
Calculated Tumor-Associated Neutrophils Are Associated with the Tumor—Stroma Ratio and Predict a Poor Prognosis in Advanced Gastric Cancer




Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Clinicopathological Data
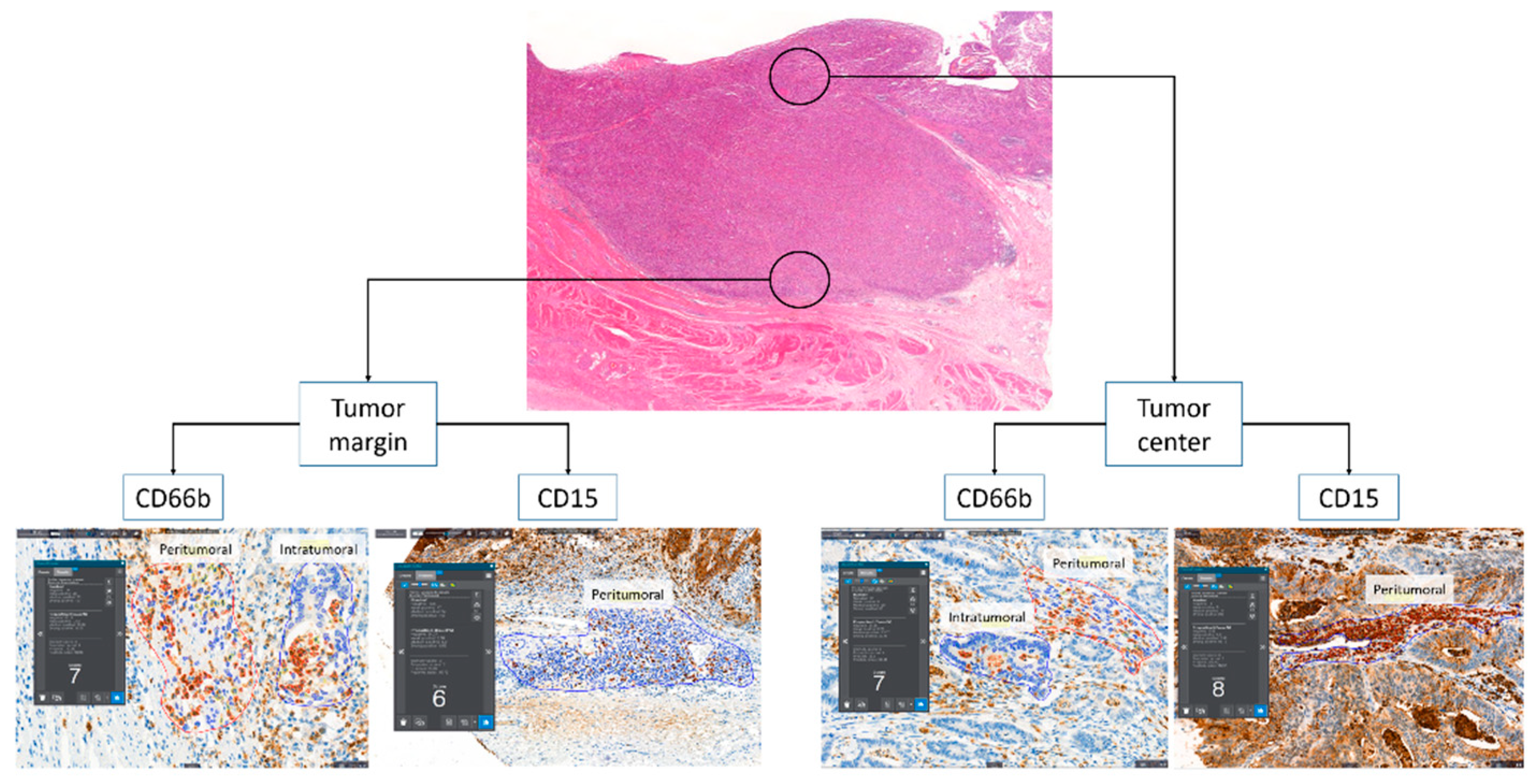
2.2. Tissue Microarray and Immunohistochemistry
2.3. Image Analysis of Immunohistochemistry
2.4. Tumor—Stroma Ratio (TSR)
2.5. Statistical Analysis
3. Results
3.1. Prognostic Value of TANs and Establishment of cN2
3.2. Clinicopathologic Characteristics Associated with cN2 and TSR in Patients with Advanced Gastric Cancer
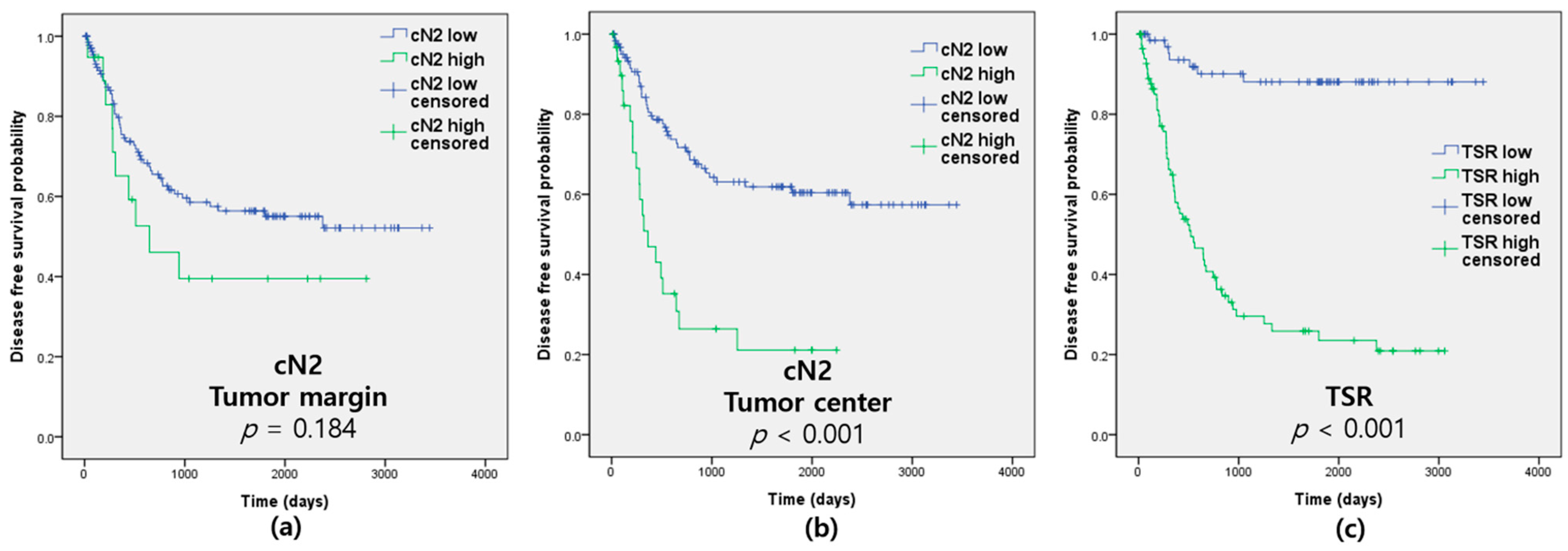
3.3. Prognostic Value of cN2 and TSR in Patients with Advanced Gastric Cancer
3.4. Multivariate Cox Proportional Hazards Model and Correlation between TANs and TSR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Murciano-Goroff, Y.R.; Warner, A.B.; Wolchok, J.D. The future of cancer immunotherapy: Microenvironment-targeting combinations. Cell Res. 2020, 30, 507–519. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Dai, Y. Tumor microenvironment and therapeutic response. Cancer Lett. 2017, 387, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Dolcetti, R.; De Re, V.; Canzonieri, V. Immunotherapy for Gastric Cancer: Time for a Personalized Approach? Int. J. Mol. Sci. 2018, 19, 1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bejarano, L.; Jordāo, M.J.C.; Joyce, J.A. Therapeutic Targeting of the Tumor Microenvironment. Cancer Discov. 2021, 11, 933–959. [Google Scholar] [CrossRef]
- Lee, D.; Ham, I.H.; Son, S.Y.; Han, S.U.; Kim, Y.B.; Hur, H. Intratumor stromal proportion predicts aggressive phenotype of gastric signet ring cell carcinomas. Gastric Cancer 2017, 20, 591–601. [Google Scholar] [CrossRef] [Green Version]
- Mao, X.; Xu, J.; Wang, W.; Liang, C.; Hua, J.; Liu, J.; Zhang, B.; Meng, Q.; Yu, X.; Shi, S. Crosstalk between cancer-associated fibroblasts and immune cells in the tumor microenvironment: New findings and future perspectives. Mol. Cancer 2021, 20, 131. [Google Scholar] [CrossRef]
- Yim, K.; Jang, W.M.; Lee, S.H. Modified Tumor Budding as a Better Predictor of Lymph Node Metastasis in Early Gastric Cancer: Possible Real-World Applications. Cancers 2021, 13, 3405. [Google Scholar] [CrossRef]
- Shen, M.; Hu, P.; Donskov, F.; Wang, G.; Liu, Q.; Du, J. Tumor-associated neutrophils as a new prognostic factor in cancer: A systematic review and meta-analysis. PLoS ONE 2014, 9, e98259. [Google Scholar] [CrossRef] [Green Version]
- Coffelt, S.B.; Wellenstein, M.D.; de Visser, K.E. Neutrophils in cancer: Neutral no more. Nat. Rev. Cancer 2016, 16, 431–446. [Google Scholar] [CrossRef] [Green Version]
- Shaul, M.E.; Fridlender, Z.G. Tumour-associated neutrophils in patients with cancer. Nat. Rev. Clin. Oncol. 2019, 16, 601–620. [Google Scholar] [CrossRef]
- Caruso, R.A.; Bellocco, R.; Pagano, M.; Bertoli, G.; Rigoli, L.; Inferrera, C. Prognostic value of intratumoral neutrophils in advanced gastric carcinoma in a high-risk area in northern Italy. Mod. Pathol. 2002, 15, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.J.; Pan, K.; Wang, W.; Chen, J.G.; Wu, Y.H.; Lv, L.; Li, J.J.; Chen, Y.B.; Wang, D.D.; Pan, Q.Z.; et al. The prognostic value of tumor-infiltrating neutrophils in gastric adenocarcinoma after resection. PLoS ONE 2012, 7, e33655. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Pan, Y.; Ma, J.; Kang, Z.; Xu, X.; Zhu, Y.; Chen, J.; Zhang, W.; Chang, W.; Zhu, J. Prognostic significance of the infiltration of CD163(+) macrophages combined with CD66b(+) neutrophils in gastric cancer. Cancer Med. 2018, 7, 1731–1741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.; Liu, H.; Shen, Z.; Lin, C.; Wang, X.; Qin, J.; Qin, X.; Xu, J.; Sun, Y. Tumor-infiltrating Neutrophils is Prognostic and Predictive for Postoperative Adjuvant Chemotherapy Benefit in Patients with Gastric Cancer. Ann. Surg. 2018, 267, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Clausen, F.; Behrens, H.M.; Krüger, S.; Röcken, C. Sexual dimorphism in gastric cancer: Tumor-associated neutrophils predict patient outcome only for women. J. Cancer Res. Clin. Oncol. 2020, 146, 53–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cong, X.; Zhang, Y.; Zhu, Z.; Li, S.; Yin, X.; Zhai, Z.; Zhang, Y.; Xue, Y. CD66b(+) neutrophils and α-SMA(+) fibroblasts predict clinical outcomes and benefits from postoperative chemotherapy in gastric adenocarcinoma. Cancer Med. 2020, 9, 2761–2773. [Google Scholar] [CrossRef] [Green Version]
- Jaillon, S.; Ponzetta, A.; Di Mitri, D.; Santoni, A.; Bonecchi, R.; Mantovani, A. Neutrophil diversity and plasticity in tumour progression and therapy. Nat. Rev. Cancer 2020, 20, 485–503. [Google Scholar] [CrossRef]
- Ohms, M.; Möller, S.; Laskay, T. An Attempt to Polarize Human Neutrophils Toward N1 and N2 Phenotypes in vitro. Front. Immunol. 2020, 11, 532. [Google Scholar] [CrossRef]
- Wang, X.; Qiu, L.; Li, Z.; Wang, X.Y.; Yi, H. Understanding the Multifaceted Role of Neutrophils in Cancer and Autoimmune Diseases. Front. Immunol. 2018, 9, 2456. [Google Scholar] [CrossRef]
- Wu, J.; Liang, C.; Chen, M.; Su, W. Association between tumor-stroma ratio and prognosis in solid tumor patients: A systematic review and meta-analysis. Oncotarget 2016, 7, 68954–68965. [Google Scholar] [CrossRef] [Green Version]
- Kemi, N.; Eskuri, M.; Herva, A.; Leppänen, J.; Huhta, H.; Helminen, O.; Saarnio, J.; Karttunen, T.J.; Kauppila, J.H. Tumour-stroma ratio and prognosis in gastric adenocarcinoma. Br. J. Cancer 2018, 119, 435–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, Y.; Li, H.; Deng, Y.; Tai, Y.; Zeng, K.; Zhang, Y.; Liu, W.; Zhang, Q.; Yang, Y. Cancer-associated fibroblasts induce PDL1+ neutrophils through the IL6-STAT3 pathway that foster immune suppression in hepatocellular carcinoma. Cell Death Dis. 2018, 9, 422. [Google Scholar] [CrossRef] [PubMed]
- Sahai, E.; Astsaturov, I.; Cukierman, E.; DeNardo, D.G.; Egeblad, M.; Evans, R.M.; Fearon, D.; Greten, F.R.; Hingorani, S.R.; Hunter, T.; et al. A framework for advancing our understanding of cancer-associated fibroblasts. Nat. Rev. Cancer 2020, 20, 174–186. [Google Scholar] [CrossRef] [Green Version]
- Tsai, Y.M.; Wu, K.L.; Liu, Y.W.; Chang, W.A.; Huang, Y.C.; Chang, C.Y.; Tsai, P.H.; Liao, S.H.; Hung, J.Y.; Hsu, Y.L. Cooperation Between Cancer and Fibroblasts in Vascular Mimicry and N2-Type Neutrophil Recruitment via Notch2-Jagged1 Interaction in Lung Cancer. Front. Oncol. 2021, 11, 696931. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing: New York, NY, USA, 2017. [Google Scholar]
- Zhu, Y.; Jin, Z.; Qian, Y.; Shen, Y.; Wang, Z. Prognostic Value of Tumor-Stroma Ratio in Rectal Cancer: A Systematic Review and Meta-analysis. Front. Oncol. 2021, 11, 685570. [Google Scholar] [CrossRef]
- Pavlou, M.; Ambler, G.; Seaman, S.R.; Guttmann, O.; Elliott, P.; King, M.; Omar, R.Z. How to develop a more accurate risk prediction model when there are few events. BMJ 2015, 351, h3868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.; Zhang, X.H. Tumor-Associated Neutrophils and Macrophages-Heterogenous but Not Chaotic. Front. Immunol. 2020, 11, 553967. [Google Scholar] [CrossRef]
- Tokumoto, M.; Tanaka, H.; Ohira, M.; Go, Y.; Okita, Y.; Sakurai, K.; Toyokawa, T.; Kubo, N.; Muguruma, K.; Maeda, K.; et al. A positive correlation between neutrophils in regional lymph nodes and progression of gastric cancer. Anticancer Res. 2014, 34, 7129–7136. [Google Scholar] [PubMed]
- Li, S.; Cong, X.; Gao, H.; Lan, X.; Li, Z.; Wang, W.; Song, S.; Wang, Y.; Li, C.; Zhang, H.; et al. Tumor-associated neutrophils induce EMT by IL-17a to promote migration and invasion in gastric cancer cells. J. Exp. Clin. Cancer Res. 2019, 38, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shan, Z.G.; Chen, J.; Liu, J.S.; Zhang, J.Y.; Wang, T.T.; Teng, Y.S.; Mao, F.Y.; Cheng, P.; Zou, Q.M.; Zhou, W.Y.; et al. Activated neutrophils polarize protumorigenic interleukin-17A-producing T helper subsets through TNF-α-B7-H2-dependent pathway in human gastric cancer. Clin. Transl. Med. 2021, 11, e484. [Google Scholar] [CrossRef]
- Abe, H.; Morikawa, T.; Saito, R.; Yamashita, H.; Seto, Y.; Fukayama, M. In Epstein-Barr virus-associated gastric carcinoma a high density of CD66b-positive tumor-associated neutrophils is associated with intestinal-type histology and low frequency of lymph node metastasis. Virchows Arch. 2016, 468, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Cuartero, M.I.; Ballesteros, I.; Moraga, A.; Nombela, F.; Vivancos, J.; Hamilton, J.A.; Corbí, Á.L.; Lizasoain, I.; Moro, M.A. N2 neutrophils, novel players in brain inflammation after stroke: Modulation by the PPARγ agonist rosiglitazone. Stroke 2013, 44, 3498–3508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grecian, R.; Whyte, M.K.B.; Walmsley, S.R. The role of neutrophils in cancer. Br. Med. Bull. 2018, 128, 5–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fridlender, Z.G.; Albelda, S.M. Tumor-associated neutrophils: Friend or foe? Carcinogenesis 2012, 33, 949–955. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.; Yang, K.; Wu, B.; Chen, H.; Chen, X.; Chen, X.; Jiang, L.; Ye, F.; He, D.; Lu, Z.; et al. Tumor-Infiltrating Immune Cells Are Associated With Prognosis of Gastric Cancer. Medicine 2015, 94, e1631. [Google Scholar] [CrossRef]
- Wang, Y.; Zhai, J.; Zhang, T.; Han, S.; Zhang, Y.; Yao, X.; Shen, L. Tumor-Associated Neutrophils Can Predict Lymph Node Metastasis in Early Gastric Cancer. Front. Oncol. 2020, 10, 570113. [Google Scholar] [CrossRef]
- Nakayama, F.; Nishihara, S.; Iwasaki, H.; Kudo, T.; Okubo, R.; Kaneko, M.; Nakamura, M.; Karube, M.; Sasaki, K.; Narimatsu, H. CD15 expression in mature granulocytes is determined by alpha 1,3-fucosyltransferase IX, but in promyelocytes and monocytes by alpha 1,3-fucosyltransferase IV. J. Biol. Chem. 2001, 276, 16100–16106. [Google Scholar] [CrossRef] [Green Version]
- McKenna, E.; Mhaonaigh, A.U.; Wubben, R.; Dwivedi, A.; Hurley, T.; Kelly, L.A.; Stevenson, N.J.; Little, M.A.; Molloy, E.J. Neutrophils: Need for Standardized Nomenclature. Front. Immunol. 2021, 12, 602963. [Google Scholar] [CrossRef]
- Ducker, T.P.; Skubitz, K.M. Subcellular localization of CD66, CD67, and NCA in human neutrophils. J. Leukoc Biol. 1992, 52, 11–16. [Google Scholar] [CrossRef]
- Mishalian, I.; Bayuh, R.; Eruslanov, E.; Michaeli, J.; Levy, L.; Zolotarov, L.; Singhal, S.; Albelda, S.M.; Granot, Z.; Fridlender, Z.G. Neutrophils recruit regulatory T-cells into tumors via secretion of CCL17—A new mechanism of impaired antitumor immunity. Int. J. Cancer 2014, 135, 1178–1186. [Google Scholar] [CrossRef]
- Masucci, M.T.; Minopoli, M.; Carriero, M.V. Tumor Associated Neutrophils. Their Role in Tumorigenesis, Metastasis, Prognosis and Therapy. Front. Oncol. 2019, 9, 1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mhaidly, R.; Mechta-Grigoriou, F. Fibroblast heterogeneity in tumor micro-environment: Role in immunosuppression and new therapies. Semin Immunol. 2020, 48, 101417. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Factors | Cutoff Values | DFS | OS | CSS | ||
|---|---|---|---|---|---|---|
| p Value | p Value | p Value | ||||
| Age | ≤ vs. >72 years old | 0.268 | <0.001 | 0.131 | ||
| Sex | Male vs. female | 0.378 | 0.984 | 0.641 | ||
| pT | T2 + T3 vs. T4 | <0.001 | <0.001 | <0.001 | ||
| pN | N0 vs. N1 + N2 + N3 | <0.001 | <0.001 | <0.001 | ||
| pM | M0 vs. M1 | 0.069 | 0.001 | <0.001 | ||
| pTNM | I + II vs. III + IV | <0.001 | <0.001 | <0.001 | ||
| Lauren classification | Intestinal vs. Others | 0.146 | 0.519 | 0.127 | ||
| Tumor differentiation | Well + moderately vs. poorly | 0.130 | 0.171 | 0.054 | ||
| Lymphatic invasion | Absent vs. present | <0.001 | <0.001 | <0.001 | ||
| Venous invasion | Absent vs. present | 0.003 | 0.096 | 0.015 | ||
| Perineural invasion | Absent vs. present | <0.001 | <0.001 | <0.001 | ||
| CD66b | Margin | Peritumoral | ≤ vs. >54.81/mm2 | 0.104 | 0.219 | 0.081 |
| Intratumoral | ≤ vs. >30.6/mm2 | 0.167 | 0.048 | 0.047 | ||
| Center | Peritumoral | ≤ vs. >4.8/mm2 | 0.053 | 0.169 | 0.097 | |
| Intratumoral | ≤ vs. >6.5/mm2 | 0.124 | 0.372 | 0.171 | ||
| CD15 | Margin | ≤ vs. >2473.3/mm2 | 0.006 | 0.001 | 0.014 | |
| Center | ≤ vs. >536.1/mm2 | 0.002 | 0.009 | 0.011 | ||
| cN2 | Margin | ≤ vs. >949.3/mm2 | 0.184 | 0.038 | 0.044 | |
| Center | ≤ vs. >954.6/mm2 | <0.001 | 0.002 | 0.002 | ||
| TSR | ≤ vs. >40% | <0.001 | <0.001 | <0.001 | ||
| Factors | cN2 of Tumor Center | p Value | TSR | p Value | ||
|---|---|---|---|---|---|---|
| Low-Grade (≤954.6/mm2) n = 126 (%) | High-Grade (>954.6 /mm2) n = 31 (%) | Low-Grade (≤40%) n = 72 (%) | High-Grade (>40%) n = 85 (%) | |||
| Age (years old) | 0.681 | 0.857 | ||||
| ≤72 | 58 (81.7) | 13 (18.3) | 32 (45.1) | 39 (54.9) | ||
| >72 | 68 (79.1) | 18 (20.9) | 40 (46.5) | 46 (53.5) | ||
| Sex | 0.167 | 0.898 | ||||
| Male | 93 (83.0) | 19 (17.0) | 51 (45.5) | 61 (54.5) | ||
| Female | 33 (73.3) | 12 (26.7) | 21 (46.7) | 24 (53.3) | ||
| pT | 0.001 | 0.000 | ||||
| T2 + T3 | 88 (88.0) | 12 (12.0) | 60 (60.0) | 40 (40.0) | ||
| T4 | 38 (66.7) | 19 (33.3) | 12 (21.1) | 45 (78.9) | ||
| pN | 0.089 | <0.001 | ||||
| N0 | 49 (87.5) | 7 (12.5) | 41 (73.2) | 15 (26.8) | ||
| N1 + N2 + N3 | 77 (76.2) | 24 (23.8) | 31 (30.7) | 70 (69.3) | ||
| pM | 0.591 | 0.013 | ||||
| M0 | 114 (79.7) | 29 (20.3) | 70 (49.0) | 73 (51.0) | ||
| M1 | 12 (85.7) | 2 (14.3) | 2 (14.3) | 12 (85.7) | ||
| pTNM | 0.260 | <0.001 | ||||
| I + II | 63 (84.0) | 12 (16.0) | 54 (72.0) | 21 (28.0) | ||
| III + IV | 63 (76.8) | 19 (23.2) | 18 (22.0) | 64 (78.0) | ||
| Lauren classification | 0.577 | 0.764 | ||||
| Intestinal | 68 (81.9) | 15 (18.1) | 39 (47.0) | 44 (53.0) | ||
| Others | 58 (78.4) | 16 (21.6) | 33 (44.6) | 41 (55.4) | ||
| Differentiation | 0.240 | <0.001 | ||||
| Well + Moderate | 51 (85.0) | 9 (15.0) | 30 (50.0) | 30 (50.0) | ||
| Poorly | 75 (77.3) | 22 (22.7) | 42 (43.3) | 55 (56.7) | ||
| Lymphatic invasion | 0.014 | <0.001 | ||||
| Absent | 59 (89.4) | 7 (10.6) | 49 (74.2) | 17 (25.8) | ||
| Present | 67 (73.6) | 24 (26.4) | 23 (25.3) | 68 (74.7) | ||
| Venous invasion | 0.223 | 0.001 | ||||
| Absent | 115 (81.6) | 26 (18.4) | 71 (50.4) | 70 (49.6) | ||
| Present | 11 (68.8) | 5 (31.3) | 1 (6.3) | 15 (93.8) | ||
| Perineural invasion | <0.001 | <0.001 | ||||
| Absent | 85 (89.5) | 10 (10.5) | 60 (63.2) | 35 (36.8) | ||
| Present | 41 (66.1) | 21 (33.9) | 12 (19.4) | 50 (80.6) | ||
| Tumor size (mm) | 0.074 | 0.079 | ||||
| ≤55.0 | 68 (86.1) | 11 (13.9) | 42 (53.2) | 37 (46.8) | ||
| >55.0 | 58 (74.4) | 20 (25.6) | 30 (38.5) | 48 (61.5) | ||
| Overall death | 0.009 | <0.001 | ||||
| Alive | 52 (91.2) | 5 (8.8) | 45 (78.9) | 12 (21.1) | ||
| Death | 74 (74.0) | 26 (26.0) | 27 (27.0) | 73 (73.0) | ||
| Recurrence | 0.001 | <0.001 | ||||
| Absent | 84 (88.4) | 11 (11.6) | 65 (68.4) | 30 (31.6) | ||
| Present | 42 (67.7) | 20 (32.3) | 7 (11.3) | 55 (88.7) | ||
| Cancer-specific death | 0.023 | <0.001 | ||||
| Alive | 81 (86.2) | 13 (13.8) | 65 (69.1) | 29 (30.9) | ||
| Death | 45 (71.4) | 18 (28.6) | 7 (11.1) | 56 (88.9) | ||
| Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|
| HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value | ||
| Age (>72 years) | 1.326 (0.803–2.190) | 0.270 | |||
| pTNM (III + IV) | 13.386 (6.031–29.708) | <0.001 | |||
| LVPI (Present) | 11.050 (4.001–30.521) | <0.001 | |||
| Tumor size (>55.0 mm) | 2.761 (1.627–4.687) | <0.001 | |||
| CD15 | Margin (>2473.3/mm2) * | 2.269 (1.149–4.484) | 0.018 | 1.539 (0.746–3.174) | 0.243 |
| Center (>536.1/mm2) * | 2.393 (1.287–4.448) | 0.006 | 1.106 (0.597–2.050) | 0.749 | |
| cN2 | Margin (>949.3/mm2) * | 1.576 (0.800–3.106) | 0.188 | 1.066 (0.521–2.181) | 0.860 |
| Center (>954.6/mm2) * | 3.241 (1.888–5.566) | <0.001 | 2.614 (1.436–4.671) | 0.001 | |
| TSR (>40%) * | 10.768 (4.877–23.775) | <0.001 | 3.976 (1.643–9.620) | 0.002 | |
| Factors | Pearson’s Coefficient | p Value | ||
|---|---|---|---|---|
| CD66b | Margin | Peritumoral | −0.095 | 0.235 |
| Intratumoral | −0.185 | 0.020 | ||
| Center | Peritumoral | −0.085 | 0.288 | |
| Intratumoral | −0.067 | 0.403 | ||
| CD15 | Margin | Peritumoral | 0.035 | 0.660 |
| Center | Peritumoral | 0.133 | 0.096 | |
| cN2 | Margin | Peritumoral | 0.088 | 0.275 |
| Center | Peritumoral | 0.179 | 0.025 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, E.Y.; Abdul-Ghafar, J.; Chong, Y.; Yim, K. Calculated Tumor-Associated Neutrophils Are Associated with the Tumor—Stroma Ratio and Predict a Poor Prognosis in Advanced Gastric Cancer. Biomedicines 2022, 10, 708. https://doi.org/10.3390/biomedicines10030708
Kim EY, Abdul-Ghafar J, Chong Y, Yim K. Calculated Tumor-Associated Neutrophils Are Associated with the Tumor—Stroma Ratio and Predict a Poor Prognosis in Advanced Gastric Cancer. Biomedicines. 2022; 10(3):708. https://doi.org/10.3390/biomedicines10030708
Chicago/Turabian StyleKim, Eun Young, Jamshid Abdul-Ghafar, Yosep Chong, and Kwangil Yim. 2022. "Calculated Tumor-Associated Neutrophils Are Associated with the Tumor—Stroma Ratio and Predict a Poor Prognosis in Advanced Gastric Cancer" Biomedicines 10, no. 3: 708. https://doi.org/10.3390/biomedicines10030708