

Evaluation of Supply–Demand Matching of Public Health Resources Based on Ga2SFCA: A Case Study of the Central Urban Area of Tianjin


Abstract
:1. Introduction
2. Study Area and Datasets
2.1. Study Area
2.2. Data Source and Process
2.2.1. Data Source
2.2.2. Data on Public Medical Health Resources
2.2.3. Data on Public Natural Health Resources
2.2.4. Data on Public Physical Health Resources
2.2.5. Basic Geographic Information Data
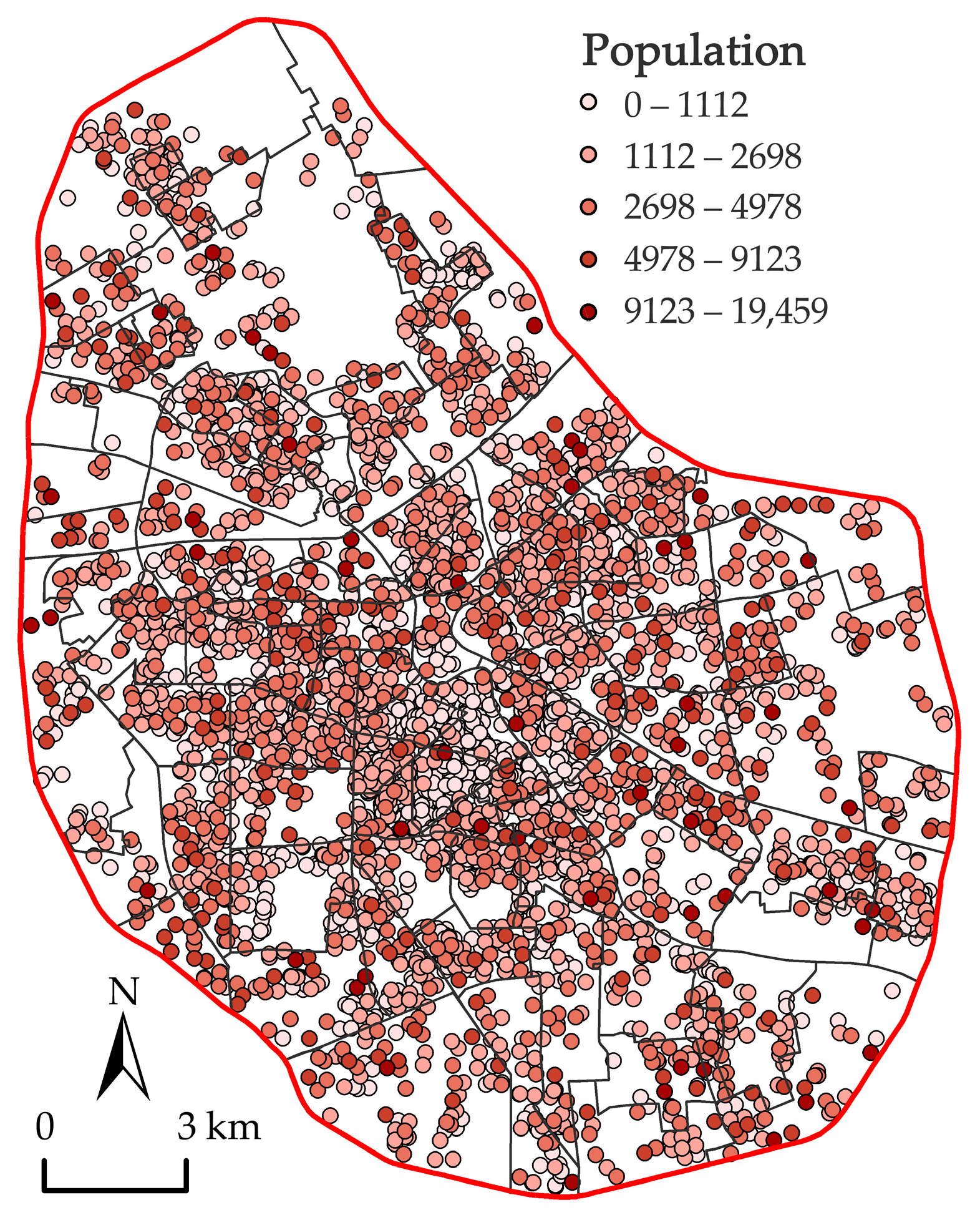
2.2.6. Demographic Data
2.3. Research Framework and Methodology
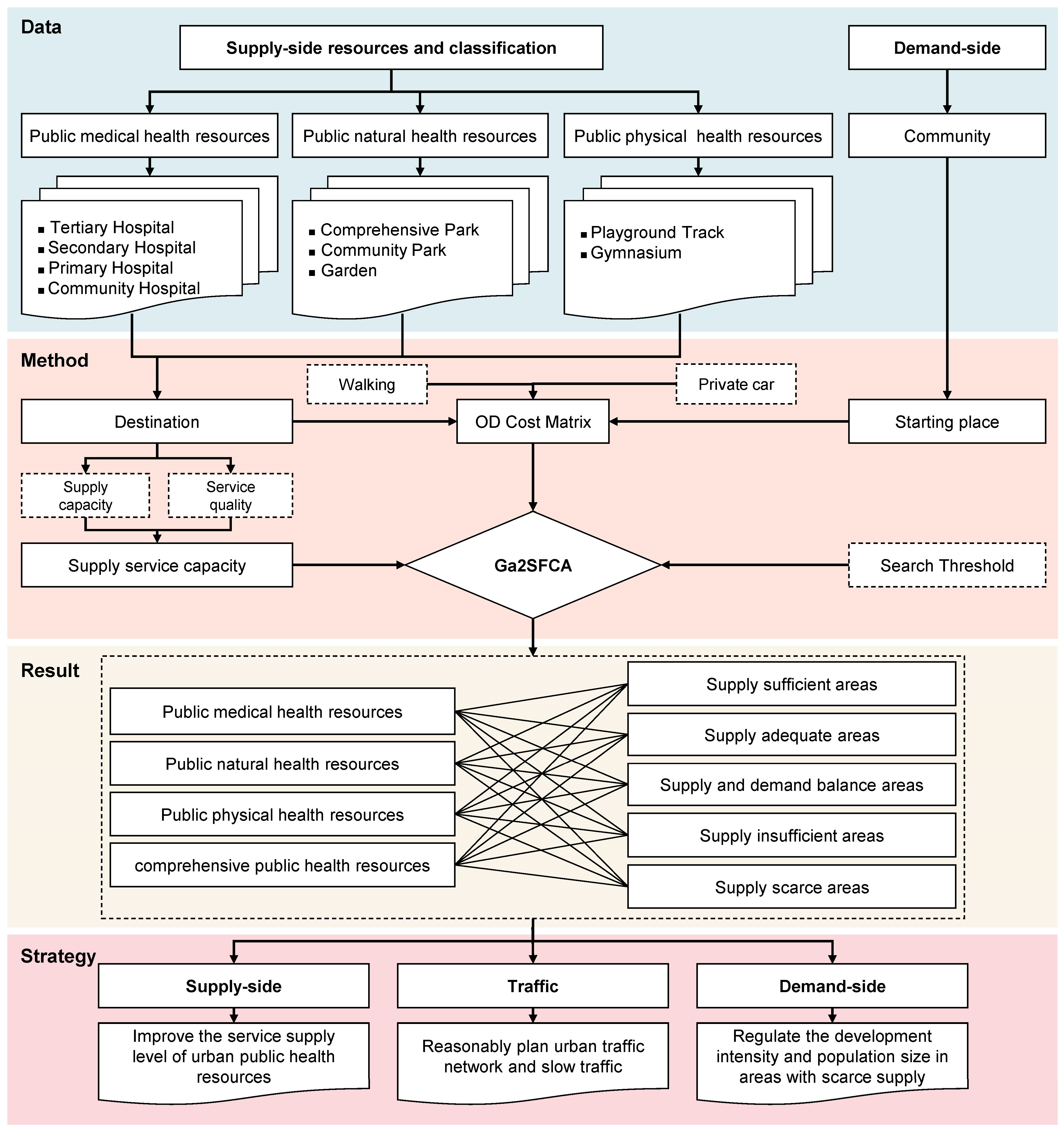
2.3.1. Research Framework
2.3.2. Methodology
3. Results and Analysis
3.1. Single Category Urban Public Health Resources
3.1.1. Public Medical Health Resources
3.1.2. Public Natural Health Resources
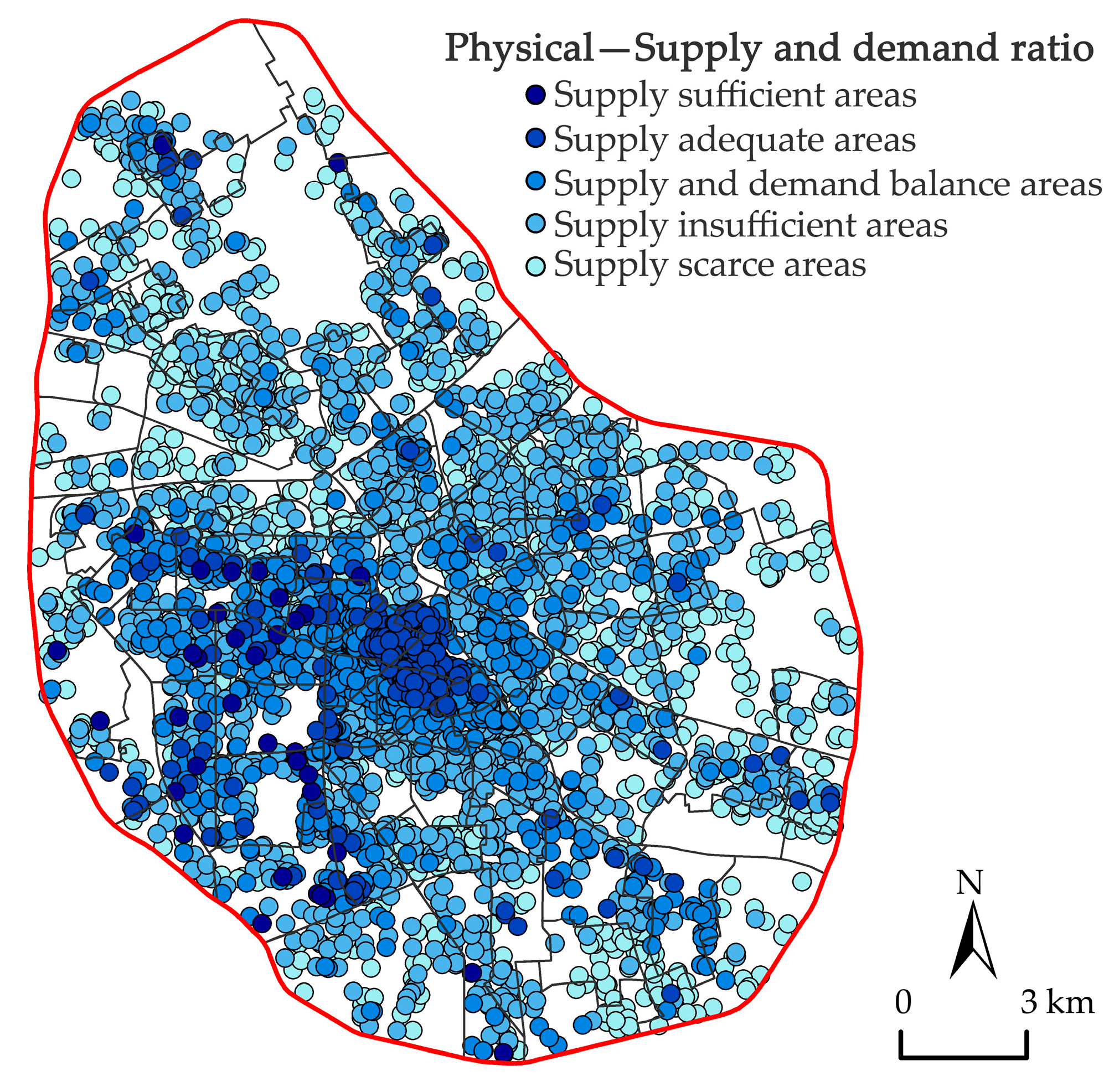
3.1.3. Public Physical Health Resources
3.2. Urban Integrated Public Health Resources
4. Discussion
4.1. Contribution
- (1)
- Firstly, in terms of research perspective, this paper was based on the perspective of urban public health resources and analyzed their SDM assessment using Ga2SFCA. At the same time, it combined two types of travel modes, namely vehicular and pedestrian, and considered a variety of travel space thresholds, which can more accurately depict how residents were traveling. We expect that the analysis in this paper can draw attention to urban public health resources and spread them to other cities and even other countries.
- (2)
- Secondly, on the supply side, this paper adopted a more scientific measurement of supply and service capacity for each category of health resource. It not only considered single-level supply capacity, such as beds, park green space area, sports facility category, etc., but also added hospital grade, blue-green space service index, sports facilities evaluation grade, etc., comprehensively considered supply capacity and service quality, and considered the supply characteristics of resources at multiple levels. It more objectively and truly reflected the supply and service capacity of urban public health resources.
- (3)
- On the demand side, we took the more accurate residential quarter as the starting point, multiplied the number of households in the residential quarter and the average population of Tianjin in 2020 to obtain more accurate population data, and simulated the real population from a more realistic perspective to overcome the problem of the poor accuracy of sub-districts and communities in the current study. The same approach can be adopted for other cities.
- (4)
- Finally, for the results of the resource SDM assessment, the graded statistics can provide precise guidance on the optimization priorities, construction directions, and capital investment in urban public health resource planning and assessment, especially in high-density urban center areas.
4.2. Suggestions
- (1)
- Improving the service supply level of urban public health resources. The Ga2SFCA method used in this paper considers both service quality and resource supply capacity. The government can improve its supply service level in two ways. Firstly, to improve the supply capacity of all kinds of resources, the top–down rational allocation and distribution of resources should be considered, such as choosing more schools in the central urban area of Tianjin to open playgrounds and gymnasiums, increasing the number and construction of playgrounds open to the public in society and calling for the construction of urban running tracks and walking paths to create a city image of fitness for all [57]. Secondly, improving the service quality of health resources should be considered; for example, by establishing a two-way flow between primary hospitals and large hospitals [58] to achieve the technical help of the grassroots medical structure. Comprehensive parks and community class I parks have a large area, and most of these resources in the central urban area of Tianjin are located in marginal areas, it is necessary to enhance the attractiveness of park green space by strengthening its recreational capacity and ecological value. Small park green spaces should increase the installation of rest facilities; larger park green spaces can be equipped with running tracks to form a comprehensive platform for nature and sports which can increase the willingness of residents to visit and to stay.
- (2)
- Reasonable planning of urban transportation road network and slow traffic to improve the accessibility of public health resources. In this study, the Tianjin Haihe River formed a natural barrier in the city, which makes the connection between the two sides of the river weak and the accessibility low; however, it also forms a good water-friendly landscape. The public health resources on both sides of the river should make the most of the natural scenery on both sides, improve pedestrian paths, slow down traffic, and make public health resources easier to access in order to better match supply with demand.
- (3)
- Regulate the development intensity and population scale of areas with scarce supply. Urban public health resources have an irreplaceable position in guaranteeing the physical and mental health of residents. The core area of Tianjin city is a high SDM area, where the population density is low and there is a waste of resources, while the middle and peripheral areas have different kinds of resource shortages, where the population density is high. Based on the principle of social equity, for public medical and physical health resources, the four districts around the city should increase the supply of resources or improve the existing resources to achieve the goal of improving the SDM. For public natural health resources, the supply of resources should be increased in the six districts of the city, while comprehensive parks in Tianjin are mostly located in urban fringe areas, pleasure gardens have greater flexibility, and so, can be injected into urban space through pocket parks and other forms [59]. The idle resources of various types of land in the city can be used to transform and upgrade; for example, small and micro spaces in residential areas can be revitalized to form outdoor fitness venues [54].
4.3. Limitations
5. Conclusions
- (1)
- In the central urban area of Tianjin, different public health resources had varying SDMs. The SDM of public medical health resources was the best, and the SDM of public physical health resources was the worst. Supply insufficient and scarce areas were primarily found in the peripheral areas of the four districts around the city and the six districts of the inner city, which are the future focus areas for optimizing the organization of diverse public health resources and enhancing the standard of care. These are the crucial areas for optimizing the organization of diverse public health resources and raising the standard of service.
- (2)
- The spatial differentiation of the supply and demand of various public health resources was obvious. The SDM of public medical health resources and public physical health resources generally showed the characteristics of high in the core and low at the periphery, while the SDM of public natural health resources generally showed the trend of high in the core, low in the middle, and high at the periphery.
- (3)
- The SDM of integrated public health resources in the central city of Tianjin was generally good. The SDM value showed a gradually decreasing circle structure from the core area to the peripheral area, with 35.47% of the population being located in insufficient and scarce areas. At the same time, the SDM in the central city of Tianjin reflected a mixed distribution of high and low values, and the distribution of high values of SDM showed a multi-center aggregation phenomenon, forming a pattern of decreasing multi-centeredness. Most of these centers were located in the sub-district of Quanyechang, Xiaobailou, Sports Center, and Liulin. From the perspective of the comprehensive regulation of the SDM of urban public health resources, the SDM degree of urban fringe areas should be systematically improved, focusing on the improvement of urban transportation road networks and slow traffic level.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Fang, P.Q.; Dong, S.P.; Xiao, J.J.; Liu, C.J.; Feng, X.W.; Wang, Y.P. Regional inequality in health and its determinants: Evidence from China. Health Policy 2010, 94, 14–25. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Deng, Z.H.; Chen, Y.Y.; Liao, J.Z.; Li, G.; Lu, Y.B. How Resource Scarcity and Accessibility Affect Patients’ Usage of Mobile Health in China: Resource Competition Perspective. JMIR mHealth uHealth 2019, 7, e13491. [Google Scholar] [CrossRef] [PubMed]
- Brown, G.; Schebella, M.F.; Weber, D. Using participatory GIS to measure physical activity and urban park benefits. Landscape Urban Plan. 2014, 121, 34–44. [Google Scholar] [CrossRef]
- White, R.L.; Babic, M.J.; Parker, P.D.; Lubans, D.R.; Astell-Burt, T.; Lonsdale, C. Domain-Specific Physical Activity and Mental Health: A Meta-analysis. Am. J. Prev. Med. 2017, 52, 653–666. [Google Scholar] [CrossRef]
- Zhu, J.X.; Xu, Q.; Pan, Y.; Qiu, L.F.; Peng, Y.; Bao, H.J. Land-Acquisition and Resettlement (LAR) Conflicts: A Perspective of Spatial Injustice of Urban Public Resources Allocation. Sustainability 2018, 10, 884. [Google Scholar] [CrossRef] [Green Version]
- Richter, R.W.; Bengen, B.; Alsup, P.A.; Bruun, B.; Kilcoyne, M.M.; Challenor, B.D. A Resource for Improved Health Care Delivery. Am. J. Public Health 1974, 64, 1056–1061. [Google Scholar] [CrossRef] [Green Version]
- Zhang, D.H.; Zhou, C.S.; He, B.J. Spatial and temporal heterogeneity of urban land area and PM2.5 concentration in China. Urban Climate 2022, 45, 101268. [Google Scholar] [CrossRef]
- Hancock, T. The evolution, impact and significance of the healthy cities/healthy communities movement. J. Public Health Policy 1993, 14, 5–18. [Google Scholar] [CrossRef]
- Hayes, M. ‘Man, disease and environmental associations’: From medical geography to health inequalities. Prog. Hum. Geog. 1999, 23, 289–296. [Google Scholar] [CrossRef]
- International Health Conference. Constitution of the World Health Organization 1946; World Health Organization: Geneva, Switzerland, 2002; Volume 80, pp. 983–984. [Google Scholar]
- Woo, J.; Chan, R.; Leung, J.; Wong, M. Relative contributions of geographic, socioeconomic, and lifestyle factors to quality of life, frailty, and mortality in elderly. PLoS ONE 2010, 5, e8775. [Google Scholar] [CrossRef]
- Padilla, C.M.; Deguen, S.; Lalloue, B.; Blanchard, O.; Beaugard, C.; Troude, F.; Navier, D.Z.; Vieira, V.M. Cluster analysis of social and environment inequalities of infant mortality. A spatial study in small areas revealed by local disease mapping in France. Sci. Total Environ. 2013, 454, 433–441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastos, L.; Silveira, J.C.; Luna, C.F.; Lucena-Silva, N. Childhood and Adolescent Cancer in the State of Pernambuco, Brazil: Incidence, Geographical Distribution, and Association with Environmental Health Indicators. J. Pediatr. Hematol. Onc. 2018, 40, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Q.; Meng, J.Q.; Leng, H. Urban spatial impacts on residents’health risk caused by climate changeand planning intervention. City Plan. Rev. 2021, 45, 71–80. (In Chinese) [Google Scholar]
- Price, C.W. Healthy Cities Indicators: Analysis of Data from Cities across Europe; WHO Regional Office for Europe: Copenhagen, Denmark, 1997. [Google Scholar]
- Wang, L.; Liao, S.W.; Zhao, X.J. Exploration of approaches and factors of healthy city planning. Urban Plan. Int. 2016, 31, 4–9. [Google Scholar] [CrossRef] [Green Version]
- Wolch, J.R.; Byrne, J.; Newell, J.P. Urban green space, public health, and environmental justice: The challenge of making cities ‘just green enough’. Landscape Urban Plan. 2014, 125, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Sallis, J.F.; Cerin, E.; Conway, T.L.; Adams, M.A.; Frank, L.D.; Pratt, M.; Salvo, D.; Schipperijn, J.; Smith, G.; Cain, K.L.; et al. Physical activity in relation to urban environments in 14 cities worldwide: A cross-sectional study. Lancet 2016, 387, 2207–2217. [Google Scholar] [CrossRef] [Green Version]
- Asaria, M.; Ali, S.; Doran, T.; Ferguson, B.; Fleetcroft, R.; Goddard, M.; Goldblatt, P.; Laudicella, M.; Raine, R.; Cookson, R. How a universal health system reduces inequalities: Lessons from England. J. Epidemiol. Commun. H 2016, 70, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.H.; Zhang, G.J.; Zhou, C.S. Differences in Accessibility of Public Health Facilities in Hierarchical Municipalities and the Spatial Pattern Characteristics of Their Services in Doumen District, China. Land 2021, 10, 1249. [Google Scholar] [CrossRef]
- Higgs, G.; Langford, M.; Norman, P. Accessibility to sport facilities in Wales: A GIS-based analysis of socioeconomic variations in provision. Geoforum 2015, 62, 105–120. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Zhou, Z.H.; Chen, J.; Cheng, W.; Chen, J. Analysis of Location Selection of Public Service Facilities Based on Urban Land Accessibility. Int. J. Env. Res. Public Health 2021, 18, 516. [Google Scholar] [CrossRef]
- Azmoodeh, M.; Haghighi, F.; Motieyan, H. Proposing an integrated accessibility-based measure to evaluate spatial equity among different social classes. Environ. Plan. B-Urban 2021, 48, 2790–2807. [Google Scholar] [CrossRef]
- Jiang, Y.P.; Zhen, F.; Sun, H.H. Spatial characteristics of urban health resources at block scale—A case study of central urban area of NanJing. Econ. Geogr. 2018, 38, 85–94. (In Chinese) [Google Scholar] [CrossRef]
- Reyes, M.; Paez, A.; Morency, C. Walking accessibility to urban parks by children: A case study of Montreal. Landscape Urban Plan. 2014, 125, 38–47. [Google Scholar] [CrossRef]
- Zeng, W.; Xiang, L.L.; Zhang, X.L. Research in spatial pattern of accessibility to community service facilitiesand spatial deprivation of low income community in NanJing. Hum. Geogr. 2017, 32, 73–81. (In Chinese) [Google Scholar] [CrossRef]
- Kelobonye, K.; Zhou, H.; McCarney, G.; Xia, J.H. Measuring the accessibility and spatial equity of urban services under competition using the cumulative opportunities measure. J. Transp. Geogr. 2020, 85, 101268. [Google Scholar] [CrossRef]
- Yang, N.; Chen, S.Y.; Hu, W.L.; Wu, Z.G.; Chao, Y. Spatial Distribution Balance Analysis of Hospitals in Wuhan. Int. J. Env. Res. Public Health 2016, 13, 971. [Google Scholar] [CrossRef] [Green Version]
- Kong, Y.F.; Li, X.J.; Zhang, X.F. Analysis of spatial accessibility for school redistricting in rural China: A case study of the secondary schools in GongYi city, HeNan Province. Natl. Remote Sens. Bull. 2008, 12, 800–809. [Google Scholar]
- Luo, W.; Wang, F.H. Measures of spatial accessibility to health care in a GIS environment: Synthesis and a case study in the Chicago region. Environ. Plan. B-Plan. Design 2003, 30, 865–884. [Google Scholar] [CrossRef] [Green Version]
- Ngui, A.N.; Apparicio, P. Optimizing the two-step floating catchment area method for measuring spatial accessibility to medical clinics in Montreal. BMC Health Serv. Res. 2011, 11, 166. [Google Scholar] [CrossRef] [Green Version]
- Luo, W.; Qi, Y. An enhanced two-step floating catchment area (E2SFCA) method for measuring spatial accessibility to primary care physicians. Health Place 2009, 15, 1100–1107. [Google Scholar] [CrossRef]
- Dai, D.J. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 2010, 16, 1038–1052. [Google Scholar] [CrossRef]
- Dai, D. Racial/ethnic and socioeconomic disparities in urban green space accessibility: Where to intervene? Landscape Urban Plan. 2011, 102, 234–244. [Google Scholar] [CrossRef]
- Tao, Z.L.; Cheng, Y.; Dai, T.Q. Measuring spatial accessibility to residential care facilities in Beijing. Prog. Geogr. 2014, 33, 616–624. (In Chinese) [Google Scholar] [CrossRef]
- Wan, N.; Zou, B.; Sternberg, T. A three-step floating catchment area method for analyzing spatial access to health services. Int. J. Geogr. Inf. Sci. 2012, 26, 1073–1089. [Google Scholar] [CrossRef]
- Bell, S.; Wilson, K.; Bissonnette, L.; Shah, T. Access to Primary Health Care: Does Neighborhood of Residence Matter? Ann. Assoc. Am. Geogr. 2013, 103, 85–105. [Google Scholar] [CrossRef]
- Delamater, P.L. Spatial accessibility in suboptimally configured health care systems: A modified two-step floating catchment area (M2SFCA) metric. Health Place 2013, 24, 30–43. [Google Scholar] [CrossRef]
- Luo, J. Integrating the Huff Model and Floating Catchment Area Methods to Analyze Spatial Access to Healthcare Services. Trans. Gis 2014, 18, 436–448. [Google Scholar] [CrossRef]
- Sahebgharani, A.; Haghshenas, H. Analyzing accessibility to fire stations: A floating catchment area model for stochastic transportation networks with travel time correlation. Trans. Gis. 2022, 26, 182–200. [Google Scholar] [CrossRef]
- Chen, B.Y.; Cheng, X.P.; Kwan, M.P.; Schwanen, T. Evaluating spatial accessibility to healthcare services under travel time uncertainty: A reliability-based floating catchment area approach. J. Transp. Geogr. 2020, 87, 102794. [Google Scholar] [CrossRef]
- Yang, L.A.; Zhang, S.M.; Guan, M.; Cao, J.F.; Zhang, B.L. An Assessment of the Accessibility of Multiple Public Service Facilities and Its Correlation with Housing Prices Using an Improved 2SFCA Method-A Case Study of Jinan City, China. Isprs Int. J. Geo-Inf. 2022, 11, 414. [Google Scholar] [CrossRef]
- Wei, Y.; Xiu, C.L.; Gao, R.; Wang, Q. Evaluation of green space accessibility of Shenyang using Gaussian-based 2step floating catchment area method. Prog. Geogr. 2014, 33, 479–487. [Google Scholar] [CrossRef]
- Hu, S.J.; Song, W.; Li, C.G.; Lu, J. A multi-mode Gaussian-based two-step floating catchment area method for measuring accessibility of urban parks. Cities 2020, 105, 102815. [Google Scholar] [CrossRef]
- Qian, T.L.; Chen, J.; Li, A.; Wang, J.C.; Shen, D.T. Evaluating Spatial Accessibility to General Hospitals with Navigation and Social Media Location Data: A Case Study in Nanjing. Int. J. Env. Res. Public Health 2020, 17, 2752. [Google Scholar] [CrossRef]
- Wei, F. Greener urbanization? Changing accessibility to parks in China. Landscape Urban Plan. 2017, 157, 542–552. [Google Scholar] [CrossRef]
- Xiao, T.; Ding, T.F.; Zhang, X.K.; Tao, Z.L.; Liu, Y. Spatial Accessibility to Sports Facilities in Dongguan, China: A Multi-Preference Gaussian Two-Step Floating Catchment Area Method. Appl. Spat. Anal. Policy 2022, 15, 1093–1114. [Google Scholar] [CrossRef]
- Ran, Z.; Zhou, G.H.; Zhang, H.H.; Tang, C.L.; Chen, W.Y. Spatial correlation between urban health resources and population distribution: A case study of the central urban area of Changsha City. Resour. Sci. 2019, 41, 1488–1499. (In Chinese) [Google Scholar] [CrossRef]
- Wang, F.; Zhu, M.W.; Chen, C.W.; Xiao, Y.; Zhang, X.X. Equity of urban health resources based on walkability and spatial distribution of population: A case study of the central urban area of Guangzhou City. Resour. Sci. 2021, 43, 390–402. [Google Scholar] [CrossRef]
- Tencent.189. School Stadiums and Gymnasiums in Tianjin are Open to the Public! (2019-12-05). Available online: https://new.qq.com/omn/20191205/20191205A0ME6G00.html (accessed on 30 April 2022).
- Rigolon, A. A complex landscape of inequity in access to urban parks: A literature review. Landscape Urban Plan. 2016, 153, 160–169. [Google Scholar] [CrossRef]
- Wang, F.Y.; Wang, K.Y.; Liu, H.C. Evaluation and influence factors of spatial accessibility of ecological space recreation service in the Pearl River Delta Urban Agglomeration: A modified Two-step Floating Catchment Area method. Acta Ecol. Sin. 2020, 40, 3622–3633. (In Chinese) [Google Scholar]
- Fu, Y.; Guo, Q.Z.; Wu, X.X. Land surface temperature inversion in Tianjin city based on landsat 8 remote sensing data. Environ. Monit. China 2018, 34, 165–172. (In Chinese) [Google Scholar] [CrossRef]
- Wei, F.; Wang, X. Measuring spatial accessibility to physical activity spaces in Hangzhou using 2SFCA method. City Plan. Rev. 2019, 43, 112–119. (In Chinese) [Google Scholar]
- Zhang, D.H.; Zhou, C.S.; Sun, D.Q.; Qian, Y. The influence of the spatial pattern of urban road networks on the quality of business environments: The case of Dalian City. Environ. Dev. Sustain. 2022, 24, 9429–9446. [Google Scholar] [CrossRef]
- Tianjin Municipal Bureau of Statistics. Survey Office of the National Bureau of Statistics in Tianjin. Tianjin Statistical Yearbook 2021; China Statistical Press: Tianjin, China, 2021. [Google Scholar]
- Giles-Corti, B.; Vernez-Moudon, A.; Reis, R.; Turrell, G.; Dannenberg, A.L.; Badland, H.; Foster, S.; Lowe, M.; Sallis, J.F.; Stevenson, M.; et al. City planning and population health: A global challenge. Lancet 2016, 388, 2912–2924. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Yin, Z.; Xie, Q. Suggestions to ameliorate the inequity in urban/rural allocation of healthcare resources in China. Int. J. Equity Health 2014, 13, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Peschardt, K.K.; Stigsdotter, U.K.; Schipperrijn, J. Identifying Features of Pocket Parks that May Be Related to Health Promoting Use. Landscape Res. 2016, 41, 79–94. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Resource Name | Data Type | Remarks | Source |
|---|---|---|---|
| Public Medical Health Resources | Directory, Grade, Address (2022) | Provided by official statistics of Tianjin Municipal Health Commission | |
| Coordinate (2022) | Baidu Maps API “https://lbsyun.baidu.com” (accessed on 25 March 2022) | ||
| Number of beds | General beds (2022) | WeDoctor “https://www.guahao.com/” (accessed on 25 March 2022) | |
| Official websites of hospitals | |||
| Missing beds | Table 2 | ||
| Public Natural Health Resources | Directory, Address (2022) | Provided by Tianjin Landscape Management Office | |
| Grade (2019) | 《GBT51346-2019 Standard for Urban Green Space Planning》 | ||
| Coordinate, Faceted data of parks (2022) | Baidu Maps API “https://lbsyun.baidu.com/” (accessed on 10 April 2022) | ||
| landsat8 OLI/TIRS (2021-8-11) | Geospatial Data Cloud “http://www.gscloud.cn/”(accessed on 10 April 2022) | ||
| Public Physical Health Resources | Directory, Address of playground track (2022) | Web published data [50] | |
| Coordinate of playground track (2022) | Baidu Maps API “https://lbsyun.baidu.com/” (accessed on 25 April 2022) | ||
| Coordinate of stadiums (2022) | Yelp “https://www.dianping.com/” (accessed on 25 April 2022) | ||
| Vectored data (2022) | Open Street Map “https://master.apis.dev.openstreetmap.org/” (accessed on 15 April 2022) | ||
| Name, Households, Coordinate (2022-2) | Anjuke “https://tianjin.anjuke.com/” (accessed on 20 April 2022) | ||
| Type of Various Function Hospital | Reference Number of Beds |
|---|---|
| Health center, infirmary, health station | 4 |
| Comprehensive outpatient clinics, Chinese medicine clinics, specialist clinics, staff hospitals | 10 |
| General hospital, community hospital, maternal and child health center | 50 |
| Chinese medicine hospital, combined Chinese and Western medicine hospital, specialist hospital | 50 |
| Resource Name | Categories | Travel Mode | Spatial Search Threshold | Weights |
|---|---|---|---|---|
| Public Medical Health Resources | Tertiary Hospital | By car | Maximum passage time between supply and demand points | 0.426 |
| Secondary Hospital | On foot | 30 min | ||
| Primary Hospital | On foot | 20 min | ||
| Community Hospital | On foot | 15 min life circle | ||
| Public Natural Health Resources | Comprehensive Park | By car | Maximum passage time between supply and demand points | 0.328 |
| Community Class I Park | By car | 30 min | ||
| Community Class II Park | On foot | 20 min | ||
| Garden | On foot | 15 min life circle | ||
| Public Physical Health Resources | Playground Track | On foot | 15 min life circle | 0.246 |
| Gymnasium | On foot | 15 min life circle |
| SDM Level | SDM Value | Population | |
|---|---|---|---|
| Quantity | Percentage | ||
| Supply sufficient areas | 0.0071–0.0564 | 345,777 | 4.73% |
| Supply adequate areas | 0.0064–0.0071 | 1,928,586 | 26.40% |
| Supply and demand balance areas | 0.0057–0.0064 | 2,884,103 | 39.48% |
| Supply insufficient areas | 0.0015–0.0057 | 2,117,395 | 28.98% |
| Supply scarce areas | 0–0.0015 | 30,034 | 0.41% |
| SDM Level | SDM Value | Population | |
|---|---|---|---|
| Quantity | Percentage | ||
| Supply sufficient areas | 6.36–9.01 | 47,600 | 0.65% |
| Supply adequate areas | 5.57–6.36 | 1,664,983 | 22.79% |
| Supply and demand balance areas | 5.25–5.57 | 2,986,481 | 40.88% |
| Supply insufficient areas | 0.80–5.25 | 2,576,797 | 35.27% |
| Supply scarce areas | 0–0.80 | 30,034 | 0.41% |
| SDM Level | SDM Value | Population | |
|---|---|---|---|
| Quantity | Percentage | ||
| Supply sufficient areas | 0.0148–0.0391 | 51,954 | 0.71% |
| Supply adequate areas | 0.0084–0.0148 | 228,396 | 3.13% |
| Supply and demand balance areas | 0.0053–0.0084 | 977,378 | 13.38% |
| Supply insufficient areas | 0.0027–0.0053 | 2,917,989 | 39.94% |
| Supply scarce areas | 0–0.0027 | 3,130,178 | 42.84% |
| SDM Level | SDM Value | Population | |
|---|---|---|---|
| Quantity | Percentage | ||
| Supply sufficient areas | 0.31–0.61 | 260,396 | 3.56% |
| Supply adequate areas | 0.28–0.31 | 1,283,130 | 17.56% |
| Supply and demand balance areas | 0.25–0.28 | 3,170,767 | 43.40% |
| Supply insufficient areas | 0.13–0.25 | 2,561,568 | 35.06% |
| Supply scarce areas | 0–0.13 | 30,034 | 0.41% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, X.; Zeng, S.; Namaiti, A.; Zeng, J. Evaluation of Supply–Demand Matching of Public Health Resources Based on Ga2SFCA: A Case Study of the Central Urban Area of Tianjin. ISPRS Int. J. Geo-Inf. 2023, 12, 156. https://doi.org/10.3390/ijgi12040156
Guo X, Zeng S, Namaiti A, Zeng J. Evaluation of Supply–Demand Matching of Public Health Resources Based on Ga2SFCA: A Case Study of the Central Urban Area of Tianjin. ISPRS International Journal of Geo-Information. 2023; 12(4):156. https://doi.org/10.3390/ijgi12040156
Chicago/Turabian StyleGuo, Xiaoyu, Suiping Zeng, Aihemaiti Namaiti, and Jian Zeng. 2023. "Evaluation of Supply–Demand Matching of Public Health Resources Based on Ga2SFCA: A Case Study of the Central Urban Area of Tianjin" ISPRS International Journal of Geo-Information 12, no. 4: 156. https://doi.org/10.3390/ijgi12040156