
Impact of Environmental Exposure on Chronic Diseases in China and Assessment of Population Health Vulnerability

Abstract
:1. Introduction
2. Materials and Methods
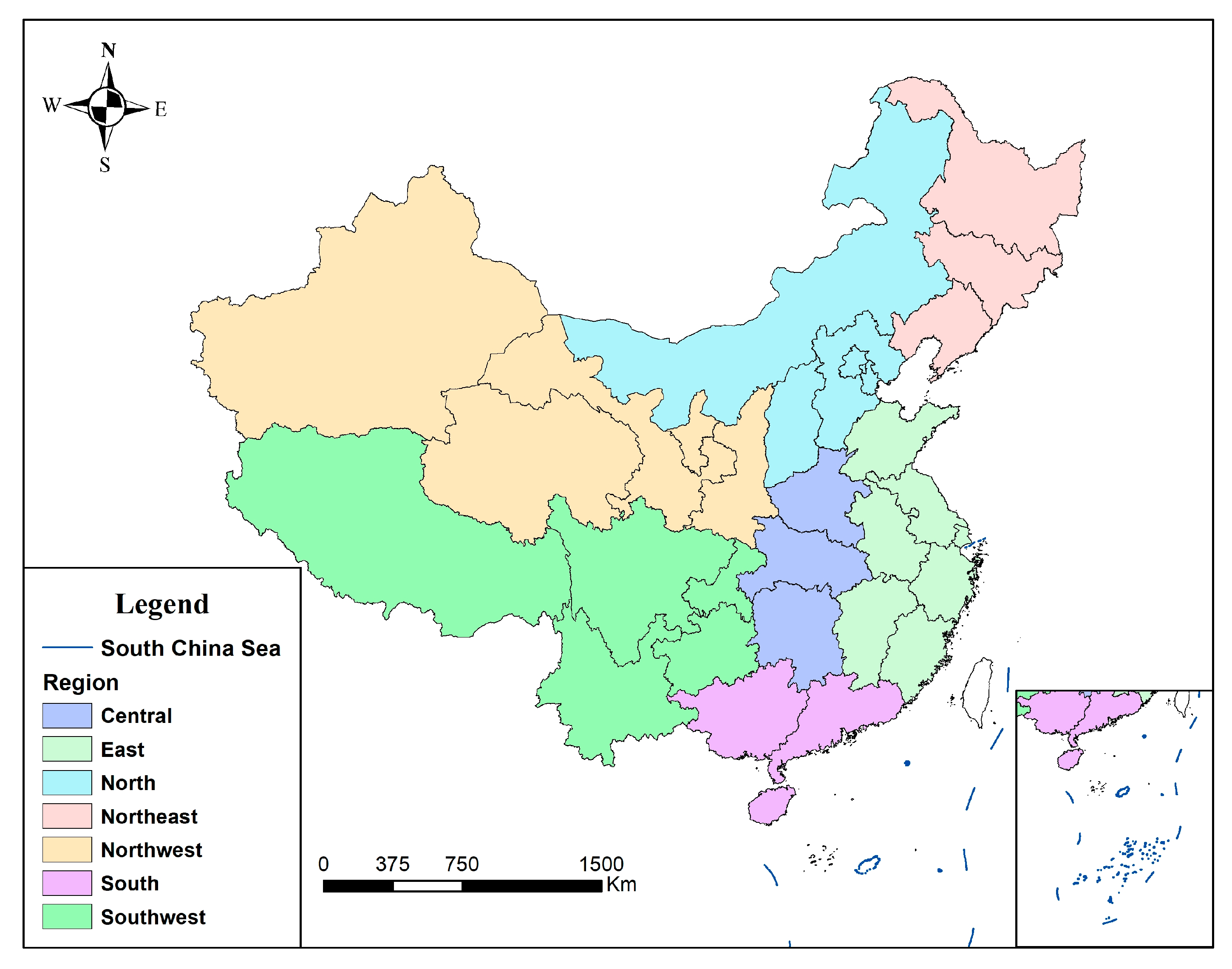
2.1. Study Area
2.2. Exposure–Sensitivity–Adaptability Framework
2.3. Calculation of Exposure Indexes
2.4. Calculation of Sensitivity and Adaptability Indexes
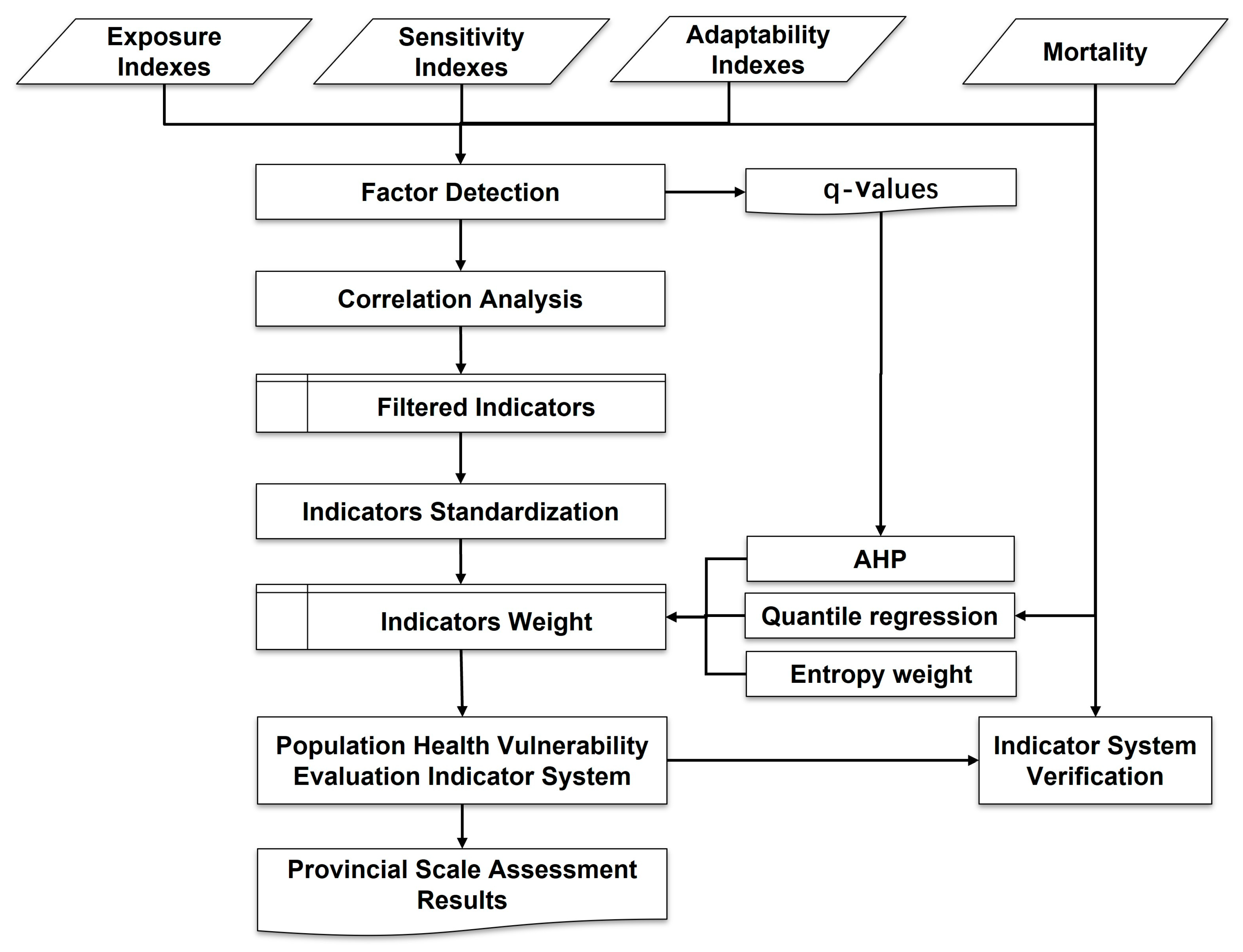
2.5. Evaluation Method of Population Health Vulnerability
3. Results
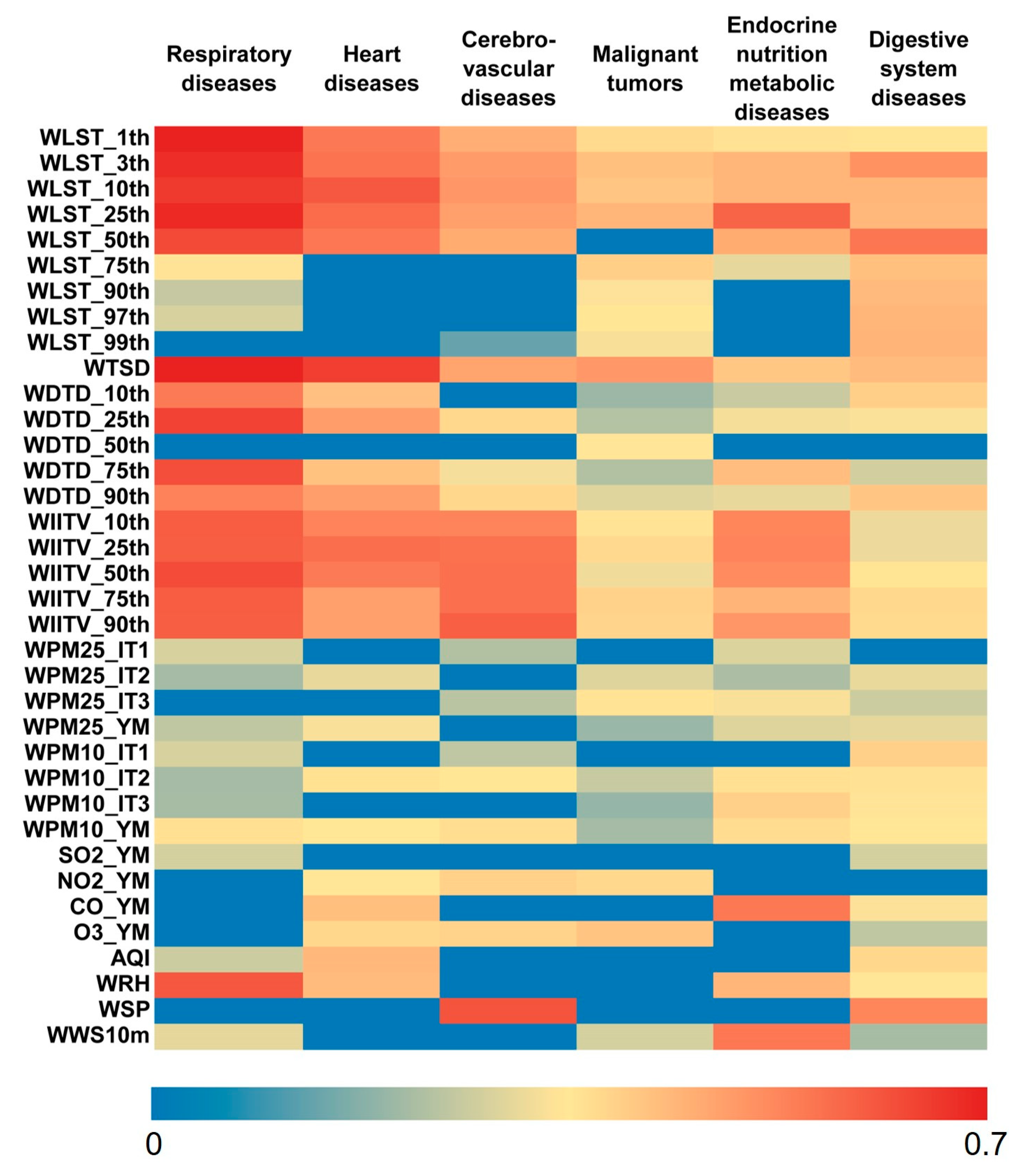
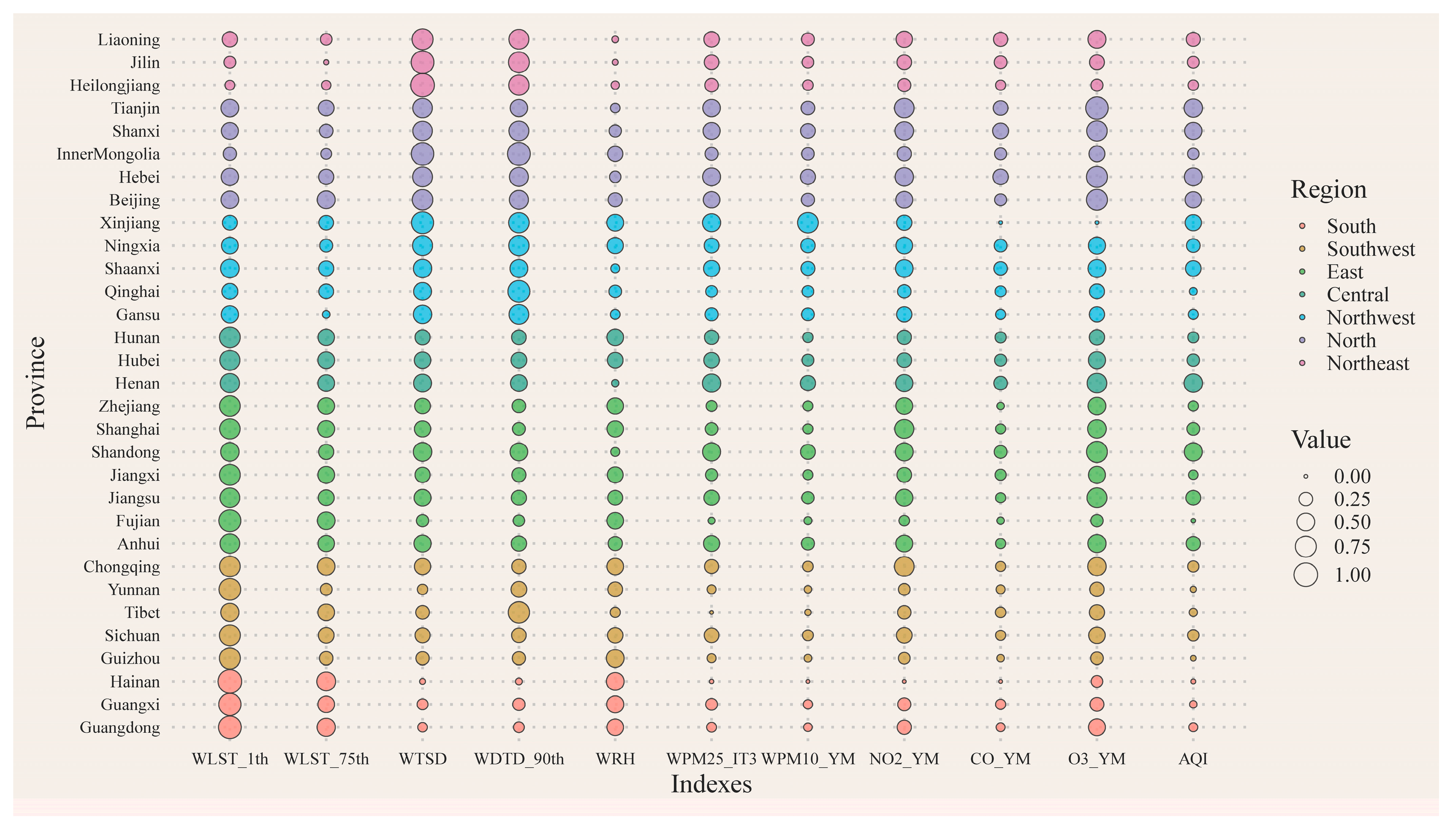
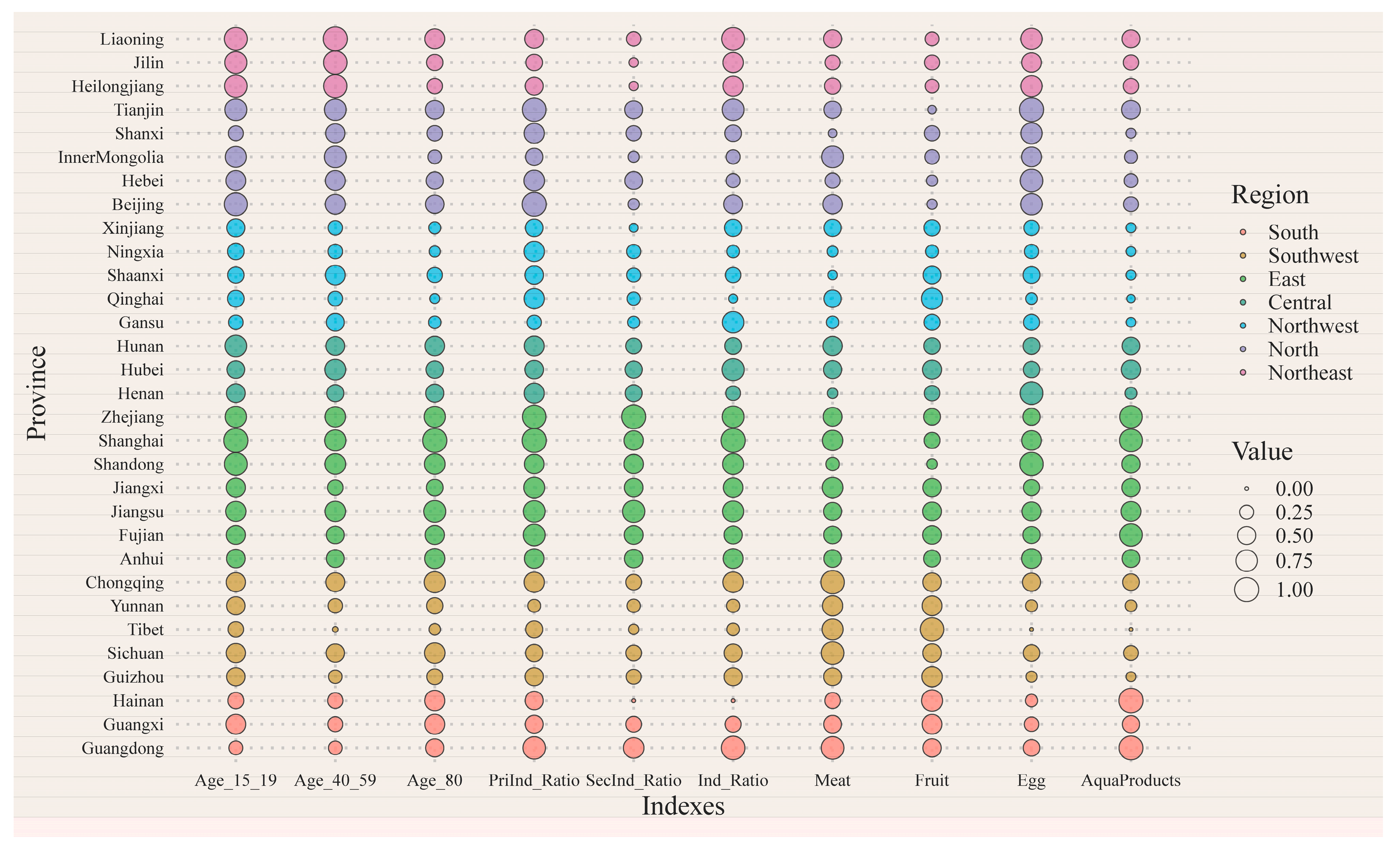
3.1. Factor Detection Results of Exposure Indexes
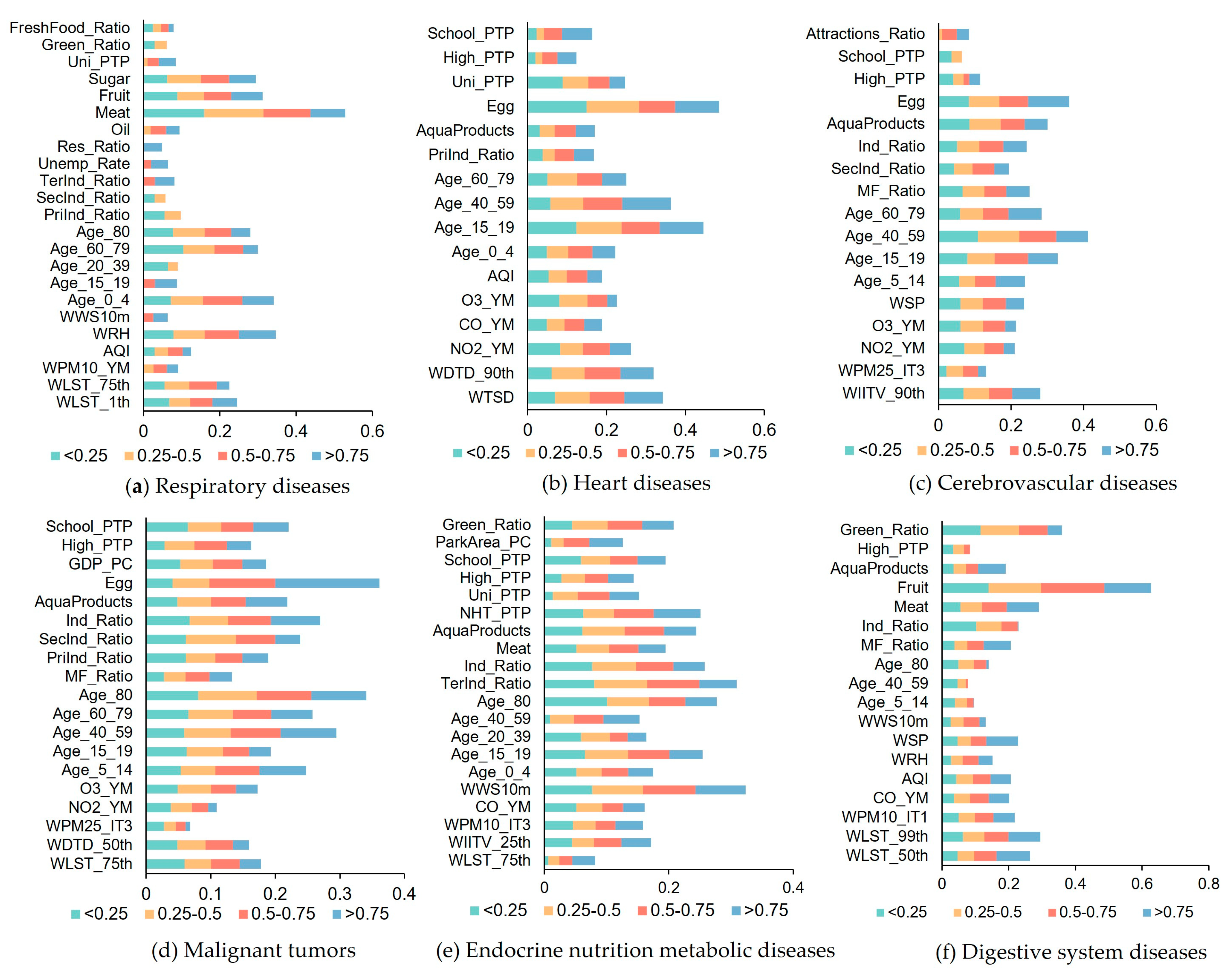
3.2. The Correlation between the Filtered Indicators and Chronic Diseases
3.3. Comparison of Different Weight Determination Methods
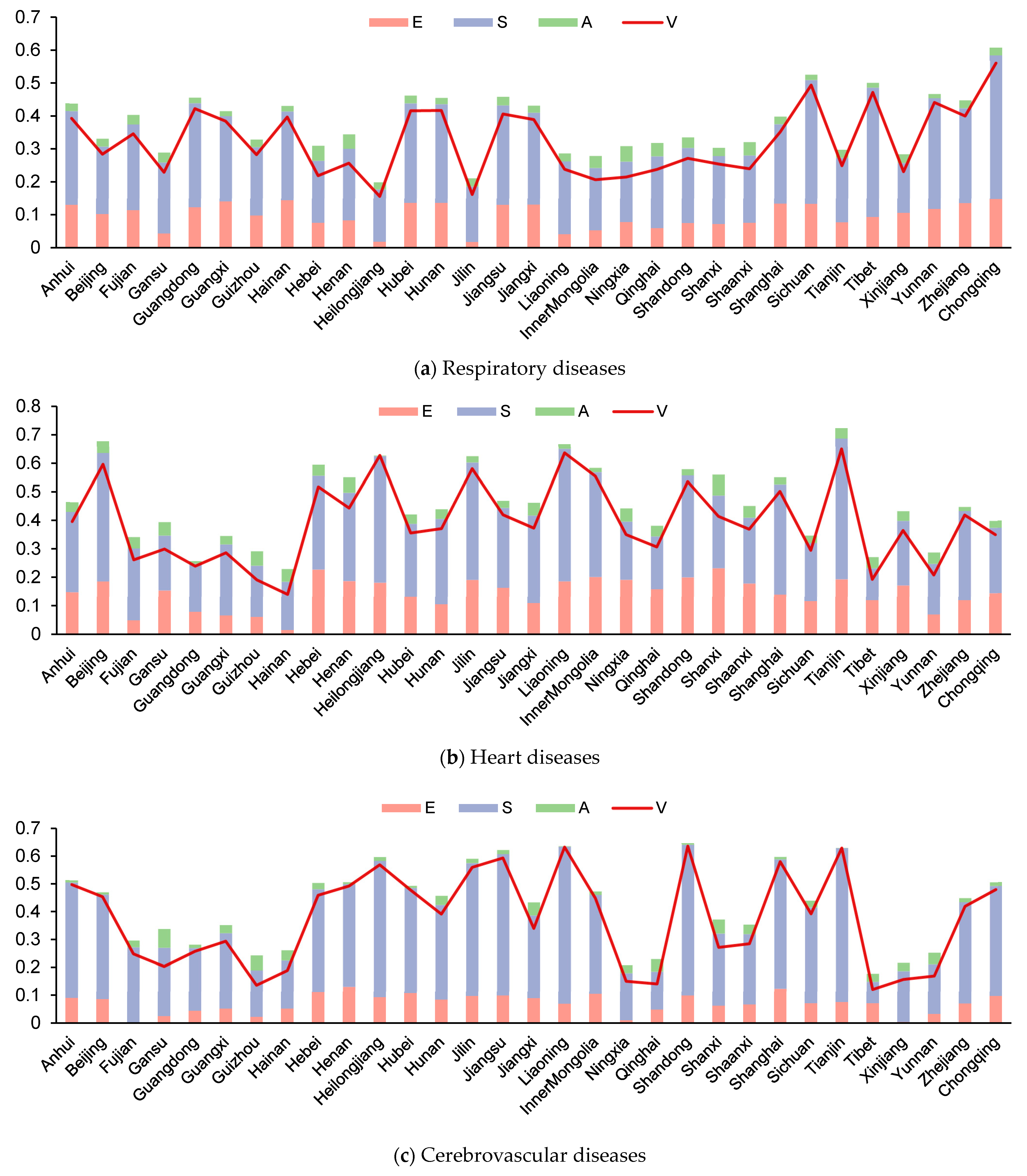
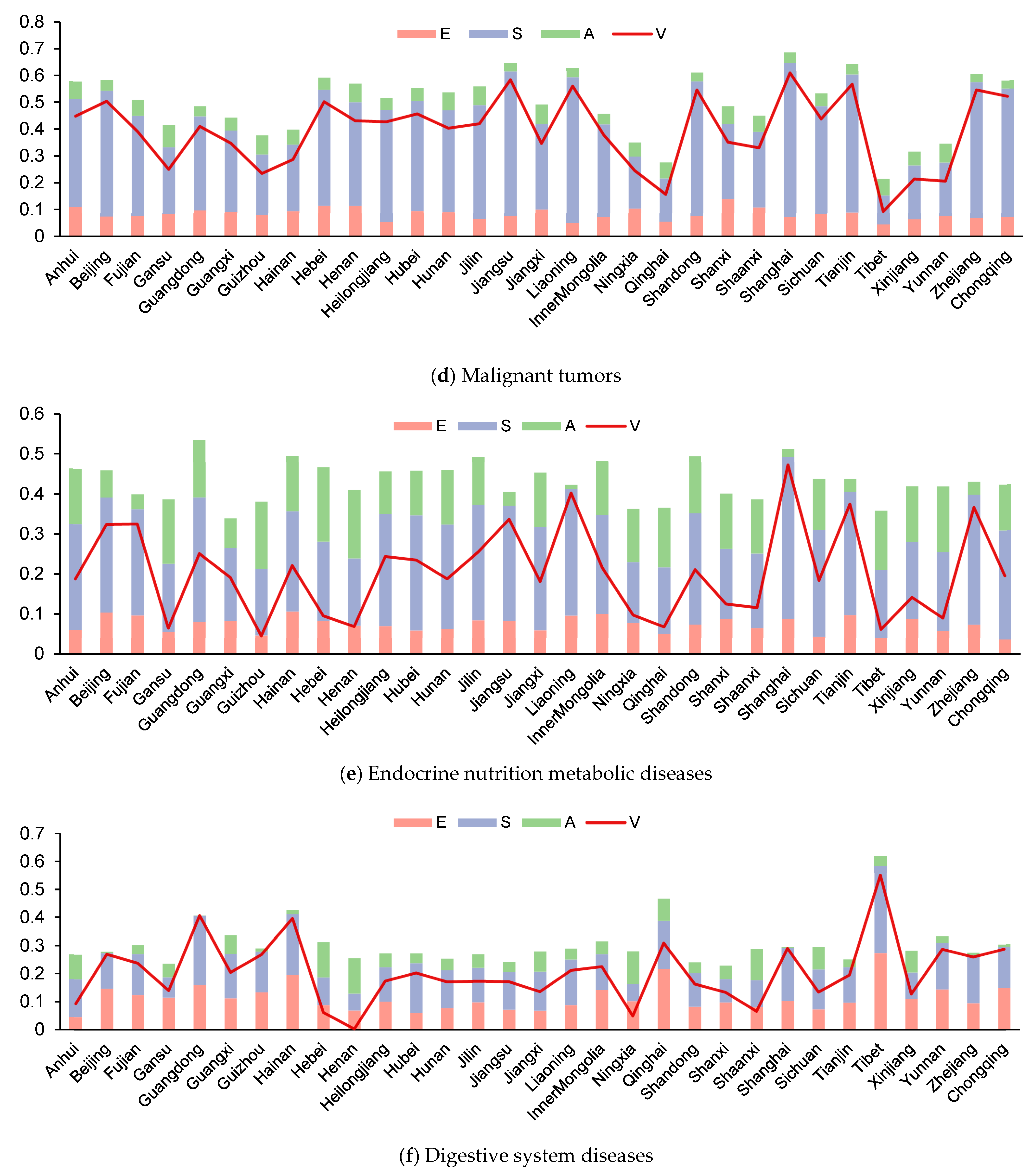
3.4. Analysis of the Results of Health Vulnerability Assessment and Main Related Factors in Different Provinces
4. Discussion
4.1. Estimation Error of Air Pollution Exposure
4.2. Explanation of the Influence of Main Sensitivity and Adaptability Indexes on the Health Vulnerability of People
4.3. Influential Factors of Chronic Diseases Not Considered in This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ghassemi, H.; Harrison, G.; Mohammad, K. An accelerated nutrition transition in Iran. Public Health Nutr. 2002, 5, 149–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gracey, M. Child health in an urbanizing world. Acta Paediatr. 2002, 91, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Keiser, J.; Utzinger, J.; Castro, M.; Smith, T.; Tanner, M.; Singer, B. Urbanization in Sub-Saharan Africa and Implication for Malaria Control. Am. J. Trop. Med. Hyg. 2004, 71, 118–127. [Google Scholar] [CrossRef] [Green Version]
- McMichael, A. The urban environment and health in a world of increasing globalization: Issues for developing countries. Bull. World Health Organ. 2000, 78, 1117–1126. [Google Scholar] [PubMed]
- Mutatkar, R.K. Public health problems of urbanization. Soc. Sci. Med. 1995, 41, 977–981. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B. The Nutrition Transition and Obesity in the Developing World. J. Nutr. 2001, 131, 871S–873S. [Google Scholar] [CrossRef] [Green Version]
- Popkin, B.M.; Gordon-Larsen, P. The nutrition transition: Worldwide obesity dynamics and their determinants. Int. J. Obes. Relat. Metab. Disord. 2004, 28 (Suppl. 3), S2–S9. [Google Scholar] [CrossRef] [Green Version]
- Xiong, Z. Challenges and countermeasures in the prevention and treatment of chronic diseases. Chin. J. Prev. Control. Chronic Dis. 2019, 27, 720–721. (In Chinese) [Google Scholar]
- Forastiere, F.; Agostini, D.; Caranci, N.; de’Donato, F.; Demaria, M.; Michelozzi, P.; Miglio, R.; Rognoni, M.; Russo, A.; Perucci, C. Factors affecting in-hospital heat-related mortality: A multi-city case-crossover analysis. J. Epidemiol. Community Health 2008, 62, 209–215. [Google Scholar]
- Zanobetti, A.; O’Neill, M.; Gronlund, C.; Schwartz, J. Susceptibility to Mortality in Weather Extremes Effect Modification by Personal and Small-Area Characteristics. Epidemiology 2013, 24, 809–819. [Google Scholar] [CrossRef] [Green Version]
- Chen, G.; Zhang, Y.; Song, G.; Jiang, L.; Zhao, N.; Chen, B.; Kan, H. Is diurnal temperature range a risk factor for acute stroke death? Int. J. Cardiol. 2007, 116, 408–409. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Zhu, R.; Xu, Z.; Wu, J.; Wang, X.; Li, K.; Wen, L.; Yang, H.; Su, H. Impact of temperature variation between adjacent days on childhood hand, foot and mouth disease during April and July in urban and rural Hefei, China. Int. J. Biometeorol. 2015, 60, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Zhang, Y.; Xu, Y.; Xu, X.; Liu, T.; Luo, Y.; Xiao, J.; Wu, W.; Ma, W. Temperature Changes between Neighboring Days and Mortality in Summer: A Distributed Lag Non-Linear Time Series Analysis. PLoS ONE 2013, 8, e66403. [Google Scholar] [CrossRef] [PubMed]
- Fan, P.; Chen, J.; John, R. Urbanization and environmental change during the economic transition on the Mongolian Plateau: Hohhot and Ulaanbaatar. Environ. Res. 2015, 144, 96–112. [Google Scholar] [CrossRef] [Green Version]
- Fan, P.; Qi, J. Assessing the sustainability of major cities in China. Sustain. Sci. 2009, 5, 51–68. [Google Scholar] [CrossRef]
- Han, L.; Zhou, W.; Li, W.; Li, L. Impact of urbanization level on urban air quality: A case of fine particles (PM2.5) in Chinese cities. Environ. Pollut. 2014, 194, 163–170. [Google Scholar] [CrossRef]
- Forouzanfar, M.H.; Alexander, L.; Anderson, H.R.; Bachman, V.F.; Biryukov, S.; Brauer, M.; Burnett, R.; Casey, D.; Coates, M.M.; Cohen, A.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 2287–2323. [Google Scholar] [CrossRef] [Green Version]
- Dockery, D.; Pope, C. An Association Between Air Pollution and Mortality in Six US Cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [Green Version]
- Lelieveld, J.; Evans, J.; Fnais, M.; Giannadaki, D.; Pozzer, A. The contribution of outdoor air pollution sources to premature mortality on a global scale. Nature 2015, 525, 367–371. [Google Scholar] [CrossRef]
- Nel, A. Corrections and Clarifications: Air Pollution-Related Illness: Effects of Particles. Science 2005, 309, 1326. [Google Scholar]
- McDonnell, W.F.; Horstman, D.H.; Hazucha, M.J.; Seal, E.; Haak, E.D.; Salaam, S.A.; House, D.E. Pulmonary effects of ozone exposure during exercise: Dose-response characteristics. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 1983, 54, 1345. [Google Scholar] [CrossRef] [PubMed]
- Kulle, T.; Sauder, L.; Hebel, J.; Chatham, M. Ozone Response Relationships in Healthy Nonsmokers. Am. Rev. Respir. Dis. 1985, 132, 36–41. [Google Scholar] [PubMed]
- Kinney, P.L.; Raizenne, T.M. The effects of ambient ozone on lung function in children: A reanalysis of six summer camp studies. Environ. Health Perspect. 1996, 104, 170–174. [Google Scholar] [PubMed] [Green Version]
- Peters, J.; Avol, E.; Gauderman, W.J.; Linn, W.; Thomas, D. A Study of Twelve Southern California Communities with Differing Levels and Types of Air Pollution: II. Effects on Pulmonary Function. Am. J. Respir. Crit. Care Med. 1999, 159, 768–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Y.C.; Lee, J.T.; Kim, H.; Ha, E.H.; Schwartz, J.; Christiani, D.C. Effects of air pollutants on acute stroke mortality. Environ. Health Perspect. 2002, 110, 187–191. [Google Scholar] [CrossRef]
- Chiu, H.-F.; Cheng, M.-H.; Tsai, S.-S.; Wu, T.-N.; Kuo, H.-W.; Yang, C.-Y. Outdoor Air Pollution and Female Lung Cancer in Taiwan. Inhal. Toxicol. 2006, 18, 1025–1031. [Google Scholar] [CrossRef]
- Liu, C.-C.; Chen, C.-C.; Wu, T.-N.; Yang, C.-Y. Association of Brain Cancer with Residential Exposure to Petrochemical Air Pollution in Taiwan. J. Toxicol. Environ. Health Part A 2008, 71, 310–314. [Google Scholar] [CrossRef]
- Tsai, S.-S.; Tiao, M.-M.; Kuo, H.-W.; Wu, T.-N.; Yang, C.-Y. Association of Bladder Cancer with Residential Exposure to Petrochemical Air Pollutant Emissions in Taiwan. J. Toxicol. Environ. Health Part A 2008, 72, 53–59. [Google Scholar] [CrossRef]
- Chiu, H.-F.; Tsai, S.-S.; Chen, P.-S.; Liao, Y.-H.; Liou, S.-H.; Wu, T.-N.; Yang, C.-Y. Traffic Air Pollution and Risk of Death from Gastric Cancer in Taiwan: Petrol Station Density as an Indicator of Air Pollutant Exposure. J. Toxicol. Environ. Health Part A 2011, 74, 1215–1224. [Google Scholar] [CrossRef]
- Hung, L.-J.; Tsai, S.-S.; Chen, P.-S.; Yang, Y.-H.; Liou, S.-H.; Wu, T.-N.; Yang, C.-Y. Traffic Air Pollution and Risk of Death from Breast Cancer in Taiwan: Fine Particulate Matter (PM2.5) as a Proxy Marker. Aerosol Air Qual. Res. 2011, 12, 275–282. [Google Scholar] [CrossRef] [Green Version]
- Rajagopalan, S.; Brook, R.D. Air Pollution and Type 2 Diabetes: Mechanistic Insights. Diabetes 2012, 61, 3037–3045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szopińska, K.; Cienciała, A.; Bieda, A.; Kwiecień, J.; Kulesza, Ł.; Parzych, P. Verification of the Perception of the Local Community concerning Air Quality Using ADMS-Roads Modeling. Int. J. Environ. Res. Public Health 2022, 19, 10908. [Google Scholar] [CrossRef] [PubMed]
- Turner, B.; Kasperson, R.E.; Matson, P.A.; McCarthy, J.J.; Schiller, A. A framework for vulnerability analysis in sustainability science. Proc. Natl. Acad. Sci. USA 2003, 100, 8074–8079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Füssel, H.M. Vulnerability: A generally applicable conceptual framework for climate change research. Glob. Environ. Chang. 2007, 17, 155–167. [Google Scholar] [CrossRef]
- Wang, Y.; Tian, S.; Zhao, Q.P.; Li, X.D. Adaptability of high temperature heat wave disaster based on vulnerability: A review of recent studies. J. Environ. Health 2017, 34, 278–281. [Google Scholar]
- Shiff, S.; Helman, D.; Lensky, I.M. Worldwide continuous gap-filled MODIS land surface temperature dataset. Sci. Data 2021, 74, 8. [Google Scholar] [CrossRef]
- Tian, H.; Zhou, Y.; Wang, Z.; Huang, X.; Ge, E.; Wu, S.; Wang, P.; Tong, X.; Ran, P.; Luo, M. Effects of high-frequency temperature variabilities on the morbidity of chronic obstructive pulmonary disease: Evidence in 21 cities of Guangdong, South China. Environ. Res. 2021, 201, 111544. [Google Scholar] [CrossRef]
- Wei, J.; Li, Z.; Lyapustin, A.; Sun, L.; Peng, Y.; Xue, W.; Su, T.; Cribb, M. Reconstructing 1-km-resolution high-quality PM2.5 data records from 2000 to 2018 in China: Spatiotemporal variations and policy implications. Remote Sens. Environ. 2021, 252, 112136. [Google Scholar] [CrossRef]
- Wei, J.; Li, Z.; Cribb, M.; Huang, W.; Xue, W.; Sun, L.; Guo, J.; Peng, Y.; Li, J.; Lyapustin, A.; et al. Improved 1 km resolution PM2.5 estimates across China using enhanced space-time extremely randomized trees. Atmos. Chem. Phys. 2020, 20, 3273–3289. [Google Scholar] [CrossRef] [Green Version]
- Wei, J.; Li, Z.; Xue, W.; Sun, L.; Cribb, M. The ChinaHighPM10 dataset: Generation, validation, and spatiotemporal variations from 2015 to 2019 across China. Environ. Int. 2021, 146, 106290. [Google Scholar] [CrossRef]
- Song, Y.; Wang, J.; Ge, Y.; Xu, C. An optimal parameters-based geographical detector model enhances geographic characteristics of explanatory variables for spatial heterogeneity analysis: Cases with different types of spatial data. GISci. Remote Sens. 2020, 57, 593–610. [Google Scholar] [CrossRef]
- de Keijzer, C.; Agis, D.; Ambrós, A.; Arévalo, G.; Baldasano, J.M.; Bande, S.; Barrera-Gómez, J.; Benach, J.; Cirach, M.; Dadvand, P.; et al. The association of air pollution and greenness with mortality and life expectancy in Spain: A small-area study. Environ. Int. 2017, 99, 170–176. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Aunan, K.; Martin Seip, H.; Larssen, S.; Liu, J.; Zhang, D. The assessment of health damage caused by air pollution and its implication for policy making in Taiyuan, Shanxi, China. Energy Policy 2010, 38, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Cipriano, B.; Moresco, D.-O.; Martins, L.; Braga, A. Poluição atmosférica e doenças respiratórias em crianças na cidade de Curitiba, PR. Rev. Saúde Pública 2004, 38, 695–700. [Google Scholar]
- Tao, Y.; Mi, S.; Zhou, S.; Wang, S.; Xie, X. Air pollution and hospital admissions for respiratory diseases in Lanzhou, China. Environ. Pollut. 2013, 185, 196–201. [Google Scholar] [CrossRef]
- An, X.; Yan, T.; Mi, S.; Sun, Z.; Hou, Q. Association between PM10 and Respiratory Hospital Admissions in Different Seasons in Heavily Polluted Lanzhou City. J. Environ. Health 2015, 77, 64–71. [Google Scholar]
- Peng, R.D.; Chang, H.H.; Bell, M.L.; McDermott, A.; Zeger, S.L.; Samet, J.M.; Dominici, F. Coarse Particulate Matter Air Pollution and Hospital Admissions for Cardiovascular and Respiratory Diseases Among Medicare Patients. JAMA 2008, 299, 2172–2179. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Dong, G.-H.; Sun, B.; Zhang, L.; Chen, X.; Ma, N.; Yu, F.; Guo, H.; Huang, H.; Lee, Y.; et al. Long-Term Exposure to Ambient Air Pollution and Mortality due to Cardiovascular Disease and Cerebrovascular Disease in Shenyang, China. PLoS ONE 2011, 6, e20827. [Google Scholar] [CrossRef]
- Wang, Y.S.; Yao, L.; Wang, L.L.; Liu, Z.R.; Ji, D.S.; Tang, G.Q.; Zhang, J.K.; Sun, Y.; Hu, B.; Xin, J.Y. Mechanism for the formation of the January 2013 heavy haze pollution episode over central and eastern China. Sci. China Earth Sci. 2014, 57, 14–25. [Google Scholar] [CrossRef]
- Guo, H.; Zhan, Q.; Ho, H.C.; Yao, F.; Li, W. Coupling mobile phone data with machine learning: How misclassification errors in ambient PM2.5 exposure estimates are produced? Sci. Total Environ. 2020, 745, 141034. [Google Scholar] [CrossRef]
- González-Martín, J.; Kraakman, N.; Pérez, C.; Lebrero, R.; Muoz, R. A state–of–the-art review on indoor air pollution and strategies for indoor air pollution control. Chemosphere 2021, 262, 128376. [Google Scholar] [CrossRef]
- Zhang, T.; Xu, W.; Lin, X.; Yan, H.; Ma, M.; He, Z. Assessment of heavy metals pollution of soybean grains in North Anhui of China. Sci. Total Environ. 2018, 646, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Wu, Q.; Hu, W.; Huang, B.; Dong, L.; Liu, G. Using multi-medium factors analysis to assess heavy metal health risks along the Yangtze River in Nanjing, Southeast China. Environ. Pollut. 2018, 243, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Liao, Y.; Shou, L. Concentration and potential health risk of heavy metals in seafoods collected from Sanmen Bay and its adjacent areas, China. Mar. Pollut. Bull. 2018, 131, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wu, J.; Yu, B.; Dong, K.F.; Ma, D.; Xiao, G.; Zhang, C. Heavy metals in aquatic products and the health risk assessment to population in China. Environ. Sci. Pollut. Res. 2020, 27, 22708–22719. [Google Scholar] [CrossRef] [PubMed]
- Etemadi, A.; Sinha, R.; Ward, M.H. Mortality from different causes associated with meat, haem iron, nitrates, and nitrites in the NIH-AARP Diet and Health Study. BMJ Br. Med. J. 2017, 357, j1957. [Google Scholar] [CrossRef] [Green Version]
- van den Brandt, P.A. Red meat, processed meat, and other dietary protein sources and risk of overall and cause-specific mortality in the Netherlands Cohort Study. Eur. J. Epidemiol. 2019, 34, 351–369. [Google Scholar] [CrossRef] [Green Version]
- Ruggiero, E.; Castelnuovo, A.D.; Costanzo, S.; Persichillo, M.; Bonaccio, M. Egg consumption and risk of all-cause and cause-specific mortality in an Italian adult population. Eur. J. Nutr. 2021, 60, 3691–3702. [Google Scholar] [CrossRef]
- Richman, E.L.; Kenfield, S.A.; Stampfer, M.J.; Giovannucci, E.L.; Chan, J.M. Egg, Red Meat, and Poultry Intake and Risk of Lethal Prostate Cancer in the Prostate-Specific Antigen-Era: Incidence and Survival. Cancer Prev. Res. 2011, 4, 2110–2121. [Google Scholar] [CrossRef] [Green Version]
- Tan, M.; He, F.J.; Wang, C.; Macgregor, G.A. Twenty-Four-Hour Urinary Sodium and Potassium Excretion in China: A Systematic Review and Meta-Analysis. J. Hypertens. 2019, 37, e12. [Google Scholar] [CrossRef]
- Mueller, N.; Rojas-Rueda, D.; Basagaña, X.; Cirach, M.; Cole-Hunter, T.; Dadvand, P.; Donaire-Gonzalez, D.; Foraster, M.; Gascon, M.; Martinez, D.; et al. Health impacts related to urban and transport planning: A burden of disease assessment. Environ. Int. 2017, 107, 243–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondo, T.; Nakano, Y.; Adachi, S.; Murohara, T. Effects of Tobacco Smoking on Cardiovascular Disease. Circ. J. 2019, 83, 1980–1985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rehm, J.; Gmel, G.E.; Gmel, G.; Hasan, O.; Imtiaz, S.; Popova, S.; Probst, C.; Roerecke, M.; Room, R.; Samokhvalov, A.V. The relationship between different dimensions of alcohol use and the burden of disease-an update. Addiction 2017, 112, 968–1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator Dimensions | Indicator Meaning | Indicator Representation |
|---|---|---|
| Exposure (36) | nth percentile of daily average temperature (population weighted) | WLST_nth (n = 1,3,10,25,50,75,90,97,99) |
| Daily temperature standard deviation (population weighted) | WTSD | |
| Daily temperature difference nth percentile (population weighted) | WDTD_nth (n = 10,25,50,75,90) | |
| Intraday–interday temperature variability nth percentile (population weighted) | WIITV_nth (n = 10,25,50,75,90) | |
| Annual average concentration (population weighted) | WPM25_YM, WPM10_YM | |
| Days when the concentrations did not reach the guideline values for the three transitional periods formulated by WHO (population weighted) | WPM25_ITn (n = 1,2,3) WPM10_ITn (n = 1,2,3) | |
| Annual average concentration | SO2_YM | |
| Annual average concentration | NO2_YM | |
| Annual average 24-h mean 95th percentile concentration | CO_YM | |
| Annual average daily maximum 8 h moving average 90th percentile concentration | O3_YM | |
| Percentage of days with AQI not in good condition in a year | AQI | |
| Annual average relative humidity, wind speed, and surface pressure (population weighted) | WRH, WSP, WWS10 m | |
| Sensitivity (24) | Proportion of population aged 0–4, 5–14, 15–19, 20–39, 40–59, 60–79 and over 80 | Age_0_4, Age_5_14, Age_15_19, Age_20_39, Age_40_59, Age_60_79, Age_80 |
| Male/female sex ratio | MF_Ratio | |
| Percentage of population with less than high school education | BHigh_Ratio | |
| Proportion of population in the primary, secondary, tertiary industry | PriInd_Ratio, SecInd_Ratio, TerInd_Ratio | |
| Unemployment rate | Unemp_Rate | |
| Per capita road area | Road_PC | |
| Proportion of residential, industrial land | Res_Ratio, Ind_Ratio | |
| Per capita edible oil, vegetable, red meat, fruit, edible sugar, aquatic products, egg, milk consumption | Oil, Veg, Meat, Fruit, Sugar, AquaProducts, Egg, Milk | |
| Adaptability (15) | GDP per capita | GDP_PC |
| Proportion of people participating in basic medical insurance | BMI_Rate | |
| Per capita disposable income of urban/rural residents | PDI_Urban, PDI_Rural | |
| Number of health technicians per thousand people | NHT_PTP | |
| Number of beds in health institutions per thousand people | NB_PTP | |
| General public budget expenditure | GPBE | |
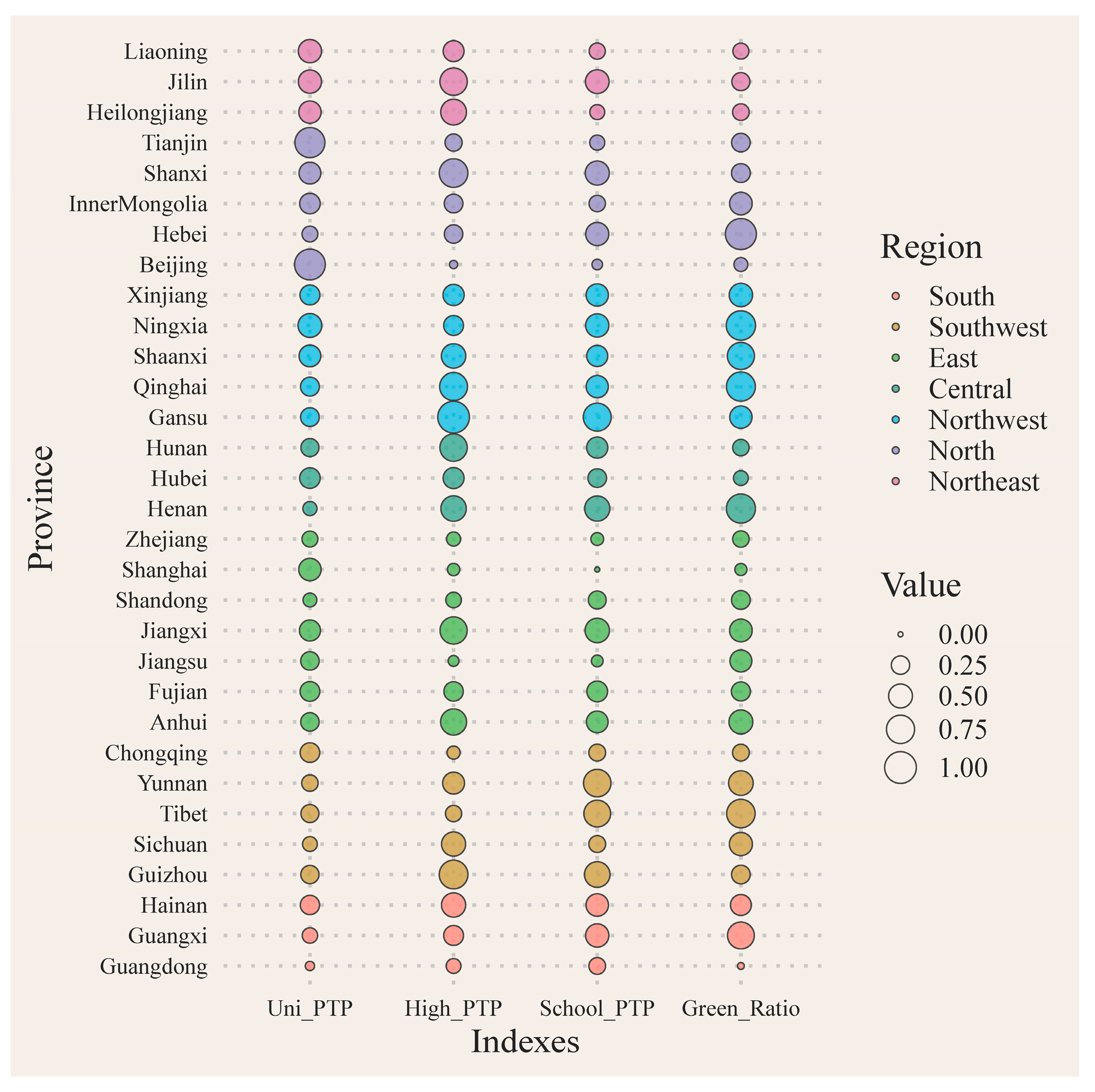
| Number of general institutions of higher learning/high schools/all schools per thousand people | Uni_PTP, High_PTP, School_PTP | |
| Per capita park area | ParkArea_PC | |
| Proportion of green space | Green_Ratio | |
| The number of attractions/supermarkets and markets/sports venues per 100,000 people | Attractions_Ratio FreshFood_Ratio Sport_Ratio |
| Quantile Regression | FAHP | Entropy Weight | |
|---|---|---|---|
| Respiratory diseases | 0.78 | 0.55 | 0.30 |
| Heart diseases | 0.65 | 0.57 | 0.28 |
| Cerebrovascular diseases | 0.58 | 0.58 | 0.41 |
| Malignant tumors | 0.73 | 0.72 | 0.42 |
| Endocrine nutrition metabolic diseases | 0.68 | 0.62 | 0.03 |
| Digestive system diseases | 0.66 | 0.44 | 0.51 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, Z.; Cao, C.; Xu, M.; Yang, X. Impact of Environmental Exposure on Chronic Diseases in China and Assessment of Population Health Vulnerability. ISPRS Int. J. Geo-Inf. 2023, 12, 155. https://doi.org/10.3390/ijgi12040155
Huang Z, Cao C, Xu M, Yang X. Impact of Environmental Exposure on Chronic Diseases in China and Assessment of Population Health Vulnerability. ISPRS International Journal of Geo-Information. 2023; 12(4):155. https://doi.org/10.3390/ijgi12040155
Chicago/Turabian StyleHuang, Zhibin, Chunxiang Cao, Min Xu, and Xinwei Yang. 2023. "Impact of Environmental Exposure on Chronic Diseases in China and Assessment of Population Health Vulnerability" ISPRS International Journal of Geo-Information 12, no. 4: 155. https://doi.org/10.3390/ijgi12040155