
Association of Pain Phenotypes with Risk of Falls and Incident Fractures
 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Measurements for Factors to Identify Pain Phenotypes
2.3. Measurements for Outcomes
2.3.1. Incident Fractures
2.3.2. Falls Risk Score
2.4. Measurements for Other Related Factors
2.5. Statistical Analysis
2.5.1. Identifying Pain Phenotypes
2.5.2. Comparing Risks of Falls and Incident Fractures over 10.7 Years across Three Knee Pain Phenotypes
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lehti, T.E.; Rinkinen, M.O.; Aalto, U.; Roitto, H.M.; Knuutila, M.; Öhman, H.; Kautiainen, H.; Karppinen, H.; Tilvis, R.; Strandberg, T.; et al. Prevalence of Musculoskeletal Pain and Analgesic Treatment Among Community-Dwelling Older Adults: Changes from 1999 to 2019. Drugs Aging 2021, 38, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Karttunen, N.M.; Turunen, J.H.; Ahonen, R.S.; Hartikainen, S.A. Persistence of noncancer-related musculoskeletal chronic pain among community-dwelling older people: A population-based longitudinal study in Finland. Clin. J. Pain 2015, 31, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Disease, G.B.D.; Injury, I.; Prevalence, C. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef] [Green Version]
- Briggs, A.M.; Cross, M.J.; Hoy, D.G.; Sànchez-Riera, L.; Blyth, F.M.; Woolf, A.D.; March, L. Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health. Gerontologist 2016, 56 (Suppl 2), S243–S255. [Google Scholar] [CrossRef] [Green Version]
- Blyth, F.M.; Briggs, A.M.; Schneider, C.H.; Hoy, D.G.; March, L.M. The Global Burden of Musculoskeletal Pain-Where to from Here? Am. J. Public Health 2019, 109, 35–40. [Google Scholar] [CrossRef]
- Kittelson, A.J.; George, S.Z.; Maluf, K.S.; Stevens-Lapsley, J.E. Future directions in painful knee osteoarthritis: Harnessing complexity in a heterogeneous population. Phys. Ther. 2014, 94, 422–432. [Google Scholar] [CrossRef] [Green Version]
- Butler, S. The impact of chronic pain—European patients’ perspective over 12 months. Scand. J. Pain 2012, 3, 21–22. [Google Scholar] [CrossRef]
- Meisingset, I.; Vasseljen, O.; Vøllestad, N.K.; Robinson, H.S.; Woodhouse, A.; Engebretsen, K.B.; Glette, M.; Øverås, C.K.; Nordstoga, A.L.; Evensen, K.A.I.; et al. Novel approach towards musculoskeletal phenotypes. Eur. J. Pain 2020, 24, 921–932. [Google Scholar] [CrossRef] [Green Version]
- ten Klooster, P.M.; de Graaf, N.; Vonkeman, H.E. Association between pain phenotype and disease activity in rheumatoid arthritis patients: A non-interventional, longitudinal cohort study. Arthritis Res. Ther. 2019, 21, 257. [Google Scholar] [CrossRef]
- Smith, D.; Wilkie, R.; Croft, P.; McBeth, J. Pain and Mortality in Older Adults: The Influence of Pain Phenotype. Arthritis Care Res. 2018, 70, 236–243. [Google Scholar] [CrossRef]
- Center, J.R.; Bliuc, D.; Nguyen, T.V.; Eisman, J.A. Risk of subsequent fracture after low-trauma fracture in men and women. JAMA 2007, 297, 387–394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center, J.R.; Nguyen, T.V.; Schneider, D.; Sambrook, P.N.; Eisman, J.A. Mortality after all major types of osteoporotic fracture in men and women: An observational study. Lancet 1999, 353, 878–882. [Google Scholar] [CrossRef]
- Klotzbuecher, C.M.; Ross, P.D.; Landsman, P.B.; Abbott, T.A., 3rd; Berger, M. Patients with prior fractures have an increased risk of future fractures: A summary of the literature and statistical synthesis. J. Bone Miner. Res. 2000, 15, 721–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stone, K.L.; Seeley, D.G.; Lui, L.Y.; Cauley, J.A.; Ensrud, K.; Browner, W.S.; Nevitt, M.C.; Cummings, S.R.; Osteoporotic Fractures Research, G. BMD at multiple sites and risk of fracture of multiple types: Long-term results from the Study of Osteoporotic Fractures. J. Bone Miner. Res. 2003, 18, 1947–1954. [Google Scholar] [CrossRef] [PubMed]
- Vranken, L.; Wyers, C.E.; van den Bergh, J.P.W.; Geusens, P. The Phenotype of Patients with a Recent Fracture: A Literature Survey of the Fracture Liaison Service. Calcif. Tissue Int. 2017, 101, 248–258. [Google Scholar] [CrossRef] [Green Version]
- Dore, A.L.; Golightly, Y.M.; Mercer, V.S.; Shi, X.A.; Renner, J.B.; Jordan, J.M.; Nelson, A.E. Lower-extremity osteoarthritis and the risk of falls in a community-based longitudinal study of adults with and without osteoarthritis. Arthritis Care Res. (Hoboken) 2015, 67, 633–639. [Google Scholar] [CrossRef] [Green Version]
- Gale, C.R.; Westbury, L.D.; Cooper, C.; Dennison, E.M. Risk factors for incident falls in older men and women: The English longitudinal study of ageing. BMC Geriatr. 2018, 18, 117. [Google Scholar] [CrossRef] [Green Version]
- Leveille, S.G.; Jones, R.N.; Kiely, D.K.; Hausdorff, J.M.; Shmerling, R.H.; Guralnik, J.M.; Kiel, D.P.; Lipsitz, L.A.; Bean, J.F. Chronic musculoskeletal pain and the occurrence of falls in an older population. JAMA 2009, 302, 2214–2221. [Google Scholar] [CrossRef]
- Welsh, V.K.; Clarson, L.E.; Mallen, C.D.; McBeth, J. Multisite pain and self-reported falls in older people: Systematic review and meta-analysis. Arthritis Res. Ther. 2019, 21, 67. [Google Scholar] [CrossRef] [Green Version]
- Cauley, J.A.; Barbour, K.E.; Harrison, S.L.; Cloonan, Y.K.; Danielson, M.E.; Ensrud, K.E.; Fink, H.A.; Orwoll, E.S.; Boudreau, R. Inflammatory Markers and the Risk of Hip and Vertebral Fractures in Men: The Osteoporotic Fractures in Men (MrOS). J. Bone Miner. Res. 2016, 31, 2129–2138. [Google Scholar] [CrossRef]
- Eriksson, A.L.; Movérare-Skrtic, S.; Ljunggren, Ö.; Karlsson, M.; Mellström, D.; Ohlsson, C. High-Sensitivity CRP Is an Independent Risk Factor for All Fractures and Vertebral Fractures in Elderly Men: The MrOS Sweden Study. J. Bone Miner. Res. 2014, 29, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Tian, J.; Aitken, D.; Cicuttini, F.; Jones, G. Pain at multiple sites is associated with prevalent and incident fractures in older adults. J. Bone Miner. Res. 2019, 34, 2012–2018. [Google Scholar] [CrossRef] [PubMed]
- Arden, N.K.; Crozier, S.; Smith, H.; Anderson, F.; Edwards, C.; Raphael, H.; Cooper, C. Knee pain, knee osteoarthritis, and the risk of fracture. Arthritis Care Res. 2006, 55, 610–615. [Google Scholar] [CrossRef]
- Munch, T.; Harrison, S.L.; Barrett-Connor, E.; Lane, N.E.; Nevitt, M.C.; Schousboe, J.T.; Stefanick, M.; Cawthon, P.M. Pain and falls and fractures in community-dwelling older men. Age Ageing 2015, 44, 973–979. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, F.; Tian, J.; Munugoda, I.P.; Graves, S.; Lorimer, M.; Cicuttini, F.; Jones, G. Do Knee Pain Phenotypes Have Different Risks of Total Knee Replacement? J. Clin. Med. 2020, 9, 632. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, F.; Tian, J.; Cicuttini, F.; Jones, G.; Aitken, D. Differentiating knee pain phenotypes in older adults: A prospective cohort study. Rheumatology 2019, 58, 274–283. [Google Scholar] [CrossRef] [PubMed]
- Doré, D.A.; Winzenberg, T.M.; Ding, C.; Otahal, P.; Pelletier, J.-P.; Martel-Pelletier, J.; Cicuttini, F.M.; Jones, G. The association between objectively measured physical activity and knee structural change using MRI. Ann. Rheum. Dis. 2013, 72, 1170–1175. [Google Scholar] [CrossRef]
- Pan, F.; Laslett, L.; Blizzard, L.; Cicuttini, F.; Winzenberg, T.; Ding, C.; Jones, G. Associations Between Fat Mass and Multisite Pain: A Five-Year Longitudinal Study. Arthritis Care Res. 2017, 69, 509–516. [Google Scholar] [CrossRef] [Green Version]
- Hoogeboom, T.J.; den Broeder, A.A.; Swierstra, B.A.; de Bie, R.A.; van den Ende, C.H. Joint-pain comorbidity, health status, and medication use in hip and knee osteoarthritis: A cross-sectional study. Arthritis Care Res. 2012, 64, 54–58. [Google Scholar] [CrossRef]
- Knoop, J.; van der Leeden, M.; Thorstensson, C.A.; Roorda, L.D.; Lems, W.F.; Knol, D.L.; Steultjens, M.P.; Dekker, J. Identification of phenotypes with different clinical outcomes in knee osteoarthritis: Data from the Osteoarthritis Initiative. Arthritis Care Res. 2011, 63, 1535–1542. [Google Scholar] [CrossRef]
- Lord, S.R.; Menz, H.B.; Tiedemann, A. A physiological profile approach to falls risk assessment and prevention. Phys. Ther. 2003, 83, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Blizzard, L.; Fell, J.; Jones, G. Ambulatory activity, body composition, and lower-limb muscle strength in older adults. Med. Sci. Sport. Exerc. 2009, 41, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Hayes, A.; Sanders, K.M.; Aitken, D.; Ebeling, P.R.; Jones, G. Operational definitions of sarcopenia and their associations with 5-year changes in falls risk in community-dwelling middle-aged and older adults. Osteoporos. Int. 2014, 25, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Lanza, S.T.; Dziak, J.J.; Huang, L.; Wagner, A.T.; Collins, L.M. LCA Stata Plugin Users’ Guide (Version 1.2); The Methodology Center: University Park, PA, USA, 2015. [Google Scholar]
- Stubbs, B.; Schofield, P.; Binnekade, T.; Patchay, S.; Sepehry, A.; Eggermont, L. Pain is associated with recurrent falls in community-dwelling older adults: Evidence from a systematic review and meta-analysis. Pain Med. 2014, 15, 1115–1128. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Binnekade, T.; Eggermont, L.; Sepehry, A.A.; Patchay, S.; Schofield, P. Pain and the risk for falls in community-dwelling older adults: Systematic review and meta-analysis. Arch. Phys. Med. Rehabil. 2014, 95, 175–187.e179. [Google Scholar] [CrossRef]
- Marshall, L.M.; Litwack-Harrison, S.; Makris, U.E.; Kado, D.M.; Cawthon, P.M.; Deyo, R.A.; Carlson, N.L.; Nevitt, M.C.; Osteoporotic Fractures in Men Study (MrOS) Research Group. A Prospective Study of Back Pain and Risk of Falls Among Older Community-dwelling Men. J. Gerontol. A Biol. Sci. Med. Sci. 2017, 72, 1264–1269. [Google Scholar] [CrossRef] [Green Version]
- Marshall, L.M.; Litwack-Harrison, S.; Cawthon, P.M.; Kado, D.M.; Deyo, R.A.; Makris, U.E.; Carlson, H.L.; Nevitt, M.C.; Study of Osteoporotic Fractures (SOF) Research Group. A Prospective Study of Back Pain and Risk of Falls among Older Community-dwelling Women. J. Gerontol. A Biol. Sci. Med. Sci. 2016, 71, 1177–1183. [Google Scholar] [CrossRef] [Green Version]
- Kitayuguchi, J.; Kamada, M.; Inoue, S.; Kamioka, H.; Abe, T.; Okada, S.; Mutoh, Y. Association of low back and knee pain with falls in Japanese community-dwelling older adults: A 3-year prospective cohort study. Geriatr. Gerontol. Int. 2017, 17, 875–884. [Google Scholar] [CrossRef]
- Cai, Y.; Leveille, S.G.; Shi, L.; Chen, P.; You, T. Chronic pain and circumstances of falls in community-living older adults: An exploratory study. Age Ageing 2022, 51, 1–6. [Google Scholar] [CrossRef]
- Awale, A.; Hagedorn, T.J.; Dufour, A.B.; Menz, H.B.; Casey, V.A.; Hannan, M.T. Foot Function, Foot Pain, and Falls in Older Adults: The Framingham Foot Study. Gerontology 2017, 63, 318–324. [Google Scholar] [CrossRef]
- Hicks, C.; Levinger, P.; Menant, J.C.; Lord, S.R.; Sachdev, P.S.; Brodaty, H.; Sturnieks, D.L. Reduced strength, poor balance and concern about falls mediate the relationship between knee pain and fall risk in older people. BMC Geriatr. 2020, 20, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hadjistavropoulos, T.; Delbaere, K. The Psychology of Fall Risk: Fear, Anxiety, Depression, and Balance Confidence. In Falls in Older People: Risk Factors, Strategies for Prevention and Implications for Practice, 3rd ed.; Sherrington, C., Lord, S.R., Naganathan, V., Eds.; Cambridge University Press: Cambridge, UK, 2021; pp. 160–171. [Google Scholar] [CrossRef]
- Kuroda, T.; Shiraki, M.; Tanaka, S.; Shiraki, Y.; Narusawa, K.; Nakamura, T. The relationship between back pain and future vertebral fracture in postmenopausal women. Spine 2009, 34, 1984–1989. [Google Scholar] [CrossRef] [PubMed]
- Barbour, K.E.; Sagawa, N.; Boudreau, R.M.; Winger, M.E.; Cauley, J.A.; Nevitt, M.C.; Fujii, T.; Patel, K.V.; Strotmeyer, E.S. Knee Osteoarthritis and the Risk of Medically Treated Injurious Falls Among Older Adults: A Community-Based US Cohort Study. Arthritis Care Res. 2019, 71, 865–874. [Google Scholar] [CrossRef]
- Yuan, S.; Chen, J.; Zeng, L.; Zhou, C.; Yu, S.; Fang, L. Association of bone mineral density and depression in different bone sites and ages: A meta-analysis. Food Sci. Nutr. 2021, 9, 4780–4792. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Hu, L.Y.; Huang, M.W.; Shen, C.C.; Huang, W.L.; Lu, T.; Hsu, C.L.; Pan, C.C. Risk of Vertebral Fracture in Patients Diagnosed with a Depressive Disorder: A Nationwide Population-Based Cohort Study. Clinics 2017, 72, 44–50. [Google Scholar] [CrossRef]
- Kelly, R.R.; McDonald, L.T.; Jensen, N.R.; Sidles, S.J.; LaRue, A.C. Impacts of Psychological Stress on Osteoporosis: Clinical Implications and Treatment Interactions. Front. Psychiatry 2019, 10, 200. [Google Scholar] [CrossRef] [PubMed]
- Talaei-Khoei, M.; Fischerauer, S.F.; Jha, R.; Ring, D.; Chen, N.; Vranceanu, A.-M. Bidirectional mediation of depression and pain intensity on their associations with upper extremity physical function. J. Behav. Med. 2018, 41, 309–317. [Google Scholar] [CrossRef]
- Ivers, R.Q.; Cumming, R.G.; Mitchell, P.; Peduto, A.J. The accuracy of self-reported fractures in older people. J. Clin. Epidemiol. 2002, 55, 452–457. [Google Scholar] [CrossRef]


{kind=link}
| Class 1 | Class 2 | Class 3 | p-Value | |||
|---|---|---|---|---|---|---|
| (n = 345) | (n = 157) | (n = 413) | ||||
| C1 vs. C2 | C1 vs. C3 | C2 vs. C3 | ||||
| Age (years) | 62.2 (7.5) | 64.0 (7.0) | 62.6 (7.3) | 0.01 | 0.44 | 0.047 |
| Female sex, n (%) | 242 (70) | 44 (28) | 179 (43) | <0.001 | <0.001 | 0.001 |
| BMI (kg/m2) | 28.4 (5.1) | 29.3 (4.5) | 26.4 (3.9) | 0.04 | <0.001 | <0.001 |
| WOMAC pain score (0–45) | 6.2 (7.3) | 3.8 (6.3) | 1.0 (2.1) | 0.001 | <0.001 | <0.001 |
| Number of painful sites (0–7) | 5.0 (1.5) | 2.7 (1.7) | 1.8 (1.6) | <0.001 | <0.001 | <0.001 |
| Hip BMD (g/cm3) | 0.95 (0.14) | 1.02 (0.16) | 0.96 (0.15) | <0.001 | 0.18 | <0.001 |
| Falls risk score (zscore) | 0.26 (0.90) | 0.05 (0.81) | 0.10 (0.76) | 0.009 | 0.007 | 0.56 |
| Incident fractures from baseline to phase 4, n (%) | ||||||
| Hip fracture | 1 (0.3) | 1 (0.6) | 1 (0.2) | 0.53 | 0.91 | 0.44 |
| Vertebral fracture | 10 (3) | 5 (3) | 4 (1) | 0.84 | 0.10 | 0.06 |
| Nonvertebral fracture | 58 (17) | 19 (12) | 44 (11) | 0.15 | 0.01 | 0.65 |
| Any site fracture | 66 (19) | 24 (15) | 48 (12) | 0.26 | 0.04 | 0.27 |
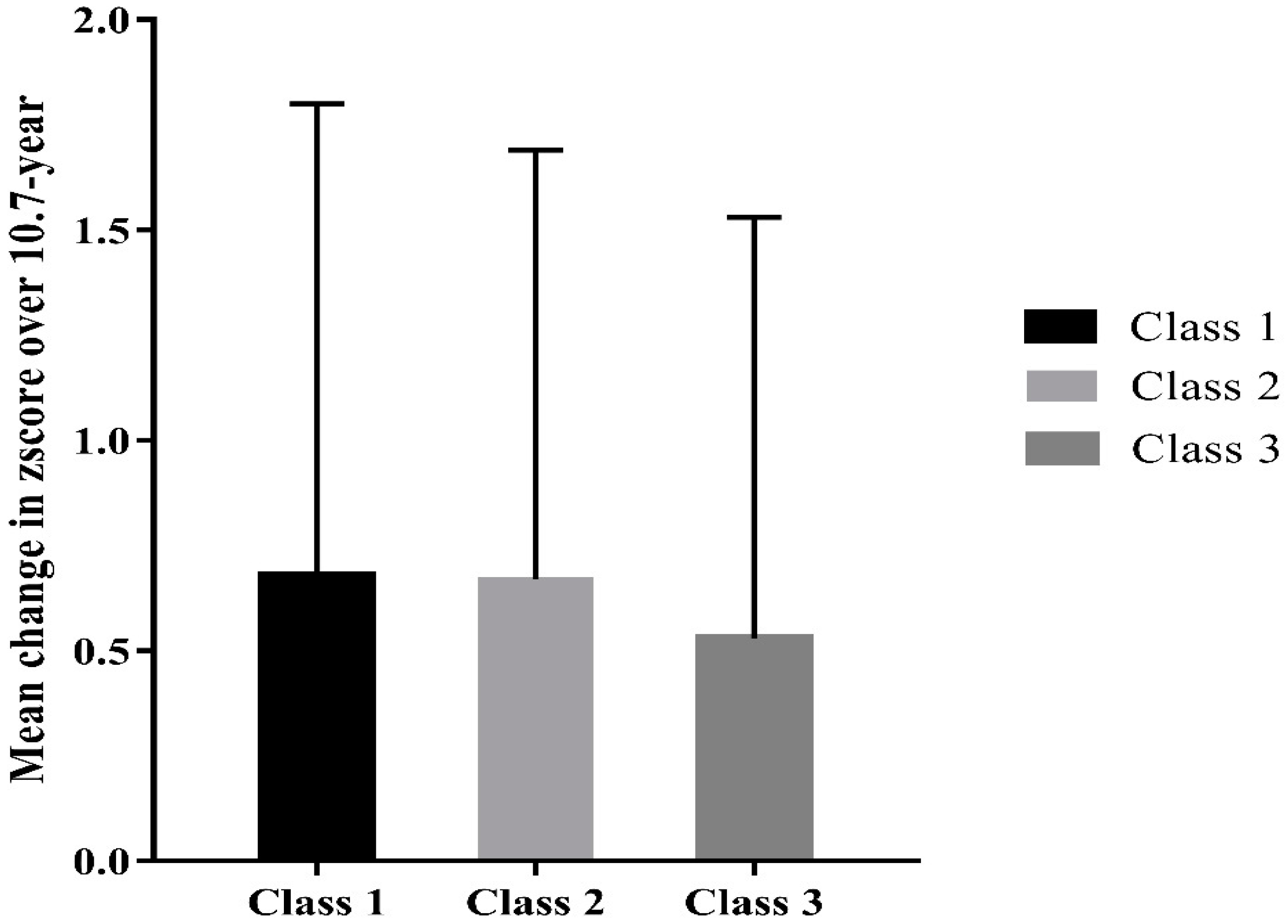
| Zscore over 10.7-Year Follow-Up β * (95% CI) | Change in Zscore from Baseline to 10.7-Year Follow-Up β † (95% CI) | |
|---|---|---|
| Class 1 vs. Class 3 | 0.16 (0.09, 0.23) | 0.03 (0.01, 0.04) |
| Class 2 vs. Class 3 | −0.09 (−0.18, −0.002) | 0.02 (−0.003, 0.04) |
| Class 1 vs. Class 2 | 0.25 (0.15, 0.34) | 0.006 (−0.02, 0.03) |
| Incident Fractures over 10.7-Year Follow-Up | |||
|---|---|---|---|
| Vertebral RR * (95% CI) | Non-Vertebral RR * (95% CI) | Any Site RR * (95% CI) | |
| Class 1 vs. Class 3 | 2.44 (1.22, 4.91) | 1.20 (1.01, 1.42) | 1.24 (1.04, 1.46) |
| Class 2 vs.Class 3 | 1.47 (0.64, 3.36) | 1.41 (1.17, 1.71) | 1.44 (1.20, 1.73) |
| Class 1 vs. Class 2 | 1.66 (0.73, 3.82) | 0.85 (0.70, 1.04) | 0.86 (0.71, 1.04) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devine, M.; Ma, C.; Tian, J.; Antony, B.; Cicuttini, F.; Jones, G.; Pan, F. Association of Pain Phenotypes with Risk of Falls and Incident Fractures. Biomedicines 2022, 10, 2924. https://doi.org/10.3390/biomedicines10112924
Devine M, Ma C, Tian J, Antony B, Cicuttini F, Jones G, Pan F. Association of Pain Phenotypes with Risk of Falls and Incident Fractures. Biomedicines. 2022; 10(11):2924. https://doi.org/10.3390/biomedicines10112924
Chicago/Turabian StyleDevine, Maxim, Canchen Ma, Jing Tian, Benny Antony, Flavia Cicuttini, Graeme Jones, and Feng Pan. 2022. "Association of Pain Phenotypes with Risk of Falls and Incident Fractures" Biomedicines 10, no. 11: 2924. https://doi.org/10.3390/biomedicines10112924