

Dehydroepiandrosterone Sulfate, an Adrenal Androgen, Is Inversely Associated with Prevalence of Dynapenia in Male Individuals with Type 2 Diabetes
 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects for Cross-Sectional Study
2.2. Biochemical Analyses
2.3. Assessments of Muscle Strength and Physical Performance
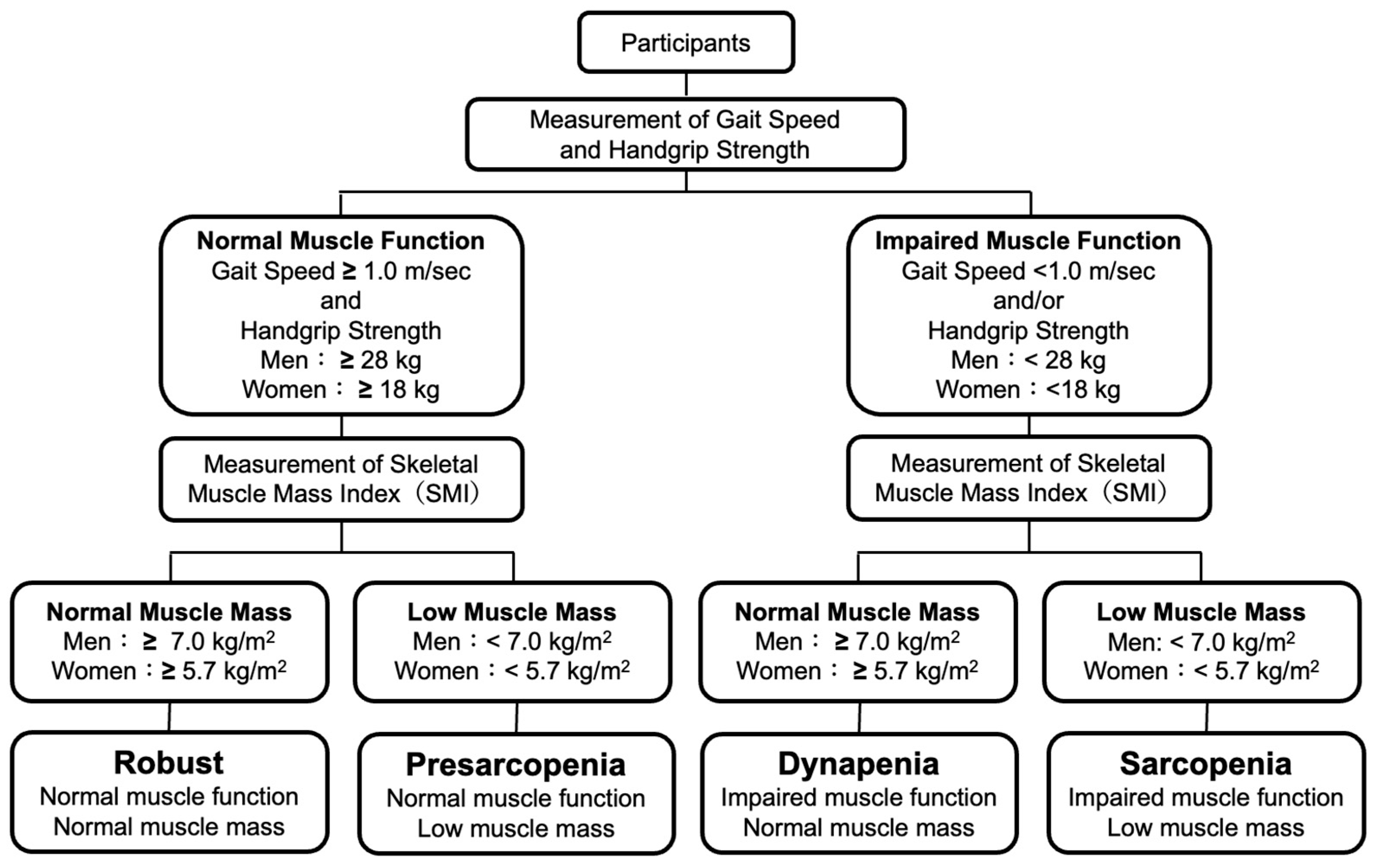
2.4. Definitions of Robust, Presarcopenia, Sarcopenia and Dynapenia
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of Subjects Enrolled in This Study
3.2. Associations of Serum Levels of DHEAS with SMI, HS and GS
3.3. Associations of Clinical Factors Including DHEAS with SMI, HS and GS
3.4. Determination of Clinical Factors for Prevalences of Presarcopenia, Sarcopenia and Dynapenia
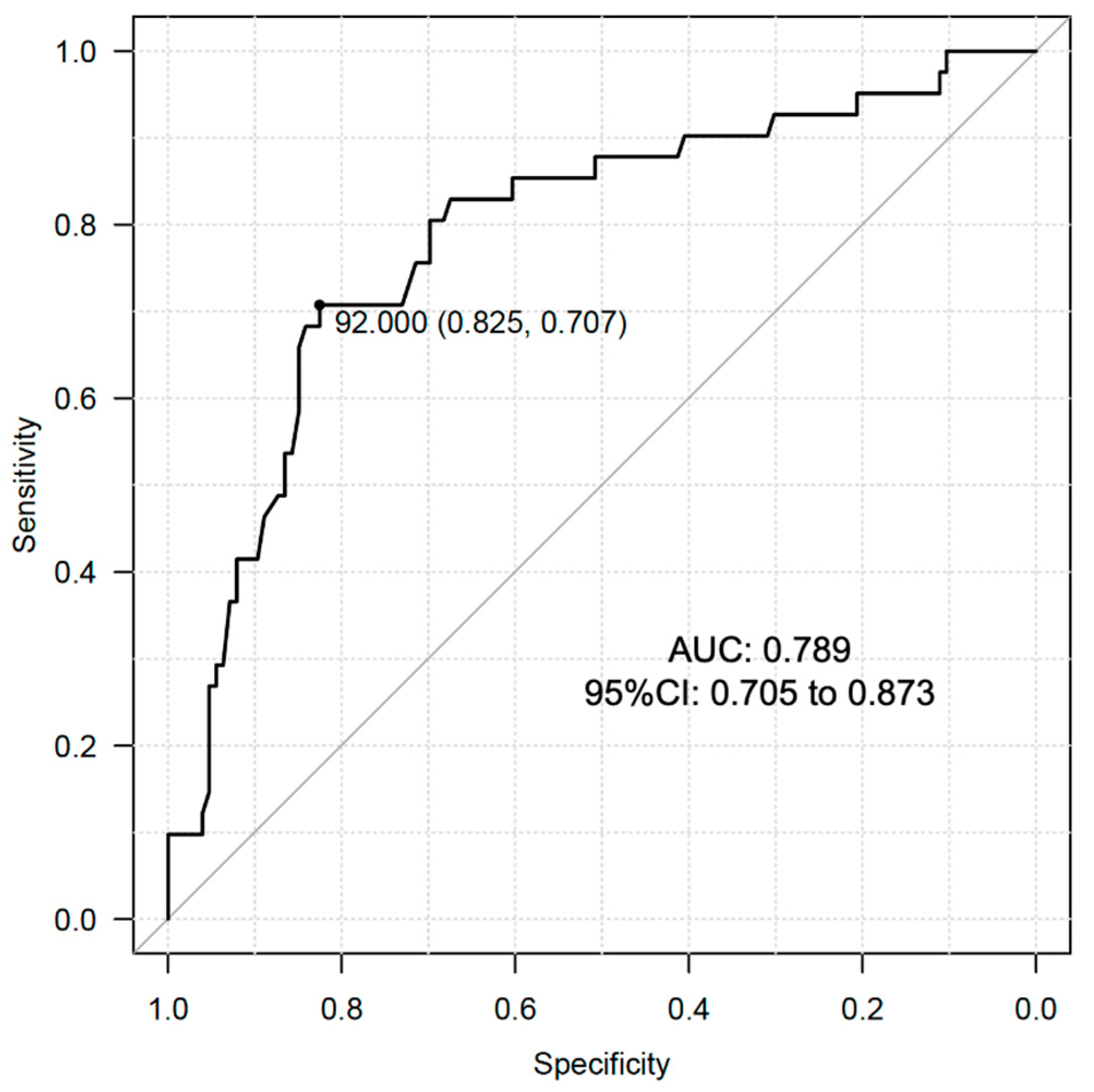
3.5. Determination of Cutoff Value of Serum DHEAS Levels for Prevalence of Dynapenia in Male Individuals with T2D
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manini, T.M.; Clark, B.C. Dynapenia and aging: An update. J. Gerontol. A Biol. Sci. Med. Sci. 2012, 67, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Feng, X.; Zhou, J.; Gong, H.; Xia, S.; Wei, Q.; Hu, X.; Tao, R.; Li, L.; Qian, F.; et al. Type 2 diabetes mellitus is associated with increased risks of sarcopenia and pre-sarcopenia in Chinese elderly. Sci. Rep. 2016, 6, 38937. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Kuroda, A.; Yoshida, S.; Yasuda, T.; Umayahara, Y.; Shimizu, S.; Ryomoto, K.; Yoshiuchi, K.; Yamamoto, T.; Matsuoka, T.A.; et al. High prevalence and clinical impact of dynapenia and sarcopenia in Japanese patients with type 1 and type 2 diabetes: Findings from the Impact of Diabetes Mellitus on Dynapenia study. J. Diabetes Investig. 2021, 12, 1050–1059. [Google Scholar] [CrossRef]
- Beretta, M.V.; Dantas Filho, F.F.; Freiberg, R.E.; Feldman, J.V.; Nery, C.; Rodrigues, T.C. Sarcopenia and Type 2 diabetes mellitus as predictors of 2-year mortality after hospital discharge in a cohort of hospitalized older adults. Diabetes Res. Clin. Pract. 2020, 159, 107969. [Google Scholar] [CrossRef]
- Lamberts, S.W.; van den Beld, A.W.; van der Lely, A.J. The endocrinology of aging. Science 1997, 278, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Swiecicka, A.; Lunt, M.; Ahern, T.; O’Neill, T.W.; Bartfai, G.; Casanueva, F.F.; Forti, G.; Giwercman, A.; Han, T.S.; Lean, M.E.J.; et al. Nonandrogenic Anabolic Hormones Predict Risk of Frailty: European Male Ageing Study Prospective Data. J. Clin. Endocrinol. Metab. 2017, 102, 2798–2806. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, S.; Aihara, K.; Azuma, H.; Uemoto, R.; Sumitomo-Ueda, Y.; Yagi, S.; Ikeda, Y.; Iwase, T.; Nishio, S.; Kawano, H.; et al. Dehydroepiandrosterone sulfate is inversely associated with sex-dependent diverse carotid atherosclerosis regardless of endothelial function. Atherosclerosis 2010, 212, 310–315. [Google Scholar] [CrossRef]
- Wu, T.T.; Chen, Y.; Zhou, Y.; Adi, D.; Zheng, Y.Y.; Liu, F.; Ma, Y.T.; Xie, X. Prognostic Value of Dehydroepiandrosterone Sulfate for Patients With Cardiovascular Disease: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2017, 6, e004896. [Google Scholar] [CrossRef]
- Yanagita, I.; Fujihara, Y.; Kitajima, Y.; Tajima, M.; Honda, M.; Kawajiri, T.; Eda, T.; Yonemura, K.; Yamaguchi, N.; Asakawa, H.; et al. A High Serum Cortisol/DHEA-S Ratio Is a Risk Factor for Sarcopenia in Elderly Diabetic Patients. J. Endocr. Soc. 2019, 3, 801–813. [Google Scholar] [CrossRef]
- American Diabetes, A. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef]
- Hori, T.; Nakamura, S.; Yamagami, H.; Yasui, S.; Hosoki, M.; Hara, T.; Mitsui, Y.; Masuda, S.; Kurahashi, K.; Yoshida, S.; et al. Phase angle and extracellular water-to-total body water ratio estimated by bioelectrical impedance analysis are associated with levels of hemoglobin and hematocrit in patients with diabetes. Heliyon 2023, 9, e14724. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- Baumann, C.W.; Kwak, D.; Liu, H.M.; Thompson, L.V. Age-induced oxidative stress: How does it influence skeletal muscle quantity and quality? J. Appl. Physiol. (1985) 2016, 121, 1047–1052. [Google Scholar] [CrossRef]
- Chao, Y.P.; Fang, W.H.; Chen, W.L.; Peng, T.C.; Yang, W.S.; Kao, T.W. Exploring Muscle Health Deterioration and Its Determinants Among Community-Dwelling Older Adults. Front. Nutr. 2022, 9, 817044. [Google Scholar] [CrossRef]
- Komatsu, T.R.; Borim, F.S.; Neri, A.L.; Corona, L.P. Association of dynapenia, obesity and chronic diseases with all-cause mortality of community-dwelling older adults: A path analysis. Geriatr. Gerontol. Int. 2019, 19, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Luiz, M.M.; Schneider, I.J.C.; Kuriki, H.U.; Fattori, A.; Correa, V.P.; Steptoe, A.; Alexandre, T.D.S.; de Oliveira, C. The combined effect of anemia and dynapenia on mortality risk in older adults: 10-Year evidence from the ELSA cohort study. Arch. Gerontol. Geriatr. 2022, 102, 104739. [Google Scholar] [CrossRef]
- Kobayashi, T.; Askanas, V.; Engel, W.K. Human muscle cultured in monolayer and cocultured with fetal rat spinal cord: Importance of dorsal root ganglia for achieving successful functional innervation. J. Neurosci. 1987, 7, 3131–3141. [Google Scholar] [CrossRef]
- Vasilaki, A.; Jackson, M.J. Role of reactive oxygen species in the defective regeneration seen in aging muscle. Free Radic. Biol. Med. 2013, 65, 317–323. [Google Scholar] [CrossRef]
- Vistoli, G.; De Maddis, D.; Cipak, A.; Zarkovic, N.; Carini, M.; Aldini, G. Advanced glycoxidation and lipoxidation end products (AGEs and ALEs): An overview of their mechanisms of formation. Free Radic. Res. 2013, 47 (Suppl. S1), 3–27. [Google Scholar] [CrossRef]
- Moldogazieva, N.T.; Mokhosoev, I.M.; Mel’nikova, T.I.; Porozov, Y.B.; Terentiev, A.A. Oxidative Stress and Advanced Lipoxidation and Glycation End Products (ALEs and AGEs) in Aging and Age-Related Diseases. Oxid. Med. Cell Longev. 2019, 2019, 3085756. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Kuroda, A.; Ishizu, M.; Ohishi, M.; Takashi, Y.; Otsuka, Y.; Taniguchi, S.; Tamaki, M.; Kurahashi, K.; Yoshida, S.; et al. Association of accumulated advanced glycation end-products with a high prevalence of sarcopenia and dynapenia in patients with type 2 diabetes. J. Diabetes Investig. 2019, 10, 1332–1340. [Google Scholar] [CrossRef] [PubMed]
- Kato, M.; Kubo, A.; Sugioka, Y.; Mitsui, R.; Fukuhara, N.; Nihei, F.; Takeda, Y. Relationship between advanced glycation end-product accumulation and low skeletal muscle mass in Japanese men and women. Geriatr. Gerontol. Int. 2017, 17, 785–790. [Google Scholar] [CrossRef]
- Brignardello, E.; Runzo, C.; Aragno, M.; Catalano, M.G.; Cassader, M.; Perin, P.C.; Boccuzzi, G. Dehydroepiandrosterone administration counteracts oxidative imbalance and advanced glycation end product formation in type 2 diabetic patients. Diabetes Care 2007, 30, 2922–2927. [Google Scholar] [CrossRef]
- Aragno, M.; Mastrocola, R.; Medana, C.; Catalano, M.G.; Vercellinatto, I.; Danni, O.; Boccuzzi, G. Oxidative stress-dependent impairment of cardiac-specific transcription factors in experimental diabetes. Endocrinology 2006, 147, 5967–5974. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.; Cai, H.L.; Bao, J.P.; Wu, L.D. Dehydroepiandrosterone and age-related musculoskeletal diseases: Connections and therapeutic implications. Ageing Res. Rev. 2020, 62, 101132. [Google Scholar] [CrossRef] [PubMed]
- Kostka, T.; Arsac, L.M.; Patricot, M.C.; Berthouze, S.E.; Lacour, J.R.; Bonnefoy, M. Leg extensor power and dehydroepiandrosterone sulfate, insulin-like growth factor-I and testosterone in healthy active elderly people. Eur. J. Appl. Physiol. 2000, 82, 83–90. [Google Scholar] [CrossRef]
- Valenti, G.; Denti, L.; Maggio, M.; Ceda, G.; Volpato, S.; Bandinelli, S.; Ceresini, G.; Cappola, A.; Guralnik, J.M.; Ferrucci, L. Effect of DHEAS on skeletal muscle over the life span: The InCHIANTI study. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 466–472. [Google Scholar] [CrossRef]
- Baker, W.L.; Karan, S.; Kenny, A.M. Effect of dehydroepiandrosterone on muscle strength and physical function in older adults: A systematic review. J. Am. Geriatr. Soc. 2011, 59, 997–1002. [Google Scholar] [CrossRef]
- Percheron, G.; Hogrel, J.Y.; Denot-Ledunois, S.; Fayet, G.; Forette, F.; Baulieu, E.E.; Fardeau, M.; Marini, J.F.; Double-blind placebo-controlled, t. Effect of 1-year oral administration of dehydroepiandrosterone to 60- to 80-year-old individuals on muscle function and cross-sectional area: A double-blind placebo-controlled trial. Arch. Intern. Med. 2003, 163, 720–727. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Robust | Pre-Sarcopenia | Sarcopenia | Dynapenia | |
|---|---|---|---|---|---|
| Number of Subjects | 361 | 233 | 22 | 37 | 69 |
| Clinical Parameters | |||||
| Male (Female) | 202 (159) | 126 (107) | 16 (6) | 19 (18) | 41 (28) |
| Age (year) | 69 (61, 75) | 64 (58, 71) | 73 (70, 78) * | 76 (72, 81) * | 75 (71, 79) ** |
| BMI (kg/m2) | 24.2 (21.9, 26.9) | 25.2 (22.9, 28.0) | 20.1 (19.0, 20.7) ** | 20.1 (18.8, 22.7) ** | 24.3 (22.5, 25.9) #$ |
| Exercise (≥3 Mets) (n, (%)) | 118 (32.7) | 79 (33.9) | 11 (50.0) | 8 (21.6) | 20 (29.0) * |
| Current Smoking (n, (%)) | 58 (16.1) | 43 (18.5) | 4 (18.2) | 4 (10.8) | 7 (10.1) |
| Hypertension (n, (%)) | 229 (63.4) | 141 (60.5) | 15 (68.2) | 27 (75.0) | 46 (66.7) |
| Dyslipidemia (n, (%)) | 274 (75.9) | 183 (78.5) | 10 (45.5) ** | 28 (75.7) | 53 (76.8) |
| Duration of T2D (year) | 9 (2, 17) | 6 (1, 12) | 16 (11, 27) ** | 12 (7, 20) * | 12 (6, 20) ** |
| SBP (mmHg) | 132 (121, 143) | 132 (121, 142) | 127 (119, 140) | 132 (121, 144) | 133 (121, 143) |
| LDL-C (mg/dL) | 98 (80, 119) | 101 (81, 121) | 102 (88, 116) | 94 (81, 110) | 89 (75, 116) |
| HDL-C (mg/dL) | 52 (44, 62) | 51 (44, 62) | 61 (52, 69.8) | 52 (44, 61) | 53 (45, 59) |
| TG (mg/dL) | 110 (78, 162) | 121 (81, 175) | 86 (69, 116) | 98 (72, 131) | 101 (72, 152) |
| Caual PG (mg/dL) | 131 (113, 171) | 130 (112, 162) | 149 (124, 189) | 124 (110, 167) | 132 (117, 175) |
| HbA1c (%) | 6.7 (6.3, 7.3) | 6.7 (6.3, 7.3) | 6.8 (6.5, 7.5) | 6.8 (6.3, 7.2) | 6.7 (6.3, 7.2) |
| UA (mg/dL) | 4.9 (4.1, 5.9) | 5.0 (4.1, 5.9) | 5.2 (4.6, 5.9) | 4.5 (3.8, 5.3) | 4.8 (4.2, 6.0) |
| Cr (mg/dL) | 0.74 (0.62. 0.92) | 0.73 (0.61. 0.90) | 0.78 (0.66. 0.96) | 0.70 (0.59, 0.92) | 0.77 (0.62, 1.05) |
| ALB (g/dL) | 4.2 (4.0, 4.4) | 4.3 (4.1, 4.5) | 4.3 (4.0, 4.4) | 4.1 (4.0, 4.3) | 4.2 (3.8, 4.4) |
| DHEAS (μg/dL) | 97 (60, 159) | 107 (63, 180) | 114 (76, 181) | 84 (47, 124) | 78 (53, 113) * |
| Skeletal Muscle-associated Indices | |||||
| SMI (kg/m2) | 7.1 (6.4, 7.8) | 7.4 (6.8, 8) | 6.6 (5.8, 6.7) ** | 5.7 (5.3, 6.5) **# | 7.1 (6.6, 7.6) #$$ |
| HS (kg) | 26.5 (20.5, 33.8) | 29.5 (23.0, 36.5) | 27.5 (24.5, 28.4) | 17.5 (14.5, 23.3) **# | 21.8 (16.8, 26.5) ** |
| GS (m/s) | 1.22 ± 0.26 | 1.32 ± 0.21 | 1.30 ± 0.20 | 1.05 ± 0.26 **# | 0.95 ± 0.19 **# |
| Medications Used | |||||
| ARB/ACEi (n, (%)) | 143 (39.6) | 92 (39.5) | 8 (36.4) | 14 (37.8) | 29 (42.0) |
| CCB (n, (%)) | 133 (36.8) | 81 (34.5) | 7 (31.8) | 15 (40.5) | 30 (43.5) |
| β blocker (n, (%)) | 10 (2.8) | 5 (2.1) | 2 (9.1) | 1 (2.7) | 2 (2.9) |
| MR blocker (n, (%)) | 4 (1.1) | 3 (1.3) | 1 (4.5) | 0 (0) | 0 (0)# |
| Stain (n, (%)) | 184 (51.0) | 117 (50.2) | 9 (40.9) | 22 (59.5) | 36 (52.2) |
| Ezetimibe (n, (%)) | 25 (6.9) | 13 (5.6) | 1 (4.5) | 2 (5.4) | 9 (13.0) |
| Other lipid-lowering drugs (n, (%)) | 7 (1.9) | 4 (1.7) | 0 (0) | 0 (0) | 3 (4.3) |
| Antiplatelet (n, (%)) | 36 (10.0) | 10 (4.3) | 0 (0) | 11 (29.7) **# | 15 (21.7) **#$ |
| SU or Glinide (n, (%)) | 68 (18.8) | 32 (13.7) | 7 (31.8) | 9 (24.3) | 20 (29.0) |
| DPP-4i (n, (%)) | 207 (57.3) | 124 (53.2) | 12 (54.5) | 27 (73.0) | 44 (63.8) |
| Metformin (n, (%)) | 180 (49.9) | 116 (49.8) | 8 (36.4) | 20 (54.1) | 36 (52.2) |
| αGI (n, (%)) | 47 (13.0) | 24 (10.3) | 2 (9.1) | 7 (19.0) | 14 (20.3) |
| Glitazone (n, (%)) | 11 (3.0) | 5 (2.1) | 2 (9.1) | 1 (2.7) | 3 (4.3) |
| SGLT2i (n, (%)) | 147 (40.7) | 98 (42.1) | 7 (31.8) | 11 (29.7) | 31 (44.9) |
| Insulin (n, (%)) | 71 (19.7) | 40 (17.2) | 8 (36.4) | 9 (24.3) | 14 (20.3) |
| GLP-1RA (n, (%)) | 37 (10.2) | 23 (9.9) | 2 (9.1) | 4 (10.8) | 8 (11.6) |
| Total | Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Skeletal Muscle-Associated Indices | Coefficient | 95% CI | p Value | Coefficient | 95% CI | p Value | Coefficient | 95% CI | p Value |
| SMI | 0.004 | 0.003 to 0.006 | <0.001 | 0.003 | 0.001 to 0.004 | <0.001 | 0.002 | −0.001 to 0.004 | 0.059 |
| HS | 0.046 | 0.036 to 0.056 | <0.001 | 0.035 | 0.022 to 0.049 | <0.001 | 0.017 | 0.005 to 0.030 | 0.006 |
| GS | 0.001 | 0.000 to 0.001 | 0.002 | 0.001 | 0.000 to 0.001 | <0.001 | 0.001 | −0.001 to 0.001 | 0.853 |
| SMI | HS | GS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | t Value | VIF | p Value | t Value | VIF | p Value | t Value | VIF | p Value |
| Age | −8.048 | 1.727 | <0.001 | −7.213 | 1.727 | <0.001 | −5.469 | 1.717 | <0.001 |
| Male | 14.500 | 1.692 | <0.001 | 11.760 | 1.692 | <0.001 | −2.051 | 1.695 | 0.041 |
| BMI | 20.670 | 1.584 | <0.001 | 2.481 | 1.584 | 0.014 | −2.356 | 1.521 | 0.019 |
| Exercise (≥3 Mets) | 2.925 | 1.100 | 0.004 | 2.213 | 1.100 | 0.028 | 2.643 | 1.103 | 0.009 |
| Current Smoking | 0.980 | 1.237 | 0.328 | 1.167 | 1.237 | 0.244 | −0.484 | 1.238 | 0.628 |
| Hypertension | 0.747 | 1.360 | 0.456 | 0.596 | 1.360 | 0.552 | −0.078 | 1.362 | 0.938 |
| Dyslipidemia | −1.752 | 1.198 | 0.081 | −0.753 | 1.198 | 0.452 | −0.662 | 1.200 | 0.509 |
| Duration of T2D | 0.512 | 1.228 | 0.609 | −3.091 | 1.228 | 0.002 | 0.365 | 1.232 | 0.715 |
| SBP | −2.654 | 1.268 | 0.008 | −0.547 | 1.268 | 0.585 | 0.602 | 1.286 | 0.547 |
| LDL-C | −2.784 | 1.216 | 0.006 | −1.740 | 1.216 | 0.083 | 1.419 | 1.226 | 0.157 |
| HDL-C | 0.985 | 1.470 | 0.326 | 0.051 | 1.470 | 0.959 | 0.313 | 1.459 | 0.754 |
| TG | 0.096 | 1.442 | 0.923 | 0.039 | 1.442 | 0.969 | 0.593 | 1.480 | 0.554 |
| HbA1c | 0.018 | 1.219 | 0.985 | −0.124 | 1.219 | 0.901 | −0.968 | 1.223 | 0.334 |
| UA | 1.467 | 1.435 | 0.143 | −2.289 | 1.435 | 0.023 | 0.618 | 1.422 | 0.537 |
| Cr | 2.880 | 1.420 | 0.004 | 3.248 | 1.420 | 0.001 | 1.153 | 1.407 | 0.250 |
| ALB | −1.314 | 1.229 | 0.190 | 3.803 | 1.229 | <0.001 | 2.691 | 1.231 | 0.008 |
| DHEAS | −0.802 | 1.381 | 0.423 | 2.822 | 1.381 | 0.005 | 1.053 | 1.409 | 0.293 |
| Pre-Sarcopenia | Sarcopenia | Dynapenia | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | VIF | p Value | OR | 95% CI | VIF | p Value | OR | 95% CI | VIF | p Value |
| Age (1 year) | 1.022 | 0.950 to 1.107 | 1.632 | 0.562 | 1.241 | 1.127 to 1.403 | 1.724 | <0.001 | 1.147 | 1.092 to 1.213 | 1.645 | <0.001 |
| Male | 14.03 | 1.734 to 176.6 | 1.762 | 0.023 | 1.066 | 0.251 to 4.518 | 1.726 | 0.930 | 1.984 | 0.844 to 4.860 | 1.718 | 0.124 |
| BMI (1 kg/m2) | 0.390 | 0.217 to 0.582 | 1.520 | <0.001 | 0.597 | 0.452 to 0.745 | 1.519 | <0.001 | 1.053 | 0.961 to 1.155 | 1.538 | 0.264 |
| Exercise (≥3 Mets) | 1.076 | 0.240 to 4.859 | 1.164 | 0.923 | 0.311 | 0.080 to 1.047 | 1.097 | 0.072 | 0.498 | 0.236 to 1.012 | 1.105 | 0.060 |
| Current Smoking | 0.839 | 0.148 to 4.026 | 1.263 | 0.830 | 1.063 | 0.181 to 5.435 | 1.269 | 0.943 | 0.996 | 0.322 to 2.877 | 1.264 | 0.994 |
| Hypertension | 1.944 | 0.376 to 11.11 | 1.400 | 0.434 | 1.991 | 0.579 to 7.521 | 1.349 | 0.287 | 1.090 | 0.508 to 2.358 | 1.378 | 0.825 |
| Dyslipidemia | 0.547 | 0.110 to 2.613 | 1.219 | 0.447 | 2.358 | 0.583 to 10.86 | 1.162 | 0.245 | 0.879 | 0.379 to 2.088 | 1.189 | 0.765 |
| Duration of T2D (1 year) | 1.063 | 1.008 to 1.128 | 1.250 | 0.029 | 0.990 | 0.942 to 1.039 | 1.261 | 0.682 | 1.016 | 0.983 to 1.050 | 1.220 | 0.343 |
| SBP (1 mmHg) | 0.975 | 0.918 to 1.030 | 1.279 | 0.371 | 1.028 | 0.989 to 1.063 | 1.289 | 0.151 | 0.991 | 0.968 to 1.013 | 1.267 | 0.446 |
| LDL-C (1 mg/dL) | 0.997 | 0.968 to 1.024 | 1.262 | 0.849 | 0.994 | 0.974 to 1.014 | 1.242 | 0.586 | 0.996 | 0.984 to 1.008 | 1.247 | 0.479 |
| HDL-C (1 mg/dL) | 1.033 | 0.978 to 1.091 | 1.481 | 0.233 | 0.973 | 0.924 to 1.021 | 1.459 | 0.282 | 1.010 | 0.983 to 1.037 | 1.471 | 0.474 |
| TG (1 mg/dL) | 1.001 | 0.987 to 1.013 | 1.421 | 0.916 | 0.991 | 0.979 to 1.003 | 1.423 | 0.145 | 1.002 | 0.996 to 1.007 | 1.425 | 0.526 |
| HbA1c (1%) | 1.099 | 0.709 to 1.577 | 1.201 | 0.623 | 1.261 | 0.894 to 1.744 | 1.212 | 0.163 | 1.011 | 0.798 to 1.243 | 1.234 | 0.922 |
| UA (1 mg/dL) | 1.595 | 0.850 to 3.126 | 1.451 | 0.153 | 1.261 | 0.783 to 2.067 | 1.452 | 0.345 | 1.159 | 0.861 to 1.565 | 1.480 | 0.331 |
| Cr (1 mg/dL) | 0.781 | 0.007 to 14.52 | 1.375 | 0.915 | 0.138 | 0.006 to 2.418 | 1.362 | 0.193 | 0.471 | 0.081 to 1.859 | 1.441 | 0.380 |
| ALB (1 g/dL) | 1.516 | 0.166 to 11.88 | 1.236 | 0.698 | 0.959 | 0.139 to 6.965 | 1.259 | 0.966 | 0.496 | 0.199 to 1.250 | 1.218 | 0.130 |
| DHEAS (1 μg/dL) | 0.999 | 0.989 to 1.009 | 1.513 | 0.884 | 0.997 | 0.987 to 1.006 | 1.498 | 0.556 | 0.993 | 0.987 to 0.998 | 1.396 | 0.014 |
| Dynapenia | ||||||||
|---|---|---|---|---|---|---|---|---|
| Males | Females | |||||||
| Variables | OR | 95% CI | VIF | p Value | OR | 95% CI | VIF | p Value |
| Age (1 year) | 1.142 | 1.060 to 1.247 | 2.114 | 0.001 | 1.261 | 1.147 to 1.418 | 1.528 | <0.001 |
| BMI (1 kg/m2) | 1.021 | 0.875 to 1.193 | 1.883 | 0.792 | 0.987 | 0.857 to 1.134 | 1.357 | 0.849 |
| Exercise (≥3 Mets) | 0.307 | 0.104 to 0.833 | 1.108 | 0.025 | 1.028 | 0.266 to 3.729 | 1.166 | 0.967 |
| Current Smoking | 1.244 | 0.301 to 4.991 | 1.295 | 0.757 | 4.608 | 0.159 to 61.720 | 1.097 | 0.280 |
| Hypertension | 1.449 | 0.472 to 4.495 | 1.561 | 0.516 | 1.048 | 0.268 to 4.130 | 1.467 | 0.945 |
| Dyslipidemia | 0.321 | 0.082 to 1.179 | 1.277 | 0.092 | 2.481 | 0.520 to 15.060 | 1.162 | 0.245 |
| Duration of T2D (1 year) | 1.056 | 0.998 to 1.122 | 1.287 | 0.066 | 0.986 | 0.930 to 1.039 | 1.307 | 0.597 |
| SBP (1 mmHg) | 0.974 | 0.940 to 1.008 | 1.472 | 0.139 | 1.014 | 0.982 to 1.040 | 1.337 | 0.297 |
| LDL-C (1 mg/dL) | 0.997 | 0.979 to 1.016 | 1.332 | 0.751 | 0.992 | 0.971 to 1.013 | 1.273 | 0.457 |
| HDL-C (1 mg/dL) | 1.005 | 0.961 to 1.049 | 1.380 | 0.807 | 0.996 | 0.950 to 1.043 | 1.459 | 0.282 |
| TG (1 mg/dL) | 1.005 | 0.998 to 1.014 | 1.462 | 0.199 | 0.995 | 0.984 to 1.006 | 1.548 | 0.370 |
| HbA1c (1%) | 0.847 | 0.547 to 1.180 | 1.346 | 0.369 | 1.048 | 0.688 to 1.492 | 1.258 | 0.812 |
| UA (1 mg/dL) | 1.444 | 0.899 to 2.429 | 1.313 | 0.144 | 0.816 | 0.452 to 1.429 | 1.714 | 0.485 |
| Cr (1 mg/dL) | 0.666 | 0.060 to 2.382 | 1.228 | 0.674 | 0.053 | 0.001 to 1.512 | 1.607 | 0.102 |
| ALB (1 g/dL) | 0.362 | 0.091 to 1.248 | 1.332 | 0.119 | 0.834 | 0.123 to 5.885 | 1.274 | 0.852 |
| DHEAS (1 μg/dL) | 0.985 | 0.975 to 0.993 | 1.366 | 0.001 | 1.008 | 0.999 to 1.016 | 1.298 | 0.059 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yasui, S.; Kaneko, Y.; Yamagami, H.; Hosoki, M.; Hori, T.; Tani, A.; Hara, T.; Kurahashi, K.; Harada, T.; Nakamura, S.; et al. Dehydroepiandrosterone Sulfate, an Adrenal Androgen, Is Inversely Associated with Prevalence of Dynapenia in Male Individuals with Type 2 Diabetes. Metabolites 2023, 13, 1129. https://doi.org/10.3390/metabo13111129
Yasui S, Kaneko Y, Yamagami H, Hosoki M, Hori T, Tani A, Hara T, Kurahashi K, Harada T, Nakamura S, et al. Dehydroepiandrosterone Sulfate, an Adrenal Androgen, Is Inversely Associated with Prevalence of Dynapenia in Male Individuals with Type 2 Diabetes. Metabolites. 2023; 13(11):1129. https://doi.org/10.3390/metabo13111129
Chicago/Turabian StyleYasui, Saya, Yousuke Kaneko, Hiroki Yamagami, Minae Hosoki, Taiki Hori, Akihiro Tani, Tomoyo Hara, Kiyoe Kurahashi, Takeshi Harada, Shingen Nakamura, and et al. 2023. "Dehydroepiandrosterone Sulfate, an Adrenal Androgen, Is Inversely Associated with Prevalence of Dynapenia in Male Individuals with Type 2 Diabetes" Metabolites 13, no. 11: 1129. https://doi.org/10.3390/metabo13111129