
Do Semaphorins Play a Role in Development of Fibrosis in Patients with Nonalcoholic Fatty Liver Disease?
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Patients and Samples
2.2. Laboratory and Clinical Data
2.3. Semaphorin Measurements
2.4. Immunohistochemical Staining
2.5. Semaphorin SNP Analysis
2.6. Statistical Analysis
3. Results
3.1. Baseline Patients’ Characteristics
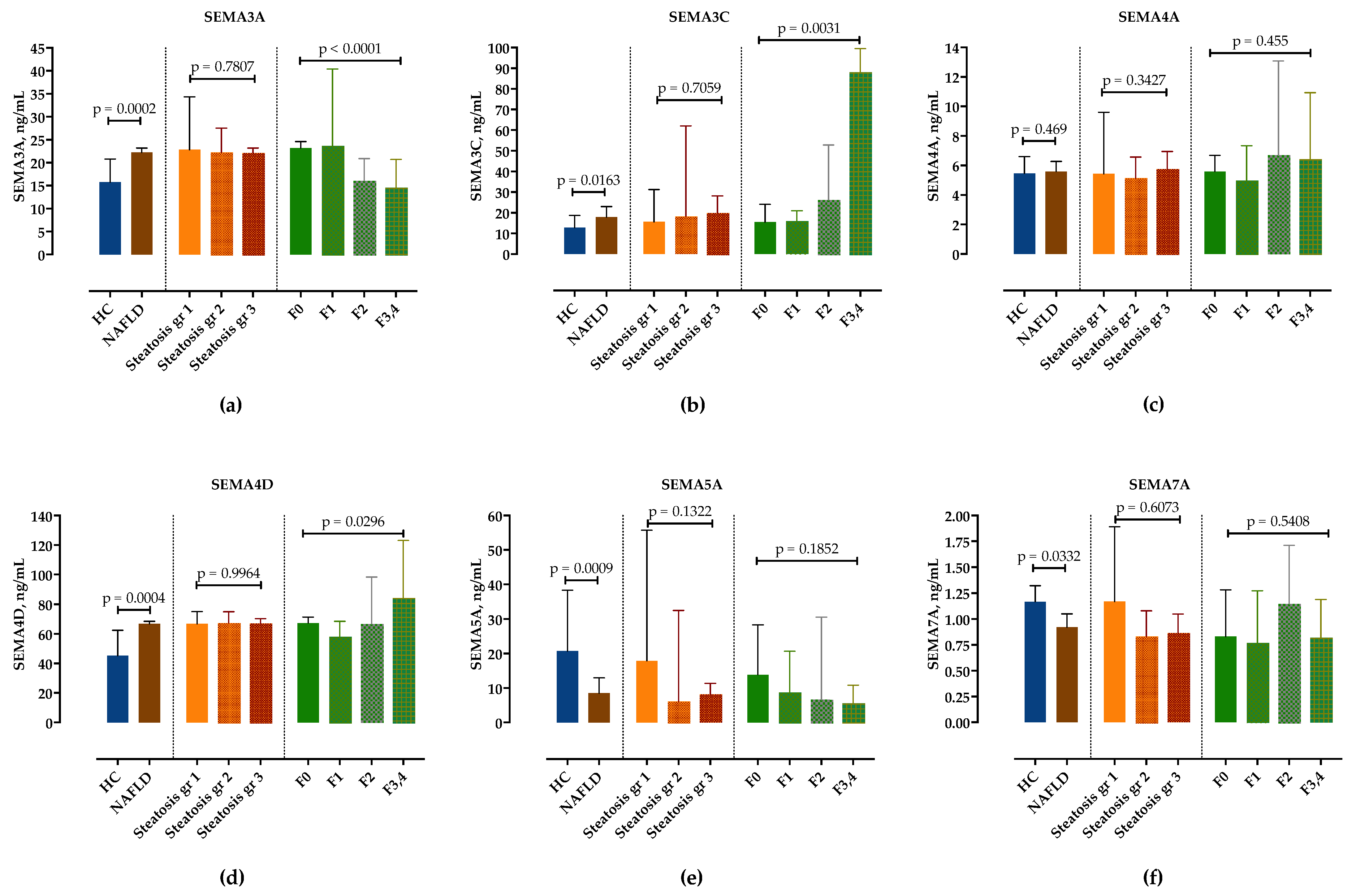
3.2. Serum Concentrations of Semaphorins in Patients with NAFLD
3.3. Correlation of Semaphorins’ Concentrations with Steatosis and Fibrosis Stages
3.4. Correlation Analysis of Serum Semaphorin Concentrations with Routine Clinical and Laboratory Findings
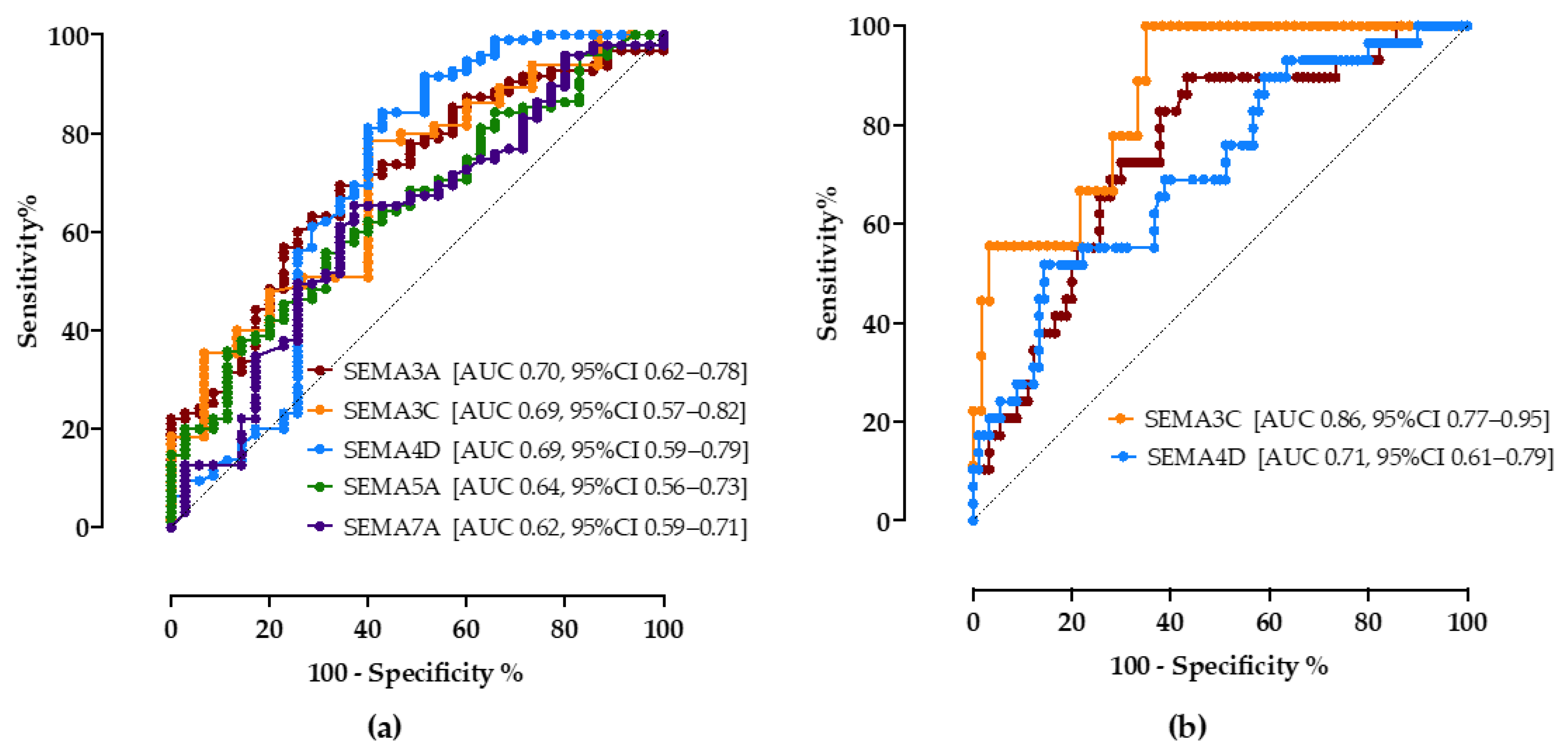
3.5. Diagnostic Value of Semaphorins to Detect Steatosis and Progressed Fibrosis
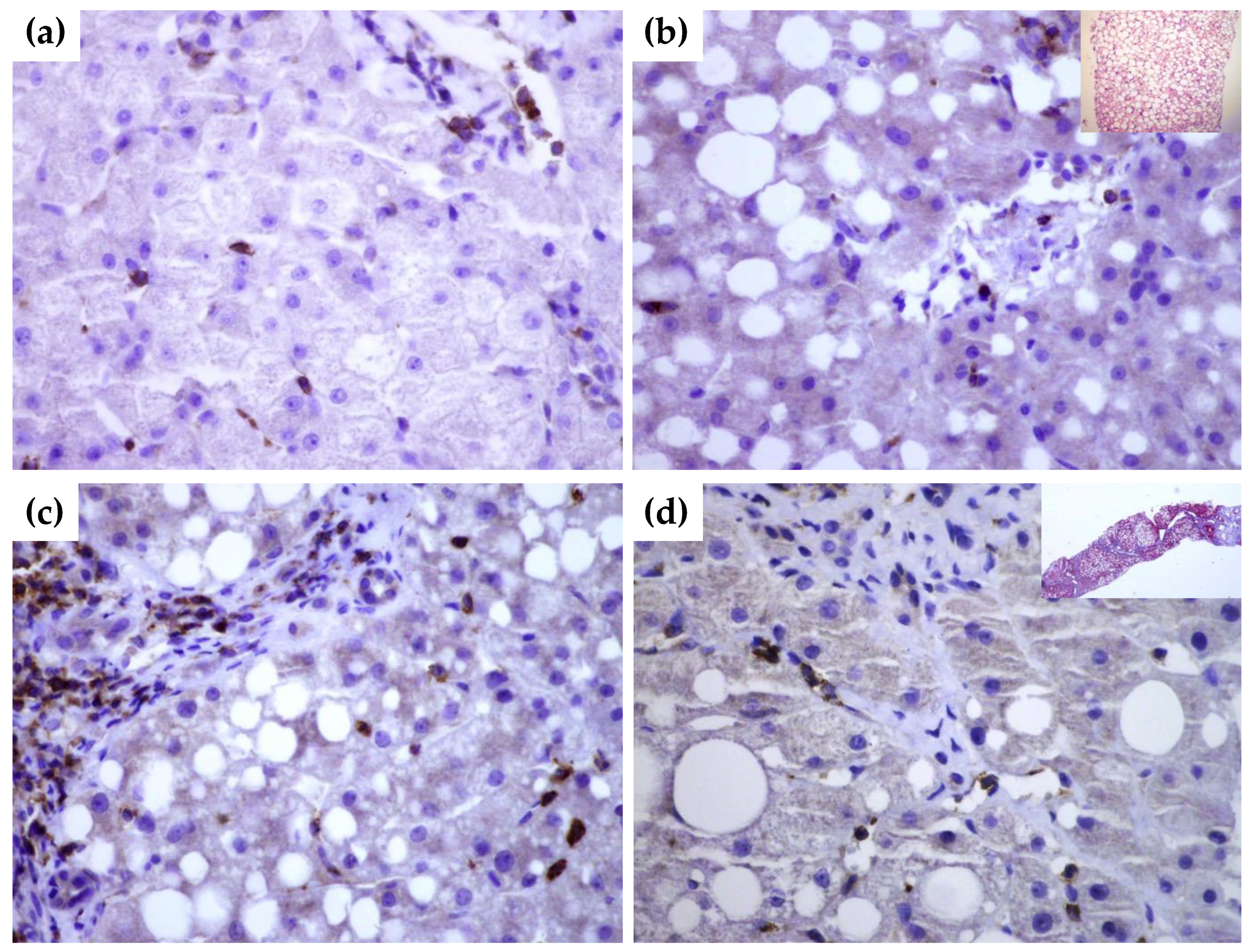
3.6. SEMA4D Expression in Liver Tissue Samples
3.7. The Frequency of SNP SEMA5A rs1319222, rs433755 and SEMA4A rs536857 in Patients with NAFLD
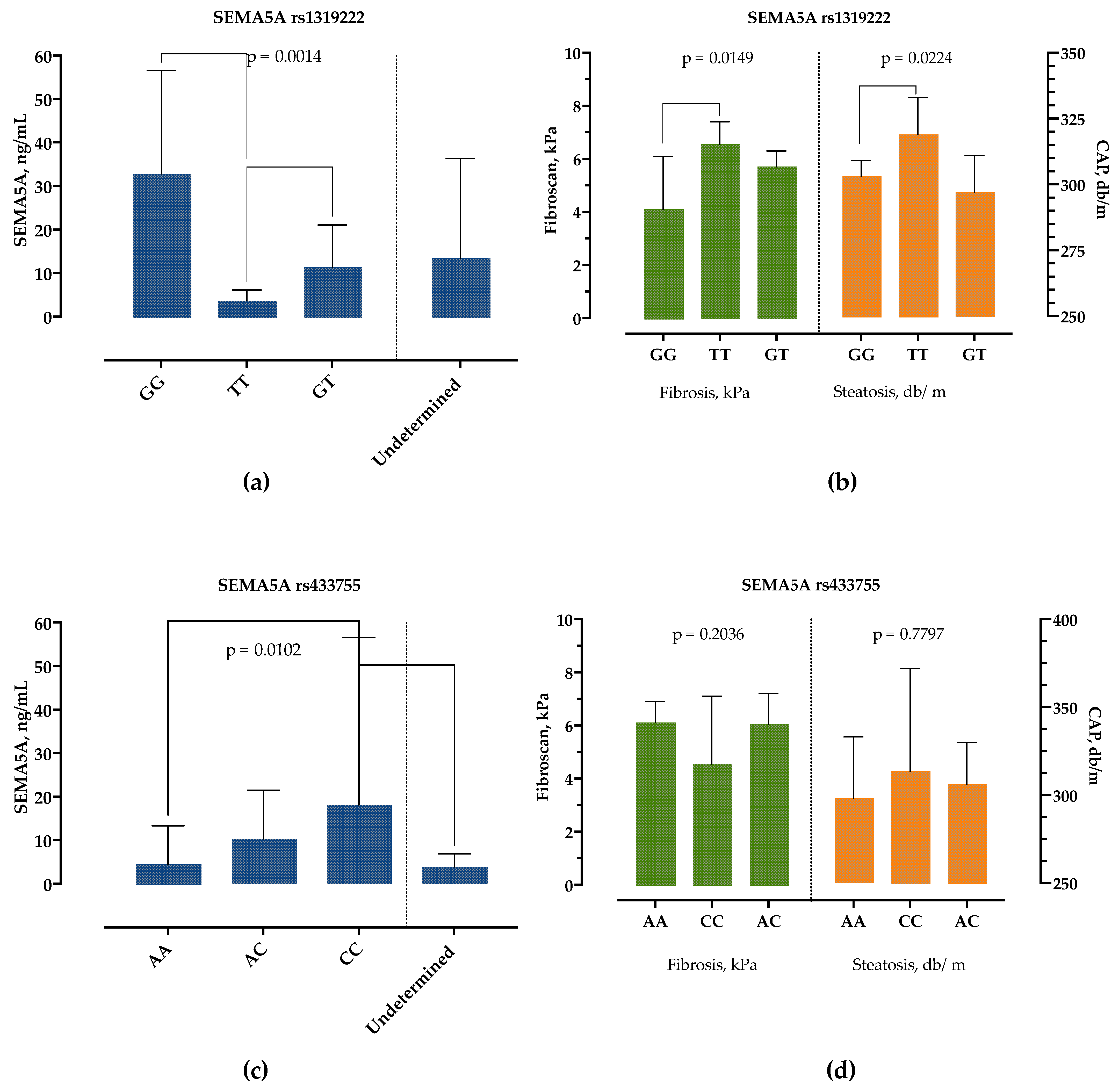
3.8. The Association of SEMA5A rs1319222 Genotype with Clinical and Laboratory Features in Patients with NAFLD
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef] [Green Version]
- Paquissi, F.C. Immune Imbalances in Non-Alcoholic Fatty Liver Disease: From General Biomarkers and Neutrophils to Interleukin-17 Axis Activation and New Therapeutic Targets. Front. Immunol. 2016, 7, 490. [Google Scholar] [CrossRef] [Green Version]
- He, B.; Wu, L.; Xie, W.; Shao, Y.; Jiang, J.; Zhao, Z.; Yan, M.; Chen, Z.; Cui, D. The imbalance of Th17/Treg cells is involved in the progression of nonalcoholic fatty liver disease in mice. BMC Immunol. 2017, 18, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, M.S.; White, A.; Perry, R.J.; Camporez, J.P.; Hidalgo, J.; Shulman, G.I.; Davis, R.J. Regulation of adipose tissue inflammation by interleukin 6. Proc. Natl. Acad. Sci. USA 2020, 117, 2751–2760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lukas, N.; Herbert, T. Cytokines and fatty liver diseases. Liver Res. 2018, 2, 14–20. [Google Scholar] [CrossRef]
- Kumanogoh, A.; Kikutani, H. Immunological functions of the neuropilins and plexins as receptors for semaphorins. Nat. Rev. Immunol. 2013, 13, 802–814. [Google Scholar] [CrossRef]
- Roney, K.; Holl, E.; Ting, J. Immune plexins and semaphorins: Old proteins, new immune functions. Protein Cell 2013, 4, 17–26. [Google Scholar] [CrossRef] [Green Version]
- Yin, Z.; Zhang, J.; Xu, S.; Liu, J.; Xu, Y.; Yu, J.; Zhao, M.; Pan, W.; Wang, M.; Wan, J. The role of semaphorins in cardiovascular diseases: Potential therapeutic targets and novel biomarkers. FASEB J. 2022, 36, e22509. [Google Scholar] [CrossRef]
- Song, Y.; Wang, L.; Zhang, L.; Huang, D. The involvement of semaphorin 7A in tumorigenic and immunoinflammatory regulation. J. Cell. Physiol. 2021, 236, 6235–6248. [Google Scholar] [CrossRef]
- Jiang, J.; Zhang, F.; Wan, Y.; Fang, K.; Yan, Z.D.; Ren, X.L.; Zhang, R. Semaphorins as Potential Immune Therapeutic Targets for Cancer. Front. Oncol. 2022, 12, 793805. [Google Scholar] [CrossRef] [PubMed]
- Papic, N.; Zidovec Lepej, S.; Gorenec, L.; Grgic, I.; Gasparov, S.; Filipec Kanizaj, T.; Vince, A. The association of semaphorins 3C, 5A and 6D with liver fibrosis stage in chronic hepatitis C. PLoS ONE 2018, 13, e0209481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertola, A.; Bonnafous, S.; Anty, R.; Patouraux, S.; Saint-Paul, M.C.; Iannelli, A.; Gugenheim, J.; Barr, J.; Mato, J.M.; Le Marchand-Brustel, Y.; et al. Hepatic expression patterns of inflammatory and immune response genes associated with obesity and NASH in morbidly obese patients. PLoS ONE 2010, 5, e13577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryaboshapkina, M.; Hammar, M. Human hepatic gene expression signature of non-alcoholic fatty liver disease progression, a meta-analysis. Sci. Rep. 2017, 7, 12361. [Google Scholar] [CrossRef]
- Paz-Filho, G.; Mastronardi, C.A.; Parker, B.J.; Khan, A.; Inserra, A.; Matthaei, K.I.; Ehrhart-Bornstein, M.; Bornstein, S.; Wong, M.L.; Licinio, J. Molecular pathways involved in the improvement of non-alcoholic fatty liver disease. J. Mol. Endocrinol. 2013, 51, 167–179. [Google Scholar] [CrossRef] [Green Version]
- European Association for the Study of the Liver; Clinical Practice Guideline Panel; EASL Governing Board representative. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis—2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef]
- Wang, Y.; Fan, Q.; Wang, T.; Wen, J.; Wang, H.; Zhang, T. Controlled attenuation parameter for assessment of hepatic steatosis grades: A diagnostic meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 17654–17663. [Google Scholar]
- Loaeza-del-Castillo, A.; Paz-Pineda, F.; Oviedo-Cardenas, E.; Sanchez-Avila, F.; Vargas-Vorackova, F. AST to platelet ratio index (APRI) for the noninvasive evaluation of liver fibrosis. Ann. Hepatol. 2008, 7, 350–357. [Google Scholar] [CrossRef]
- Sumida, Y.; Yoneda, M.; Hyogo, H.; Itoh, Y.; Ono, M.; Fujii, H.; Eguchi, Y.; Suzuki, Y.; Aoki, N.; Kanemasa, K.; et al. Validation of the FIB4 index in a Japanese nonalcoholic fatty liver disease population. BMC Gastroenterol. 2012, 12, 2. [Google Scholar] [CrossRef] [Green Version]
- Buniello, A.; MacArthur, J.A.L.; Cerezo, M.; Harris, L.W.; Hayhurst, J.; Malangone, C.; McMahon, A.; Morales, J.; Mountjoy, E.; Sollis, E.; et al. The NHGRI-EBI GWAS Catalog of published genome-wide association studies, targeted arrays and summary statistics 2019. Nucleic Acids Res. 2019, 47, D1005–D1012. [Google Scholar] [CrossRef] [Green Version]
- Duan, Y.; Pan, X.; Luo, J.; Xiao, X.; Li, J.; Bestman, P.L.; Luo, M. Association of Inflammatory Cytokines With Non-Alcoholic Fatty Liver Disease. Front. Immunol. 2022, 13, 880298. [Google Scholar] [CrossRef] [PubMed]
- Rienks, M.; Carai, P.; Bitsch, N.; Schellings, M.; Vanhaverbeke, M.; Verjans, J.; Cuijpers, I.; Heymans, S.; Papageorgiou, A. Sema3A promotes the resolution of cardiac inflammation after myocardial infarction. Basic Res. Cardiol. 2017, 112, 42. [Google Scholar] [CrossRef] [Green Version]
- Movassagh, H.; Saati, A.; Nandagopal, S.; Mohammed, A.; Tatari, N.; Shan, L.; Duke-Cohan, J.S.; Fowke, K.R.; Lin, F.; Gounni, A.S. Chemorepellent Semaphorin 3E Negatively Regulates Neutrophil Migration In Vitro and In Vivo. J. Immunol. 2017, 198, 1023–1033. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiseleva, E.P.; Rutto, K.V. Semaphorin 3A in the Immune System: Twenty Years of Study. Biochemistry 2022, 87, 640–657. [Google Scholar] [CrossRef] [PubMed]
- Vadasz, Z.; Haj, T.; Halasz, K.; Rosner, I.; Slobodin, G.; Attias, D.; Kessel, A.; Kessler, O.; Neufeld, G.; Toubi, E. Semaphorin 3A is a marker for disease activity and a potential immunoregulator in systemic lupus erythematosus. Arthritis Res. Ther. 2012, 14, R146. [Google Scholar] [CrossRef] [Green Version]
- Catalano, A. The neuroimmune semaphorin-3A reduces inflammation and progression of experimental autoimmune arthritis. J. Immunol. 2010, 185, 6373–6383. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Tan, N.; Zhou, Y.; Zhou, X.; Chen, H.; Wei, H.; Chen, J.; Xu, X.; Zhang, S.; Yang, G.; et al. Semaphorin 3A Shifts Adipose Mesenchymal Stem Cells towards Osteogenic Phenotype and Promotes Bone Regeneration In Vivo. Stem Cells Int. 2016, 2016, 2545214. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Chen, Q.; Yin, D.; Shi, S.; Yu, L.; Zhou, S.; Chen, E.; Zhou, Z.; Shi, Y.; Fan, J.; et al. Novel role of semaphorin 3A in the growth and progression of hepatocellular carcinoma. Oncol. Rep. 2017, 37, 3313–3320. [Google Scholar] [CrossRef] [Green Version]
- Mejhert, N.; Wilfling, F.; Esteve, D.; Galitzky, J.; Pellegrinelli, V.; Kolditz, C.I.; Viguerie, N.; Tordjman, J.; Naslund, E.; Trayhurn, P.; et al. Semaphorin 3C is a novel adipokine linked to extracellular matrix composition. Diabetologia 2013, 56, 1792–1801. [Google Scholar] [CrossRef] [Green Version]
- De Angelis Rigotti, F.; Wiedmann, L.; Hubert, M.O.; Vacca, M.; Hasan, S.; Moll, I.; Carvajal, S.; Jiménez, W.; Starostecka, M.; Billeter, A.; et al. Semaphorin 3C exacerbates liver fibrosis. Eur. PMC 2021. [Google Scholar] [CrossRef]
- Nkyimbeng-Takwi, E.; Chapoval, S.P. Biology and function of neuroimmune semaphorins 4A and 4D. Immunol. Res. 2011, 50, 10–21. [Google Scholar] [CrossRef]
- Nishide, M.; Nojima, S.; Ito, D.; Takamatsu, H.; Koyama, S.; Kang, S.; Kimura, T.; Morimoto, K.; Hosokawa, T.; Hayama, Y.; et al. Semaphorin 4D inhibits neutrophil activation and is involved in the pathogenesis of neutrophil-mediated autoimmune vasculitis. Ann. Rheum. Dis. 2017, 76, 1440–1448. [Google Scholar] [CrossRef]
- Xie, J.; Wang, Z.; Wang, W. Semaphorin 4D Induces an Imbalance of Th17/Treg Cells by Activating the Aryl Hydrocarbon Receptor in Ankylosing Spondylitis. Front. Immunol. 2020, 11, 2151. [Google Scholar] [CrossRef] [PubMed]
- Gras, C.; Eiz-Vesper, B.; Jaimes, Y.; Immenschuh, S.; Jacobs, R.; Witte, T.; Blasczyk, R.; Figueiredo, C. Secreted semaphorin 5A activates immune effector cells and is a biomarker for rheumatoid arthritis. Arthritis Rheumatol. 2014, 66, 1461–1471. [Google Scholar] [CrossRef]
- Sadanandam, A.; Rosenbaugh, E.G.; Singh, S.; Varney, M.; Singh, R.K. Semaphorin 5A promotes angiogenesis by increasing endothelial cell proliferation, migration, and decreasing apoptosis. Microvasc. Res. 2010, 79, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namjou, B.; Lingren, T.; Huang, Y.; Parameswaran, S.; Cobb, B.L.; Stanaway, I.B.; Connolly, J.J.; Mentch, F.D.; Benoit, B.; Niu, X.; et al. GWAS and enrichment analyses of non-alcoholic fatty liver disease identify new trait-associated genes and pathways across eMERGE Network. BMC Med. 2019, 17, 135. [Google Scholar] [CrossRef]
- Karczewski, K.J.; Francioli, L.C.; Tiao, G.; Cummings, B.B.; Alfoldi, J.; Wang, Q.; Collins, R.L.; Laricchia, K.M.; Ganna, A.; Birnbaum, D.P.; et al. The mutational constraint spectrum quantified from variation in 141,456 humans. Nature 2020, 581, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Okuno, T.; Takegahara, N.; Takamatsu, H.; Nojima, S.; Kimura, T.; Yoshida, Y.; Ito, D.; Ohmae, S.; You, D.J.; et al. Intestinal epithelial cell-derived semaphorin 7A negatively regulates development of colitis via alphavbeta1 integrin. J. Immunol. 2012, 188, 1108–1116. [Google Scholar] [CrossRef] [Green Version]
- Korner, A.; Bernard, A.; Fitzgerald, J.C.; Alarcon-Barrera, J.C.; Kostidis, S.; Kaussen, T.; Giera, M.; Mirakaj, V. Sema7A is crucial for resolution of severe inflammation. Proc. Natl. Acad. Sci. USA 2021, 118, e2017527118. [Google Scholar] [CrossRef]
- Zhao, N.; Zhang, X.; Ding, J.; Pan, Q.; Zheng, M.H.; Liu, W.Y.; Luo, G.; Qu, J.; Li, M.; Li, L.; et al. SEMA7AR148W mutation promotes lipid accumulation and NAFLD progression via increased localization on the hepatocyte surface. JCI Insight 2022, 7, e154113. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No Fibrosis n = 39 | Fibrosis Stage 1,2 n = 42 | Fibrosis Stage 3,4 n = 14 | |
|---|---|---|---|
| Age, years | 53 (46–65) | 55 (42–64) | 53 (49–68) |
| Male sex | 12 (30.7%) | 29 (69%) | 8 (57.1%) |
| Diabetes mellitus | 13 (33.3%) | 8 (19.0%) | 4 (28.5%) |
| Hypertension | 20 (51.8%) | 19 (45.2%) | 8 (57.1%) |
| Dyslipidemia | 10 (25.6%) | 12 (28.6%) | 5 (35.7%) |
| BMI, kg/m2 | 30 (28–33) | 31 (28–33) | 32 (27–35) |
| Waist hip ratio (WHR) | 0.91 (0.88–0.98) | 0.97 (0.94–0.99) | 0.98 (0.88–1.1) |
| Waist height ratio (WHtR) | 0.59 (0.56–0.62) | 0.62 (0.58–0.67) | 0.57 (0.52–0.63) |
| Neutrophils/lymphocytes ratio | 1.8 (1.5–2.2) | 2.0 (1.4–2.6) | 1.4 (1.1–2.3) |
| Bilirubin, µmol/L | 11 (8–14) | 13 (9–15) | 15 (8.5–15) |
| AST, IU/L | 27 (20–34) | 30 (24–39) | 46 (25–77) |
| ALT, IU/L | 35 (22–56) | 44 (32–59) | 58 (39–115) |
| GGT, IU/L | 33 (20–77) | 51 (30–101) | 78 (37–127) |
| Cholesterol, mmol/L | 5.3 (4.2–6.1) | 5.3 (4.7–5.9) | 6.0 (4.5–6.9) |
| Triglycerides, mmol/L | 1.6 (1.3–2.3) | 1.5 (1.1–2.1) | 1.7 (1.6–3.3) |
| LDL, mmol/L | 2.9 (2.4–3.8) | 3.3 (2.9–4.3) | 3.5 (1.9–4.5) |
| HDL, mmol/L | 1.3 (1.0–1.4) | 1.2 (1.0–1.6) | 1.2 (0.94–1.3) |
| APRI score | 0.28 (0.17–0.35) | 0.34 (0.22–0.46) | 0.68 (0.27–1.3) |
| FIB-4 score | 1.0 (0.79–1.4) | 0.95 (0.66–1.4) | 1.4 (0.94–4.0) |
| Liver stiffness, kPa | 4.3 (3.7–4.8) | 6.8 (6.1–7.4) | 15 (9.9–25) |
| CAP, dB/m | 305 (279–353) | 307 (287–335) | 330 (290–391) |
| Steatosis grade 1 | 11 (28.2%) | 9 (21.4%) | 2 (14.3%) |
| Steatosis grade 2 | 6 (15.4%) | 7 (16.7%) | 2 (14.3%) |
| Steatosis grade 3 | 22 (56.4%) | 26 (61.9%) | 10 (71.4%) |
| NAFLD n = 95 | Healthy Controls n = 35 | p-Value 1 | |
|---|---|---|---|
| SEMA5A rs1319222 | |||
| TT | 50 (52.2%) | 6 (18.5%) | |
| GG | 5 (5.3%) | 5 (14.3%) | |
| GT | 34 (36.2%) | 18 (51.4%) | 0.0031 |
| Undetermined | 5 (6.3%) | 5 (14.3%) | |
| SEMA5A rs433755 | |||
| AA | 26 (27.5%) | 12 (33.3%) | |
| AC | 41(43.5%) | 17 (48.1%) | 0.3248 |
| CC | 21 (21.7%) | 6 (18.5%) | |
| Undetermined | 7 (7.2%) | 0 | |
| SEMA4A rs536857 | |||
| AA | 15 (15.9%) | 3 (7.4%) | |
| AG | 25 (26.1%) | 10 (29.6%) | 0.1089 |
| GG | 28 (29.0%) | 17 (48.1%) | |
| Undetermined | 28 (29.0%) | 5 (14.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Šamadan, L.; Papić, N.; Mijić, M.; Knežević Štromar, I.; Gašparov, S.; Vince, A. Do Semaphorins Play a Role in Development of Fibrosis in Patients with Nonalcoholic Fatty Liver Disease? Biomedicines 2022, 10, 3014. https://doi.org/10.3390/biomedicines10123014
Šamadan L, Papić N, Mijić M, Knežević Štromar I, Gašparov S, Vince A. Do Semaphorins Play a Role in Development of Fibrosis in Patients with Nonalcoholic Fatty Liver Disease? Biomedicines. 2022; 10(12):3014. https://doi.org/10.3390/biomedicines10123014
Chicago/Turabian StyleŠamadan, Lara, Neven Papić, Maja Mijić, Ivana Knežević Štromar, Slavko Gašparov, and Adriana Vince. 2022. "Do Semaphorins Play a Role in Development of Fibrosis in Patients with Nonalcoholic Fatty Liver Disease?" Biomedicines 10, no. 12: 3014. https://doi.org/10.3390/biomedicines10123014