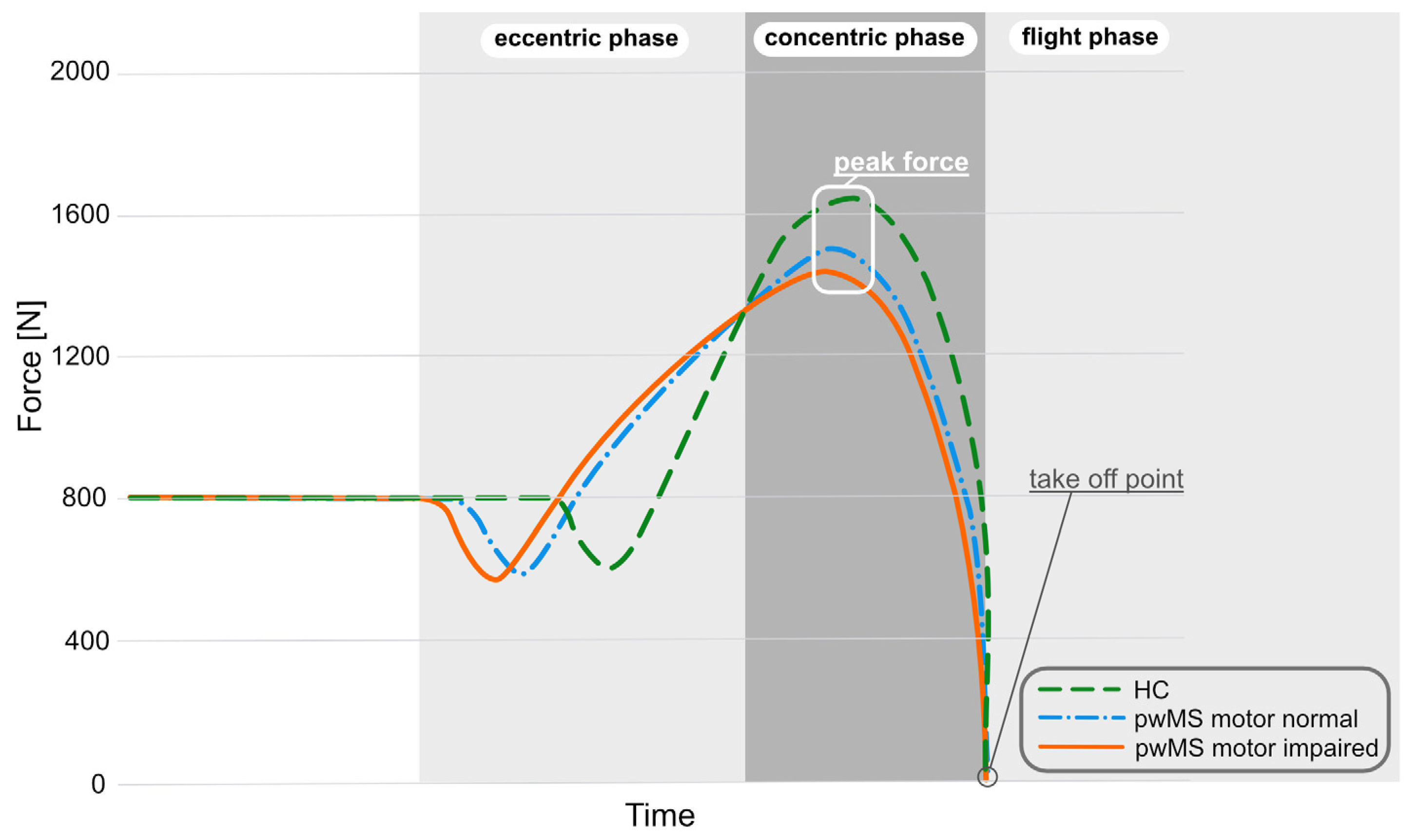
3.2. Group Comparison between MS Groups and HC in CMJ Performance
3.3. Group Comparision between pwMS with Normal Motor Function and HC
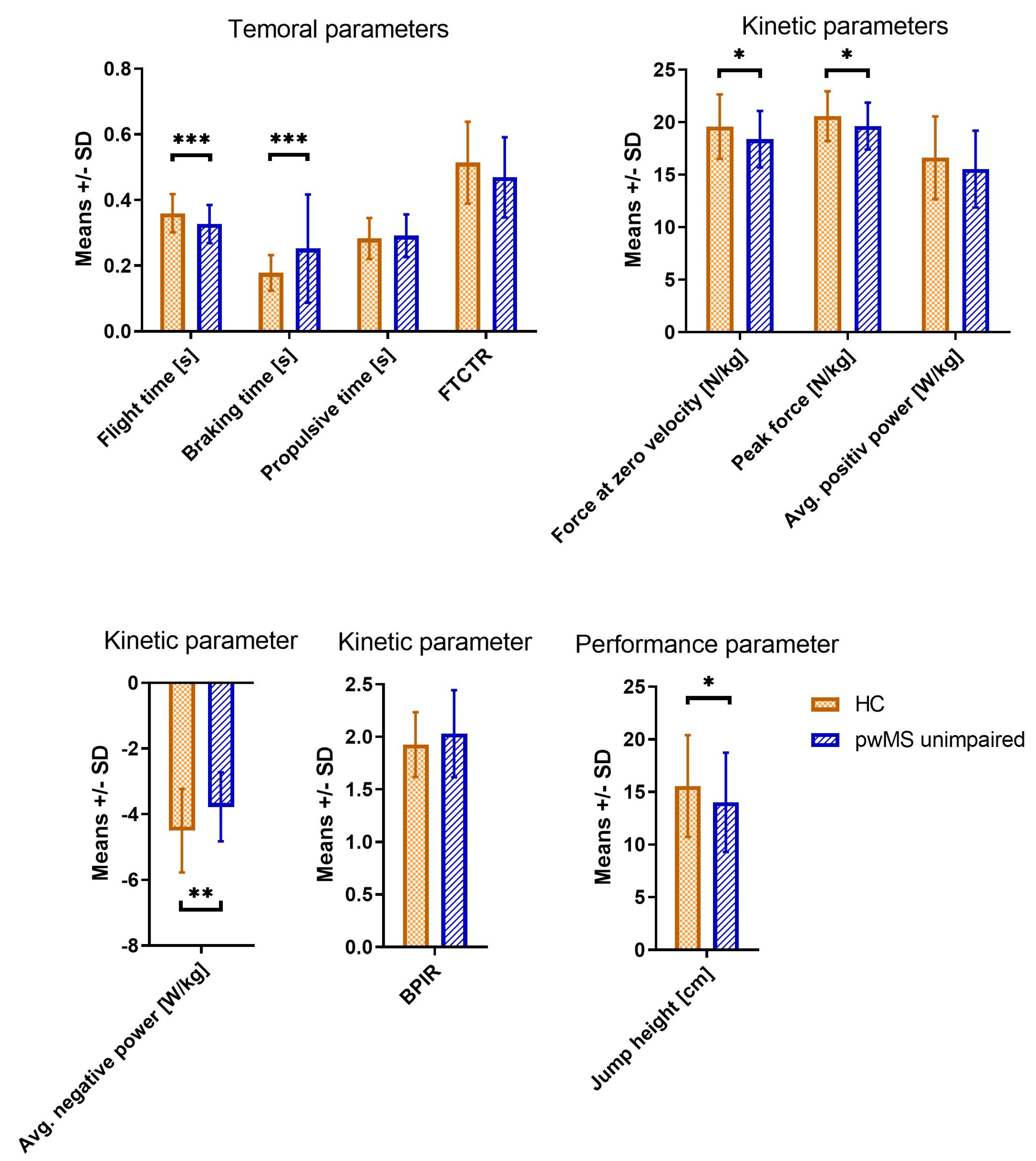
3.4. Group Comparision between HC and pwMS with Full Motor, Sensory and Cerebellar Function
3.5. Correlation of Jump Parameters According to EDSS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Goldenberg, M.M. Multiple Sclerosis Review. Pharm. Ther. 2012, 37, 175–184. [Google Scholar]
- Ziemssen, T.; Kern, R.; Thomas, K. Multiple sclerosis: Clinical profiling and data collection as prerequisite for personalized medicine approach. BMC Neurol. 2016, 16, 124. [Google Scholar] [CrossRef] [Green Version]
- Reuben, D.B.; Magasi, S.; McCreath, H.E.; Bohannon, R.W.; Wang, Y.-C.; Bubela, D.J.; Rymer, W.Z.; Beaumont, J.; Rine, R.M.; Lai, J.-S.; et al. Motor assessment using the NIH Toolbox. Neurology 2013, 80, S65–S75. [Google Scholar] [CrossRef] [Green Version]
- Kirkland, M.C.; Wadden, K.P.; Ploughman, M. Bipedal hopping as a new measure to detect subtle sensorimotor impairment in people with multiple sclerosis. Disabil. Rehabil. 2020, 44, 1544–1555. [Google Scholar] [CrossRef]
- Ziemssen, T.; De Stefano, N.; Sormani, M.P.; Van Wijmeersch, B.; Wiendl, H.; Kieseier, B.C. Optimizing therapy early in multiple sclerosis: An evidence-based view. Mult. Scler. Relat. Disord. 2015, 4, 460–469. [Google Scholar] [CrossRef] [Green Version]
- Ziemssen, T.; Derfuss, T.; de Stefano, N.; Giovannoni, G.; Palavra, F.; Tomic, D.; Vollmer, T.; Schippling, S. Optimizing treatment success in multiple sclerosis. J. Neurol. 2015, 263, 1053–1065. [Google Scholar] [CrossRef] [Green Version]
- Francis, D.A.; Bain, P.; Swan, A.V.; Hughes, R.A.C. An Assessment of Disability Rating Scales Used in Multiple Sclerosis. Arch. Neurol. 1991, 48, 299–301. [Google Scholar] [CrossRef]
- Krieger, S.C.; Antoine, A.; Sumowski, J.F. EDSS 0 is not normal: Multiple sclerosis disease burden below the clinical threshold. Mult. Scler. J. 2022, 28, 2299–2303. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [Green Version]
- Van Hooren, B.; Zolotarjova, J. The Difference Between Countermovement and Squat Jump Performances: A Review of Underlying Mechanisms With Practical Applications. J. Strength Cond. Res. 2017, 31, 2011–2020. [Google Scholar] [CrossRef] [Green Version]
- Quagliarella, L.; Sasanelli, N.; Belgiovine, G.; Accettura, D.; Notarnicola, A.; Moretti, B. Evaluation of counter movement jump parameters in young male soccer players. J. Appl. Biomater. Funct. Mater. 2011, 9, 40–46. [Google Scholar] [CrossRef]
- Gannon, E.A.; Higham, D.G.; Gardner, B.W.; Nan, N.; Zhao, J.; Bisson, L.J. Changes in Neuromuscular Status Across a Season of Professional Men’s Ice Hockey. J. Strength Cond. Res. 2021, 35, 1338–1344. [Google Scholar] [CrossRef]
- Helland, C.; Midttun, M.; Saeland, F.; Haugvad, L.; Olstad, D.S.; Solberg, P.A.; Paulsen, G. A strength-oriented exercise session required more recovery time than a power-oriented exercise session with equal work. PeerJ 2020, 8, e10044. [Google Scholar] [CrossRef]
- Lombard, W.; Reid, S.; Pearson, K.; Lambert, M. Reliability of metrics associated with a counter-movement jump performed on a force plate. Meas. Phys. Educ. Exerc. Sci. 2017, 21, 235–243. [Google Scholar] [CrossRef]
- Aragón, L.F. Evaluation of Four Vertical Jump Tests: Methodology, Reliability, Validity, and Accuracy. Meas. Phys. Educ. Exerc. Sci. 2000, 4, 215–228. [Google Scholar] [CrossRef] [Green Version]
- Slinde, F.; Suber, C.; Suber, L.; Edwén, C.E.; Svantesson, U. Test-Retest Reliability of Three Different Countermovement Jumping Tests. J. Strength Cond. Res. 2008, 22, 640–644. [Google Scholar] [CrossRef]
- Hori, N.; Newton, R.U.; Kawamori, N.; McGuigan, M.R.; Kraemer, W.J.; Nosaka, K. Reliability of Performance Measurements Derived From Ground Reaction Force Data During Countermovement Jump and the Influence of Sampling Frequency. J. Strength Cond. Res. 2009, 23, 874–882. [Google Scholar] [CrossRef] [Green Version]
- Meylan, C.; McMaster, T.; Cronin, J.; Mohammad, N.I.; Rogers, C.; Deklerk, M. Single-Leg Lateral, Horizontal, and Vertical Jump Assessment: Reliability, Interrelationships, and Ability to Predict Sprint and Change-of-Direction Performance. J. Strength Cond. Res. 2009, 23, 1140–1147. [Google Scholar] [CrossRef]
- Rauch, R.; Veilleux, L.; Rauch, F.; Bock, D.; Welisch, E.; Filler, G.; Robinson, T.; Burrill, E.; Norozi, K.R. Muscle force and power in obese and overweight children. J. Musculoskelet. Neuronal Interact. 2012, 12, 80–83. [Google Scholar]
- Singh, H.; Kim, D.; Kim, E.; Bemben, M.G.; Anderson, M.; Seo, D.-I.; Bemben, D.A. Jump Test Performance and Sarcopenia Status in Men and Women, 55 to 75 Years of Age. J. Geriatr. Phys. Ther. 2014, 37, 76–82. [Google Scholar] [CrossRef]
- Kirkland, M.C.; Downer, M.B.; Holloway, B.J.; Wallack, E.M.; Lockyer, E.J.; Buckle, N.C.M.; Abbott, C.L.; Ploughman, M. Bipedal Hopping Reveals Evidence of Advanced Neuromuscular Aging Among People With Mild Multiple Sclerosis. J. Mot. Behav. 2016, 49, 505–513. [Google Scholar] [CrossRef] [PubMed]
- Kirkland, M.C.; Chen, A.; Downer, M.B.; Holloway, B.J.; Wallack, E.M.; Lockyer, E.J.; Buckle, N.C.; Abbott, C.L.; Ploughman, M. Bipedal hopping timed to a metronome to detect impairments in anticipatory motor control in people with mild multiple sclerosis. Clin. Biomech. 2018, 55, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Van Munster, C.E.P.; Uitdehaag, B.M.J. Outcome Measures in Clinical Trials for Multiple Sclerosis. CNS Drugs 2017, 31, 217–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vanhoutte, E.K.; Faber, C.G.; Van Nes, S.I.; Jacobs, B.C.; Van Doorn, P.A.; Van Koningsveld, R.; Cornblath, D.R.; Van Der Kooi, A.J.; Cats, E.A.; Berg, L.H.V.D.; et al. Modifying the Medical Research Council grading system through Rasch analyses. Brain 2011, 135, 1639–1649. [Google Scholar] [CrossRef] [Green Version]
- Godin, G. The Godin-Shephard Leisure-Time Physical Activity Questionnaire. Health Fit. J. Can. 2011, 4, 18–22. [Google Scholar] [CrossRef]
- Yingling, V.R.; Castro, D.A.; Duong, J.T.; Malpartida, F.J.; Usher, J.R.; Jenny, O. The Reliability of Vertical Jump Tests between the Vertec and My Jump Phone Application. PeerJ 2018, 6, e4669. [Google Scholar] [CrossRef] [Green Version]
- Kershner, A.L.; Fry, A.C.; Cabarkapa, D. Effect of Internal vs. External Focus of Attention Instructions on Countermovement Jump Variables in NCAA Division I Student-Athletes. J. Strength Cond. Res. 2019, 33, 1467–1473. [Google Scholar] [CrossRef] [PubMed]
- Ruffieux, J.; Wälchli, M.; Kim, K.-M.; Taube, W. Countermovement Jump Training Is More Effective Than Drop Jump Training in Enhancing Jump Height in Non-professional Female Volleyball Players. Front. Physiol. 2020, 11, 231. [Google Scholar] [CrossRef]
- McMahon, J.J.; Suchomel, T.J.; Lake, J.P.; Comfort, P. Understanding the Key Phases of the Countermovement Jump Force-Time Curve. Strength Cond. J. 2018, 40, 96–106. [Google Scholar] [CrossRef] [Green Version]
- Buckthorpe, M.; Morris, J.; Folland, J.P. Validity of vertical jump measurement devices. J. Sports Sci. 2012, 30, 63–69. [Google Scholar] [CrossRef]
- Cronin, J.B.; Hing, R.D.; McNair, P.J. Reliability and Validity of a Linear Position Transducer for Measuring Jump Performance. J. Strength Cond. Res. 2004, 18, 590–593. [Google Scholar] [CrossRef] [PubMed]
- Koltermann, J.J.; Gerber, M.; Beck, H.; Beck, M. Validation of the HUMAC Balance System in Comparison with Conventional Force Plates. Technologies 2017, 5, 44. [Google Scholar] [CrossRef] [Green Version]
- Eagles, A.N.; Sayers, M.G.L.; Bousson, M.; Lovell, D.I. Current Methodologies and Implications of Phase Identification of the Vertical Jump: A Systematic Review and Meta-analysis. Sports Med. 2015, 45, 1311–1323. [Google Scholar] [CrossRef]
- Gathercole, R.; Sporer, B.; Stellingwerff, T.; Sleivert, G. Alternative Countermovement-Jump Analysis to Quantify Acute Neuromuscular Fatigue. Int. J. Sports Physiol. Perform. 2015, 10, 84–92. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Markovic, G.; Dizdar, D.; Jukic, I.; Cardinale, M. Reliability and Factorial Validity of Squat and Countermovement Jump Tests. J. Strength Cond. Res. 2004, 18, 551–555. [Google Scholar] [CrossRef] [PubMed]
- Riemenschneider, M.; Hvid, L.G.; Stenager, E.; Dalgas, U. Is there an overlooked “window of opportunity” in MS exercise therapy? Perspectives for early MS rehabilitation. Mult. Scler. J. 2018, 24, 886–894. [Google Scholar] [CrossRef]
- Aeles, J.; Vanwanseele, B. Do Stretch-Shortening Cycles Really Occur in the Medial Gastrocnemius? A Detailed Bilateral Analysis of the Muscle-Tendon Interaction During Jumping. Front. Physiol. 2019, 10, 1504. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Jump Parameters | Description | Interpretation |
|---|---|---|
| Temporal parameters | ||
| Flight time (s) | time in the air from jump take-off to landing | longer = better |
| Braking time (s) | duration of the eccentric phase | shorter = better |
| Propulsive time (s) | duration of the concentric phase | shorter = better |
| FTCTR | ratio of flight to contraction time | higher = better |
| Kinetic parameters | ||
| FZV (N/kg) | maximum force during eccentric phase | higher = better |
| Peak force (N/kg) | maximum force during concentric phase | higher = better |
| ANP (W/kg) APP (W/kg) | average power during eccentric phase average power during concentric phase | higher = better higher = better |
| BPIR | ratio of braking to propulsive impulse | lower = better |
| Performance parameter | ||
| Jump height (cm) | jump height calculated by force impact | higher = better |
| HC (n = 33) | pwMS Motor Normal (n = 77) | pwMS Motor Impaired (n = 22) | |
|---|---|---|---|
| Age (years) | 34.82 (±9.68) a | 35.86 (±8.83) a | 41.91 (±10.63) |
| Gender (female) n (%) | 21 (63.6%) | 54 (70.1%) | 16 (72.7%) |
| Disease duration (years) | n.a | 7.05 (±5.86) | 9.27 (±6.63) |
| MS Subtype | |||
| RRMS (%) | n.a | 100% | 100% |
| BMI EDSS (median, IQR) | 24.95 (±4.97) 1.0 (0–1.0) a | 24.58 (±4.26) 1.5 (1.0–1.5) a | 25.63 (±5.26) 3.0 (2.5–3.5) |
| Pyramidal FSS | 1.0 (0–1.0) a | 1.0 (1.0–1.0) a | 2.0 (2.0–2.5) |
| Cerebellar FSS | 0 (0–0) a | 0 (0–1.0) a | 1.0 (1.0–2.0) |
| Sensory FSS | 0 (0–0) a | 0 (0–1.0) a | 1.5 (1.0–2.0) |
| Jump Parameters | HC (n = 33) | pwMS Motor Normal (n = 77) | pwMS Motor Impaired (n = 22) | F (2,126) | p-Value |
|---|---|---|---|---|---|
| Temporal parameters | |||||
| Flight time (s) | 0.36 ± 0.06 b,c | 0.32 ± 0.05 a,c | 0.27 ± 0.06 a,b | 22.24 | <0.001 * |
| Braking time (s) | 0.18 ± 0.05 b,c | 0.25 ± 0.15 a | 0.30 ± 0.19 a | 9.49 | <0.001 * |
| Propulsive time (s) | 0.28 ± 0.06 c | 0.30 ± 0.07 c | 0.43 ± 0.19 a,b | 10.57 | <0.001 * |
| FTCTR | 0.51 ± 0.12 b,c | 0.45 ± 0.11 a,c | 0.34 ± 0.12 a,b | 11.86 | <0.001 * |
| Kinetic parameters | |||||
| FZV (N/kg) | 19.61 ± 3.0 b,c | 17.52 ± 2.93 a,c | 14.99 ± 3.63 a,b | 11.43 | <0.001 * |
| Peak force (N/kg) | 20.57 ± 2.30 b,c | 19.34 ± 2.18 a | 17.92 ± 2.69 a | 5.711 | 0.004 * |
| ANP (W/kg) | −4.53 ± 3.86 b,c | −3.41 ± 1.07 a,c | −2.29 ± 0.89 a,b | 10.66 | <0.001 * |
| APP (W/kg) BPIR | 16.38 ± 3.86 b,c 1.92 ± 0.31 b,c | 15.08 ± 3.22 a,c 2.29 ± 1.14 a,c | 11.51 ± 3.76 a,b 2.29 ± 1.14 a,b | 25.56 13.71 | <0.001 * <0.001 * |
| Performance parameter | |||||
| Jump height (cm) | 15.38 ± 4.78 c | 13.73 ± 4.28 | 11.03 ± 5.22 a | 3.07 | 0.050 |
| Jump Parameters | EDSS | Pyramidal FSS | Cerebellar FSS | Sensory FSS |
|---|---|---|---|---|
| Temporal parameters | ||||
| Flight time (s) | −0.295 ** | −0.382 ** | −0.263 ** | −0.248 ** |
| Braking time (s) | 0.125 | 0.290 ** | 0.149 | −0.68 |
| Propulsive time (s) | 0.225 * | 0.267 ** | 0.337 ** | 0.143 |
| FTCTR | −0.338 ** | −0.391 ** | −0.405 ** | −0.188 |
| Kinetic parameters | ||||
| FZV (N/kg) | −0.299 ** | −0.336 ** | −0.417 ** | −0.239 * |
| Peak force (N/kg) | −0.249 * | −0.305 ** | −0.348 ** | −0.163 |
| ANP (W/kg) | 0.385 ** | 0.421 ** | 0.408 ** | 0.354** |
| APP (W/kg) BPIR | −0.374 ** 0.274 | −0.440 ** 0.283 ** | −0.358 ** 0.314 ** | −0.203 * 0.325 ** |
| Performance parameter | ||||
| Jump height (cm) | −0.248 * | −0.275 ** | −0.108 | −0.166 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Geßner, A.; Stölzer-Hutsch, H.; Trentzsch, K.; Schriefer, D.; Ziemssen, T. Countermovement Jumps Detect Subtle Motor Deficits in People with Multiple Sclerosis below the Clinical Threshold. Biomedicines 2023, 11, 774. https://doi.org/10.3390/biomedicines11030774
Geßner A, Stölzer-Hutsch H, Trentzsch K, Schriefer D, Ziemssen T. Countermovement Jumps Detect Subtle Motor Deficits in People with Multiple Sclerosis below the Clinical Threshold. Biomedicines. 2023; 11(3):774. https://doi.org/10.3390/biomedicines11030774
Chicago/Turabian StyleGeßner, Anne, Heidi Stölzer-Hutsch, Katrin Trentzsch, Dirk Schriefer, and Tjalf Ziemssen. 2023. "Countermovement Jumps Detect Subtle Motor Deficits in People with Multiple Sclerosis below the Clinical Threshold" Biomedicines 11, no. 3: 774. https://doi.org/10.3390/biomedicines11030774