
Morphometric Changes of Osteocyte Lacunar in Diabetic Pig Mandibular Cancellous Bone

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Pig Diabetes Model and Mandibular Bone Sample Preparation
2.2. BSE Image Acquisition for the Analysis of Osteocyte/Lacunae
2.3. Post-Acquisition Image Processing
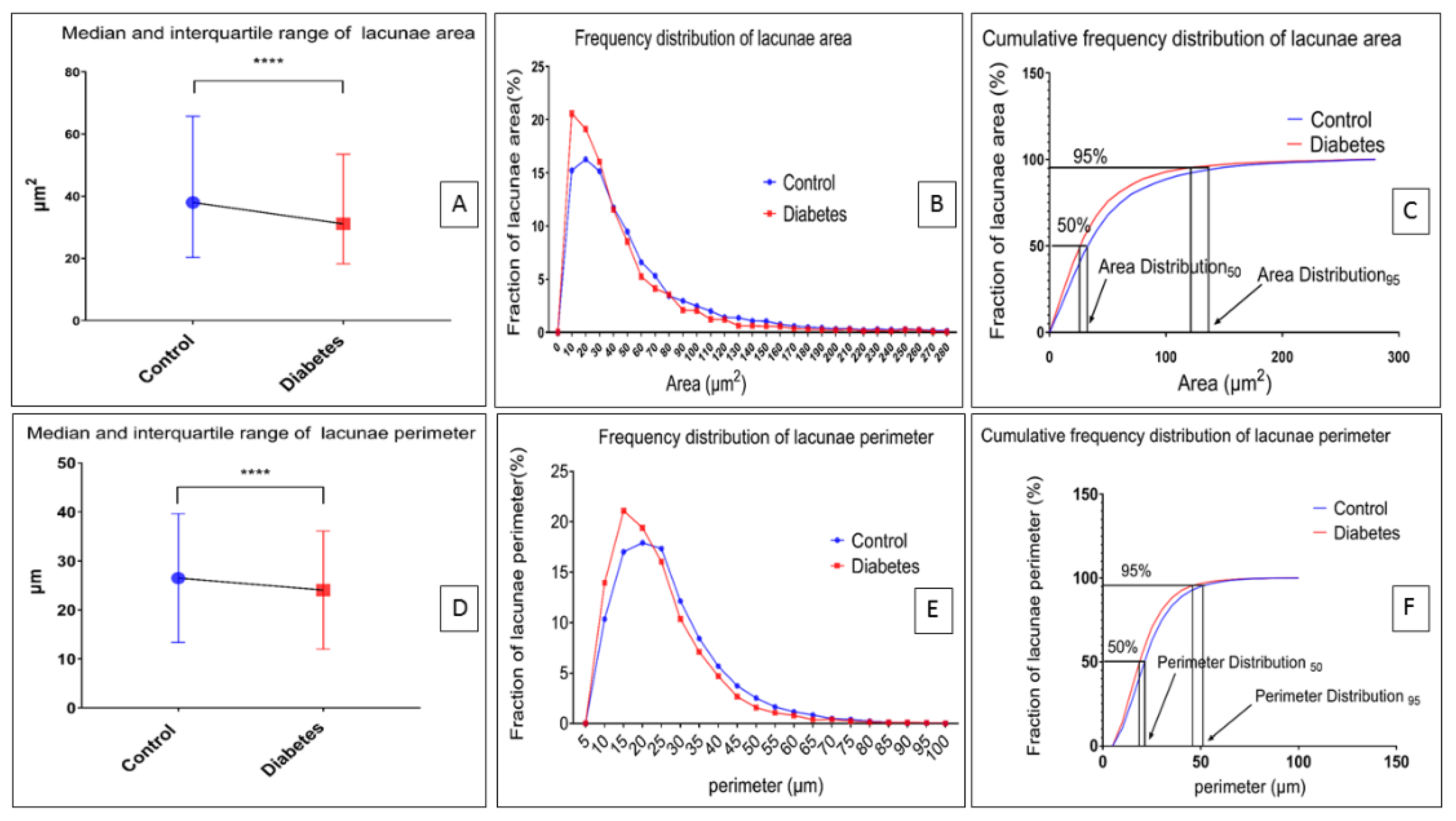
2.4. Acquisition of Osteocyte Lacunae Morphometric Data
- Area: Area of selection in square units
- Perimeter: The length of the outside boundary of the selection
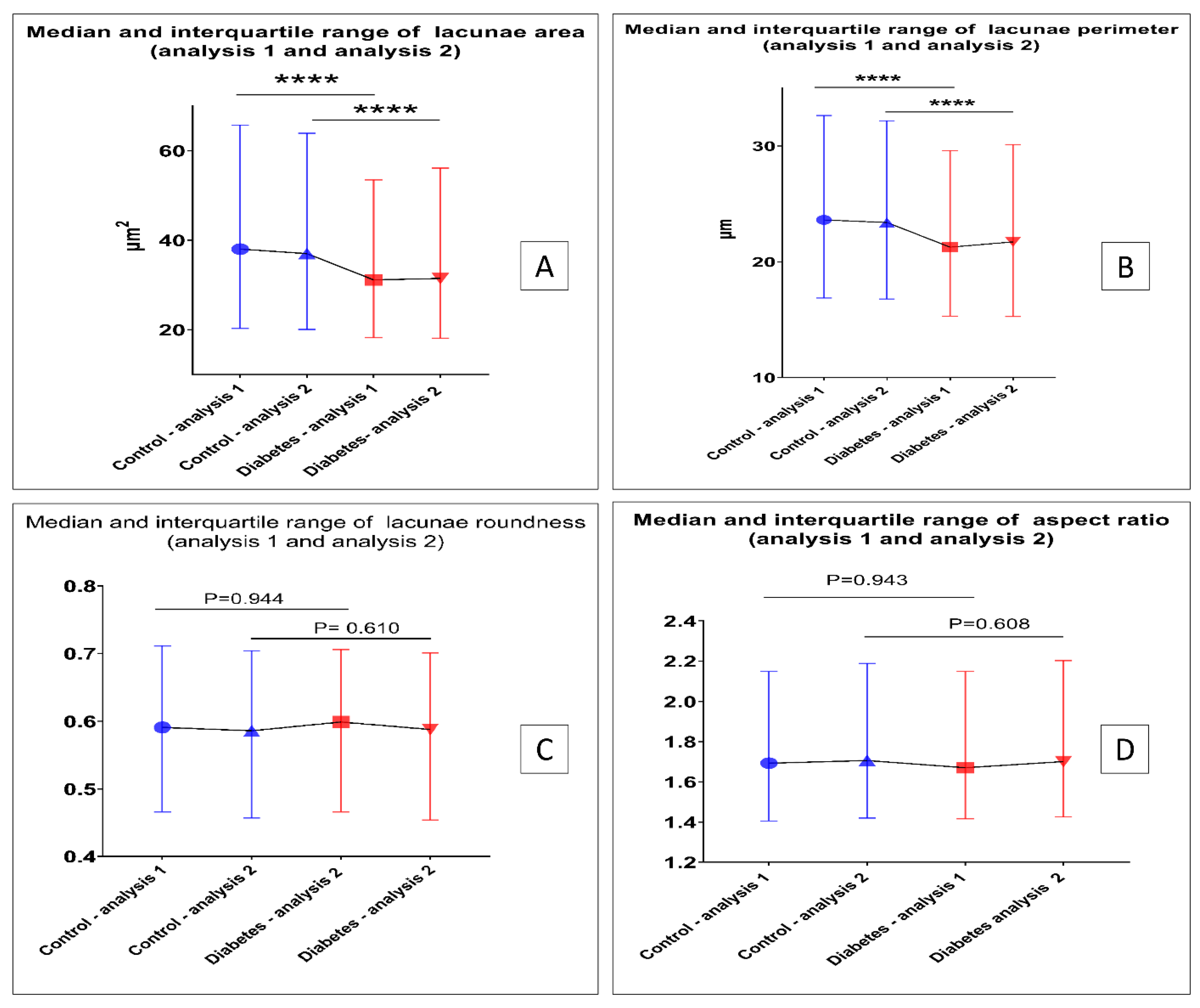
- Aspect ratio: The aspect ratio of the particle’s fitted ellipse, [Major Axis]/[Minor Axis]
- or the inverse of the aspect ratio
2.5. Method Reproducibility Analysis
2.6. BSE Image for Acid-Etched Resin Embedded Samples
2.7. Micro-CT Data Acquisition for Trabecular Bone
2.8. Statistical Analysis
3. Results
3.1. Establishment of a Diabetic Pig Model
3.2. Establishment of BSE Image Processing Workflow
3.3. Morphometric Changes of Osteocyte Lacunar in Diabetic Pig Mandibular Cancellous Bone
3.4. The Reproducibility and Robustness of Our BSE Image Analysis Method
3.5. Morphometric Changes of Trabecular Bone in Diabetic Pig Mandibular Cancellous Bone
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dallas, S.L.; Prideaux, M.; Bonewald, L.F. The Osteocyte: An Endocrine Cell and More. Endocr. Rev. 2013, 34, 658–690. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brun, J.; Berthou, F.; Trajkovski, M.; Maechler, P.; Foti, M.; Bonnet, N. Bone Regulates Browning and Energy Metabolism Through Mature Osteoblast/Osteocyte PPAR gamma Expression. Diabetes 2017, 66, 2541–2554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonewald, L.F. The amazing osteocyte. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2011, 26, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Vatsa, A.; Breuls, R.G.; Semeins, C.M.; Salmon, P.L.; Smit, T.H.; Klein-Nulend, J. Osteocyte morphology in fibula and calvaria—Is there a role for mechanosensing? Bone 2008, 43, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Hesse, B.; Varga, P.; Langer, M.; Pacureanu, A.; Schrof, S.; Mannicke, N.; Suhonen, H.; Maurer, P.; Cloetens, P.; Peyrin, F.; et al. Canalicular Network Morphology is the Major Determinant of the Spatial Distribution of Mass Density in Human Bone Tissue: Evidence by Means of Synchrotron Radiation Phase-Contrast nano-CT. J. Bone Miner. Res. 2015, 30, 346–356. [Google Scholar] [CrossRef]
- Qing, H.; Ardeshirpour, L.; Pajevic, P.D.; Dusevich, V.; Jahn, K.; Kato, S.; Wysolmerski, J.; Bonewald, L.F. Demonstration of osteocytic perilacunar/canalicular remodeling in mice during lactation. J. Bone Miner. Res. 2012, 27, 1018–1029. [Google Scholar] [CrossRef] [Green Version]
- Klein-Nulend, J.; Nijweide, P.J.; Burger, E.H. Osteocyte and bone structure. Curr. Osteoporos. Rep. 2003, 1, 5–10. [Google Scholar] [CrossRef]
- Bacabac, R.G.; Mizuno, D.; Schmidt, C.F.; MacKintosh, F.C.; Van Loon, J.J.W.A.; Klein-Nulend, J.; Smit, T.H. Round versus flat: Bone cell morphology, elasticity, and mechanosensing. J. Biomech. 2008, 41, 1590–1598. [Google Scholar] [CrossRef]
- van Oers, R.F.; Wang, H.; Bacabac, R.G. Osteocyte shape and mechanical loading. Curr. Osteoporos. Rep. 2015, 13, 61–66. [Google Scholar] [CrossRef] [Green Version]
- van Hove, R.P.; Nolte, P.A.; Vatsa, A.; Semeins, C.M.; Salmon, P.L.; Smit, T.H.; Klein-Nulend, J. Osteocyte morphology in human tibiae of different bone pathologies with different bone mineral density—Is there a role for mechanosensing? Bone 2009, 45, 321–329. [Google Scholar] [CrossRef]
- Jaiprakash, A.; Prasadam, I.; Feng, J.Q.; Liu, Y.; Crawford, R.; Xiao, Y. Phenotypic characterization of osteoarthritic osteocytes from the sclerotic zones: A possible pathological role in subchondral bone sclerosis. Int. J. Biol. Sci. 2012, 8, 406–417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Y.Y.; Xiao, E.; Graves, D.T. Diabetes mellitus related bone metabolism and periodontal disease. Int. J. Oral. Sci. 2015, 7, 63–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghodsi, M.; Larijani, B.; Keshtkar, A.A.; Nasli-Esfahani, E.; Alatab, S.; Mohajeri-Tehrani, M.R. Mechanisms involved in altered bone metabolism in diabetes: A narrative review. J. Diabetes Metab. Disord. 2016, 15, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starup-Linde, J.; Vestergaard, P. Biochemical bone turnover markers in diabetes mellitus—A systematic review. Bone 2016, 82, 69–78. [Google Scholar] [CrossRef]
- Schwartz, A.V. Epidemiology of fractures in type 2 diabetes. Bone 2016, 82, 2–8. [Google Scholar] [CrossRef]
- Boyde, A.; Jones, S.J. Scanning electron microscopy of bone: Instrument, specimen, and issues. Microsc. Res. Tech. 1996, 33, 92–120. [Google Scholar] [CrossRef]
- Du, Z.B.; Ivanovski, S.; Hamlet, S.M.; Feng, J.Q.; Xiao, Y. The Ultrastructural Relationship Between Osteocytes and Dental Implants Following Osseointegration. Clin. Implant. Dent. R. 2016, 18, 270–280. [Google Scholar] [CrossRef]
- Boyde, A. Scanning Electron Microscopy of Bone. Methods Mol. Biol. 2019, 1914, 571–616. [Google Scholar]
- Suthagar, E.; Soudamani, S.; Yuvaraj, S.; Khan, A.I.; Aruldhas, M.M.; Balasubramanian, K. Effects of streptozotocin (STZ)-induced diabetes and insulin replacement on rat ventral prostate. Biomed. Pharmacother. 2009, 63, 43–50. [Google Scholar] [CrossRef]
- Goyal, S.N.; Reddy, N.M.; Patil, K.R.; Nakhate, K.T.; Ojha, S.; Patil, C.R.; Agrawal, Y.O. Challenges and issues with streptozotocin-induced diabetes—A clinically relevant animal model to understand the diabetes pathogenesis and evaluate therapeutics. Chem.-Biol. Interact. 2016, 244, 49–63. [Google Scholar] [CrossRef]
- Kubek, D.J.; Gattone, V.H., II; Allen, M.R. Methodological assessment of acid-etching for visualizing the osteocyte lacunar-canalicular networks using scanning electron microscopy. Microsc. Res. Tech. 2010, 73, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Jandl, N.M.; von Kroge, S.; Sturznickel, J.; Baranowsky, A.; Stockhausen, K.E.; Mushumba, H.; Beil, F.T.; Puschel, K.; Amling, M.; Rolvien, T. Large osteocyte lacunae in iliac crest infantile bone are not associated with impaired mineral distribution or signs of osteocytic osteolysis. Bone 2020, 135, 115324. [Google Scholar] [CrossRef] [PubMed]
- Blouin, S.; Fratzl-Zelman, N.; Glorieux, F.H.; Roschger, P.; Klaushofer, K.; Marini, J.C.; Rauch, F. Hypermineralization and High Osteocyte Lacunar Density in Osteogenesis Imperfecta Type V Bone Indicate Exuberant Primary Bone Formation. J. Bone Miner. Res. 2017, 32, 1884–1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knothe Tate, M.L.; Adamson, J.R.; Tami, A.E.; Bauer, T.W. The osteocyte. Int. J. Biochem. Cell. Biol. 2004, 36, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Arena, E.T.; Rueden, C.T.; Hiner, M.C.; Wang, S.; Yuan, M.; Eliceiri, K.W. Quantitating the cell: Turning images into numbers with ImageJ. Wiley Interdiscip. Rev. Dev. Biol. 2017, 6, e260. [Google Scholar] [CrossRef]
- Baud, C.A.; Auil, E. Osteocyte Differential Count in Normal Human Alveolar Bone. Acta Anat. 1971, 78, 321–327. [Google Scholar] [CrossRef]
- Heveran, C.M.; Rauff, A.; King, K.B.; Carpenter, R.D.; Ferguson, V.L. A new open-source tool for measuring 3D osteocyte lacunar geometries from confocal laser scanning microscopy reveals age-related changes to lacunar size and shape in cortical mouse bone. Bone 2018, 110, 115–127. [Google Scholar] [CrossRef]
- Portal-Nunez, S.; Lozano, D.; de Castro, L.F.; de Gortazar, A.R.; Nogues, X.; Esbrit, P. Alterations of the Wnt/beta-catenin pathway and its target genes for the N- and C-terminal domains of parathyroid hormone-related protein in bone from diabetic mice. Febs Lett. 2010, 584, 3095–3100. [Google Scholar] [CrossRef] [Green Version]
- Parajuli, A.; Liu, C.; Li, W.; Gu, X.Y.; Lai, X.H.; Pei, S.P.; Price, C.; You, L.D.; Lu, X.L.; Wang, L.Y. Bone’s responses to mechanical loading are impaired in type 1 diabetes. Bone 2015, 81, 152–160. [Google Scholar] [CrossRef] [Green Version]
- Leslie, W.D.; Aubry-Rozier, B.; Lamy, O.; Hans, D.; Manitoba Bone Density, P. TBS (trabecular bone score) and diabetes-related fracture risk. J. Clin. Endocrinol. Metab. 2013, 98, 602–609. [Google Scholar] [CrossRef] [Green Version]
- Farr, J.N.; Drake, M.T.; Amin, S.; Melton, L.J., 3rd; McCready, L.K.; Khosla, S. In vivo assessment of bone quality in postmenopausal women with type 2 diabetes. J. Bone Miner. Res. Off. J. Am. Soc. Bone Miner. Res. 2014, 29, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Belanger, L.F. Osteocytic Osteolysis. Calcif. Tissue Res. 1969, 4, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Belanger, L.F. Osteocytic Osteolysis in a Cretaceous Reptile. Rev. Can. Biol. 1977, 36, 71–73. [Google Scholar] [PubMed]
- Doty, S.B.; Nunez, E.A. Activation of Osteoclasts and the Repopulation of Bone Surfaces Following Hibernation in the Bat, Myotis-Lucifugus. Anat. Rec. 1985, 213, 481–495. [Google Scholar] [CrossRef] [PubMed]
- Milovanovic, P.; Zimmermann, E.A.; Hahn, M.; Djonic, D.; Puschel, K.; Djuric, M.; Amling, M.; Busse, B. Osteocytic canalicular networks: Morphological implications for altered mechanosensitivity. ACS Nano 2013, 7, 7542–7551. [Google Scholar] [CrossRef]











Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yao, S.; Du, Z.; Xiao, L.; Yan, F.; Ivanovski, S.; Xiao, Y. Morphometric Changes of Osteocyte Lacunar in Diabetic Pig Mandibular Cancellous Bone. Biomolecules 2023, 13, 49. https://doi.org/10.3390/biom13010049
Yao S, Du Z, Xiao L, Yan F, Ivanovski S, Xiao Y. Morphometric Changes of Osteocyte Lacunar in Diabetic Pig Mandibular Cancellous Bone. Biomolecules. 2023; 13(1):49. https://doi.org/10.3390/biom13010049
Chicago/Turabian StyleYao, Sheng, Zhibin Du, Lan Xiao, Fuhua Yan, Saso Ivanovski, and Yin Xiao. 2023. "Morphometric Changes of Osteocyte Lacunar in Diabetic Pig Mandibular Cancellous Bone" Biomolecules 13, no. 1: 49. https://doi.org/10.3390/biom13010049