
Identification of a Fatty Acid for Diagnosing Non-Alcoholic Steatohepatitis in Patients with Severe Obesity Undergoing Metabolic Surgery
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Data Collection
2.3. Lipidomics Analysis
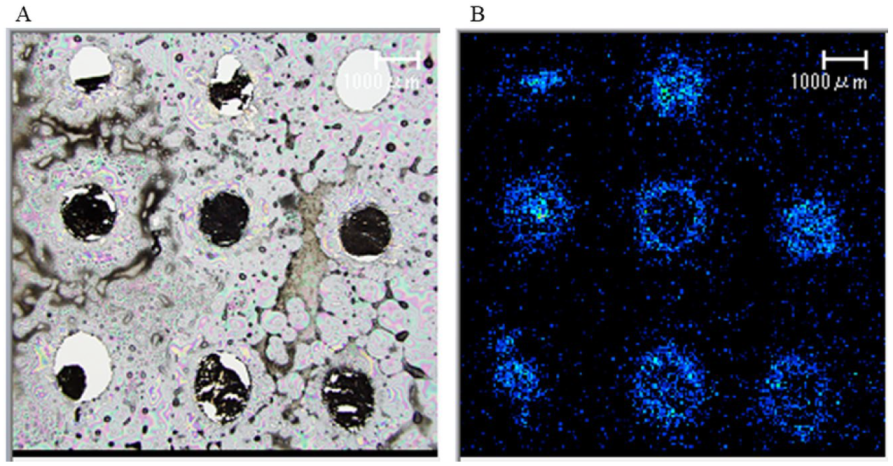
2.4. Matrix-Assisted Laser Desorption/Ionization-Imaging Mass Spectrometry (MALDI-IMS)
2.5. Liver Histology
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Weight Loss and Metabolic Improvement Effects
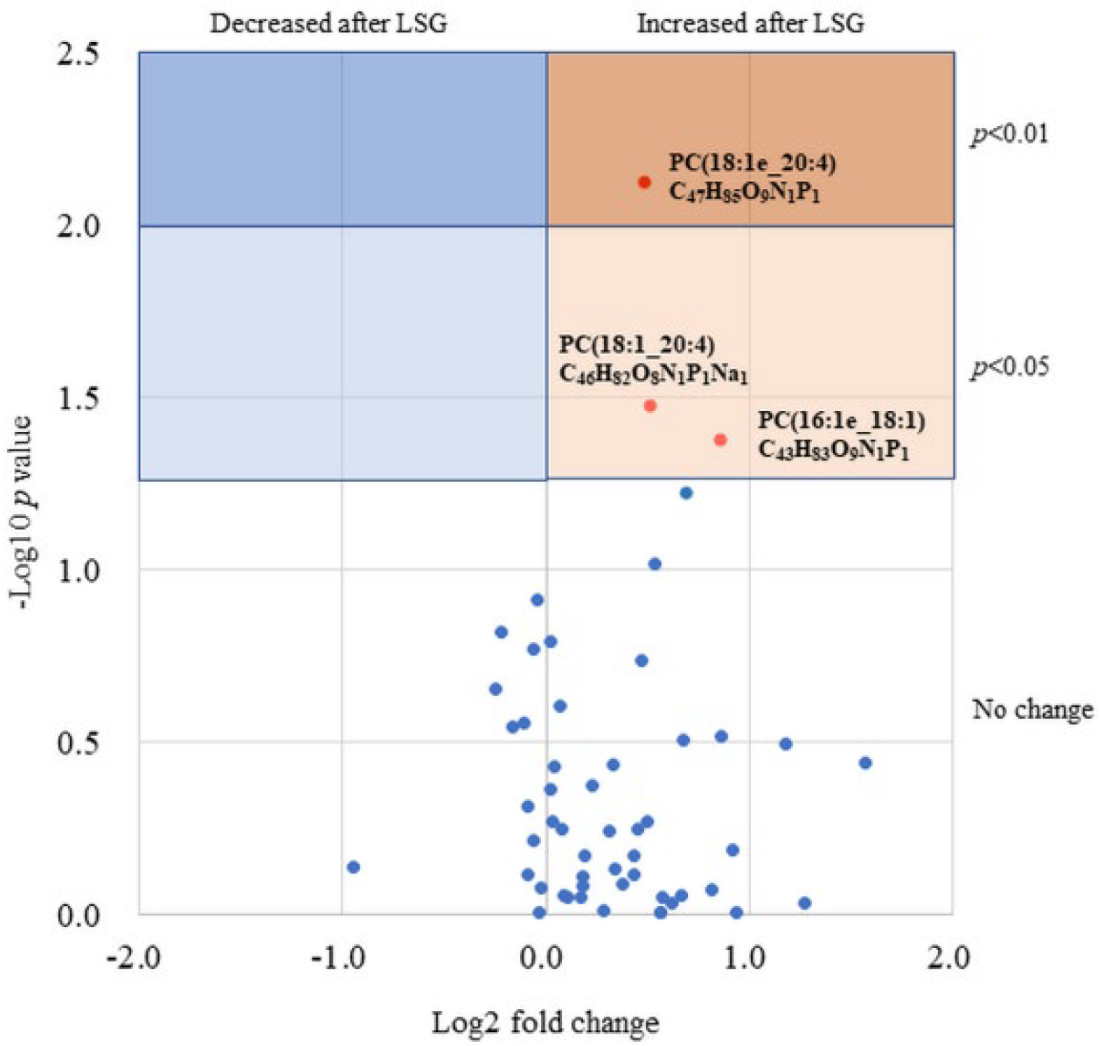
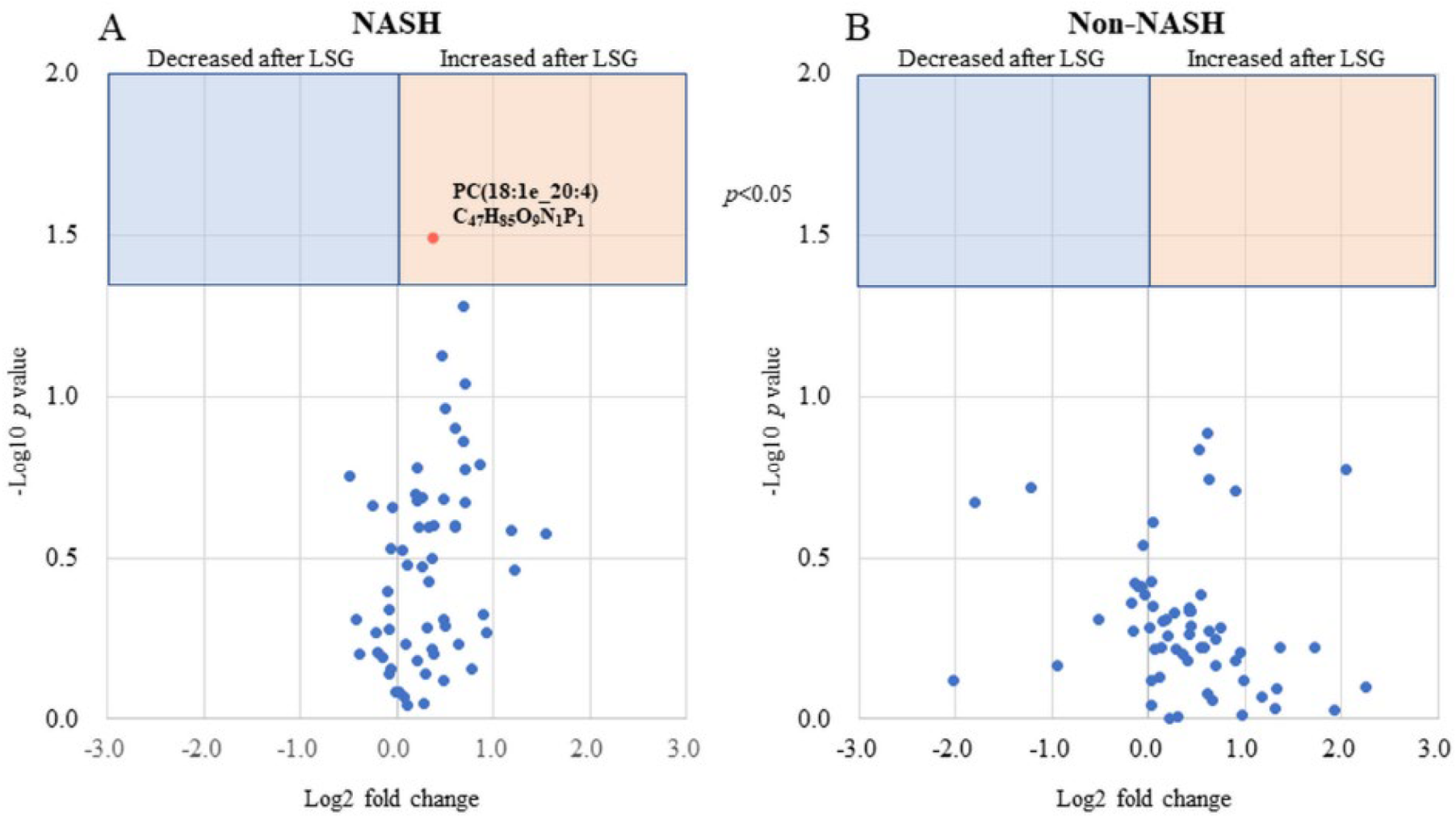
3.3. Serum FFA Analysis
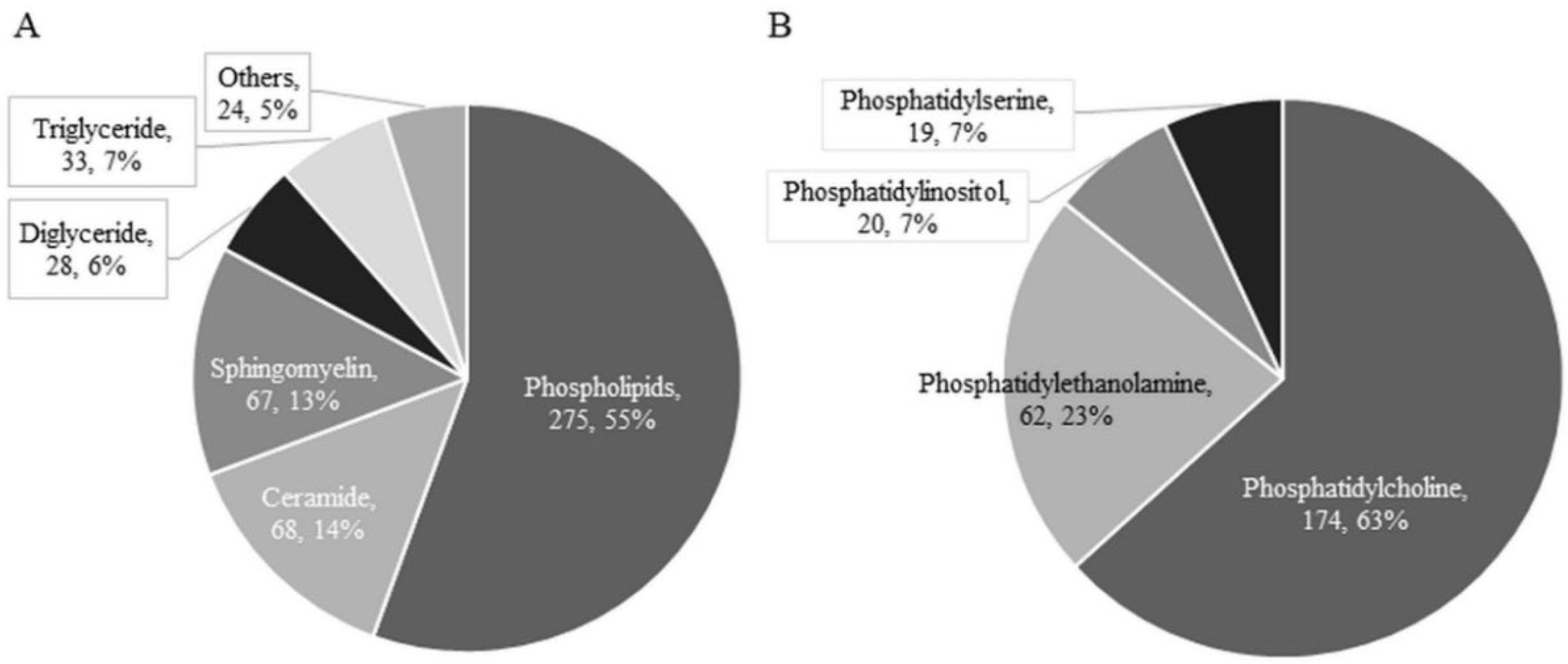
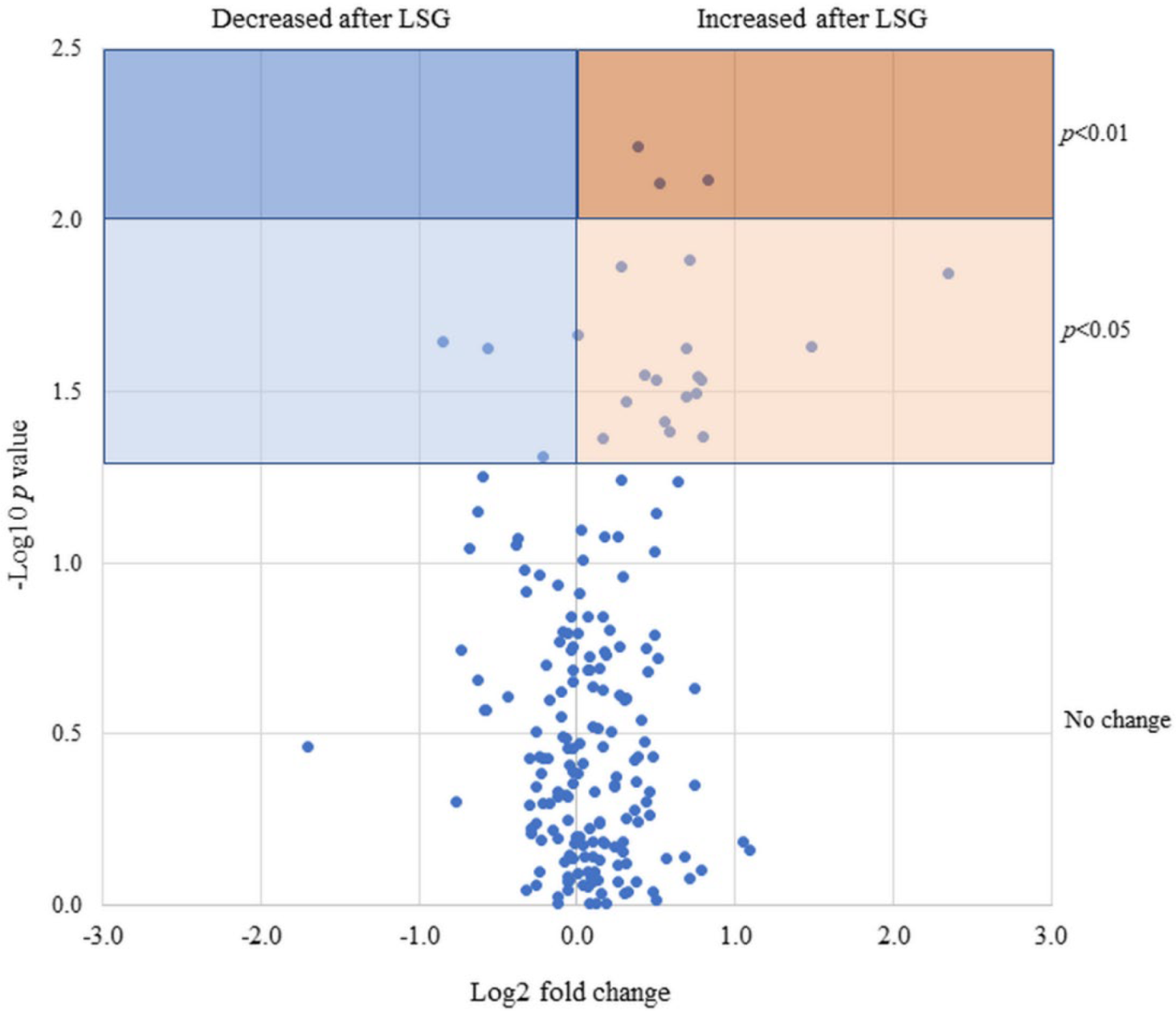
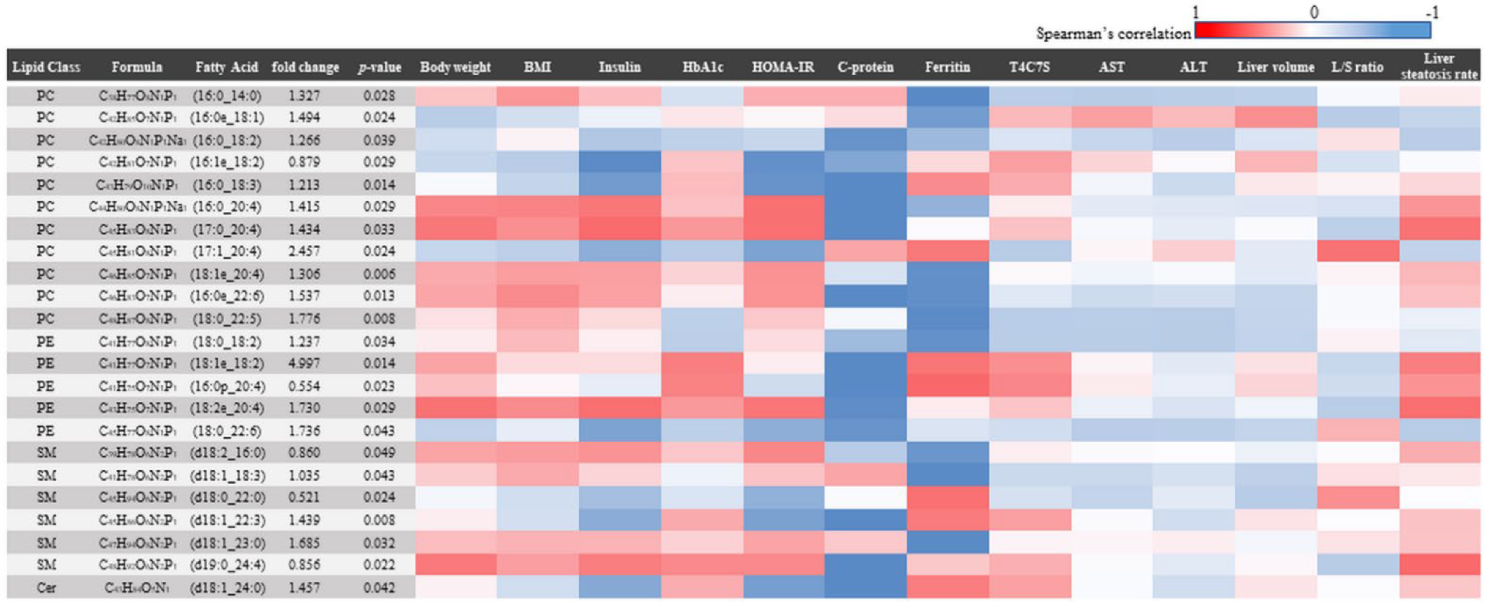
3.4. FA Analysis of Liver Tissue
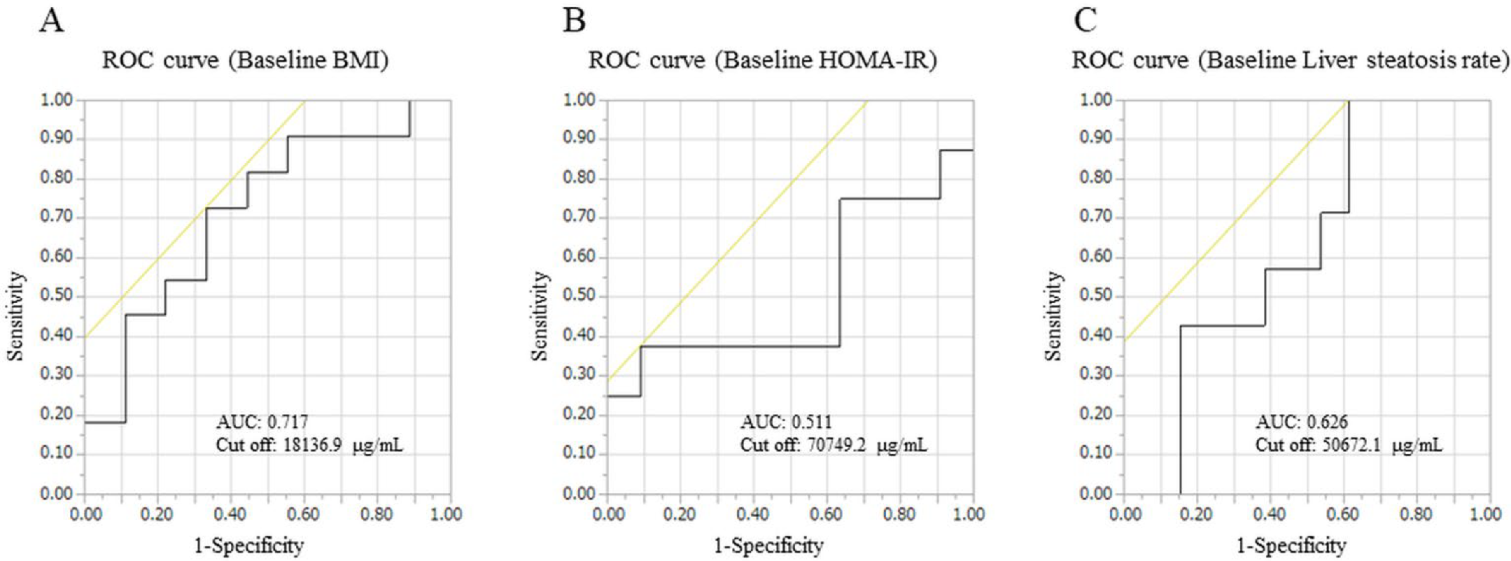
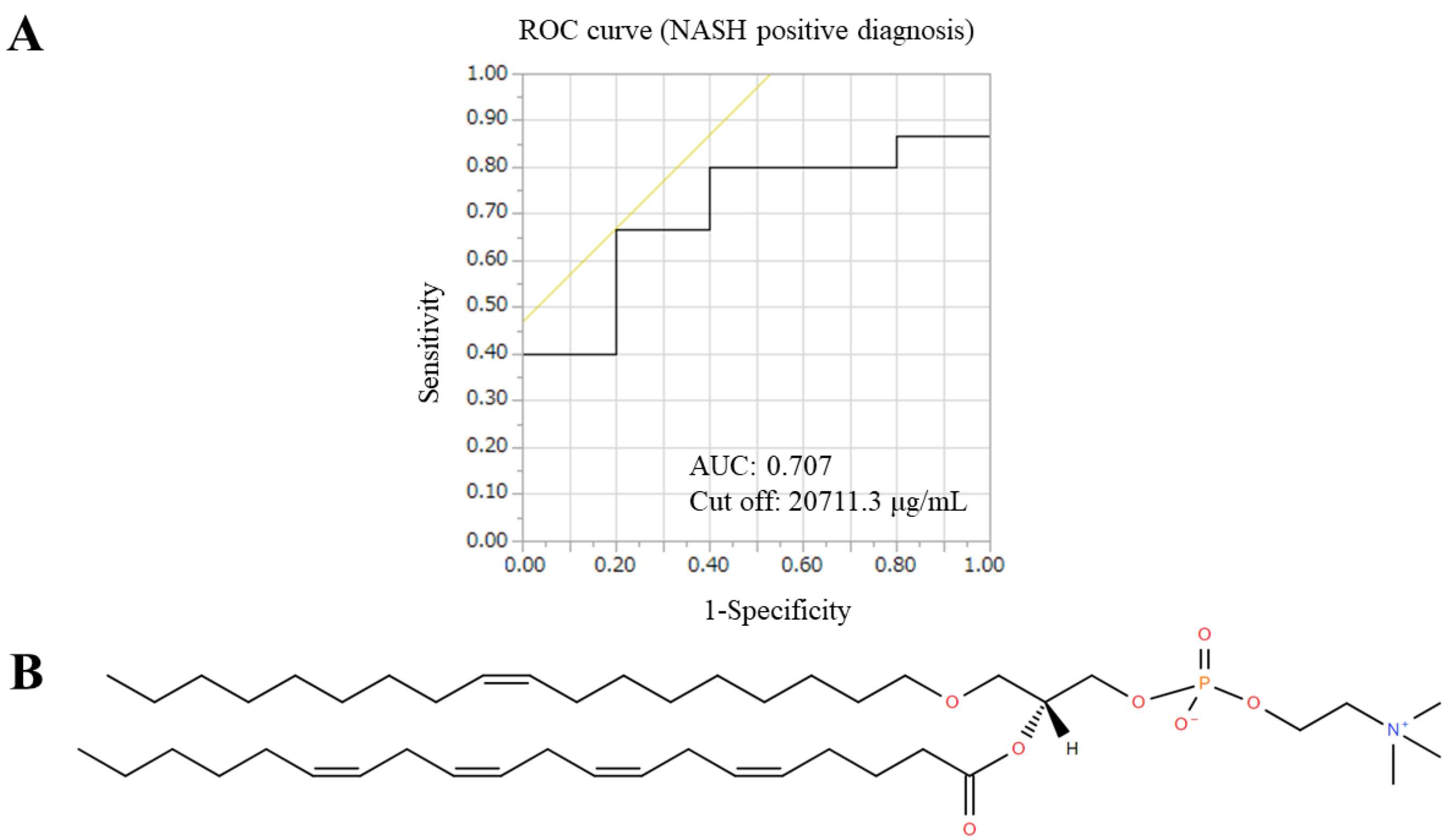
3.5. Validity as a Surrogate Marker
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Flegal, K.M.; Carroll, M.D.; Ogden, C.L.; Curtin, L.R. Prevalence and Trends in Obesity Among US Adults, 1999–2008. JAMA 2010, 303, 235–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, A.; Nitta, H.; Otsuka, K.; Umemura, A.; Baba, S.; Obuchi, T.; Wakabayashi, G. Bariatric Surgery and Non-Alcoholic Fatty Liver Disease: Current and Potential Future Treatments. Front. Endocrinol. 2014, 5, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nikai, H.; Ishida, K.; Umemura, A.; Baba, S.; Nitta, H.; Sugai, T.; Sasaki, A. Effects of Laparoscopic Sleeve Gastrectomy on Non-Alcoholic Steatohepatitis and Liver Fibrosis in Japanese Patients with Severe Obesity. Obes. Surg. 2020, 30, 2579–2587. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, A.; Umemura, A.; Ishida, K.; Takahashi, N.; Nikai, H.; Nitta, H.; Takikawa, Y.; Kakisaka, K.; Abe, T.; Nishiya, M.; et al. The Concept of Indeterminable NASH Inducted by Preoperative Diet and Metabolic Surgery: Analyses of Histopathological and Clinical Features. Biomedicines 2022, 10, 453. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef] [PubMed]
- Barbois, S.; Arvieux, C.; Leroy, V.; Reche, F.; Stürm, N.; Borel, A.-L. Benefit–risk of intraoperative liver biopsy during bariatric surgery: Review and perspectives. Surg. Obes. Relat. Dis. 2017, 13, 1780–1786. [Google Scholar] [CrossRef]
- Spengler, E.K.; Loomba, R. Recommendations for Diagnosis, Referral for Liver Biopsy, and Treatment of Nonalcoholic Fatty Liver Disease and Nonalcoholic Steatohepatitis. Mayo Clin. Proc. 2015, 90, 1233–1246. [Google Scholar] [CrossRef] [Green Version]
- Boden, G. Obesity, insulin resistance and free fatty acids. Curr. Opin. Endocrinol. Diabetes Obes. 2011, 18, 139–143. [Google Scholar] [CrossRef] [Green Version]
- Feng, R.; Luo, C.; Li, C.; Du, S.; Okekunle, A.P.; Li, Y.; Chen, Y.; Zi, T.; Niu, Y. Free fatty acids profile among lean, overweight and obese non-alcoholic fatty liver disease patients: A case–control study. Lipids Health Dis. 2017, 16, 165. [Google Scholar] [CrossRef] [Green Version]
- Lin, C.; Våge, V.; Mjøs, S.A.; Kvalheim, O.M. Changes in Serum Fatty Acid Levels During the First Year After Bariatric Surgery. Obes. Surg. 2015, 26, 1735–1742. [Google Scholar] [CrossRef]
- Rodríguez-Gallego, E.; Guirro, M.; Riera-Borrull, M.; Hernández-Aguilera, A.; Mariné-Casadó, R.; Fernández-Arroyo, S.; Beltrán-Debón, R.; Sabench, F.; Hernández, M.; Del Castillo, D.; et al. Mapping of the circulating metabolome reveals α-ketoglutarate as a predictor of morbid obesity-associated non-alcoholic fatty liver disease. Int. J. Obes. 2014, 39, 279–287. [Google Scholar] [CrossRef]
- Sasaki, A.; Yokote, K.; Naitoh, T.; Fujikura, J.; Hayashi, K.; Hirota, Y.; Inagaki, N.; Ishigaki, Y.; Kasama, K.; Kikkawa, E.; et al. Metabolic surgery in treatment of obese Japanese patients with type 2 diabetes: A joint consensus statement from the Japanese Society for Treatment of Obesity, the Japan Diabetes Society, and the Japan Society for the Study of Obesity. Diabetol. Int. 2021, 13, 1–30. [Google Scholar] [CrossRef]
- Sumida, Y.; Japan Study Group of Nonalcoholic Fatty Liver Disease (JSG-NAFLD); Yoneda, M.; Hyogo, H.; Yamaguchi, K.; Ono, M.; Fujii, H.; Eguchi, Y.; Suzuki, Y.; Imai, S.; et al. A simple clinical scoring system using ferritin, fasting insulin, and type IV collagen 7S for predicting steatohepatitis in nonalcoholic fatty liver disease. J. Gastroenterol. 2010, 46, 257–268. [Google Scholar] [CrossRef]
- Shah, A.G.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J.; Nash Clinical Research Network. Use of the fib4 index for non-invasive evaluation of fibrosis in nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef] [Green Version]
- Angulo, P.; Hui, J.M.; Marchesini, G.; Bugianesi, E.; George, J.; Farrell, G.C.; Enders, F.; Saksena, S.; Burt, A.D.; Bida, J.P.; et al. The NAFLD fibrosis score: A noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology 2007, 45, 846–854. [Google Scholar] [CrossRef]
- Yamada, T.; Uchikata, T.; Sakamoto, S.; Yokoi, Y.; Fukusaki, E.; Bamba, T. Development of a lipid profiling system using reverse-phase liquid chromatography coupled to high-resolution mass spectrometry with rapid polarity switching and an automated lipid identification software. J. Chromatogr. A 2013, 1292, 211–218. [Google Scholar] [CrossRef]
- Sakurai, N.; Shibata, D. Tools and databases for an integrated metabolite annotation environment for liquid chromatog-raphy-mass spectrometry-based untargeted metabolomics. Carotenoid Sci. 2017, 22, 16–22. [Google Scholar]
- Sakurai, N.; Narise, T.; Sim, J.-S.; Lee, C.-M.; Ikeda, C.; Akimoto, N.; Kanaya, S. UC2 search: Using unique connectivity of uncharged compounds for metabolite annotation by database searching in mass spectrometry-based metabolomics. Bioinformatics 2017, 34, 698–700. [Google Scholar] [CrossRef] [Green Version]
- Afendi, F.M.; Okada, T.; Yamazaki, M.; Hirai-Morita, A.; Nakamura, Y.; Nakamura, K.; Ikeda, S.; Takahashi, H.; Amin, A.U.; Darusman, L.K.; et al. KNApSAcK Family Databases: Integrated Metabolite–Plant Species Databases for Multifaceted Plant Research. Plant Cell Physiol. 2011, 53, e1. [Google Scholar] [CrossRef] [Green Version]
- Sakurai, N.; Ara, T.; Kanaya, S.; Nakamura, Y.; Iijima, Y.; Enomoto, M.; Motegi, T.; Aoki, K.; Suzuki, H.; Shibata, D. An application of a relational database system for high-throughput prediction of elemental compositions from accurate mass values. Bioinformatics 2012, 29, 290–291. [Google Scholar] [CrossRef] [Green Version]
- Worley, B. Multivariate Analysis in Metabolomics. Curr. Metabolomics 2012, 1, 92–107. [Google Scholar] [CrossRef]
- Harada, T.; Yuba-Kubo, A.; Sugiura, Y.; Zaima, N.; Hayasaka, T.; Goto-Inoue, N.; Wakui, M.; Suematsu, M.; Takeshita, K.; Ogawa, K.; et al. Visualization of Volatile Substances in Different Organelles with an Atmospheric-Pressure Mass Microscope. Anal. Chem. 2009, 81, 9153–9157. [Google Scholar] [CrossRef] [PubMed]
- Kleiner, D.E.; Brunt, E.M.; Van Natta, M.; Behling, C.; Contos, M.J.; Cummings, O.W.; Ferrell, L.D.; Liu, Y.-C.; Torbenson, M.S.; Unalp-Arida, A.; et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology 2005, 41, 1313–1321. [Google Scholar] [CrossRef] [PubMed]
- Tokushige, K.; Ikejima, K.; Ono, M.; Eguchi, Y.; Kamada, Y.; Itoh, Y.; Akuta, N.; Yoneda, M.; Iwasa, M.; Yoneda, M.; et al. Evidence-based clinical practice guidelines for nonalcoholic fatty liver disease/nonalcoholic steatohepatitis 2020. Hepatol. Res. 2021, 51, 1013–1025. [Google Scholar] [CrossRef]
- Brunt, E.M.; Janney, C.G.; Di Bisceglie, A.M.; Neuschwander-Tetri, B.A.; Bacon, B.R. Nonalcoholic Steatohepatitis: A Proposal for Grading and Staging the Histological Lesions. Am. J. Gastroenterol. 1999, 94, 2467–2474. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Koulman, A.; Sharp, S.J.; Imamura, F.; Kröger, J.; Schulze, M.B.; Crowe, F.L.; Huerta, J.M.; Guevara, M.; Beulens, J.W.; et al. Differences in the prospective association between individual plasma phospholipid saturated fatty acids and incident type 2 diabetes: The EPIC-InterAct case-cohort study. Lancet Diabetes Endocrinol. 2014, 2, 810–818. [Google Scholar] [CrossRef] [Green Version]
- Boden, G. Effects of Free Fatty Acids (FFA) on Glucose Metabolism: Significance for Insulin Resistance and Type 2 Diabetes. Exp. Clin. Endocrinol. Diabetes 2003, 111, 121–124. [Google Scholar] [CrossRef]
- Boden, G.; I Shulman, G. Free fatty acids in obesity and type 2 diabetes: Defining their role in the development of insulin resistance and β-cell dysfunction. Eur. J. Clin. Investig. 2002, 32 (Suppl. S3), 14–23. [Google Scholar] [CrossRef]
- Pereira-Lancha, L.O.; Coelho, D.F.; de Campos-Ferraz, P.L.; Lancha, A.H., Jr. Body Fat Regulation: Is It a Result of a Simple Energy Balance or a High Fat Intake? J. Am. Coll. Nutr. 2010, 29, 343–351. [Google Scholar] [CrossRef]
- Boateng, L.; Ansong, R.; Owusu, W.B.; Asiedu, M.S. Coconut oil and palm oil’s role in nutrition, health and national devel-opment: A review. Ghana Med. J. 2016, 50, 189–196. [Google Scholar] [CrossRef]
- Siri-Tarino, P.W.; Sun, Q.; Hu, F.B.; Krauss, R.M. Saturated Fatty Acids and Risk of Coronary Heart Disease: Modulation by Replacement Nutrients. Curr. Atheroscler. Rep. 2010, 12, 384–390. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; Lucan, S.; O’Keefe, J.H. The Evidence for Saturated Fat and for Sugar Related to Coronary Heart Disease. Prog. Cardiovasc. Dis. 2015, 58, 464–472. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuthbertson, D.; Steele, T.; Wilding, J.; Halford, J.C.; A Harrold, J.; Hamer, M.; Karpe, F. What have human experimental overfeeding studies taught us about adipose tissue expansion and susceptibility to obesity and metabolic complications? Int. J. Obes. 2017, 41, 853–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nowak, J.Z. Anti-inflammatory pro-resolving derivatives of omega-3 and omega-6 polyunsaturated fatty acids. Postepy Hig. Med. Dosw. Online 2010, 64, 115–132. [Google Scholar] [PubMed]
- Watanabe, S.; Sakai, N.; Yasui, Y.; Kimura, Y.; Kobayashi, T.; Mizutani, T.; Okuyama, H. A high alpha-linolenate diet suppresses antigen-induced immunoglobulin E response and anaphylactic shock in mice. J. Nutr. 1994, 124, 1566–1573. [Google Scholar] [CrossRef]
- Huang, C.Y.; Sheu, W.H.; Chiang, A.N. Docosahexaenoic acid and eicosapentaenoic acid suppress adhesion molecule ex-pression in human aortic endothelial cells via differential mechanisms. Mol. Nutr. Food Res. 2015, 59, 751–762. [Google Scholar] [CrossRef]
- Bucher, H.C.; Hengstler, P.; Schindler, C.; Meier, G. N-3 polyunsaturated fatty acids in coronary heart disease: A meta-analysis of randomized controlled trials. Am. J. Med. 2002, 112, 298–304. [Google Scholar] [CrossRef]
- Ni, Y.; Zhao, L.; Yu, H.; Ma, X.; Bao, Y.; Rajani, C.; Loo, L.W.; Shvetsov, Y.B.; Yu, H.; Chen, T.; et al. Circulating Unsaturated Fatty Acids Delineate the Metabolic Status of Obese Individuals. eBioMedicine 2015, 2, 1513–1522. [Google Scholar] [CrossRef] [Green Version]
- Reis, A.; Spickett, C.M. Chemistry of phospholipid oxidation. Biochim. Biophys. Acta (BBA)-Biomembr. 2012, 1818, 2374–2387. [Google Scholar] [CrossRef] [Green Version]
- Wattacheril, J.; Seeley, E.H.; Angel, P.; Chen, H.; Bowen, B.P.; Lanciault, C.; Caprioli, R.M.; Abumrad, N.; Flynn, C.R. Differential Intrahepatic Phospholipid Zonation in Simple Steatosis and Nonalcoholic Steatohepatitis. PLoS ONE 2013, 8, e57165. [Google Scholar] [CrossRef] [Green Version]
- Mitrovic, M.; Sistilli, G.; Horakova, O.; Rossmeisl, M. Omega-3 phospholipids and obesity-associated NAFLD: Potential mechanisms and therapeutic perspectives. Eur. J. Clin. Investig. 2021, 52, e13650. [Google Scholar] [CrossRef]
- Sun, X.; Seidman, J.S.; Zhao, P.; Troutman, T.D.; Spann, N.J.; Que, X.; Zhou, F.; Liao, Z.; Pasillas, M.; Yang, X.; et al. Neutralization of Oxidized Phospholipids Ameliorates Non-alcoholic Steatohepatitis. Cell Metab. 2019, 31, 189–206.e8. [Google Scholar] [CrossRef]
- Kang, M.-J.; Fujino, T.; Sasano, H.; Minekura, H.; Yabuki, N.; Nagura, H.; Iijima, H.; Yamamoto, T.T. A novel arachidonate-preferring acyl-CoA synthetase is present in steroidogenic cells of the rat adrenal, ovary, and testis. Proc. Natl. Acad. Sci. USA 1997, 94, 2880–2884. [Google Scholar] [CrossRef] [Green Version]
- Manca, C.; Pintus, S.; Murru, E.; Fantola, G.; Vincis, M.; Batetta, B.; Moroni, E.; Carta, G.; Banni, S. Fatty Acid Metabolism and Derived-Mediators Distinctive of PPAR-α Activation in Obese Subjects Post Bariatric Surgery. Nutrients 2021, 13, 4340. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 20) | NASH (n = 15) | Non-NASH (n = 5) | p-Value (NASH vs. Non-NASH) | |
|---|---|---|---|---|
| Age (years) | 38.3 ± 12.0 | 37.3 ± 12.3 | 42 ± 11.4 | 0.499 |
| Male (n,%) | 6, 30.0 | 5, 31.3 | 1, 25.0 | 0.819 |
| T2D (n,%) | 9, 45.0 | 8, 50.0 | 1, 25.0 | 0.395 |
| Body weight (kg) | 118.7 ± 21.8 | 120.4 ± 22.3 | 111.9 ± 21.5 | 0.500 |
| BMI (kg/m2) | 43.9 ± 4.9 | 44.8 ± 4.9 | 40.5 ± 2.9 | 0.115 |
| Insulin (μU/mL) | 16.8 ± 6.2 | 17.3 ± 6.7 | 14.9 ± 3.4 | 0.500 |
| FBS (mg/dL) | 114.4 ± 35.9 | 119.5 ± 38.2 | 94.0 ± 13.8 | 0.212 |
| HbA1c (%) | 6.8 ± 1.2 | 6.9 ± 1.2 | 6.0 ± 0.4 | 0.172 |
| HOMA-IR (no unit) | 4.6 ± 1.7 | 4.9 ± 1.8 | 3.4 ± 0.6 | 0.134 |
| HOMA-β (no unit) | 176.6 ± 126.7 | 168.9 ± 134.7 | 205.7 ± 101.5 | 0.620 |
| C-peptide (ng/mL) | 3.0 ± 1.2 | 3.1 ± 1.3 | 2.4 ± 0.2 | 0.465 |
| Ferritin (ng/mL) | 147.8 ± 178.8 | 162.6 ± 196.3 | 84.0 ± 33.0 | 0.511 |
| T4C7S (ng/mL) | 4.8 ± 1.1 | 4.9 ± 1.1 | 4.4 ± 1.0 | 0.452 |
| VFA (cm2) | 252.6 ± 87.9 | 251.1 ± 89.7 | 259.7 ± 97.3 | 0.884 |
| Waist (cm) | 120.8 ± 12.3 | 121.2 ± 13.1 | 118.7 ± 9.6 | 0.761 |
| Liver volume (mL) | 2259.1 ± 446.3 | 2337.6 ± 445.3 | 1945.3 ± 344.8 | 0.182 |
| L/S ratio | 0.8 ± 0.2 | 0.8 ± 0.2 | 0.9 ± 0.3 | 0.378 |
| NAFIC (point) | 1.6 ± 1.0 | 1.4 ± 0.9 | 2.0 ± 1.2 | 0.406 |
| FIB-4 (point) | 0.8 ± 0.8 | 0.9 ± 0.9 | 0.5 ± 0.2 | 0.100 |
| NFS (point) | 1.2 ± 1.7 | 1.5 ± 1.6 | 0.4 ± 2.0 | 0.303 |
| NASH Baseline (n = 15) | NASH Continuation (n = 8) | NASH Improved (n = 7) | p-Value (Continuation vs. Improved) | |
|---|---|---|---|---|
| Steatosis rate (%) | 25.7 ± 17.1 | 7.1 ± 2.7 | 5.9 ± 6.4 | 0.638 |
| PFS (point) | 1.5 ± 0.9 | 2.1 ± 0.9 | 0.7 ± 0.8 | 0.010 |
| NAS steatosis (point) | 1.3 ± 0.5 | 0.8 ± 0.4 | 0.3 ± 0.5 | 0.094 |
| NAS inflammation (point) | 1.1 ± 0.4 | 0.6 ± 0.5 | 0.3 ± 0.5 | 0.317 |
| NAS ballooning (point) | 0.5 ± 0.6 | 0.3 ± 0.8 | 0.0 ± 0.0 | 0.356 |
| NAS total (point) | 2.9 ± 0.9 | 1.6 ± 1.4 | 0.6 ± 0.8 | 0.132 |
| Brunt inflammation (point) | 0.9 ± 0.3 | 1.1 ± 0.4 | 0.7 ± 0.5 | 0.093 |
| Brunt fibrosis (point) | 1.4 ± 0.6 | 1.3 ± 1.3 | 0.4 ± 0.8 | 0.156 |
| Baseline | 6 Months after LSG | Continuation vs. Improved (6 Months after LSG) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Lipid Class | Formula | NASH | Non-NASH | p-Value | NASH | Non-NASH | p-Value | NASH Continuation | NASH Improved | p-Value |
| PC(16:0e_16:1) | C40H81O7N1P1 | 7062.6 | 23,758.3 | 0.015 | 12,492.9 | 20,665.9 | 0.441 | 18,439.2 | 5697.1 | 0.239 |
| PC(16:0e_18:1) | C42H85O7N1P1 | 4,569,271.9 | 11,999,844.0 | 0.047 | 5,198,314.3 | 12,383,645.0 | 0.098 | 6,060,208.6 | 4,213,292.3 | 0.654 |
| PC(16:1e_18:2) | C42H81O7N1P1 | 298,943.3 | 770,318.8 | 0.050 | 315,576.7 | 605,506.6 | 0.030 | 395,094.5 | 224,699.2 | 0.164 |
| PC(16:0e_20:4) | C44H83O7N1P1 | 7689.8 | 30,707.7 | 0.064 | 16,365.2 | 58,769.0 | 0.032 | 18,230.5 | 14,233.5 | 0.804 |
| PC(18:1e_20:4) | C46H85O7N1P1 | 21,9594.4 | 277,865.5 | 0.224 | 344,802.5 | 436,341.1 | 0.050 | 401,461.4 | 280,049.5 | 0.419 |
| PE(18:0_20:4) | C43H77O8N1P1 | 12,511.4 | 65,084.8 | 0.007 | 15,613.8 | 24,979.4 | 0.399 | 25,130.9 | 4737.1 | 0.069 |
| PI(18:0_20:4) | C47H82O13N0P1 | 47,376.4 | 91,142.9 | 0.150 | 54,536.2 | 118,370.1 | 0.044 | 64,666.8 | 42,958.3 | 0.450 |
| SM(d18:1_22:0) | C46H92O8N2P1 | 331,092.1 | 113,458.9 | 0.046 | 315,178.6 | 160,150.2 | 0.166 | 354,962.2 | 269,711.6 | 0.456 |
| SM(d18:1_24:3) | C47H90O6N2P1 | 599,456.7 | 2,241,115.3 | 0.050 | 555,019.4 | 623,832.8 | 0.894 | 744,161.8 | 338,856.6 | 0.428 |
| Cer(d18:1_23:0) | C42H82O5N1 | 95,317.8 | 442,889.9 | 0.040 | 127,706.1 | 185,562.2 | 0.473 | 150,156.7 | 102,048.2 | 0.558 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takahashi, N.; Sasaki, A.; Umemura, A.; Sugai, T.; Kakisaka, K.; Ishigaki, Y. Identification of a Fatty Acid for Diagnosing Non-Alcoholic Steatohepatitis in Patients with Severe Obesity Undergoing Metabolic Surgery. Biomedicines 2022, 10, 2920. https://doi.org/10.3390/biomedicines10112920
Takahashi N, Sasaki A, Umemura A, Sugai T, Kakisaka K, Ishigaki Y. Identification of a Fatty Acid for Diagnosing Non-Alcoholic Steatohepatitis in Patients with Severe Obesity Undergoing Metabolic Surgery. Biomedicines. 2022; 10(11):2920. https://doi.org/10.3390/biomedicines10112920
Chicago/Turabian StyleTakahashi, Naoto, Akira Sasaki, Akira Umemura, Tamotsu Sugai, Keisuke Kakisaka, and Yasushi Ishigaki. 2022. "Identification of a Fatty Acid for Diagnosing Non-Alcoholic Steatohepatitis in Patients with Severe Obesity Undergoing Metabolic Surgery" Biomedicines 10, no. 11: 2920. https://doi.org/10.3390/biomedicines10112920