
Relationship among Body Composition, Adipocytokines, and Irisin on Exercise Capacity and Quality of Life in COPD: A Pilot Study
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
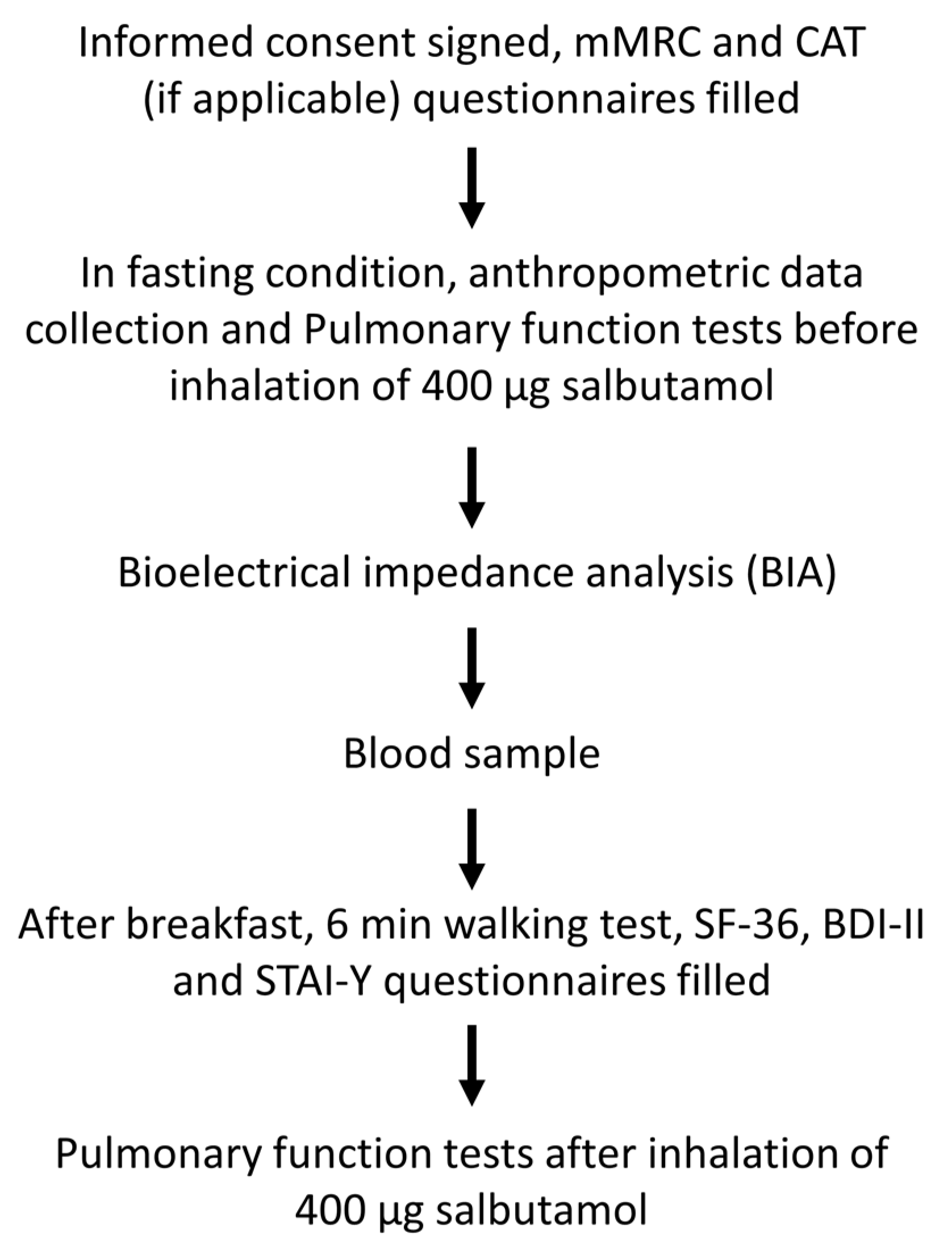
2.1. Study Design and Subjects Enrolled
2.2. Bioelectrical Impedance Analysis (BIA)
2.3. Respiratory Functions and Walking Test
2.4. SF-36, mMRC, CAT, BDI–II, and the STAI-Y Questionnaires
2.5. Adipocytokines, Irisin, and Intestinal Fatty Acid Binding Protein Measurement
2.6. Statistical Analysis
3. Results
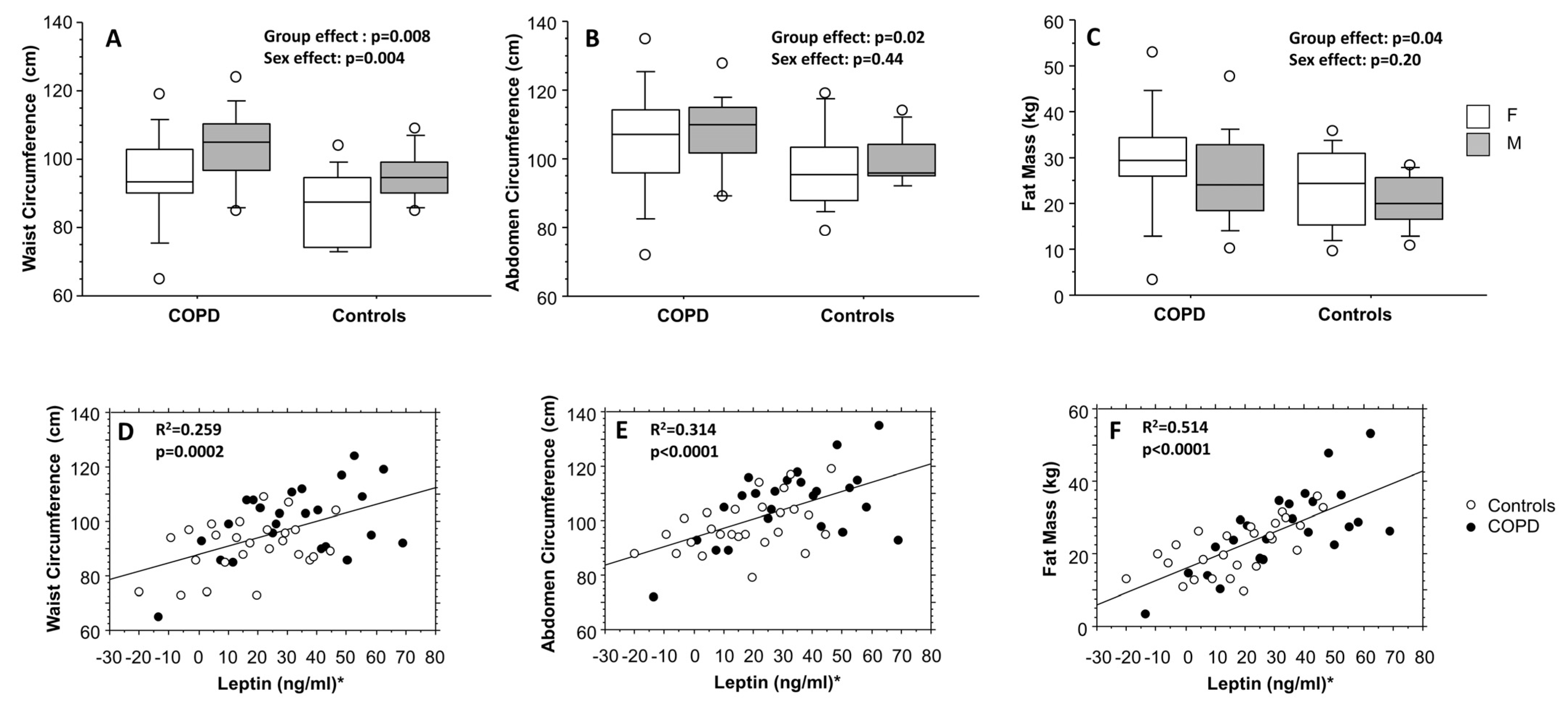
3.1. Anthropometric and Functional Data
3.2. Data from Questionnaires
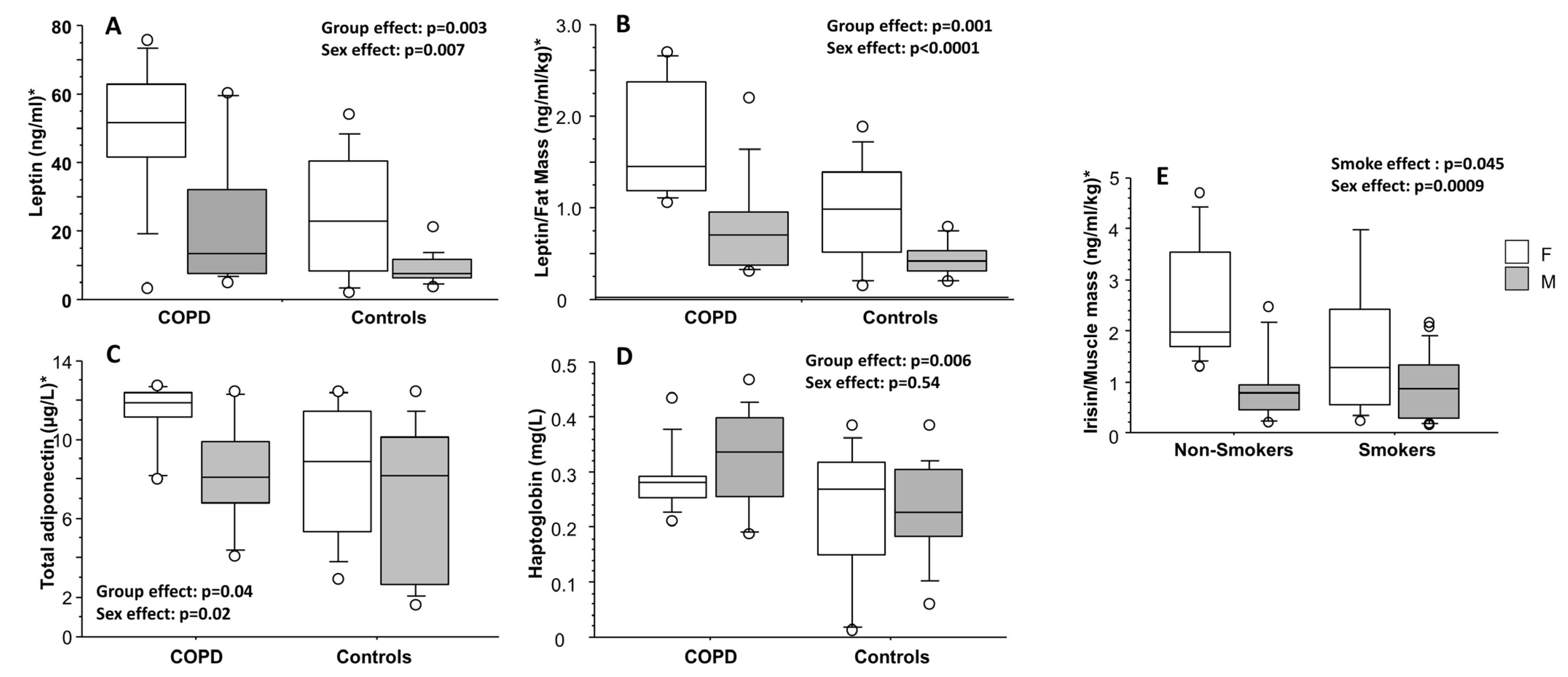
3.3. Adipocytokines, Irisin, and I-FABP Evaluations
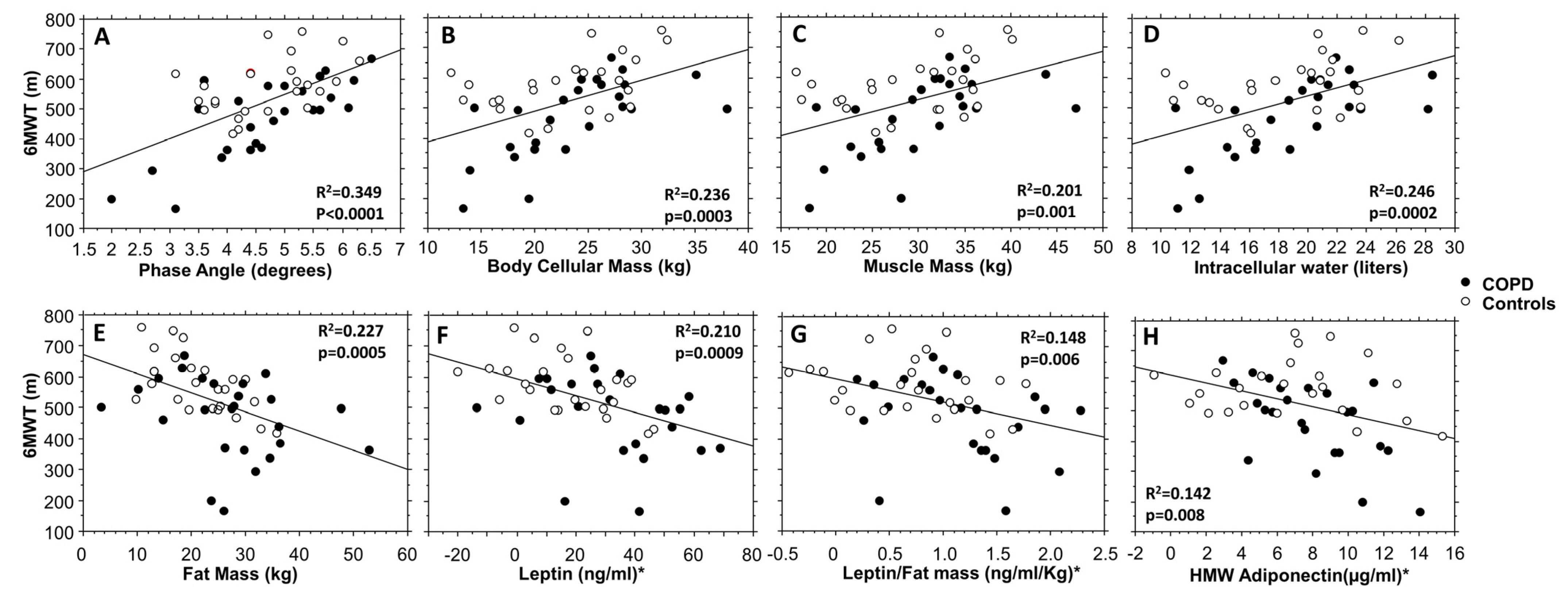
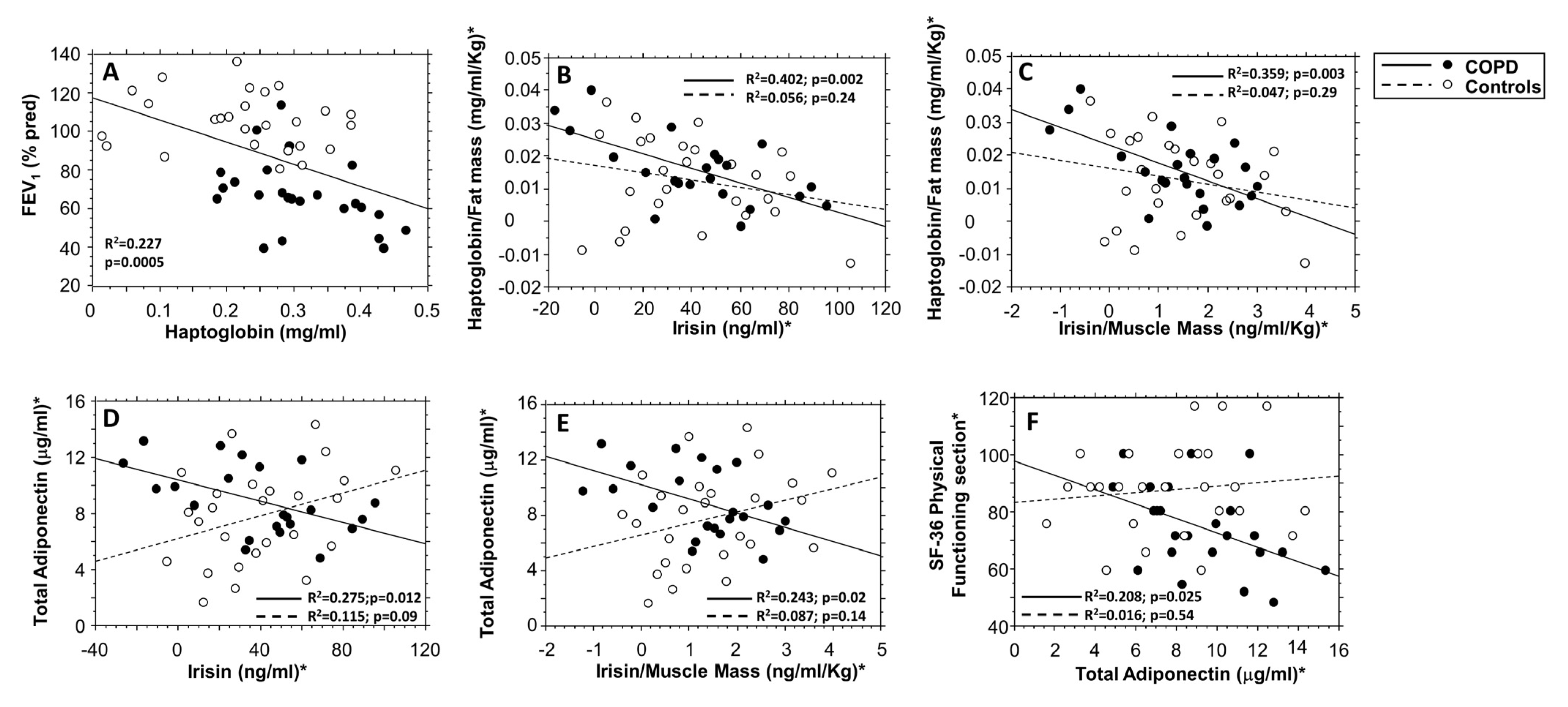
3.4. Correlation Data among the Evaluated Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kershaw, E.E.; Flier, J.S. Adipose Tissue as an Endocrine Organ. J. Clin. Endocrinol. Metab. 2004, 89, 2548–2556. [Google Scholar] [CrossRef] [PubMed]
- Khudiakova, A.D.; Polonskaya, Y.V.; Shramko, V.S.; Shcherbakova, L.V.; Striukova, E.V.; Kashtanova, E.V.; Ragino, Y.I. Blood Adipokines/Cytokines in Young People with Chronic Bronchitis and Abdominal Obesity. Biomolecules 2022, 12, 1502. [Google Scholar] [CrossRef] [PubMed]
- Blanco, I.; Diego, I.; Bueno, P.; Casas-Maldonado, F.; Miravitlles, M. Geographic Distribution of COPD Prevalence in the World Displayed by Geographic Information System Maps. Eur. Respir. J. 2019, 54, 1900610. [Google Scholar] [CrossRef] [PubMed]
- Bennett, J.E.; Kontis, V.; Mathers, C.D.; Guillot, M.; Rehm, J.; Chalkidou, K.; Ezzati, M. NCD Countdown 2030: Pathways to Achieving Sustainable Development Goal Target 3.4. Lancet 2020, 396, 918–934. [Google Scholar] [CrossRef] [PubMed]
- Goërtz, Y.M.J.; Looijmans, M.; Prins, J.B.; Janssen, D.J.A.; Thong, M.S.Y.; Peters, J.B.; Burtin, C.; Meertens-Kerris, Y.; Coors, A.; Muris, J.W.M.; et al. Fatigue in Patients with Chronic Obstructive Pulmonary Disease: Protocol of the Dutch Multicentre, Longitudinal, Observational FAntasTIGUE Study. BMJ Open 2018, 8, e021745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanania, N.A.; Müllerova, H.; Locantore, N.W.; Vestbo, J.; Watkins, M.L.; Wouters, E.F.M.; Rennard, S.I.; Sharafkhaneh, A. Determinants of Depression in the ECLIPSE Chronic Obstructive Pulmonary Disease Cohort. Am. J. Respir. Crit. Care Med. 2011, 183, 604–611. [Google Scholar] [CrossRef]
- Blakemore, A.; Dickens, C.; Chew-Graham, C.A.; Afzal, C.W.; Tomenson, B.; Coventry, P.A.; Guthrie, E. Depression Predicts Emergency Care Use in People with Chronic Obstructive Pulmonary Disease: A Large Cohort Study in Primary Care. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 1343–1353. [Google Scholar] [CrossRef] [Green Version]
- Agusti, A.; Soriano, J.B. COPD as a Systemic Disease. Chronic Obstr. Pulm. Dis. COPD 2008, 5, 133–138. [Google Scholar] [CrossRef]
- Barnes, P.J.; Celli, B.R. Systemic Manifestations and Comorbidities of COPD. Eur. Respir. J. 2009, 33, 1165–1185. [Google Scholar] [CrossRef] [Green Version]
- Karanikas, I.; Karayiannis, D.; Karachaliou, A.; Papanikolaou, A.; Chourdakis, M.; Kakavas, S. Body Composition Parameters and Functional Status Test in Predicting Future Acute Exacerbation Risk among Hospitalized Patients with Chronic Obstructive Pulmonary Disease. Clin. Nutr. Edinb. Scotl. 2021, 40, 5605–5614. [Google Scholar] [CrossRef]
- Takabatake, N.; Nakamura, H.; Abe, S.; Hino, T.; Saito, H.; Yuki, H.; Kato, S.; Tomoike, H. Circulating Leptin in Patients with Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 1999, 159, 1215–1219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancuso, P. Obesity and Lung Inflammation. J. Appl. Physiol. 2010, 108, 722–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lisi, S.; Gamucci, O.; Vottari, T.; Scabia, G.; Funicello, M.; Marchi, M.; Galli, G.; Arisi, I.; Brandi, R.; D’Onofrio, M.; et al. Obesity-Associated Hepatosteatosis and Impairment of Glucose Homeostasis Are Attenuated by Haptoglobin Deficiency. Diabetes 2011, 60, 2496–2505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Pérez, A.; Vilariño-García, T.; Fernández-Riejos, P.; Martín-González, J.; Segura-Egea, J.J.; Sánchez-Margalet, V. Role of Leptin as a Link between Metabolism and the Immune System. Cytokine Growth Factor Rev. 2017, 35, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Conus, S.; Bruno, A.; Simon, H.-U. Leptin Is an Eosinophil Survival Factor. J. Allergy Clin. Immunol. 2005, 116, 1228–1234. [Google Scholar] [CrossRef]
- Bruno, A.; Conus, S.; Schmid, I.; Simon, H.-U. Apoptotic Pathways Are Inhibited by Leptin Receptor Activation in Neutrophils. J. Immunol. 2005, 174, 8090–8096. [Google Scholar] [CrossRef] [Green Version]
- Bruno, A.; Pace, E.; Chanez, P.; Gras, D.; Vachier, I.; Chiappara, G.; La Guardia, M.; Gerbino, S.; Profita, M.; Gjomarkaj, M. Leptin and Leptin Receptor Expression in Asthma. J. Allergy Clin. Immunol. 2009, 124, 230–237.e4. [Google Scholar] [CrossRef]
- Guo, Z.; Yang, H.; Zhang, J.-R.; Zeng, W.; Hu, X. Leptin Receptor Signaling Sustains Metabolic Fitness of Alveolar Macrophages to Attenuate Pulmonary Inflammation. Sci. Adv. 2022, 8, eabo3064. [Google Scholar] [CrossRef]
- Bruno, A.; Chanez, P.; Chiappara, G.; Siena, L.; Giammanco, S.; Gjomarkaj, M.; Bonsignore, G.; Bousquet, J.; Vignola, A.M. Does Leptin Play a Cytokine-like Role within the Airways of COPD Patients? Eur. Respir. J. 2005, 26, 398–405. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, K.; Suzukawa, M.; Arakawa, S.; Kobayashi, K.; Igarashi, S.; Tashimo, H.; Nagai, H.; Tohma, S.; Nagase, T.; Ohta, K. Leptin Enhances Cytokine/Chemokine Production by Normal Lung Fibroblasts by Binding to Leptin Receptor. Allergol. Int. Off. J. Jpn. Soc. Allergol. 2019, 68S, S3–S8. [Google Scholar] [CrossRef]
- Vernooy, J.H.J.; Drummen, N.E.A.; van Suylen, R.J.; Cloots, R.H.E.; Möller, G.M.; Bracke, K.R.; Zuyderduyn, S.; Dentener, M.A.; Brusselle, G.G.; Hiemstra, P.S.; et al. Enhanced Pulmonary Leptin Expression in Patients with Severe COPD and Asymptomatic Smokers. Thorax 2009, 64, 26–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, P.-S.; Lin, C.-M.; Chang, J.-F.; Wu, C.-S.; Sia, K.-C.; Lee, I.-T.; Huang, K.-Y.; Lin, W.-N. Participation of NADPH Oxidase-Related Reactive Oxygen Species in Leptin-Promoted Pulmonary Inflammation: Regulation of CPLA2α and COX-2 Expression. Int. J. Mol. Sci. 2019, 20, 1078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali Assad, N.; Sood, A. Leptin, Adiponectin and Pulmonary Diseases. Biochimie 2012, 94, 2180–2189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creutzberg, E.C.; Wouters, E.F.; Vanderhoven-Augustin, I.M.; Dentener, M.A.; Schols, A.M. Disturbances in Leptin Metabolism Are Related to Energy Imbalance during Acute Exacerbations of Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2000, 162, 1239–1245. [Google Scholar] [CrossRef]
- Miller, M.; Cho, J.Y.; Pham, A.; Ramsdell, J.; Broide, D.H. Adiponectin and Functional Adiponectin Receptor 1 Are Expressed by Airway Epithelial Cells in Chronic Obstructive Pulmonary Disease. J. Immunol. 2009, 182, 684–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaswal, S.; Saini, V.; Kaur, J.; Gupta, S.; Kaur, H.; Garg, K. Association of Adiponectin with Lung Function Impairment and Disease Severity in Chronic Obstructive Pulmonary Disease. Int. J. Appl. Basic Med. Res. 2018, 8, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.I.; Li, Y.; Man, S.F.P.; Tashkin, D.; Wise, R.A.; Connett, J.E.; Anthonisen, N.A.; Churg, A.; Wright, J.L.; Sin, D.D. The Complex Relationship of Serum Adiponectin to COPD Outcomes COPD and Adiponectin. Chest 2012, 142, 893–899. [Google Scholar] [CrossRef]
- Maffei, M.; Barone, I.; Scabia, G.; Santini, F. The Multifaceted Haptoglobin in the Context of Adipose Tissue and Metabolism. Endocr. Rev. 2016, 37, 403–416. [Google Scholar] [CrossRef] [Green Version]
- Torres, A.; Vivanco, S.; Lavín, F.; Pereda, C.; Chernobrovkin, A.; Gleisner, A.; Alcota, M.; Larrondo, M.; López, M.N.; Salazar-Onfray, F.; et al. Haptoglobin Induces a Specific Proteomic Profile and a Mature-Associated Phenotype on Primary Human Monocyte-Derived Dendritic Cells. Int. J. Mol. Sci. 2022, 23, 6882. [Google Scholar] [CrossRef]
- Lee, P.-L.; Lee, K.-Y.; Cheng, T.-M.; Chuang, H.-C.; Wu, S.-M.; Feng, P.-H.; Liu, W.-T.; Chen, K.-Y.; Ho, S.-C. Relationships of Haptoglobin Phenotypes with Systemic Inflammation and the Severity of Chronic Obstructive Pulmonary Disease. Sci. Rep. 2019, 9, 189. [Google Scholar] [CrossRef]
- Zhang, L.; Li, C.; Xiong, J.; Chang, C.; Sun, Y. Dysregulated Myokines and Signaling Pathways in Skeletal Muscle Dysfunction in a Cigarette Smoke-Induced Model of Chronic Obstructive Pulmonary Disease. Front. Physiol. 2022, 13, 929926. [Google Scholar] [CrossRef] [PubMed]
- Machado, F.V.C.; Schneider, L.P.; Fonseca, J.; Belo, L.F.; Bonomo, C.; Morita, A.A.; Furlanetto, K.C.; Felcar, J.M.; Rodrigues, A.; Franssen, F.M.E.; et al. Clinical Impact of Body Composition Phenotypes in Patients with COPD: A Retrospective Analysis. Eur. J. Clin. Nutr. 2019, 73, 1512–1519. [Google Scholar] [CrossRef] [PubMed]
- Degens, H.; Gayan-Ramirez, G.; van Hees, H.W.H. Smoking-Induced Skeletal Muscle Dysfunction: From Evidence to Mechanisms. Am. J. Respir. Crit. Care Med. 2015, 191, 620–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, A.M.W.; Magkos, F.; Atherton, P.; Selby, A.; Smith, K.; Rennie, M.J.; Pedersen, B.K.; Mittendorfer, B. Smoking Impairs Muscle Protein Synthesis and Increases the Expression of Myostatin and MAFbx in Muscle. Am. J. Physiol. Endocrinol. Metab. 2007, 293, E843–E848. [Google Scholar] [CrossRef] [Green Version]
- Kirschner, S.K.; Deutz, N.E.P.; Jonker, R.; Olde Damink, S.W.M.; Harrykissoon, R.I.; Zachria, A.J.; Dasarathy, S.; Engelen, M.P.K.J. Intestinal Function Is Impaired in Patients with Chronic Obstructive Pulmonary Disease. Clin. Nutr. Edinb. Scotl. 2021, 40, 2270–2277. [Google Scholar] [CrossRef]
- Rutten, E.P.A.; Lenaerts, K.; Buurman, W.A.; Wouters, E.F.M. Disturbed Intestinal Integrity in Patients with COPD: Effects of Activities of Daily Living. Chest 2014, 145, 245–252. [Google Scholar] [CrossRef]
- McKenna, Z.; Houck, J.; Ducharme, J.; Li, Z.; Berkemeier, Q.; Fennel, Z.; Wells, A.; Mermier, C.; Deyhle, M.; Laitano, O.; et al. The Effect of Prolonged Interval and Continuous Exercise in the Heat on Circulatory Markers of Intestinal Barrier Integrity. Eur. J. Appl. Physiol. 2022, 122, 2651–2659. [Google Scholar] [CrossRef]
- Bruno, A.; Uasuf, C.G.; Insalaco, G.; Barazzoni, R.; Ballacchino, A.; Gjomarkaj, M.; Pace, E. Nutritional Status and Physical Inactivity in Moderated Asthmatics: A Pilot Study. Medicine 2016, 95, e4485. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical Impedance Analysis—Part I: Review of Principles and Methods. Clin. Nutr. Edinb. Scotl. 2004, 23, 1226–1243. [Google Scholar] [CrossRef]
- Kyle, U.G.; Bosaeus, I.; De Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Manuel Gómez, J.; Lilienthal Heitmann, B.; Kent-Smith, L.; Melchior, J.-C.; Pirlich, M.; et al. Bioelectrical Impedance Analysis-Part II: Utilization in Clinical Practice. Clin. Nutr. Edinb. Scotl. 2004, 23, 1430–1453. [Google Scholar] [CrossRef]
- Zanella, P.B.; Àvila, C.C.; Chaves, F.C.; Gazzana, M.B.; Berton, D.C.; Knorst, M.M.; de Souza, C.G. Phase Angle Evaluation of Lung Disease Patients and Its Relationship with Nutritional and Functional Parameters. J. Am. Coll. Nutr. 2021, 40, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.; van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of Spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.M.; Zheng, J.; et al. Multi-Ethnic Reference Values for Spirometry for the 3-95-Yr Age Range: The Global Lung Function 2012 Equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef] [PubMed]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An Official European Respiratory Society/American Thoracic Society Technical Standard: Field Walking Tests in Chronic Respiratory Disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.C.; Jones, P.W. A Comparison of the Visual Analogue Scale and Modified Borg Scale for the Measurement of Dyspnoea during Exercise. Clin. Sci. 1989, 76, 277–282. [Google Scholar] [CrossRef] [Green Version]
- Apolone, G.; Mosconi, P. The Italian SF-36 Health Survey: Translation, Validation and Norming. J. Clin. Epidemiol. 1998, 51, 1025–1036. [Google Scholar] [CrossRef]
- Bestall, J.C.; Paul, E.A.; Garrod, R.; Garnham, R.; Jones, P.W.; Wedzicha, J.A. Usefulness of the Medical Research Council (MRC) Dyspnoea Scale as a Measure of Disability in Patients with Chronic Obstructive Pulmonary Disease. Thorax 1999, 54, 581–586. [Google Scholar] [CrossRef] [Green Version]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.-H.; Kline Leidy, N. Development and First Validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef] [Green Version]
- Sica, C.; Ghisi, M.; Altoè, G.; Chiri, L.R.; Franceschini, S.; Coradeschi, D.; Melli, G. The Italian Version of the Obsessive Compulsive Inventory: Its Psychometric Properties on Community and Clinical Samples. J. Anxiety Disord. 2009, 23, 204–211. [Google Scholar] [CrossRef]
- Di Sano, C.; Lazzara, V.; Durante, M.; D’Anna, C.; Bonura, A.; Dino, P.; Uasuf, C.G.; Pace, E.; Lenucci, M.S.; Bruno, A. The Protective Anticancer Effect of Natural Lycopene Supercritical CO(2) Watermelon Extracts in Adenocarcinoma Lung Cancer Cells. Antioxidants 2022, 11, 1150. [Google Scholar] [CrossRef]
- Cruz Rivera, P.N.; Goldstein, R.L.; Polak, M.; Lazzari, A.A.; Moy, M.L.; Wan, E.S. Performance of Bioelectrical Impedance Analysis Compared to Dual X-Ray Absorptiometry (DXA) in Veterans with COPD. Sci. Rep. 2022, 12, 1946. [Google Scholar] [CrossRef] [PubMed]
- Higham, A.; Baker, J.M.; Jackson, N.; Shah, R.; Lea, S.; Singh, D. Dysregulation of the CD163-Haptoglobin Axis in the Airways of COPD Patients. Cells 2021, 11, 2. [Google Scholar] [CrossRef]
- Arinc, S.; Agca, M.; Yaman, F. Evaluation of Nutritional Status in COPD According to the GOLD-2015 Staging System: A Prospective Observational Study. Eur. J. Clin. Nutr. 2020, 74, 1354–1361. [Google Scholar] [CrossRef] [PubMed]
- Boström, P.; Wu, J.; Jedrychowski, M.P.; Korde, A.; Ye, L.; Lo, J.C.; Rasbach, K.A.; Boström, E.A.; Choi, J.H.; Long, J.Z.; et al. A PGC1-α-Dependent Myokine That Drives Brown-Fat-like Development of White Fat and Thermogenesis. Nature 2012, 481, 463–468. [Google Scholar] [CrossRef] [Green Version]
- Liu, S.; Cui, F.; Ning, K.; Wang, Z.; Fu, P.; Wang, D.; Xu, H. Role of Irisin in Physiology and Pathology. Front. Endocrinol. 2022, 13, 962968. [Google Scholar] [CrossRef] [PubMed]
- Carolan, B.J.; Kim, Y.; Williams, A.A.; Kechris, K.; Lutz, S.; Reisdorph, N.; Bowler, R.P. The Association of Adiponectin with Computed Tomography Phenotypes in Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2013, 188, 561–566. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Han, J.M.; Kim, H.; Lee, K.-B.; Chung, W.; Kim, Y.-S.; Park, S.K.; Chae, D.W.; Ahn, C.; Oh, K.-H.; et al. Low Serum Adiponectin Level Is Associated with Better Physical Health-Related Quality of Life in Chronic Kidney Disease. Sci. Rep. 2021, 11, 10928. [Google Scholar] [CrossRef]
- Martins, A.D.; Oliveira, R.; Brito, J.P.; Costa, T.; Ramalho, F.; Pimenta, N.; Santos-Rocha, R. Phase Angle Cutoff Value as a Marker of the Health Status and Functional Capacity in Breast Cancer Survivors. Physiol. Behav. 2021, 235, 113400. [Google Scholar] [CrossRef]
- Matias, C.N.; Nunes, C.L.; Francisco, S.; Tomeleri, C.M.; Cyrino, E.S.; Sardinha, L.B.; Silva, A.M. Phase Angle Predicts Physical Function in Older Adults. Arch. Gerontol. Geriatr. 2020, 90, 104151. [Google Scholar] [CrossRef]
- Oliveira, R.; Leão, C.; Silva, A.F.; Clemente, F.M.; Santamarinha, C.T.; Nobari, H.; Brito, J.P. Comparisons between Bioelectrical Impedance Variables, Functional Tests and Blood Markers Based on BMI in Older Women and Their Association with Phase Angle. Int. J. Environ. Res. Public. Health 2022, 19, 6851. [Google Scholar] [CrossRef]
- Bering, T.; Diniz, K.G.D.; Coelho, M.P.P.; de Souza, A.C.M.; de Melo, L.F.; Vieira, D.A.; Soares, M.M.S.; Kakehasi, A.M.; Correia, M.I.T.D.; Teixeira, R.; et al. Bioelectrical Impedance Analysis-Derived Measurements in Chronic Hepatitis C: Clinical Relevance of Fat-Free Mass and Phase Angle Evaluation. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2018, 33, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Norman, K.; Stobäus, N.; Zocher, D.; Bosy-Westphal, A.; Szramek, A.; Scheufele, R.; Smoliner, C.; Pirlich, M. Cutoff Percentiles of Bioelectrical Phase Angle Predict Functionality, Quality of Life, and Mortality in Patients with Cancer. Am. J. Clin. Nutr. 2010, 92, 612–619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maddocks, M.; Kon, S.S.C.; Jones, S.E.; Canavan, J.L.; Nolan, C.M.; Higginson, I.J.; Gao, W.; Polkey, M.I.; Man, W.D.-C. Bioelectrical Impedance Phase Angle Relates to Function, Disease Severity and Prognosis in Stable Chronic Obstructive Pulmonary Disease. Clin. Nutr. Edinb. Scotl. 2015, 34, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Primo, D.; Izaola, O.; Gómez, J.J.L.; de Luis, D. Correlation of the Phase Angle with Muscle Ultrasound and Quality of Life in Obese Females. Dis. Markers 2022, 2022, 7165126. [Google Scholar] [CrossRef] [PubMed]
- Stridsman, C.; Skär, L.; Hedman, L.; Rönmark, E.; Lindberg, A. Fatigue Affects Health Status and Predicts Mortality Among Subjects with COPD: Report from the Population-Based OLIN COPD Study. Chronic Obstr. Pulm. Dis. COPD 2015, 12, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Leelarungrayub, J.; Puntumetakul, R.; Sriboonreung, T.; Pothasak, Y.; Klaphajone, J. Preliminary Study: Comparative Effects of Lung Volume Therapy between Slow and Fast Deep-Breathing Techniques on Pulmonary Function, Respiratory Muscle Strength, Oxidative Stress, Cytokines, 6-Minute Walking Distance, and Quality of Life in Persons with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 3909–3921. [Google Scholar] [CrossRef] [Green Version]
- Leivo-Korpela, S.; Lehtimäki, L.; Vuolteenaho, K.; Nieminen, R.; Kööbi, L.; Järvenpää, R.; Kankaanranta, H.; Saarelainen, S.; Moilanen, E. Adiponectin Is Associated with Dynamic Hyperinflation and a Favourable Response to Inhaled Glucocorticoids in Patients with COPD. Respir. Med. 2014, 108, 122–128. [Google Scholar] [CrossRef] [Green Version]
- Perna, S.; Gasparri, C.; Ferraris, C.; Barrile, G.C.; Cavioni, A.; Mansueto, F.; Patelli, Z.; Peroni, G.; Tartara, A.; Zese, M.; et al. Validation of the Italian Version of the SARC-F Questionnaire to Assess Sarcopenia in Older Adults. Nutrients 2022, 14, 2533. [Google Scholar] [CrossRef]
- Planella-Farrugia, C.; Comas, F.; Sabater-Masdeu, M.; Moreno, M.; Moreno-Navarrete, J.M.; Rovira, O.; Ricart, W.; Fernández-Real, J.M. Circulating Irisin and Myostatin as Markers of Muscle Strength and Physical Condition in Elderly Subjects. Front. Physiol. 2019, 10, 871. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, J.M.; Orsso, C.E.; Nourouzpour, S.; Elangeswaran, B.; Chohan, K.; Orchanian-Cheff, A.; Fidler, L.; Mathur, S.; Rozenberg, D. Computed Tomography-Based Body Composition Measures in COPD and Their Association with Clinical Outcomes: A Systematic Review. Chron. Respir. Dis. 2022, 19, 14799731221133388. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| GROUPS | p Value | ||
|---|---|---|---|
| COPD (No. = 25) | Controls (No. = 26) | ||
| Anthropometric | |||
| Sex (No., F/M) | 10/15 | 12/14 | 0.66 # |
| Age (years, mean ± SD) | 68.7 ± 8.6 | 66.5 ± 8.2 | 0.34 § |
| Weight (kg, mean ± SD) | 78.6 ± 17.0 | 72.2 ± 12.1 | 0.13 § |
| BMI (kg/m2, mean ± SD) | 29.8 ± 5.6 | 27.5 ± 3.9 | 0.09 § |
| Waist circumference (cm, mean ± SD) | 100.0 ± 12.8 | 91.0 ± 9.8 | 0.007 § |
| Abdomen circumference (cm, mean ± SD) | 106.6 ± 13.3 | 98.5 ± 9.7 | 0.017 § |
| Hip circumference (cm, mean ± SD) | 107.4 ± 15.3 | 102.7 ± 8.4 | 0.18 § |
| Wrist circumference (cm, mean ± SD) | 17.1 ± 1.4 | 16.5 ± 1.5 | 0.25 § |
| Smokers (No., current/former/never) | 4/17/4 | 3/9/14 | 0.02 # |
| Functional | |||
| FVC (% predicted, mean ± SD) | 88.2 ± 16.2 | 103.5 ± 10.0 | 0.0002 § |
| FEV1 (% predicted, mean ± SD) | 66.9 ± 18.0 | 105.4 ± 14.6 | <0.0001 § |
| FEV1/FVC (%, mean ± SD) | 58.6 ± 10.4 | 78.9 ± 8.3 | <0.0001 § |
| FEF25–75% (% predicted, mean ± SD) | 41.1 ± 35.3 | 122.9 ± 54.8 | <0.0001 § |
| 6 min walking test (m, mean ± SD) | 470 ± 132 | 577 ± 93 | 0.002 § |
| Comorbidities | |||
| Diabetes (No., %) | 3 (12%) | 2 (8%) | 0.61 # |
| Systemic hypertension (No., %) | 22 (88%) | 13 (50%) | 0.004 # |
| Dyslipidemia (No., %) | 8 (32%) | 10 (38%) | 0.63 # |
| Bioelectrical impedance analysis | |||
| Phase angle (degrees, mean ± SD) | 4.7 ± 1.1 | 4.7 ± 0.8 | 0.94 § |
| Total body water (liters, mean ± SD) | 40.8 ± 7.3 | 39.5 ± 7.4 | 0.54 § |
| Extracellular water (liters, median and IQR range) | 20.4 (18.6–24.2) | 20.8 (18.2–23.1) | 0.72 ‡ |
| Intracellular water (liters, mean ± SD) | 18.9 ± 4.8 | 18.7 ± 4.6 | 0.86 § |
| Fat-free mass (kg, mean ± SD) | 51.6 ± 9.5 | 50.5 ± 9.5 | 0.68 § |
| Body cellular mass (kg, mean ± SD) | 23.6 ± 6.1 | 23.4 ± 6.0 | 0.90 § |
| Body cellular mass index (BCM/height2, median and IQR range) | 8.9 ± 1.8 | 8.8 ± 1.6 | 0.88 § |
| Muscle mass (kg, mean ± SD) | 30.1 ± 7.1 | 29.7 ± 7.2 | 0.84 § |
| Fat mass (kg, mean ± SD) | 27.0 ± 10.9 | 21.8 ± 7.3 | 0.046 § |
| Questionnaires | |||
| SF-36 Physical Functioning section | 75.0 (68.8–86.3) | 90.0 (80.0–95.0) | 0.004 ‡ |
| mMRC (median and IQR range) | 1.0 (1.0–2.0) | 0.0 (0.0–1.0) | <0.0001 ‡ |
| CAT (mean ± SD) | 11.4 ± 3.8 | N/A | N/A |
| BDI–II (median and IQR range) | 9.0 (4.8–11.5) | 8.5 (6.0–12.0) | 0.96 ‡ |
| STAI-Y (mean ± SD) | 43.0 ± 9.3 | 43.0 ± 4.9 | 0.97 § |
| GROUPS | ||||||||
|---|---|---|---|---|---|---|---|---|
| COPD (No. = 25) | Controls (No. = 26) | |||||||
| Whole Subgroup | Females (No. = 10) | Males (No. = 15) | Whole Subgroup | Females (No.= 12) | Males (No. = 14) | p Value for Group Effect | p Value for Sex Effect | |
| Leptin (ng/mL, median and IQR range) | 34.0 (10.0–58.8) | 51.5 (41.8–63.0) | 13.4 (7.6–32.0) | 10.0 (6.2–21.0) | 23.1 (8.5–40.3) | 7.5 (6.2–11.7) | 0.003 | 0.007 |
| Leptin/fat mass (ng/mL/kg, median, and IQR range) | 1.07 (0.56–1.64) | 1.46 (1.18–2.37) | 0.78 (0.37–0.95) | 0.52 (0.34–0.84) | 0.98 (0.52–1.38) | 0.42 (0.31–0.53) | 0.001 | <0.0001 |
| Total adiponectin (µg/mL, median, and IQR range) | 8.8 (8.0–12.1) | 11.9 (11.2–12.4) | 8.1 (6.8–10.0) | 8.4 (4.2–11.1) | 8.9 (5.3–11.4) | 8.1 (2.610.2) | 0.04 | 0.02 |
| Total adiponectin/fat mass (µg/mL/kg, median, and IQR range) | 0.31 (0.23–0.50) | 0.37 (0.28–0.49) | 0.24 (0.23–0.50) | 0.40 (0.17–0.53) | 0.37 (0.19–0.45) | 0.42 (0.11–0.61) | 0.73 | 0.68 |
| Haptoglobin (mg/mL, mean ± SD) | 0.31 ± 0.08 | 0.28 ± 0.06 | 0.33 ± 0.09 | 0.23 ± 0.11 | 0.23 ± 0.13 | 0.22 ± 0.09 | 0.006 | 0.54 |
| Haptoglobin/fat mass (mg/mL/kg, median, and IQR range) | 0.011 (0.009–0.014) | 0.010 (0.007–0.012) | 0.011 (0.009–0.017) | 0.011 (0.008–0.015) | 0.010 (0.008–0.012) | 0.011 (0.008–0.015) | 0.77 | 0.09 |
| HMW adiponectin (µg/mL, median, and IQR range) | 7.38 (4.59–9.99) | 9.34 (7.52–12.82) | 6.11 (4.31–8.35) | 6.62 (2.74–9.45) | 7.09 (3.17–11.82) | 6.62 (2.42–8.66) | 0.13 | 0.07 |
| HMW adiponectin/fat mass (µg/mL/kg, median, and IQR range) | 0.22 (0.17–0.47) | 0.31 (0.21–0.50) | 0.21 (0.15–0.42) | 0.33 (0.11–0.47) | 0.32 0.16–0.40) | 0.37 (0.10–0.52) | 0.96 | 0.73 |
| Irisin (ng/mL, median, and IQR range) | 41.1 (12.7–50.3) | 40.7 (13.5–61.9) | 41.5 (12.8–50.6) | 28.5 (10.1–49.0) | 47.4 (22.6–81.9) | 15.9 (9.4–33.7) | 0.83 | 0.18 |
| Irisin/muscle mass (ng/mL/kg, median, and IQR range) | 1.22 (0.52–1.96) | 1.65 (0.54–2.42) | 1.07 (0.44–1.60) | 0.87 (0.36–1.88) | 1.89 (1.03–3.34) | 0.44 (0.28–0.93) | 0.67 | 0.003 |
| I-FABP (ng/mL, median, and IQR range) | 1.63 (1.15–1.98) | 1.42 (1.05–1.83) | 1.71 (1.19–2.00) | 1.68 (1.31–2.30) | 1.97 (1.42–2.35) | 1.53 (1.31–2.19) | 0.18 | 0.75 |
| B | Lower 95%CI | Upper 95%CI | p Value | |
|---|---|---|---|---|
| Group (Ref. Controls) | −26.7 | −98.0 | 44.7 | 0.46 |
| Sex (Ref. Males) | −20.7 | −72.2 | 30.9 | 0.42 |
| Age | −2.7 | −5.86 | 0.36 | 0.08 |
| FEV1 (% of pred.) | 0.88 | −0.46 | 2.21 | 0.19 |
| Leptin (ng/mL) * | −2.65 | −3.91 | −1.39 | <0.0001 |
| Phase angle (degrees) | 57.3 | 27.5 | 87.2 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cuttitta, G.; Ferraro, M.; Cibella, F.; Alfano, P.; Bucchieri, S.; Patti, A.M.; Muratori, R.; Pace, E.; Bruno, A. Relationship among Body Composition, Adipocytokines, and Irisin on Exercise Capacity and Quality of Life in COPD: A Pilot Study. Biomolecules 2023, 13, 48. https://doi.org/10.3390/biom13010048
Cuttitta G, Ferraro M, Cibella F, Alfano P, Bucchieri S, Patti AM, Muratori R, Pace E, Bruno A. Relationship among Body Composition, Adipocytokines, and Irisin on Exercise Capacity and Quality of Life in COPD: A Pilot Study. Biomolecules. 2023; 13(1):48. https://doi.org/10.3390/biom13010048
Chicago/Turabian StyleCuttitta, Giuseppina, Maria Ferraro, Fabio Cibella, Pietro Alfano, Salvatore Bucchieri, Angelo Maria Patti, Rosalba Muratori, Elisabetta Pace, and Andreina Bruno. 2023. "Relationship among Body Composition, Adipocytokines, and Irisin on Exercise Capacity and Quality of Life in COPD: A Pilot Study" Biomolecules 13, no. 1: 48. https://doi.org/10.3390/biom13010048