
COVID-19 in Patients with Hematologic Diseases


Abstract
:1. Introduction
2. Impact of COVID-19 in Patients with Hematological Malignancies
2.1. Risk of COVID-19 in Patients with HM
2.2. Psychological Distress of Patients with HM during the Pandemic
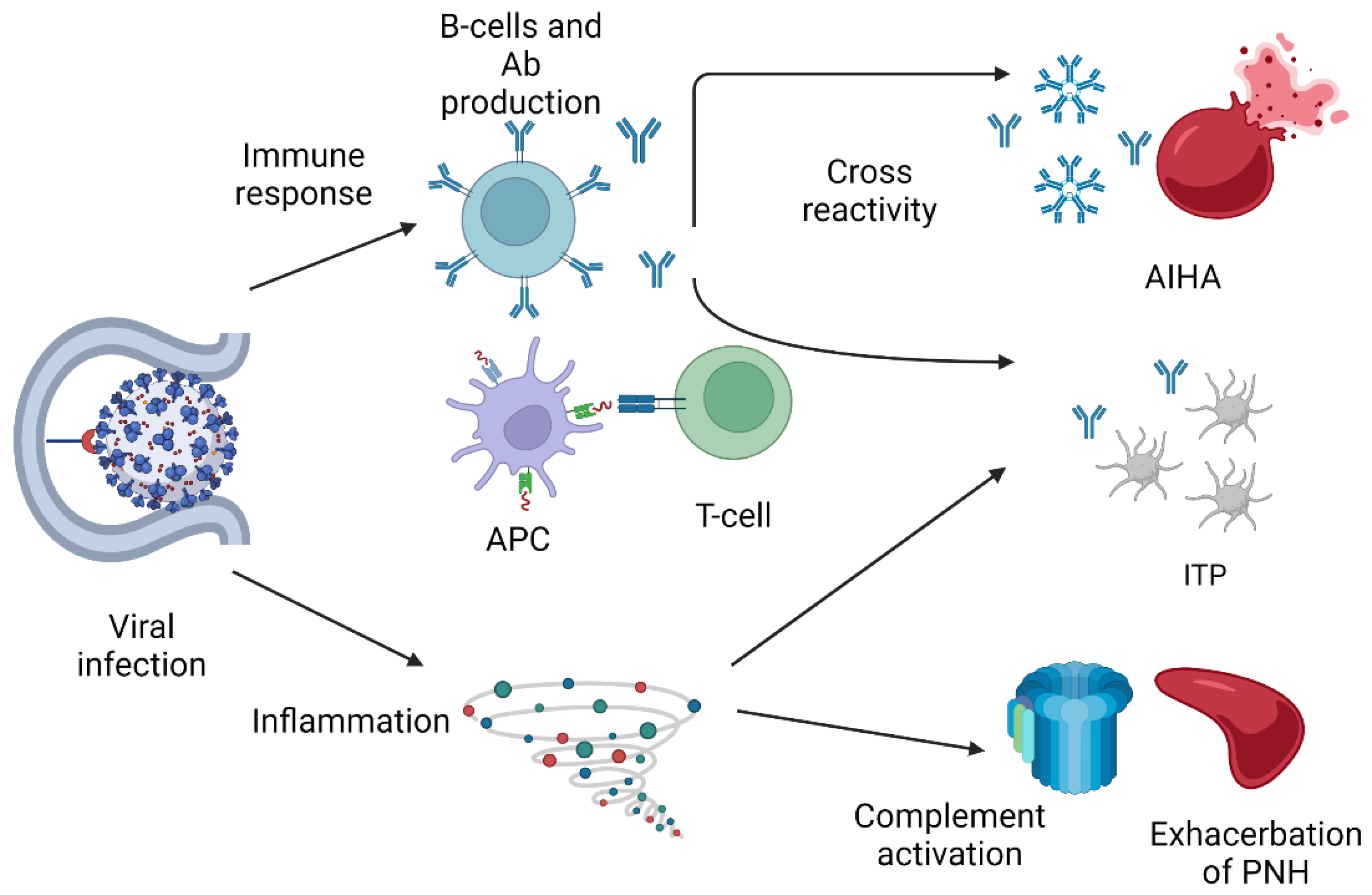
3. Immune-Mediated Cytopenias Triggered by COVID-19 Infection
4. Vaccination against COVID-19 and Response of HM Patients to Vaccines
5. Antiviral Therapies and Prevention of COVID-19 in Immunocompromised Patients
6. Autoimmune Blood Disorders Triggered by COVID Vaccine
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Zhang, L. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Cao, B. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Volz, E.; Mishra, S.; Chand, M.; Barrett, J.C.; Johnson, R.; Geidelberg, L.; Hinsley, W.R.; Laydon, D.J.; Dabrera, G.; O’Toole, Á.; et al. Assessing transmissibility of SARS-CoV-2 lineage B.1.1.7 in England. Nature 2021, 593, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Dejnirattisai, W.; Supasa, P.; Liu, C.; Mentzer, A.J.; Ginn, H.M.; Zhao, Y.; Duyvesteyn, H.M.E.; Tuekprakhon, A.; Nutalai, R.; et al. Evidence of escape of SARS-CoV-2 variant B.1.351 from natural and vaccine-induced sera. Cell 2021, 184, 2348–2361.e6. [Google Scholar] [CrossRef] [PubMed]
- Dai, M.; Liu, D.; Liu, M.; Zhou, F.; Li, G.; Chen, Z.; Zhang, Z.; You, H.; Wu, M.; Zheng, Q.; et al. Patients with Cancer Appear More Vulnerable to SARS-CoV-2: A Multicenter Study during the COVID-19 Outbreak. Cancer Discov. 2020, 10, 783–791. [Google Scholar] [CrossRef] [PubMed]
- Fattizzo, B.; Pasquale, R.; Bellani, V.; Barcellini, W.; Kulasekararaj, A.G. Complement Mediated Hemolytic Anemias in the COVID-19 Era: Case Series and Review of the Literature. Front. Immunol. 2021, 12, 791429. [Google Scholar] [CrossRef]
- David, P.; Dotan, A.; Mahroum, N.; Shoenfeld, Y. Immune Thrombocytopenic Purpura (ITP) Triggered by COVID-19 Infection and Vaccination. Isr. Med. Assoc. J. 2021, 23, 378–380. [Google Scholar]
- He, W.; Chen, L.; Yuan, G.; Fang, Y.; Chen, W.; Wu, D.; Liang, B.; Lu, X.; Ma, Y.; Li, L.; et al. COVID-19 in persons with haematological cancers. Leukemia 2020, 34, 1637–1645. [Google Scholar] [CrossRef]
- Aries, J.A.; Davies, J.K.; Auer, R.L.; Hallam, S.L.; Montoto, S.; Smith, M.; Sevillano, B.; Foggo, V.; Wrench, B.; Zegocki, K.; et al. Clinical outcome of coronavirus disease 2019 in haemato-oncology patients. Br. J. Haematol. 2020, 190, e64–e67. [Google Scholar] [CrossRef]
- Lim, S.H.; Stuart, B.; Joseph-Pietras, D.; Johnson, M.; Campbell, N.; Kelly, A.; Jeffrey, D.; Turaj, A.H.; Rolfvondenbaumen, K.; Galloway, C.; et al. Immune responses against SARS-CoV-2 variants after two and three doses of vaccine in B-cell malignancies: UK PROSECO study. Nat. Cancer 2022, 3, 552–564. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; de Lima Lopes, G.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef] [PubMed]
- Grivas, P.; Khaki, A.R.; Wise-Draper, T.M.; French, B.; Hennessy, C.; Hsu, C.Y.; Shyr, Y.; Li, X.; Choueiri, T.K.; Painter, C.A.; et al. Association of clinical factors and recent anticancer therapy with COVID-19 severity among patients with cancer: A report from the COVID-19 and Cancer Consortium. Ann. Oncol. 2021, 32, 787–800. [Google Scholar] [CrossRef] [PubMed]
- Fattizzo, B.; Giannotta, J.A.; Sciumè, M.; Cattaneo, D.; Bucelli, C.; Fracchiolla, N.S.; Onida, F.; Baldini, L.; Barcellini, W.; Iurlo, A. Reply to “COVID-19 in persons with haematological cancers”: A focus on myeloid neoplasms and risk factors for mortality. Leukemia 2020, 34, 1957–1960. [Google Scholar] [CrossRef] [PubMed]
- Shah, V.; Ko Ko, T.; Zuckerman, M.; Vidler, J.; Sharif, S.; Mehra, V.; Gandhi, S.; Kuhnl, A.; Yallop, D.; Avenoso, D.; et al. Poor outcome and prolonged persistence of SARS-CoV-2 RNA in COVID-19 patients with haematological malignancies; King’s College Hospital experience. Br. J. Haematol. 2020, 190, e279–e282. [Google Scholar] [CrossRef]
- Passamonti, F.; Cattaneo, C.; Arcaini, L.; Bruna, R.; Cavo, M.; Merli, F.; Angelucci, E.; Krampera, M.; Cairoli, R.; Della Porta, M.G.; et al. Clinical characteristics and risk factors associated with COVID-19 severity in patients with haematological malignancies in Italy: A retrospective, multicentre, cohort study. Lancet Haematol. 2020, 7, e737–e745. [Google Scholar] [CrossRef]
- Borsani, O.; Bastard, P.; Rosain, J.; Gervais, A.; Sant’Antonio, E.; Vanni, D.; Casetti, I.C.; Pietra, D.; Trotti, C.; Catricalà, S.; et al. Autoantibodies against type I IFNs in patients with Ph-negative myeloproliferative neoplasms. Blood 2022, 139, 2716–2720. [Google Scholar] [CrossRef]
- Bastard, P.; Rosen, L.B.; Zhang, Q.; Michailidis, E.; Hoffmann, H.H.; Zhang, Y.; Dorgham, K.; Philippot, Q.; Rosain, J.; Béziat, V.; et al. Autoantibodies against type I IFNs in patients with life-threatening COVID-19. Science 2020, 370, eabd4585. [Google Scholar] [CrossRef]
- Bastard, P.; Gervais, A.; Le Voyer, T.; Rosain, J.; Philippot, Q.; Manry, J.; Michailidis, E.; Hoffmann, H.H.; Eto, S.; Garcia-Prat, M.; et al. Autoantibodies neutralizing type I IFNs are present in. Sci. Immunol. 2021, 6, eabl4340. [Google Scholar] [CrossRef]
- Passamonti, F.; Romano, A.; Salvini, M.; Merli, F.; Porta, M.G.D.; Bruna, R.; Coviello, E.; Romano, I.; Cairoli, R.; Lemoli, R.; et al. COVID-19 elicits an impaired antibody response against SARS-CoV-2 in patients with haematological malignancies. Br. J. Haematol. 2021, 195, 371–377. [Google Scholar] [CrossRef]
- London, J.W.; Fazio-Eynullayeva, E.; Palchuk, M.B.; Sankey, P.; McNair, C. Effects of the COVID-19 Pandemic on Cancer-Related Patient Encounters. JCO Clin. Cancer Inform. 2020, 4, 657–665. [Google Scholar] [CrossRef]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Moraliyage, H.; De Silva, D.; Ranasinghe, W.; Adikari, A.; Alahakoon, D.; Prasad, R.; Lawrentschuk, N.; Bolton, D. Cancer in Lockdown: Impact of the COVID-19 Pandemic on Patients with Cancer. Oncologist 2021, 26, e342–e344. [Google Scholar] [CrossRef] [PubMed]
- Caston, N.E.; Lawhon, V.M.; Smith, K.L.; Gallagher, K.; Angove, R.; Anderson, E.; Balch, A.; Azuero, A.; Huang, C.S.; Rocque, G.B. Examining the association among fear of COVID-19, psychological distress, and delays in cancer care. Cancer Med. 2021, 10, 8854–8865. [Google Scholar] [CrossRef]
- Zomerdijk, N.; Jongenelis, M.; Short, C.E.; Smith, A.; Turner, J.; Huntley, K. Prevalence and correlates of psychological distress, unmet supportive care needs, and fear of cancer recurrence among haematological cancer patients during the COVID-19 pandemic. Support. Care Cancer 2021, 29, 7755–7764. [Google Scholar] [CrossRef]
- Dotan, A.; Muller, S.; Kanduc, D.; David, P.; Halpert, G.; Shoenfeld, Y. The SARS-CoV-2 as an instrumental trigger of autoimmunity. Autoimmun. Rev. 2021, 20, 102792. [Google Scholar] [CrossRef]
- Vojdani, A.; Kharrazian, D. Potential antigenic cross-reactivity between SARS-CoV-2 and human tissue with a possible link to an increase in autoimmune diseases. Clin. Immunol. 2020, 217, 108480. [Google Scholar] [CrossRef]
- Ma, L.; Sahu, S.K.; Cano, M.; Kuppuswamy, V.; Bajwa, J.; McPhatter, J.N.; Pine, A.; Meizlish, M.L.; Goshua, G.; Chang, C.H. Increased complement activation is a distinctive feature of severe SARS-CoV-2 infection. Sci. Immunol. 2021, 6, abh2259. [Google Scholar] [CrossRef]
- Zulfiqar, A.A.; Lorenzo-Villalba, N.; Hassler, P.; Andrès, E. Immune Thrombocytopenic Purpura in a Patient with COVID-19. N. Engl. J. Med. 2020, 382, e43. [Google Scholar] [CrossRef]
- Pedroso, A.; Frade, L.; Trevas, S.; Correia, M.J.; Esteves, A.L. Immune Thrombocytopenic Purpura—Different Presentations in Two COVID-19 Patients. Cureus 2020, 12, e11202. [Google Scholar] [CrossRef] [PubMed]
- Revuz, S.; Vernier, N.; Saadi, L.; Campagne, J.; Poussing, S.; Maurier, F. Immune Thrombocytopenic Purpura in Patients with COVID-19. Eur. J. Case Rep. Intern. Med. 2020, 7, 001751. [Google Scholar] [CrossRef] [PubMed]
- Murt, A.; Eskazan, A.E.; Yılmaz, U.; Ozkan, T.; Ar, M.C. COVID-19 presenting with immune thrombocytopenia: A case report and review of the literature. J. Med. Virol. 2021, 93, 43–45. [Google Scholar] [CrossRef]
- Bomhof, G.; Mutsaers, P.G.N.J.; Leebeek, F.W.G.; Te Boekhorst, P.A.W.; Hofland, J.; Croles, F.N.; Jansen, A.J.G. COVID-19-associated immune thrombocytopenia. Br. J. Haematol. 2020, 190, e61–e64. [Google Scholar] [CrossRef] [PubMed]
- Schüller, H.; Klein, F.; Lübbert, M.; Prager, E.P. Hemolytic crisis in a patient treated with eculizumab for paroxysmal nocturnal hemoglobinuria possibly triggered by SARS-CoV-2 (COVID-19): A case report. Ann. Hematol. 2021, 100, 841–842. [Google Scholar] [CrossRef] [PubMed]
- Genthon, A.; Chiarabini, T.; Baylac, P.; Valin, N.; Urbina, T.; Pacanowski, J.; Mekinian, A.; Brissot, E.; Hammedi-Bouzina, F.M.; Lapusan, S.; et al. Severe COVID-19 infection in a patient with paroxysmal nocturnal hemoglobinuria on eculizumab therapy. Leuk. Lymphoma 2021, 62, 1502–1505. [Google Scholar] [CrossRef]
- Sokol, J.; Nehaj, F.; Mokan, M.; Lisa, L.; Stasko, J. COVID-19 infection in a patient with paroxysmal nocturnal hemoglobinuria: A case report. Medicine 2021, 100, e25456. [Google Scholar] [CrossRef] [PubMed]
- Kulasekararaj, A.G.; Lazana, I.; Large, J.; Posadas, K.; Eagleton, H.; Lord Villajin, J.; Zuckerman, M.; Gandhi, S.; Marsh, J.C.W. Terminal complement inhibition dampens the inflammation during COVID-19. Br. J. Haematol. 2020, 190, e141–e143. [Google Scholar] [CrossRef]
- Araten, D.J.; Belmont, H.M.; Schaefer-Cutillo, J.; Iyengar, A.; Mattoo, A.; Reddy, R. Mild Clinical Course of COVID-19 in 3 Patients Receiving Therapeutic Monoclonal Antibodies Targeting C5 Complement for Hematologic Disorders. Am. J. Case Rep. 2020, 21, e927418. [Google Scholar] [CrossRef] [PubMed]
- Barcellini, W.; Fattizzo, B.; Giannotta, J.A.; Quattrocchi, L.; Aydin, S.; Barone, F.; Carbone, C.; Pomponi, F.; Metafuni, E.; Beggiato, E.; et al. COVID-19 in patients with paroxysmal nocturnal haemoglobinuria: An Italian multicentre survey. Br. J. Haematol. 2021, 194, 854–856. [Google Scholar] [CrossRef] [PubMed]
- Lazarian, G.; Quinquenel, A.; Bellal, M.; Siavellis, J.; Jacquy, C.; Re, D.; Merabet, F.; Mekinian, A.; Braun, T.; Damaj, G.; et al. Autoimmune haemolytic anaemia associated with COVID-19 infection. Br. J. Haematol. 2020, 190, 29–31. [Google Scholar] [CrossRef]
- Zagorski, E.; Pawar, T.; Rahimian, S.; Forman, D. Cold agglutinin autoimmune haemolytic anaemia associated with novel coronavirus (COVID-19). Br. J. Haematol. 2020, 190, e183–e184. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, J.; Eichbaum, Q. COVID-19 associated with severe autoimmune hemolytic anemia. Transfusion 2021, 61, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Capes, A.; Bailly, S.; Hantson, P.; Gerard, L.; Laterre, P.F. COVID-19 infection associated with autoimmune hemolytic anemia. Ann. Hematol. 2020, 99, 1679–1680. [Google Scholar] [CrossRef] [PubMed]
- Huscenot, T.; Galland, J.; Ouvrat, M.; Rossignol, M.; Mouly, S.; Sène, D.; Group, A.L.C. SARS-CoV-2-associated cold agglutinin disease: A report of two cases. Ann. Hematol. 2020, 99, 1943–1944. [Google Scholar] [CrossRef]
- Barcellini, W.; Giannotta, J.A.; Fattizzo, B. Are Patients With Autoimmune Cytopenias at Higher Risk of COVID-19 Pneumonia? The Experience of a Reference Center in Northern Italy and Review of the Literature. Front. Immunol. 2020, 11, 609198. [Google Scholar] [CrossRef]
- Angileri, F.; Légaré, S.; Marino Gammazza, A.; Conway de Macario, E.; Macario, A.J.L.; Cappello, F. Is molecular mimicry the culprit in the autoimmune haemolytic anaemia affecting patients with COVID-19? Br. J. Haematol. 2020, 190, e92–e93. [Google Scholar] [CrossRef] [PubMed]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef] [PubMed]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Shao, W.; Chen, X.; Zhang, B.; Wang, G.; Zhang, W. Real-world effectiveness of COVID-19 vaccines: A literature review and meta-analysis. Int. J. Infect. Dis. 2022, 114, 252–260. [Google Scholar] [CrossRef]
- Yri, O.E.; Torfoss, D.; Hungnes, O.; Tierens, A.; Waalen, K.; Nordøy, T.; Dudman, S.; Kilander, A.; Wader, K.F.; Ostenstad, B.; et al. Rituximab blocks protective serologic response to influenza A (H1N1) 2009 vaccination in lymphoma patients during or within 6 months after treatment. Blood 2011, 118, 6769–6771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spagnolo, F.; Boutros, A.; Croce, E.; Cecchi, F.; Arecco, L.; Tanda, E.; Pronzato, P.; Lambertini, M. Influenza vaccination in cancer patients receiving immune checkpoint inhibitors: A systematic review. Eur. J. Clin. Investig. 2021, 51, e13604. [Google Scholar] [CrossRef]
- Thakkar, A.; Gonzalez-Lugo, J.D.; Goradia, N.; Gali, R.; Shapiro, L.C.; Pradhan, K.; Rahman, S.; Kim, S.Y.; Ko, B.; Sica, R.A.; et al. Seroconversion rates following COVID-19 vaccination among patients with cancer. Cancer Cell 2021, 39, 1081–1090.e2. [Google Scholar] [CrossRef]
- Fendler, A.; Shepherd, S.T.C.; Au, L.; Wilkinson, K.A.; Wu, M.; Byrne, F.; Cerrone, M.; Schmitt, A.M.; Joharatnam-Hogan, N.; Shum, B.; et al. Adaptive immunity and neutralizing antibodies against SARS-CoV-2 variants of concern following vaccination in patients with cancer: The CAPTURE study. Nat. Cancer 2021, 2, 1305–1320. [Google Scholar] [CrossRef]
- Mencoboni, M.; Fontana, V.; Damiani, A.; Spitaleri, A.; Raso, A.; Bottaro, L.C.; Rossi, G.; Canobbio, L.; La Camera, A.; Filiberti, R.A.; et al. Antibody Response to COVID-19 mRNA Vaccines in Oncologic and Hematologic Patients Undergoing Chemotherapy. Curr. Oncol. 2022, 29, 3364–3374. [Google Scholar] [CrossRef]
- Addeo, A.; Shah, P.K.; Bordry, N.; Hudson, R.D.; Albracht, B.; Di Marco, M.; Kaklamani, V.; Dietrich, P.Y.; Taylor, B.S.; Simand, P.F.; et al. Immunogenicity of SARS-CoV-2 messenger RNA vaccines in patients with cancer. Cancer Cell 2021, 39, 1091–1098.e2. [Google Scholar] [CrossRef]
- Guven, D.C.; Sahin, T.K.; Akın, S.; Uckun, F.M. Impact of Therapy in Patients with Hematologic Malignancies on Seroconversion Rates After SARS-CoV-2 Vaccination. Oncologist 2022, 27, e357–e361. [Google Scholar] [CrossRef]
- Pagano, L.; Salmanton-García, J.; Marchesi, F.; López-García, A.; Lamure, S.; Itri, F.; Gomes-Silva, M.; Dragonetti, G.; Falces-Romero, I.; van Doesum, J.; et al. COVID-19 in vaccinated adult patients with hematological malignancies: Preliminary results from EPICOVIDEHA. Blood 2022, 139, 1588–1592. [Google Scholar] [CrossRef]
- Pagano, L.; Salmanton-García, J.; Marchesi, F.; Blennow, O.; Gomes da Silva, M.; Glenthøj, A.; van Doesum, J.A.; Bilgin, Y.M.; Lopez-Garcia, A.; Itri, F.; et al. Breakthrough COVID-19 in vaccinated patients with hematologic malignancies: Results from EPICOVIDEHA survey. Blood 2022. [Google Scholar] [CrossRef]
- Chalkias, S.; Harper, C.; Vrbicky, K.; Walsh, S.R.; Essink, B.; Brosz, A.; McGhee, N.; Tomassini, J.E.; Chen, X.; Chang, Y.; et al. A Bivalent Omicron-Containing Booster Vaccine against COVID-19. N. Engl. J. Med. 2022, 387, 1279–1291. [Google Scholar] [CrossRef] [PubMed]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Arbel, R.; Wolff Sagy, Y.; Hoshen, M.; Battat, E.; Lavie, G.; Sergienko, R.; Friger, M.; Waxman, J.G.; Dagan, N.; Balicer, R.; et al. Nirmatrelvir Use and Severe COVID-19 Outcomes during the Omicron Surge. N. Engl. J. Med. 2022, 387, 790–798. [Google Scholar] [CrossRef]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early Remdesivir to Prevent Progression to Severe COVID-19 in Outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Jayk Bernal, A.; Gomes da Silva, M.M.; Musungaie, D.B.; Kovalchuk, E.; Gonzalez, A.; Delos Reyes, V.; Martín-Quirós, A.; Caraco, Y.; Williams-Diaz, A.; Brown, M.L.; et al. Molnupiravir for Oral Treatment of COVID-19 in Nonhospitalized Patients. N. Engl. J. Med. 2022, 386, 509–520. [Google Scholar] [CrossRef] [PubMed]
- Dougan, M.; Nirula, A.; Azizad, M.; Mocherla, B.; Gottlieb, R.L.; Chen, P.; Hebert, C.; Perry, R.; Boscia, J.; Heller, B.; et al. Bamlanivimab plus Etesevimab in Mild or Moderate COVID-19. N. Engl. J. Med. 2021, 385, 1382–1392. [Google Scholar] [CrossRef] [PubMed]
- Weinreich, D.M.; Sivapalasingam, S.; Norton, T.; Ali, S.; Gao, H.; Bhore, R.; Xiao, J.; Hooper, A.T.; Hamilton, J.D.; Musser, B.J.; et al. REGEN-COV Antibody Combination and Outcomes in Outpatients with COVID-19. N. Engl. J. Med. 2021, 385, e81. [Google Scholar] [CrossRef] [PubMed]
- Takashita, E.; Yamayoshi, S.; Fukushi, S.; Suzuki, T.; Maeda, K.; Sakai-Tagawa, Y.; Ito, M.; Uraki, R.; Halfmann, P.; Watanabe, S.; et al. Efficacy of Antiviral Agents against the Omicron Subvariant BA.2.75. N. Engl. J. Med. 2022, 387, 1236–1238. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Gonzalez-Rojas, Y.; Juarez, E.; Crespo Casal, M.; Moya, J.; Falci, D.R.; Sarkis, E.; Solis, J.; Zheng, H.; Scott, N.; et al. Early Treatment for COVID-19 with SARS-CoV-2 Neutralizing Antibody Sotrovimab. N. Engl. J. Med. 2021, 385, 1941–1950. [Google Scholar] [CrossRef]
- Iketani, S.; Liu, L.; Guo, Y.; Chan, J.F.; Huang, Y.; Wang, M.; Luo, Y.; Yu, J.; Chu, H.; Chik, K.K.; et al. Antibody evasion properties of SARS-CoV-2 Omicron sublineages. Nature 2022, 604, 553–556. [Google Scholar] [CrossRef]
- Levin, M.J.; Ustianowski, A.; De Wit, S.; Launay, O.; Avila, M.; Templeton, A.; Yuan, Y.; Seegobin, S.; Ellery, A.; Levinson, D.J.; et al. Intramuscular AZD7442 (Tixagevimab-Cilgavimab) for Prevention of COVID-19. N. Engl. J. Med. 2022, 386, 2188–2200. [Google Scholar] [CrossRef]
- Greinacher, A. CLINICAL PRACTICE. Heparin-Induced Thrombocytopenia. N. Engl. J. Med. 2015, 373, 252–261. [Google Scholar] [CrossRef] [PubMed]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef] [PubMed]
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef] [PubMed]
- Scully, M.; Singh, D.; Lown, R.; Poles, A.; Solomon, T.; Levi, M.; Goldblatt, D.; Kotoucek, P.; Thomas, W.; Lester, W. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2202–2211. [Google Scholar] [CrossRef]
- Greinacher, A.; Selleng, K.; Warkentin, T.E. Autoimmune heparin-induced thrombocytopenia. J. Thromb. Haemost. 2017, 15, 2099–2114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muir, K.L.; Kallam, A.; Koepsell, S.A.; Gundabolu, K. Thrombotic Thrombocytopenia after Ad26.COV2.S Vaccination. N. Engl. J. Med. 2021, 384, 1964–1965. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. COVID-19: European countries suspend use of Oxford-Astra Zeneca vaccine after reports of blood clots. BMJ 2021, 372, n699. [Google Scholar] [CrossRef]
- Barda, N.; Dagan, N.; Ben-Shlomo, Y.; Kepten, E.; Waxman, J.; Ohana, R.; Hernán, M.A.; Lipsitch, M.; Kohane, I.; Netzer, D.; et al. Safety of the BNT162b2 mRNA COVID-19 Vaccine in a Nationwide Setting. N. Engl. J. Med. 2021, 385, 1078–1090. [Google Scholar] [CrossRef]
- Nazy, I.; Sachs, U.J.; Arnold, D.M.; McKenzie, S.E.; Choi, P.; Althaus, K.; Ahlen, M.T.; Sharma, R.; Grace, R.F.; Bakchoul, T. Recommendations for the clinical and laboratory diagnosis of VITT against COVID-19: Communication from the ISTH SSC Subcommittee on Platelet Immunology. J. Thromb. Haemost. 2021, 19, 1585–1588. [Google Scholar] [CrossRef]
- Lee, E.J.; Cines, D.B.; Gernsheimer, T.; Kessler, C.; Michel, M.; Tarantino, M.D.; Semple, J.W.; Arnold, D.M.; Godeau, B.; Lambert, M.P.; et al. Thrombocytopenia following Pfizer and Moderna SARS-CoV-2 vaccination. Am. J. Hematol. 2021, 96, 534–537. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Beltrami-Moreira, M.; Al-Samkari, H.; Cuker, A.; DiRaimo, J.; Gernsheimer, T.; Kruse, A.; Kessler, C.; Kruse, C.; Leavitt, A.D.; et al. SARS-CoV-2 vaccination and ITP in patients with de novo or preexisting ITP. Blood 2022, 139, 1564–1574. [Google Scholar] [CrossRef]
- Welsh, K.J.; Baumblatt, J.; Chege, W.; Goud, R.; Nair, N. Thrombocytopenia including immune thrombocytopenia after receipt of mRNA COVID-19 vaccines reported to the Vaccine Adverse Event Reporting System (VAERS). Vaccine 2021, 39, 3329–3332. [Google Scholar] [CrossRef] [PubMed]
- Kuter, D.J. Exacerbation of immune thrombocytopenia following COVID-19 vaccination. Br. J. Haematol. 2021, 195, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Visser, C.; Swinkels, M.; van Werkhoven, E.D.; Croles, F.N.; Noordzij-Nooteboom, H.S.; Eefting, M.; Last-Koopmans, S.M.; Idink, C.; Westerweel, P.E.; Santbergen, B.; et al. COVID-19 vaccination in patients with immune thrombocytopenia. Blood Adv. 2022, 6, 1637–1644. [Google Scholar] [CrossRef]
- Jacobs, J.W.; Booth, G.S. COVID-19 and Immune-Mediated RBC Destruction. Am. J. Clin. Pathol. 2022, 157, 844–851. [Google Scholar] [CrossRef] [PubMed]
- Jaydev, F.; Kumar, V.; Khatri, J.; Shahani, S.; Beganovic, S. A Case of Autoimmune Hemolytic Anemia after the First Dose of COVID-19 mRNA-1273 Vaccine with Undetected Pernicious Anemia. Case Rep. Hematol. 2022, 2022, 2036460. [Google Scholar] [CrossRef]
- Fattizzo, B.; Giannotta, J.A.; Cecchi, N.; Barcellini, W. SARS-CoV-2 vaccination in patients with autoimmune cytopenias: The experience of a reference center. Am. J. Hematol. 2021, 96, E413–E416. [Google Scholar] [CrossRef]
- Aoun, S.A.; Motabi, I. Cold agglutinin disease after COVID-19 vaccine. Br. J. Haematol. 2021, 195, 650. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference | Patient Population | Risk Factors | Clinical Severity | Mortality |
|---|---|---|---|---|
| [8] | 128 pts with HM (13 with COVID-19) Median age 35 y | Co-bacterial infections | 10 pts required oxygen | 62% |
| [9] | 35 pts with HM and COVID-19 Median age 69 y | Age, number of comorbidities | 40% | |
| [11] | 928 pts with cancer and COVID-19 Median age 66 y | Age, male sex, smoking, number of comorbidities, ECOG > 2, active cancer | 14% admitted to ICU 12% required ventilation | 13% |
| [12] | 4966 pts with cancer and COVID-19 (10% with HM) Median age 66 y | Age, male sex, obesity, CV and lung comorbidities, renal disease, diabetes mellitus, non-Hispanic black race, Hispanic ethnicity, worse ECOG, recent cytotoxic chemotherapy, HM | Hospitalization 58.7% | 14% |
| [13] | 1250 pts with HM (16 pts with COVID-19) | Age, number of comorbidities | Hospitalization 80% 12% admitted to ICU | 30% |
| [14] | 80 pts with HM and COVID-19 Mean age 69 y | Age, intensive therapy | 39% | |
| [15] | 536 pts with HM and COVID-19 Median age 68 y | Age, AML diagnosis, indolent and aggressive NHL, PC neoplasms, severe COVID-19 | 15% admitted to ICU | 36.9% |
| [16] | 219 pts with MPN (29 pts with COVID-19) Median age 62 y | Presence of AAbs against type I IFN | Hospitalization 27.6% |
| Immune Mediated Cytopenia | Reference | Median Hb/PLT Value at Nadir | N. of Patients | Management of the Cytopenia | Outcome |
|---|---|---|---|---|---|
| AIHA (warm and cold antibodies) | [36] | 7 g/dL | 7 (3 CAD) | Steroid, Rituximab, Transfusion | 3 remission, 4 ongoing at the time of publication |
| [37] | 5.3 g/dL | 1 (CAD) | Transfusion | Death | |
| [38] | 1.6 g/dL | 1 (mixed Abs) | Transfusion, steroid, Rituximab | Remission | |
| [39] | 6.9 g/dL | 1 (CAD) | Transfusion | Remission | |
| [40] | 7.1 g/dL | 2 (CAD) | Transfusion | Remission | |
| [41] | 7.3 g/dL | 3 (1 CAD) | Steroid, transfusion | Remission | |
| ITP | [25] | 2000/mmc | 1 | IVIg, steroid, transfusion, Rituximab | Remission |
| [26] | 20,000/mmc | 2 | Steroid | Remission | |
| [27] | 17,000/mmc | 3 | IVIg | Remission | |
| [28] | 9000/mmc | 1 | IVIg | Remission | |
| [29] | 3000/mmc | 3 | Transfusion, IVIg, steroid | 2 remissions, 1 death | |
| PNH | [30] | 6.5 g/dL | 1 | Eculizumab | Remission |
| [31] | 8.9 g/dL | 1 | Eculizumab | Remission | |
| [32] | 9.8 g/dL | 1 | Steroid | Remission | |
| [33] | NA | 4 | Eculizumab, Ravulizumab, transfusion | 3 remissions, 1 ongoing at the time of publication | |
| [34] | NA | 3 | Eculizumab | Remission | |
| [35] | NA | 4 | Eculizumab, Ravulizumab | Remission |
| Pre-Exposure/Prophylactic Treatment | Schedule | Activity against Omicron Variant |
|---|---|---|
| Vaccines (most used in Western countries) | ||
| mRNA-based | ||
| BNT162b(Pfizer/Biontech) mRNA-1273 (Moderna) | 2 doses 21 days 2 doses 28 days | Bivalent booster Bivalent booster |
| AdV-vectored | ||
| ChAdOx1 nCov-19 (AstraZeneca/Oxford) Ad26.CoV2.S (Johnson& Johnson) | 2 doses 4–12 weeks 1 dose | NA NA |
| Monoclonal antibodies | ||
| Tixagevimab/Cilgavimab | 150/150 mg iv day 1 | BA.1 (reduced) and BA.2 |
| Post-exposure/confirmed COVID-19 Treatment | ||
| Antiviral therapy | ||
| Remdesivir Nirmatrelvir + Ritonavir Molnupiravir | 200 mg iv, day 1, 100 mg iv day 2–3 2 × 300/100 mg po for 5 days 2 × 800 mg po for 5 days | Yes Yes Yes |
| Monoclonal antibodies | ||
| Etesevimab/Bamlanivimab Imdevimab/Casirivimab Sotrovimab Bebtelovimab (US only) Tixagevimab/Cilgavimab | 1400/700 mg iv day 1 1200/1200 mg iv day 1 500 mg iv day 1 175 mg iv day 1 300/300 mg iv day 1 | Markedly reduced Markedly reduced BA.1 only BA.1 and BA.2 BA.1 (reduced) and BA.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casetti, I.C.; Borsani, O.; Rumi, E. COVID-19 in Patients with Hematologic Diseases. Biomedicines 2022, 10, 3069. https://doi.org/10.3390/biomedicines10123069
Casetti IC, Borsani O, Rumi E. COVID-19 in Patients with Hematologic Diseases. Biomedicines. 2022; 10(12):3069. https://doi.org/10.3390/biomedicines10123069
Chicago/Turabian StyleCasetti, Ilaria Carola, Oscar Borsani, and Elisa Rumi. 2022. "COVID-19 in Patients with Hematologic Diseases" Biomedicines 10, no. 12: 3069. https://doi.org/10.3390/biomedicines10123069