
Bacterial and Viral Infection and Sepsis in Kidney Transplanted Patients

 , , , and
, , , and
Abstract
:1. Introduction
2. General Considerations about Infection in Kidney Transplanted Patients
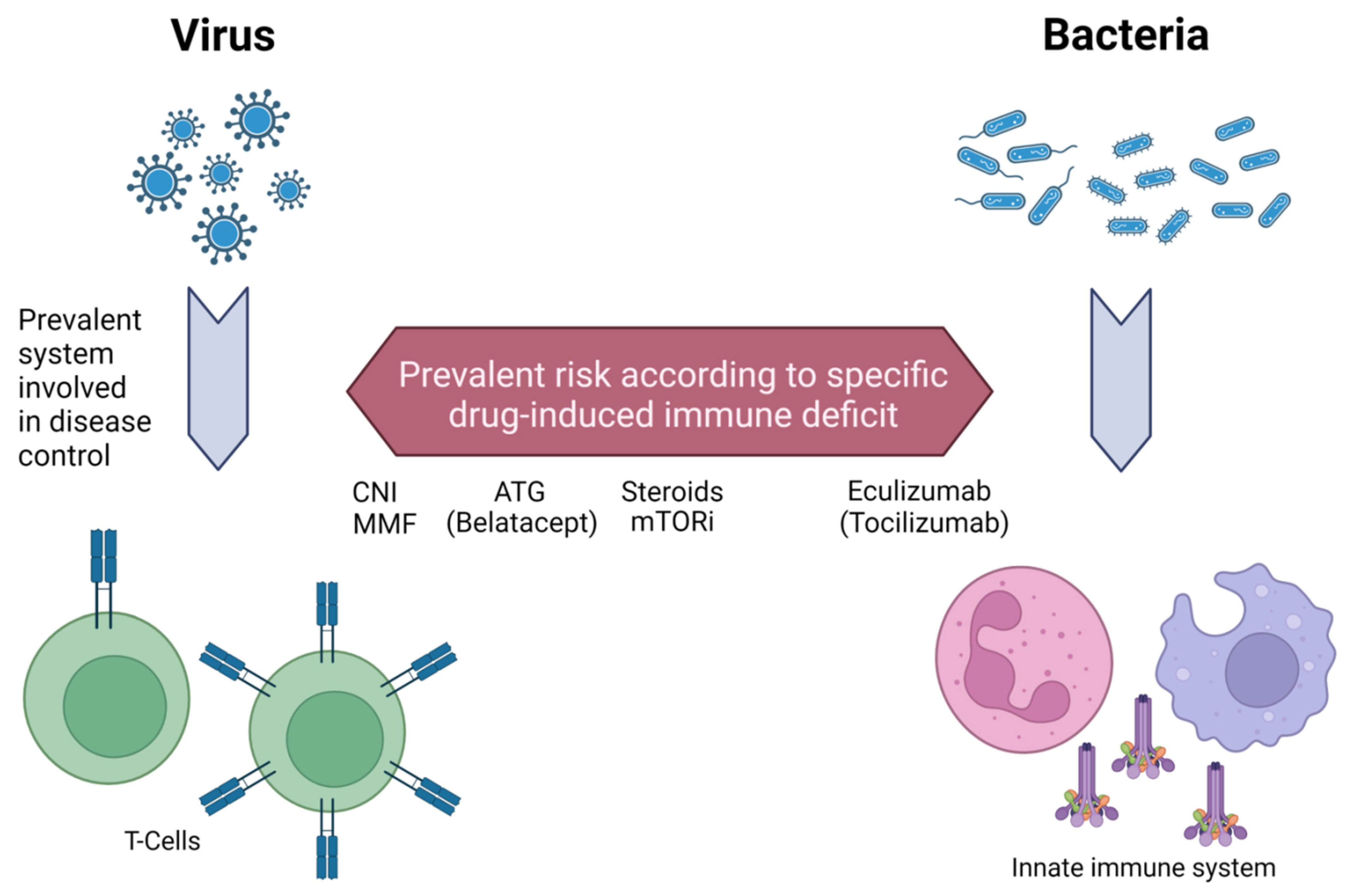
3. Immunosuppressants Role and Selective Immunosuppression Load
4. Bacterial Infections
4.1. Urinary Tract Infections
4.2. Respiratory Infections
4.3. Mycobacteria
4.4. Nocardia Species
4.5. Listeria Monocytogenes
5. Viral Infections
5.1. Cytomegalovirus
5.2. Polyomaviruses
5.3. Epstein-Barr Virus
5.4. Other Common Herpes Viruses (Herpes Simplex and Varicella Zoster Viruses)
5.5. Therapeutic Advances: HBV, HCV, and HIV
5.6. Emergent Issue: West-Nile Virus
6. Sepsis in Kidney Transplanted Patients

{kind=link}
| Bacterial Infections | Viral Infections |
|---|---|
| Urinary tract infection (UTI) [65,154] | Citomegalovirus (CMV) [46,103] |
|
|
| Respiratory tract infection (pneumonia) [67] | Polyomavirus (BK) [109] |
|
|
| Tubercolosis [79,86,87] | Epstein-Barr Virus (EBV) [120] |
|
|
| Nocardia [92] | Herpesviridae (HSV-1,2 [120] and VZV [131]) |
|
|
| Listeria [98,99] | West-Nile virus [140] |
|
|
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fishman, J.A. Infection in Organ Transplantation. Am. J. Transplant. 2017, 17, 856–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karuthu, S.; Blumberg, E.A. Common infections in kidney transplant recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 2058–2070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cippà, P.E.; Schiesser, M.; Ekberg, H.; van Gelder, T.; Mueller, N.J.; Cao, C.A.; Fehr, T.; Bernasconi, C. Risk stratification for rejection and infection after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2015, 10, 2213–2220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinnunen, S.; Karhapää, P.; Juutilainen, A.; Finne, P.; Helanterä, I. Secular trends in infection-related mortality after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2018, 13, 755–762. [Google Scholar] [CrossRef]
- Fishman, J.A. Infection in solid-organ transplant recipients. N. Engl. J. Med. 2007, 357, 2601–2614. [Google Scholar] [CrossRef] [Green Version]
- Roberts, M.B.; Fishman, J.A. Immunosuppressive Agents and Infectious Risk in Transplantation: Managing the “Net State of Immunosuppression”. Clin. Infect. Dis. 2021, 73, e1302–e1317. [Google Scholar] [CrossRef]
- Iglesias, J.; Ledesma, K.J.; Couto, P.J.; Liu, J. Immune Reconstitution Inflammatory Syndrome Occurring in a Kidney Transplant Patient with Extrapulmonary Tuberculosis. Case Rep. Transplant. 2017, 2017, 6290987. [Google Scholar] [CrossRef] [Green Version]
- Nelson, C.A.; Zunt, J.R. Tuberculosis of the central nervous system in immunocompromised patients: HIV infection and solid organ transplant recipients. Clin. Infect. Dis. 2011, 53, 915–926. [Google Scholar] [CrossRef] [Green Version]
- Webster, A.C.; Wu, S.; Tallapragada, K.; Park, M.Y.; Chapman, J.R.; Carr, S.J. Polyclonal and monoclonal antibodies for treating acute rejection episodes in kidney transplant recipients. Cochrane Database Syst. Rev. 2017, 7, CD004756. [Google Scholar] [CrossRef]
- Pham, C.; Kuten, S.A.; Knight, R.J.; Nguyen, D.T.; Graviss, E.A.; Gaber, A.O. Assessment of infectious complications in elderly kidney transplant recipients receiving induction with anti-thymocyte globulin vs. basiliximab. Transpl. Infect. Dis. 2020, 22, e13257. [Google Scholar] [CrossRef]
- Clark, R.; Gallin, J.; Fauci, A. Effects of in vivo prednisone on in vitro eosinophil and neutrophil adherence and chemotaxis. Blood 1979, 53, 633–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cain, D.W.; Cidlowski, J.A. Immune regulation by glucocorticoids. Nat. Rev. Immunol. 2017, 17, 233–247. [Google Scholar] [CrossRef] [PubMed]
- Ritter, M.L.; Pirofski, L. Mycophenolate mofetil: Effects on cellular immune subsets, infectious complications, and antimicrobial activity: Review article. Transpl. Infect. Dis. 2009, 11, 290–297. [Google Scholar] [CrossRef] [Green Version]
- Gummert, J.F.; Barten, M.J.; Sherwood, S.W.; Van Gelder, T.; Morris, R.E. Pharmacodynamics of immunosuppression by mycophenolic acid: Inhibition of both lymphocyte proliferation and activation correlates with pharmacokinetics. J. Pharmacol. Exp. Ther. 1999, 291, 1100–1112. [Google Scholar] [PubMed]
- Halloran, P.F. Mechanism of action of the calcineurin inhibitors. Transplant. Proc. 2001, 33, 3067–3069. [Google Scholar] [CrossRef]
- Tsuda, K.; Yamanaka, K.; Kitagawa, H.; Akeda, T.; Naka, M.; Niwa, K.; Nakanishi, T.; Kakeda, M.; Gabazza, E.C.; Mizutani, H. Calcineurin inhibitors suppress cytokine production from memory T cells and differentiation of naïve T cells into cytokine-producing mature T cells. PLoS ONE 2012, 7, e31465. [Google Scholar] [CrossRef]
- Scottà, C.; Fanelli, G.; Hoong, S.J.; Romano, M.; Lamperti, E.N.; Sukthankar, M.; Guggino, G.; Fazekasova, H.; Ratnasothy, K.; Becker, P.D.; et al. Impact of immunosuppressive drugs on the therapeutic efficacy of ex vivo expanded human regulatory T cells. Haematologica 2016, 101, 91–100. [Google Scholar] [CrossRef]
- Riella, L.V.; Alegre, M.L. Novel Role of Calcineurin Inhibitors in Curbing T Cells’ Sweet Tooth. Am. J. Transplant. 2018, 18, 3. [Google Scholar] [CrossRef] [Green Version]
- Baan, C.C.; Van Der Mast, B.J.; Klepper, M.; Mol, W.M.; Peeters, A.M.A.; Korevaar, S.S.; Balk, A.H.M.M.; Weimar, W. Differential effect of calcineurin inhibitors, anti-CD25 antibodies and rapamycin on the induction of FOXP3 in human T cells. Transplantation 2005, 80, 110–117. [Google Scholar] [CrossRef]
- Emal, D.; Rampanelli, E.; Claessen, N.; Bemelman, F.J.; Leemans, J.C.; Florquin, S.; Dessing, M.C. Calcineurin inhibitor Tacrolimus impairs host immune response against urinary tract infection. Sci. Rep. 2019, 9, 106. [Google Scholar] [CrossRef] [Green Version]
- Howell, J.; Sawhney, R.; Testro, A.; Skinner, N.; Gow, P.; Angus, P.; Ratnam, D.; Visvanathan, K. Cyclosporine and tacrolimus have inhibitory effects on toll-like receptor signaling after liver transplantation. Liver Transpl. 2013, 10, 1099–1107. [Google Scholar] [CrossRef]
- Ventura-Aguiar, P.; Campistol, J.M.; Diekmann, F. Safety of mTOR inhibitors in adult solid organ transplantation. Expert Opin. Drug Saf. 2016, 15, 303–319. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zhou, X. Research progress of mTOR inhibitors. Eur. J. Med. Chem. 2020, 208, 112820. [Google Scholar] [CrossRef] [PubMed]
- Gee, I.; Trull, A.K.; Charman, S.C.; Alexander, G.J.M. Sirolimus inhibits oxidative burst activity in transplant recipients. Transplantation 2003, 76, 1766–1768. [Google Scholar] [CrossRef] [PubMed]
- Mella, A.; Messina, M.; Ranghino, A.; Solidoro, P.; Tabbia, G.; Segoloni, G.P.; Biancone, L. Pulmonary toxicity in a renal transplant recipient treated with amiodarone and everolimus: A case of hypothetical synergy and a proposal for a screening protocol. Case Rep. Neurol. 2014, 4, 75–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pascual, J.; Royuela, A.; Fernández, A.M.; Herrero, I.; Delgado, J.F.; Solé, A.; Guirado, L.; Serrano, T.; de la Torre-Cisneros, J.; Moreno, A.; et al. Role of mTOR inhibitors for the control of viral infection in solid organ transplant recipients. Transpl. Infect. Dis. 2016, 18, 819–831. [Google Scholar] [CrossRef]
- Cooper, N.; Arnold, D.M. The effect of rituximab on humoral and cell mediated immunity and infection in the treatment of autoimmune diseases. Br. J. Haematol. 2010, 149, 3–13. [Google Scholar] [CrossRef]
- Leibler, C.; Thiolat, A.; Hénique, C.; Samson, C.; Pilon, C.; Tamagne, M.; Pirenne, F.; Vingert, B.; Cohen, J.L.; Grimbert, P. Control of humoral response in renal transplantation by belatacept depends on a direct effect on B cells and impaired T follicular helper-B cell crosstalk. J. Am. Soc. Nephrol. 2018, 29, 1049–1062. [Google Scholar] [CrossRef]
- Cortés-Hernández, A.; Alvarez-Salazar, E.; Arteaga-Cruz, S.; Alberu-Gómez, J.; Soldevila, G. Ex vivo expansion of regulatory T cells from long-term Belatacept-treated kidney transplant patients restores their phenotype and suppressive function but not their FOXP3 TSDR demethylation status. Cell. Immunol. 2020, 348, 104044. [Google Scholar] [CrossRef]
- Moots, R.J.; Sebba, A.; Rigby, W.; Ostor, A.; Porter-Brown, B.; Donaldson, F.; Dimonaco, S.; Rubbert-Roth, A.; van Vollenhoven, R.; Genovese, M.C. Effect of tocilizumab on neutrophils in adult patients with rheumatoid arthritis: Pooled analysis of data from phase 3 and 4 clinical trials. Rheumatology 2017, 56, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Gaber, T.; Hahne, M.; Strehl, C.; Hoff, P.; Dörffel, Y.; Feist, E.; Burmester, G.R.; Buttgereit, F. Disentangling the effects of tocilizumab on neutrophil survival and function. Immunol. Res. 2016, 64, 665–676. [Google Scholar] [CrossRef] [PubMed]
- Doberer, K.; Duerr, M.; Halloran, P.F.; Eskandary, F.; Budde, K.; Regele, H.; Reeve, J.; Borski, A.; Kozakowski, N.; Reindl-Schwaighofer, R.; et al. A randomized clinical trial of anti⇓IL-6 antibody clazakizumab in late antibody-mediated kidney transplant rejection. J. Am. Soc. Nephrol. 2021, 32, 708–722. [Google Scholar] [CrossRef] [PubMed]
- Benamu, E.; Montoya, J.G. Infections associated with the use of eculizumab: Recommendations for prevention and prophylaxis. Curr. Opin. Infect. Dis. 2016, 29, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Bozio, C.H.; Isenhour, C.; McNamara, L.A. Characteristics of and meningococcal disease prevention strategies for commercially insured persons receiving eculizumab in the United States. PLoS ONE 2020, 15, 1–12. [Google Scholar] [CrossRef]
- Ling, X.; Xiong, J.; Liang, W.; Schroder, P.M.; Wu, L.; Ju, W.; Kong, Y.; Shang, Y.; Guo, Z.; He, X. Can immune cell function assay identify patients at risk of infection or rejection? A meta-analysis. Transplantation 2012, 93, 737–743. [Google Scholar] [CrossRef]
- Pérez-Jacoiste Asín, M.A.; Fernández-Ruiz, M.; López-Medrano, F.; Aquilino, C.; González, E.; Ruiz-Merlo, T.; Gutiérrez, E.; San Juan, R.; Paz-Artal, E.; Andrés, A.; et al. Monitoring of intracellular adenosine triphosphate in CD4+ T cells to predict the occurrence of cytomegalovirus disease in kidney transplant recipients. Transpl. Int. 2016, 29, 1094–1105. [Google Scholar] [CrossRef] [Green Version]
- Mian, M.; Natori, Y.; Ferreira, V.; Selzner, N.; Husain, S.; Singer, L.; Kim, S.J.; Humar, A.; Kumar, D. Evaluation of a Novel Global Immunity Assay to Predict Infection in Organ Transplant Recipients. Clin. Infect. Dis. 2018, 66, 1392–1397. [Google Scholar] [CrossRef] [Green Version]
- Blazik, M.; Hutchinson, P.; Jose, M.D.; Polkinghorne, K.R.; Holdsworth, S.R.; Atkins, R.C.; Chadban, S.J. Leukocyte phenotype and function predicts infection risk in renal transplant recipients. Nephrol. Dial. Transplant. 2005, 20, 2226–2230. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Ruiz, M.; López-Medrano, F.; Allende, L.M.; San Juan, R.; Andrés, A.; Aguado, J.M. Immune risk phenotype in kidney transplant recipients: A reliable surrogate for premature immune senescence and increased susceptibility to infection? Transpl. Infect. Dis. 2016, 18, 968–970. [Google Scholar] [CrossRef]
- Maggi, F.; Focosi, D.; Statzu, M.; Bianco, G.; Costa, C.; Macera, L.; Spezia, P.G.; Medici, C.; Albert, E.; Navarro, D.; et al. Early Post-Transplant Torquetenovirus Viremia Predicts Cytomegalovirus Reactivations In Solid Organ Transplant Recipients. Sci. Rep. 2018, 8, 6–13. [Google Scholar] [CrossRef]
- Strassl, R.; Schiemann, M.; Doberer, K.; Görzer, I.; Puchhammer-Stöckl, E.; Eskandary, F.; Kikić, Ž.; Gualdoni, G.A.; Vossen, M.G.; Rasoul-Rockenschaub, S.; et al. Quantification of torque teno virus viremia as a prospective biomarker for infectious disease in kidney allograft recipients. J. Infect. Dis. 2018, 218, 1191–1199. [Google Scholar] [CrossRef] [PubMed]
- Sen, P.; Wilkie, A.R.; Ji, F.; Yang, Y.; Taylor, I.J.; Velazquez-Palafox, M.; Vanni, E.A.H.; Pesola, J.M.; Fernandez, R.; Chen, H.; et al. Linking indirect effects of cytomegalovirus in transplantation to modulation of monocyte innate immune function. Sci. Adv. 2020, 6, eaax9856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haidar, G.; Boeckh, M.; Singh, N. Cytomegalovirus infection in solid organ and hematopoietic cell transplantation: State of the evidence. J. Infect. Dis. 2021, 221, S23–S31. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, H.; Fishman, J.A. The Cell Biology of Cytomegalovirus: Implications for Transplantation. Am. J. Transplant. 2016, 16, 2254–2269. [Google Scholar] [CrossRef]
- Hardinger, K.L.; Koch, M.J.; Bohl, D.J.; Storch, G.A.; Brennan, D.C. BK-virus and the impact of pre-emptive immunosuppression reduction: 5-year results. Am. J. Transplant. 2010, 10, 407–415. [Google Scholar] [CrossRef] [Green Version]
- Kotton, C.N.; Kumar, D.; Caliendo, A.M.; Huprikar, S.; Chou, S.; Danziger-Isakov, L.; Humar, A.; The Transplantation Society International CMV Consensus Group. The Third International Consensus Guidelines on the Management of Cytomegalovirus in Solid-Organ Transplantation. Transplantation 2018, 102, 900–931. [Google Scholar] [CrossRef] [Green Version]
- Alangaden, G.J.; Thyagarajan, R.; Gruber, S.A.; Morawski, K.; Garnick, J.; El-Amm, J.M.; West, M.S.; Sillix, D.H.; Chandrasekar, P.H.; Haririan, A. Infectious complications after kidney transplantation: Current epidemiology and associated risk factors. Clin. Transplant. 2006, 20, 401–409. [Google Scholar] [CrossRef]
- Pellé, G.; Vimont, S.; Levy, P.P.; Hertig, A.; Ouali, N.; Chassin, C.; Arlet, G.; Rondeau, E.; Vandewalle, A. Acute pyelonephritis represents a risk factor impairing long-term kidney graft function. Am. J. Transplant. 2007, 7, 899–907. [Google Scholar] [CrossRef]
- Bodro, M.; Linares, L.; Chiang, D.; Moreno, A.; Cervera, C. Managing recurrent urinary tract infections in kidney transplant patients. Expert Rev. Anti. Infect. Ther. 2018, 16, 723–732. [Google Scholar] [CrossRef]
- Lee, J.R.; Bang, H.; Dadhania, D.; Hartono, C.; Aull, M.J.; Satlin, M.; August, P.; Suthanthiran, M.; Muthukumar, T. Independent risk factors for urinary tract infection and for subsequent bacteremia or acute cellular rejection: A single-center report of 1166 kidney allograft recipients. Transplantation 2013, 96, 732–738. [Google Scholar] [CrossRef]
- Ariza-Heredia, E.J.; Beam, E.N.; Lesnick, T.G.; Cosio, F.G.; Kremers, W.K.; Razonable, R.R. Impact of urinary tract infection on allograft function after kidney transplantation. Clin. Transplant. 2014, 28, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Fiorentino, M.; Pesce, F.; Schena, A.; Simone, S.; Castellano, G.; Gesualdo, L. Updates on urinary tract infections in kidney transplantation. J. Nephrol. 2019, 32, 751–761. [Google Scholar] [CrossRef] [PubMed]
- Brennan, D.C.; Daller, J.A.; Lake, K.D.; Cibrik, D.; Del Castillo, D. Rabbit Antithymocyte Globulin versus Basiliximab in Renal Transplantation. N. Engl. J. Med. 2006, 355, 1967–1977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, J.H.; Cho, J.H.; Lee, J.H.; Park, Y.J.; Jin, S.; Park, G.Y.; Kim, J.S.; Kang, Y.J.; Kwon, O.; Choi, J.Y.; et al. Risk factors for recurrent urinary tract infection in kidney transplant recipients. Transplant. Proc. 2013, 45, 1584–1589. [Google Scholar] [CrossRef]
- López-Medrano, F.; García-Bravo, M.; Morales, J.M.; Andrés, A.; San Juan, R.; Lizasoain, M.; Aguado, J.M. Urinary tract infection due to Corynebacterium urealyticum in kidney transplant recipients: An underdiagnosed etiology for obstructive uropathy and graft dysfunction—Results of a prospective cohort study. Clin. Infect. Dis. 2008, 46, 825–830. [Google Scholar] [CrossRef] [Green Version]
- Abbo, L.M.; Grossi, P.A. Surgical site infections: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13589. [Google Scholar] [CrossRef]
- Goldman, J.D.; Julian, K. Urinary tract infections in solid organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13507. [Google Scholar] [CrossRef]
- Coussement, J.; Kaminski, H.; Scemla, A.; Manuel, O. Asymptomatic bacteriuria and urinary tract infections in kidney transplant recipients. Curr. Opin. Infect. Dis. 2020, 33, 419–425. [Google Scholar] [CrossRef]
- Parasuraman, R.; Julian, K. Urinary tract infections in solid organ transplantation. Am. J. Transplant. 2013, 13, 327–336. [Google Scholar] [CrossRef]
- Green, H.; Rahamimov, R.; Gafter, U.; Leibovitci, L.; Paul, M. Antibiotic prophylaxis for urinary tract infections in renal transplant recipients: A systematic review and meta-analysis. Transpl. Infect. Dis. 2011, 13, 441–447. [Google Scholar] [CrossRef]
- Rosado-Canto, R.; Parra-Avila, I.; Tejeda-Maldonado, J.; Kauffman-Ortega, C.; Rodriguez-Covarrubias, F.T.; Trujeque-Matos, M.; Cruz-Martínez, R.; Maravilla-Franco, E.; Criollo-Mora, E.; Arreola-Guerra, J.M.; et al. Perioperative fosfomycin disodium prophylaxis against urinary tract infection in renal transplant recipients: A randomized clinical trial. Nephrol. Dial. Transplant. 2020, 35, 1996–2003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horwedel, T.A.; Bowman, L.J.; Saab, G.; Brennan, D.C. Benefits of sulfamethoxazole-trimethoprim prophylaxis on rates of sepsis after kidney transplant. Transpl. Infect. Dis. 2014, 16, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Maanaoui, M.; Baes, D.; Hamroun, A.; Khedjat, K.; Vuotto, F.; Faure, E.; Lopez, B.; Bouyé, S.; Caes, T.; Lionet, A.; et al. Association between acute graft pyelonephritis and kidney graft survival: A single-center observational study. Am. J. Transplant. 2021, 21, 3640–3648. [Google Scholar] [CrossRef] [PubMed]
- Mitra, S.; Alangaden, G.J. Recurrent urinary tract infections in kidney transplant recipients. Curr. Infect. Dis. Rep. 2011, 13, 579–587. [Google Scholar] [CrossRef]
- Säemann, M.; Hörl, W.H. Urinary tract infection in renal transplant recipients. Eur. J. Clin. Investig. 2008, 38, 58–65. [Google Scholar] [CrossRef]
- Wolf, S.; Lauseker, M.; Schiergens, T.; Wirth, U.; Drefs, M.; Renz, B.; Ryll, M.; Bucher, J.; Werner, J.; Guba, M.; et al. Infections after kidney transplantation: A comparison of mTOR-Is and CNIs as basic immunosuppressants. A systematic review and meta-analysis. Transpl. Infect. Dis. 2020, 22, e13267. [Google Scholar] [CrossRef] [Green Version]
- Dulek, D.E.; Mueller, N.J. Pneumonia in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13545. [Google Scholar] [CrossRef]
- Huang, S.T.; Yu, T.M.; Chuang, Y.W.; Chen, C.H.; Wu, M.J.; Wang, I.K.; Li, C.Y.; Lin, C.L.; Kao, C.H. Pneumococcal pneumonia in adult hospitalised solid organ transplant recipients: Nationwide, population-based surveillance. Int. J. Clin. Pract. 2021, 75, 1–10. [Google Scholar] [CrossRef]
- Fisher, C.E.; Preiksaitis, C.M.; Lease, E.D.; Edelman, J.; Kirby, K.A.; Leisenring, W.M.; Raghu, G.; Boeckh, M.; Limaye, A.P. Symptomatic respiratory virus infection and chronic lung allograft dysfunction. Clin. Infect. Dis. 2016, 62, 313–319. [Google Scholar] [CrossRef]
- Cervera, C.; Agustí, C.; Angeles Marcos, M.; Pumarola, T.; Cofán, F.; Navasa, M.; Pérez-Villa, F.; Torres, A.; Moreno, A. Microbiologic features and outcome of pneumonia in transplanted patients. Diagn. Microbiol. Infect. Dis. 2006, 55, 47–54. [Google Scholar] [CrossRef]
- Olarte, L.; Lin, P.L.; Barson, W.J.; Romero, J.R.; Tan, T.Q.; Givner, L.B.; Hoffman, J.A.; Bradley, J.S.; Hultén, K.G.; Mason, E.O.; et al. Invasive pneumococcal infections in children following transplantation in the pneumococcal conjugate vaccine era. Transpl. Infect. Dis. 2017, 19, e12630. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Tuberculosis Report 2021; World Health Organization: Geneva, Switzerland, 2021; ISBN 9789240037021.
- Krishnamoorthy, S.; Kumaresan, N.; Zumla, A. Latent tuberculosis infection and renal transplantation—Diagnosis and management. Int. J. Infect. Dis. 2019, 80, S73–S76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Latent Tuberculosis Infection: Updated and Consolidated Guidelines for Programmatic Management; World Health Organization: Geneva, Switzerland, 2018; ISBN 9789241550239.
- Hasan, T.; Au, E.; Chen, S.; Tong, A.; Wong, G. Screening and prevention for latent tuberculosis in immunosuppressed patients at risk for tuberculosis: A systematic review of clinical practice guidelines. BMJ Open 2018, 8, e022445. [Google Scholar] [CrossRef]
- Fishman, J.A. Mycobacterium tuberculosis in transplantation: Immunity sufficient to perpetuate disease? Am. J. Transplant. 2019, 19, 1262–1263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez De Castilla, D.; Schluger, N.W. Tuberculosis following solid organ transplantation. Transpl. Infect. Dis. 2010, 12, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Anand, M.; Nayyar, E.; Concepcion, B.; Salani, M.; Schaefer, H. Tuberculosis in kidney transplant recipients: A case series. World J. Transpl. 2017, 7, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, A.K.; Theodoropoulos, N.M. Mycobacterium tuberculosis infections in solid organ transplantation: Guidelines from the infectious diseases community of practice of the American Society of Transplantation. Clin. Transplant. 2019, 33, e13513. [Google Scholar] [CrossRef] [PubMed]
- Viana, L.A.; Cristelli, M.P.; Santos, D.W.; Tavares, M.G.; Dantas, M.T.C.; Felipe, C.R.; Silva, H.T.; Pestana, J.M. Influence of epidemiology, immunosuppressive regimens, clinical presentation, and treatment on kidney transplant outcomes of patients diagnosed with tuberculosis: A retrospective cohort analysis. Am. J. Transplant. 2019, 19, 1421–1431. [Google Scholar] [CrossRef]
- Abad, C.L.R.; Razonable, R.R. Donor derived Mycobacterium tuberculosis infection after solid-organ transplantation: A comprehensive review. Transpl. Infect. Dis. 2018, 20, e12971. [Google Scholar] [CrossRef]
- Abad, C.L.R.; Razonable, R.R. Mycobacterium tuberculosis after solid organ transplantation: A review of more than 2000 cases. Clin. Transplant. 2018, 32, e13259. [Google Scholar] [CrossRef]
- Pai, M.; Denkinger, C.M.; Kik, S.V.; Rangaka, M.X.; Zwerling, A.; Oxlade, O.; Metcalfe, J.Z.; Cattamanchi, A.; Dowdy, D.W.; Dheda, K.; et al. Gamma interferon release assays for detection of Mycobacterium tuberculosis infection. Clin. Microbiol. Rev. 2014, 27, 3–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guirao-Arrabal, E.; Torre-Cisneros, J. Tuberculin skin test, Interferon gamma release assays or just chest x-ray to study latent tuberculosis before solid organ transplantation? Transpl. Infect. Dis. 2018, 20, 12920. [Google Scholar] [CrossRef] [PubMed]
- Rahimifard, N.; Mahmoudi, S.; Mamishi, S.; Pourakbari, B. Prevalence of latent tuberculosis infection in transplant candidates: A systematic review and meta-analysis. Microb. Pathog. 2018, 125, 401–410. [Google Scholar] [CrossRef]
- LTBI: A Guide for Primary Health Care Providers—CDC. Available online: https://www.cdc.gov/tb/publications/ltbi/default.htm (accessed on 18 January 2022).
- Lewinsohn, D.M.; Leonard, M.K.; Lobue, P.A.; Cohn, D.L.; Daley, C.L.; Desmond, E.; Keane, J.; Lewinsohn, D.A.; Loeffler, A.M.; Mazurek, G.H.; et al. Official American thoracic society/Infectious diseases society of America/Centers for disease control and prevention clinical practice guidelines: Diagnosis of tuberculosis in adults and children. Clin. Infect. Dis. 2017, 64, 111–115. [Google Scholar] [CrossRef]
- Sparkes, T.; Lemonovich, T.L. Interactions between anti-infective agents and immunosuppressants—Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Anjan, S.; Morris, M.I. Nontuberculous mycobacteria in solid organ transplant. Curr. Opin. Organ Transplant. 2019, 24, 476–482. [Google Scholar] [CrossRef]
- Longworth, S.A.; Daly, J.S. Management of infections due to nontuberculous mycobacteria in solid organ transplant recipients—Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13588. [Google Scholar] [CrossRef]
- Brown-Elliott, B.A.; Brown, J.M.; Conville, P.S.; Wallace, R.J. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin. Microbiol. Rev. 2006, 19, 259–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saullo, J.L.; Miller, R.A. Update on Nocardia infections in solid-organ transplantation. Curr. Opin. Organ Transplant. 2020, 25, 383–392. [Google Scholar] [CrossRef]
- Conville, P.S.; Brown-Elliott, B.A.; Smith, T.; Zelazny, A.M. The complexities of nocardia taxonomy and identification. J. Clin. Microbiol. 2018, 56, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Coussement, J.; Lebeaux, D.; van Delden, C.; Guillot, H.; Freund, R.; Marbus, S.; Melica, G.; Van Wijngaerden, E.; Douvry, B.; Van Laecke, S.; et al. Nocardia Infection in Solid Organ Transplant Recipients: A Multicenter European Case-control Study. Clin. Infect. Dis. 2016, 63, 338–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernàndez-Sabé, N.; Cervera, C.; López-Medrano, F.; Llano, M.; Sáez, E.; Len, Ó.; Fortún, J.; Blenes, M.; Laporta, R.; TorreCisneros, J.; et al. Risk factors, clinical features, and outcomes of listeriosis in solid-organ transplant recipients: A matched case-control study. Clin. Infect. Dis. 2009, 49, 1153–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swaminathan, B.; Gerner-Smidt, P. The epidemiology of human listeriosis. Microbes Infect. 2007, 9, 1236–1243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thønnings, S.; Knudsen, J.D.; Schønheyder, H.C.; Søgaard, M.; Arpi, M.; Gradel, K.O.; Østergaard, C.; Jensen, U.S.; Koch, K.; Smit, J.; et al. Antibiotic treatment and mortality in patients with Listeria monocytogenes meningitis or bacteraemia. Clin. Microbiol. Infect. 2016, 22, 725–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Temple, M.E.; Nahata, M.C. Treatment of listeriosis. Ann. Pharmacother. 2000, 34, 656–661. [Google Scholar] [CrossRef] [PubMed]
- Dickstein, Y.; Oster, Y.; Shimon, O.; Nesher, L.; Yahav, D.; Wiener-Well, Y.; Cohen, R.; Ben-Ami, R.; Weinberger, M.; Rahav, G.; et al. Antibiotic treatment for invasive nonpregnancy-associated listeriosis and mortality: A retrospective cohort study. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2243–2251. [Google Scholar] [CrossRef]
- Madeo, M.; Musumeci, R.; Laura Careddu, A.M.; Amato, E.; Pontello, M.M.; Cocuzza, C.E. Antimicrobial susceptibility of Listeria monocytogenes isolates from human cases in northern Italy, 2008–2010: MIC determination according to EUCAST broth microdilution method. J. Chemother. 2015, 27, 201–206. [Google Scholar] [CrossRef]
- Davis, N.L.; King, C.C.; Kourtis, A.P. Cytomegalovirus infection in pregnancy. Birth Defects Res. 2017, 109, 336–346. [Google Scholar] [CrossRef] [Green Version]
- Lisboa, L.F.; Kumar, D.; Wilson, L.E.; Humar, A. Clinical utility of cytomegalovirus cell-mediated immunity in transplant recipients with cytomegalovirus viremia. Transplantation 2012, 93, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Razonable, R.R.; Humar, A. Cytomegalovirus in solid organ transplant recipients—Guidelines of the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13512. [Google Scholar] [CrossRef]
- Gerna, G.; Lilleri, D.; Chiesa, A.; Zelini, P.; Furione, M.; Comolli, G.; Pellegrini, C.; Sarchi, E.; Migotto, C.; Regazzi Bonora, M.; et al. Virologic and immunologic monitoring of cytomegalovirus to guide preemptive therapy in solid-organ transplantation. Am. J. Transplant. 2011, 11, 2463–2471. [Google Scholar] [CrossRef] [PubMed]
- Humar, A.; Limaye, A.P.; Blumberg, E.A.; Hauser, I.A.; Vincenti, F.; Jardine, A.G.; Abramowicz, D.; Ives, J.A.L.; Farhan, M.; Peeters, P. Extended valganciclovir prophylaxis in D+/R− kidney transplant recipients is associated with long-term reduction in cytomegalovirus disease: Two-year results of the impact study. Transplantation 2010, 90, 1427–1431. [Google Scholar] [CrossRef] [PubMed]
- Griffiths, P.D.; Rothwell, E.; Raza, M.; Wilmore, S.; Doyle, T.; Harber, M.; O’Beirne, J.; Mackinnon, S.; Jones, G.; Thorburn, D.; et al. Randomized controlled trials to define viral load thresholds for cytomegalovirus pre-emptive therapy. PLoS ONE 2016, 11, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Meesing, A.; Razonable, R.R. New Developments in the Management of Cytomegalovirus Infection After Transplantation. Drugs 2018, 78, 1085–1103. [Google Scholar] [CrossRef]
- Winstead, R.J.; Kumar, D.; Brown, A.; Yakubu, I.; Song, C.; Thacker, L.; Gupta, G. Letermovir prophylaxis in solid organ transplant—Assessing CMV breakthrough and tacrolimus drug interaction. Transpl. Infect. Dis. 2021, 23, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, H.H.; Randhawa, P.S. BK polyomavirus in solid organ transplantation—Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, 1–19. [Google Scholar] [CrossRef]
- Maung Myint, T.; Chong, C.H.Y.; Wyld, M.; Nankivell, B.; Kable, K.; Wong, G. Polyoma BK Virus in Kidney Transplant Recipients. Transplantation 2022, 106, e76–e89. [Google Scholar] [CrossRef]
- Kartau, M.; Auvinen, E.; Verkkoniemi-Ahola, A.; Mannonen, L.; Helanterä, I.; Anttila, V.-J. JC polyomavirus DNA detection in clinical practice. J. Clin. Virol. 2022, 146, 105051. [Google Scholar] [CrossRef]
- Nickeleit, V.; Singh, H.K.; Randhawa, P.; Drachenberg, C.B.; Bhatnagar, R.; Bracamonte, E.; Chang, A.; James Chon, W.; Dadhania, D.; Davis, V.G.; et al. The Banff Working Group Classification of Definitive Polyomavirus Nephropathy: Morphologic Definitions and Clinical Correlations. J. Am. Soc. Nephrol. 2018, 29, 680–693. [Google Scholar] [CrossRef] [Green Version]
- Nickeleit, V.; Singh, H.K.; Dadhania, D.; Cornea, V.; El-Husseini, A.; Castellanos, A.; Davis, V.G.; Waid, T.; Seshan, S.V. The 2018 Banff Working Group classification of definitive polyomavirus nephropathy: A multicenter validation study in the modern era. Am. J. Transplant. 2021, 21, 669–680. [Google Scholar] [CrossRef]
- Vu, D.; Shah, T.; Ansari, J.; Naraghi, R.; Min, D. Efficacy of intravenous immunoglobulin in the treatment of persistent BK viremia and BK virus nephropathy in renal transplant recipients. Transplant. Proc. 2015, 47, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Matsumura, S.; Kato, T.; Taniguchi, A.; Kawamura, M.; Nakazawa, S.; Namba-Hamano, T.; Abe, T.; Nonomura, N.; Imamura, R. Clinical efficacy of intravenous immunoglobulin for BK polyomavirus-associated nephropathy after living kidney transplantation. Ther. Clin. Risk Manag. 2020, 16, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Mallat, S.G.; Tanios, B.Y.; Itani, H.S.; Lotfi, T.; McMullan, C.; Gabardi, S.; Akl, E.A.; Azzi, J.R. CMV and BKPyV infections in renal transplant recipients receiving an mtor inhibitor–based regimen versus a cni-based regimen: A systematic review and meta-analysis of randomized, controlled trials. Clin. J. Am. Soc. Nephrol. 2017, 12, 1321–1336. [Google Scholar] [CrossRef]
- Hahn, D.; Hodson, E.M.; Hamiwka, L.A.; Lee, V.W.S.; Chapman, J.R.; Craig, J.C.; Webster, A.C. Target of rapamycin inhibitors (TOR-I; sirolimus and everolimus) for primary immunosuppression in kidney transplant recipients. Cochrane Database Syst. Rev. 2019, 12, CD004290. [Google Scholar] [CrossRef]
- Dunmire, S.K.; Verghese, P.S.; Balfour, H.H. Primary Epstein-Barr virus infection. J. Clin. Virol. 2018, 102, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Le, J.; Durand, C.M.; Agha, I.; Brennan, D.C. Epstein–Barr virus and renal transplantation. Transplant. Rev. 2017, 31, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Allen, U.D.; Preiksaitis, J.K. Post-transplant lymphoproliferative disorders, Epstein-Barr virus infection, and disease in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13652. [Google Scholar] [CrossRef]
- AlDabbagh, M.A.; Gitman, M.R.; Kumar, D.; Humar, A.; Rotstein, C.; Husain, S. The Role of Antiviral Prophylaxis for the Prevention of Epstein–Barr Virus–Associated Posttransplant Lymphoproliferative Disease in Solid Organ Transplant Recipients: A Systematic Review. Am. J. Transplant. 2017, 17, 770–781. [Google Scholar] [CrossRef]
- Reshef, R.; Vardhanabhuti, S.; Luskin, M.R.; Heitjan, D.F.; Hadjiliadis, D.; Goral, S.; Krok, K.L.; Goldberg, L.R.; Porter, D.L.; Stadtmauer, E.A.; et al. Reduction of immunosuppression as initial therapy for posttransplantation lymphoproliferative disorder. Am. J. Transplant. 2011, 11, 336–347. [Google Scholar] [CrossRef]
- Lee, D.H.; Zuckerman, R.A. Herpes simplex virus infections in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13526. [Google Scholar] [CrossRef]
- McQuillan, G.; Kruszon-Moran, D.; Flagg, E.W.; Paulose-Ram, R. Prevalence of Herpes Simplex Virus Type 1 and Type 2 in Persons Aged 14–49: United States, 2015–2016; NCHS Data Brief No. 304; National Center for Health Statistics: Hyattsville, MD, USA, 2018; pp. 1–8.
- Singh, N.; Tscharke, D.C. Herpes Simplex Virus Latency Is Noisier the Closer We Look. J. Virol. 2020, 94, e01701-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naraqi, S.; Jackson, G.G.; Jonasson, O.; Yamashiroya, H.M. Prospective study of prevalence, incidence, and source of herpesvirus infections in patients with renal allografts. J. Infect. Dis. 1977, 136, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, M.S.; Friedman, H.; Cohen, S.G.; Oh, S.H.; Laster, L.; Starr, S. A Comparative Study of Herpes Simplex Infections in Renal Transplant and Leukemic Patients. J. Infect. Dis. 1987, 156, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Fife, K.H.; Warren, T.J.; Justus, S.E.; Heitman, C.K. An international, randomized, double-blind, placebo-controlled, study of valacyclovir for the suppression of herpes simplex virus type 2 genital herpes in newly diagnosed patients. Sex. Transm. Dis. 2008, 35, 666–673. [Google Scholar] [CrossRef]
- Valencia, I.; Miles, D.K.; Melvin, J.; Khurana, D.; Kothare, S.; Hardison, H.; Legido, A. Relapse of herpes encephalitis after acyclovir therapy: Report of two new cases and review of the literature. Neuropediatrics 2004, 35, 371–376. [Google Scholar] [CrossRef]
- Jantsch, J.; Schmidt, B.; Bardutzky, J.; Bogdan, C.; Eckardt, K.U.; Raff, U. Lethal varicella-zoster virus reactivation without skin lesions following renal transplantation. Nephrol. Dial. Transplant. 2011, 26, 365–368. [Google Scholar] [CrossRef]
- Pergam, S.A.; Limaye, A.P. Varicella zoster virus in solid organ transplantation: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13622. [Google Scholar] [CrossRef]
- Gilden, D.H.; Kleinschmidt-DeMasters, B.K.; La Guardia, J.J.; Mahalingam, R.; Cohrs, R.J. Neurologic Complications of the Reactivation of Varicella—Zoster Virus. N. Engl. J. Med. 2000, 342, 635–646. [Google Scholar] [CrossRef]
- Avettand-Fenoël, V.; Rouzioux, C.; Legendre, C.; Canaud, G. HIV Infection in the native and allograft kidney: Implications for management, diagnosis, and transplantation. Transplantation 2017, 101, 2003–2008. [Google Scholar] [CrossRef]
- Chan, S.; Isbel, N.M.; Hawley, C.M.; Campbell, S.B.; Campbell, K.L.; Morrison, M.; Francis, R.S.; Playford, E.G.; Johnson, D.W. Infectious complications following kidney transplantation—A focus on hepatitis c infection, cytomegalovirus infection and novel developments in the gut microbiota. Medicina 2019, 55, 672. [Google Scholar] [CrossRef] [Green Version]
- Wolfe, C.R.; Ison, M.G. Donor-derived infections: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13547. [Google Scholar] [CrossRef] [PubMed]
- Mercado-Crespo, M.C.; Sumner, S.A.; Spelke, M.B.; Sugerman, D.E.; Stanley, C. EIS officer, CDC Notes from the field: Increase in fentanyl-related overdose deaths—Rhode Island, November 2013–March 2014. MMWR. Morb. Mortal. Wkly. Rep. 2014, 63, 531. [Google Scholar] [PubMed]
- Yango, A.F.; Fischbach, B.V.; Levy, M.; Chandrakantan, A.; Tan, V.; Spak, C.; Melton, L.; Rice, K.; Barri, Y.; Rajagopal, A.; et al. West nile virus infection in kidney and pancreas transplant recipients in the dallas-fort worth metroplex during the 2012 texas epidemic. Transplantation 2014, 97, 953–957. [Google Scholar] [CrossRef] [PubMed]
- Winston, D.J.; Vikram, H.R.; Rabe, I.B.; Dhillon, G.; Mulligan, D.; Hong, J.C.; Busuttil, R.W.; Nowicki, M.J.; Mone, T.; Civen, R.; et al. Donor-derived West Nile virus infection in solid organ transplant recipients: Report of four additional cases and review of clinical, diagnostic, and therapeutic features. Transplantation 2014, 97, 881–889. [Google Scholar] [CrossRef] [Green Version]
- Aziz, F.; Saddler, C.; Jorgenson, M.; Smith, J.; Mandelbrot, D. Epidemiology, management, and graft outcomes after West Nile virus encephalitis in kidney transplant recipients. Transpl. Infect. Dis. 2020, 22, e13317. [Google Scholar] [CrossRef]
- Anesi, J.A.; Silveira, F.P. Arenaviruses and West Nile Virus in solid organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13576. [Google Scholar] [CrossRef]
- Tsikala-Vafea, M.; Basoulis, D.; Pavlopoulou, I.; Darema, M.; Deliolanis, J.; Daikos, G.L.; Boletis, J.; Psichogiou, M. Bloodstream infections by gram-negative bacteria in kidney transplant patients: Incidence, risk factors, and outcome. Transpl. Infect. Dis. 2020, 22, e13442. [Google Scholar] [CrossRef]
- Silva, M.; Marra, A.R.; Pereira, C.A.P.; Medina-Pestana, J.O.; Camargo, L.F.A. Bloodstream infection after kidney transplantation: Epidemiology, microbiology, associated risk factors, and outcome. Transplantation 2010, 90, 581–587. [Google Scholar] [CrossRef]
- Moreno, A.; Cervera, C.; Gavaldá, J.; Rovira, M.; De La Cámara, R.; Jarque, I.; Montejo, M.; De La Torre-Cisneros, J.; Miguel Cisneros, J.; Fortún, J.; et al. Bloodstream infections among transplant recipients: Results of a nationwide surveillance in Spain. Am. J. Transplant. 2007, 7, 2579–2586. [Google Scholar] [CrossRef]
- Aguado, J.M.; Silva, J.T.; Fernández-Ruiz, M.; Cordero, E.; Fortún, J.; Gudiol, C.; Martínez-Martínez, L.; Vidal, E.; Almenar, L.; Almirante, B.; et al. Management of multidrug resistant Gram-negative bacilli infections in solid organ transplant recipients: SET/GESITRA-SEIMC/REIPI recommendations. Transplant. Rev. 2018, 32, 36–57. [Google Scholar] [CrossRef] [Green Version]
- Rice, L.B. Federal funding for the study of antimicrobial resistance in nosocomial pathogens: No ESKAPE. J. Infect. Dis. 2008, 197, 1079–1081. [Google Scholar] [CrossRef]
- Nellore, A.; Huprikar, S. Vancomycin-resistant Enterococcus in solid organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13549. [Google Scholar] [CrossRef] [PubMed]
- Pouch, S.M.; Patel, G. Multidrug-resistant Gram-negative bacterial infections in solid organ transplant recipients—Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin. Transplant. 2019, 33, e13594. [Google Scholar] [CrossRef] [PubMed]
- De Rosa, F.G.; Corcione, S.; Pagani, N.; Di Perri, G. From ESKAPE to ESCAPE, From KPC to CCC. Clin. Infect. Dis. 2015, 60, 1289–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomsen, R.W.; Hundborg, H.H.; Lervang, H.H.; Johnsen, S.P.; Schønheyder, H.C.; Sørensen, H.T. Diabetes mellitus as a risk and prognostic factor for community-acquired bacteremia due to enterobacteria: A 10-year, population-based study among adults. Clin. Infect. Dis. 2005, 40, 628–631. [Google Scholar] [CrossRef] [Green Version]
- De Carvalho, M.A.; Freitas, F.G.R.; Silva, H.T.; Bafi, A.T.; Machado, F.R.; Pestana, J.O.M. Mortality predictors in renal transplant recipients with severe sepsis and septic shock. PLoS ONE 2014, 9, e111610. [Google Scholar] [CrossRef] [Green Version]
- Bafi, A.T.; Tomotani, D.Y.V.; De Freitas, F.G.R. Sepsis in solid-organ transplant patients. Shock 2017, 47, 12–16. [Google Scholar] [CrossRef]
- Hahner, S.; Allolio, B. Management of adrenal insufficiency in different clinical settings. Expert Opin. Pharmacother. 2005, 6, 2407–2417. [Google Scholar] [CrossRef]
- McCreery, R.J.; Florescu, D.F.; Kalil, A.C. Sepsis in immunocompromised patients without human immunodeficiency virus. J. Infect. Dis. 2020, 222, S156–S165. [Google Scholar] [CrossRef]
- Akalin, E.; Azzi, Y.; Bartash, R.; Seethamraju, H.; Parides, M.; Hemmige, V.; Ross, M.; Forest, S.; Goldstein, Y.D.; Ajaimy, M.; et al. COVID-19 and Kidney Transplantation. N. Engl. J. Med. 2020, 382, 2475–2477. [Google Scholar] [CrossRef]
- Mella, A.; Mingozzi, S.; Gallo, E.; Lavacca, A.; Rossetti, M.; Clari, R.; Randone, O.; Maffei, S.; Salomone, M.; Imperiale, D.; et al. Case series of six kidney transplanted patients with COVID-19 pneumonia treated with tocilizumab. Transpl. Infect. Dis. 2020, 22, e13348. [Google Scholar] [CrossRef] [PubMed]

| Implement All Available Preventive Strategies According to the Predictable Risk of Infection |
|---|
| Obtain precise radiological and microbiological assessment |
|
|
| Consider the selective immunosuppressive load (see Section 3 and Figure 1) |
| Pay attention to the potential risk of rejection after reduction/suspension of immunosuppressive drugs |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mella, A.; Mariano, F.; Dolla, C.; Gallo, E.; Manzione, A.M.; Di Vico, M.C.; Cavallo, R.; De Rosa, F.G.; Costa, C.; Biancone, L. Bacterial and Viral Infection and Sepsis in Kidney Transplanted Patients. Biomedicines 2022, 10, 701. https://doi.org/10.3390/biomedicines10030701
Mella A, Mariano F, Dolla C, Gallo E, Manzione AM, Di Vico MC, Cavallo R, De Rosa FG, Costa C, Biancone L. Bacterial and Viral Infection and Sepsis in Kidney Transplanted Patients. Biomedicines. 2022; 10(3):701. https://doi.org/10.3390/biomedicines10030701
Chicago/Turabian StyleMella, Alberto, Filippo Mariano, Caterina Dolla, Ester Gallo, Ana Maria Manzione, Maria Cristina Di Vico, Rossana Cavallo, Francesco Giuseppe De Rosa, Cristina Costa, and Luigi Biancone. 2022. "Bacterial and Viral Infection and Sepsis in Kidney Transplanted Patients" Biomedicines 10, no. 3: 701. https://doi.org/10.3390/biomedicines10030701