
External Validation of the Augmented Renal Clearance Predictor in Critically Ill COVID-19 Patients
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
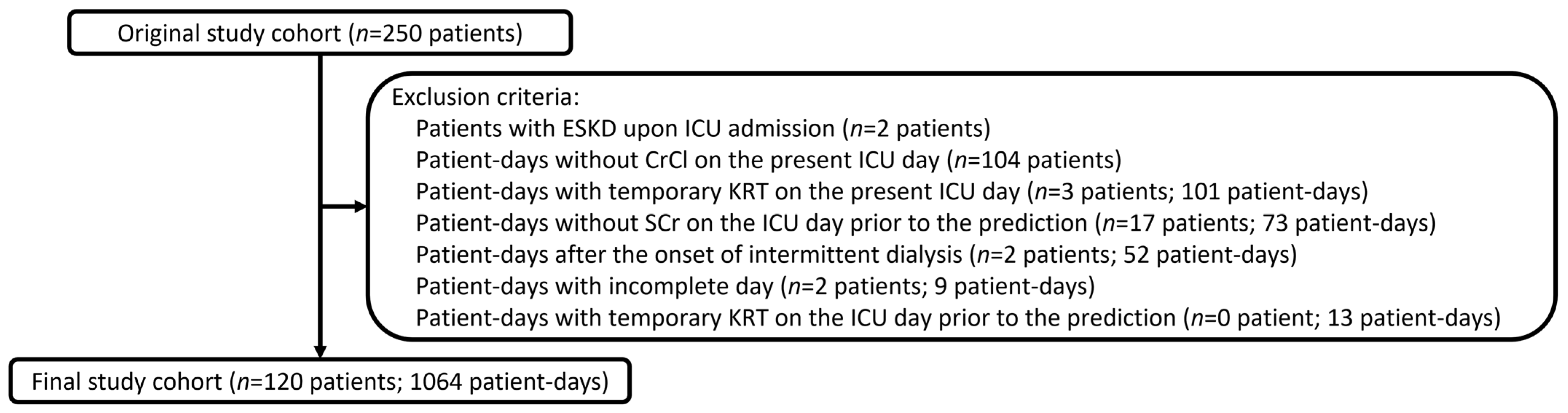
2.1. Study Cohort
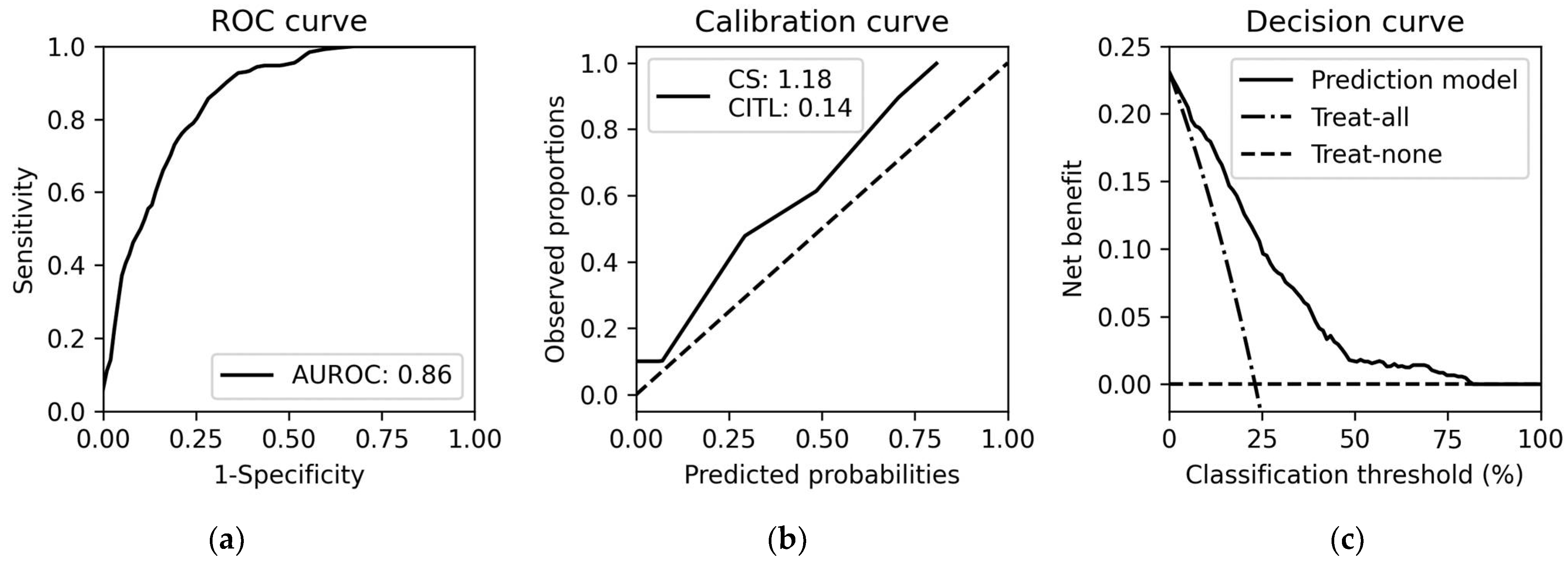
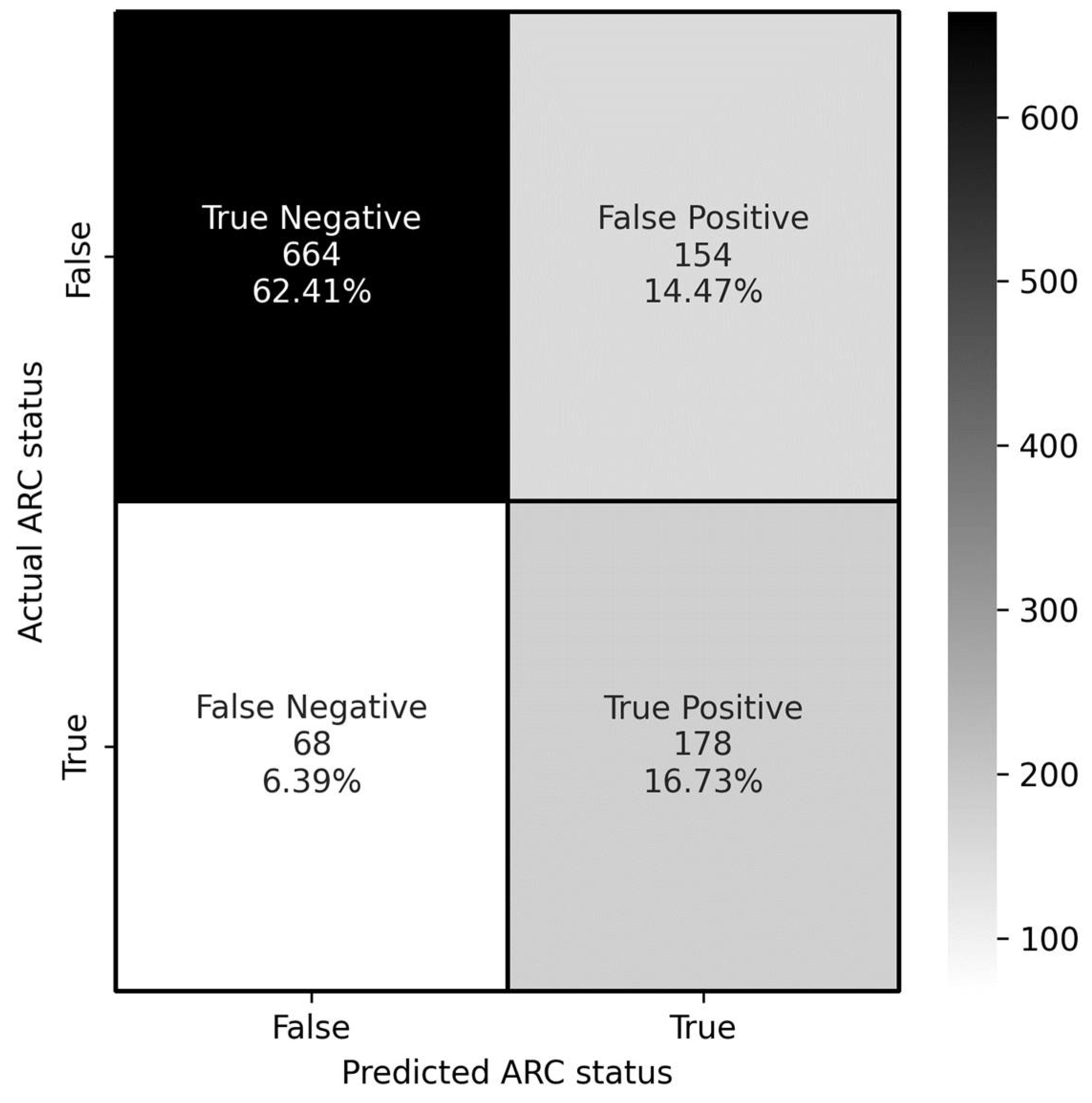
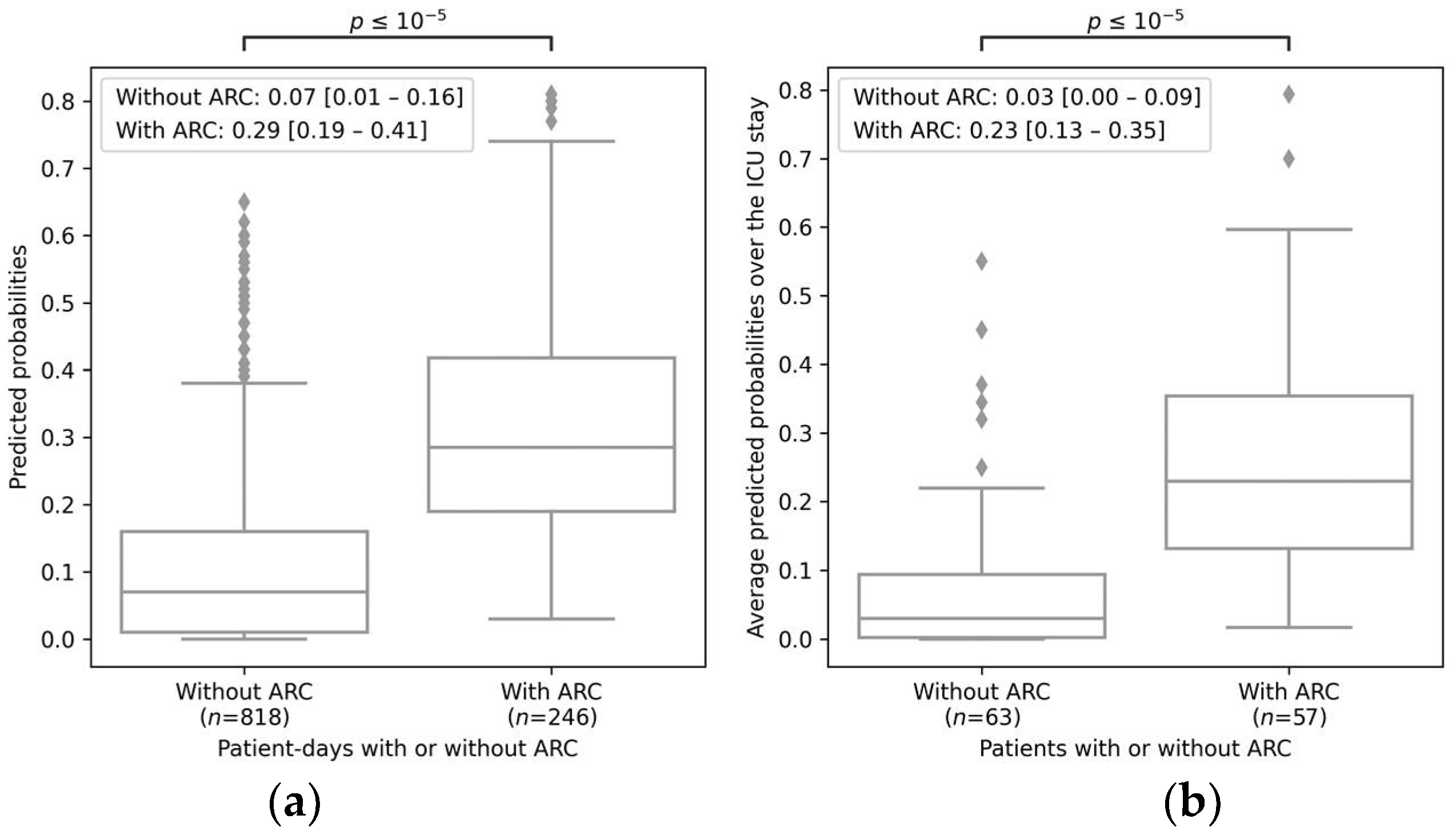
2.2. ARC Predictor External Validation Performance
2.3. ARC Predictor Feature Importance
3. Discussion
4. Materials and Methods
4.1. Study Databases with Inclusion and Exclusion Criteria
4.2. ARC Definition
4.3. ARC Predictor
4.4. Evaluation Metrics for Predictive Performance
4.5. Descriptive Analyses and Software Used
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bilbao-Meseguer, I.; Rodríguez-Gascón, A.; Barrasa, H.; Isla, A.; Solinís, M.Á. Augmented Renal Clearance in Critically Ill Patients: A Systematic Review. Clin. Pharmacokinet. 2018, 57, 1107–1121. [Google Scholar] [CrossRef] [PubMed]
- Cherry, R.A.; Eachempati, S.R.; Hydo, L.; Barie, P.S. Accuracy of Short-Duration Creatinine Clearance Determinations in Predicting 24-Hour Creatinine Clearance in Critically Ill and Injured Patients. J. Trauma: Inj. Infect. Crit. Care 2002, 53, 267–271. [Google Scholar] [CrossRef] [PubMed]
- He, J.; Yang, Z.-T.; Qian, X.; Zhao, B.; Mao, E.-Q.; Chen, E.-Z.; Bian, X.-L. A higher dose of vancomycin is needed in critically ill patients with augmented renal clearance. Transl. Androl. Urol. 2020, 9, 2166–2171. [Google Scholar] [CrossRef]
- Huttner, A.; Von Dach, E.; Renzoni, A.; Huttner, B.D.; Affaticati, M.; Pagani, L.; Daali, Y.; Pugin, J.; Karmime, A.; Fathi, M.; et al. Augmented renal clearance, low beta-lactam concentrations and clinical outcomes in the critically ill: An observational prospective cohort study. Int. J. Antimicrob. Agents 2015, 45, 385–392. [Google Scholar] [CrossRef]
- Udy, A.A.; Varghese, J.M.; Altukroni, M.; Briscoe, S.; McWhinney, B.C.; Ungerer, J.P.; Lipman, J.; Roberts, J.A. Subtherapeutic Initial β-Lactam Concentrations in Select Critically Ill Patients. Chest 2012, 142, 30–39. [Google Scholar] [CrossRef] [PubMed]
- El Naeem, H.E.M.A.; Abdelhamid, M.H.E.; Atteya, D.A.M. Impact of augmented renal clearance on enoxaparin therapy in critically ill patients. Egypt. J. Anaesth. 2017, 33, 113–117. [Google Scholar] [CrossRef] [Green Version]
- Claus, B.O.; Hoste, E.A.; Colpaert, K.; Robays, H.; Decruyenaere, J.; De Waele, J.J. Augmented renal clearance is a common finding with worse clinical outcome in critically ill patients receiving antimicrobial therapy. J. Crit. Care 2013, 28, 695–700. [Google Scholar] [CrossRef]
- Udy, A.A.; Roberts, J.A.; Shorr, A.F.; Boots, R.J.; Lipman, J. Augmented renal clearance in septic and traumatized patients with normal plasma creatinine concentrations: Identifying at-risk patients. Crit. Care 2013, 17, R35. [Google Scholar] [CrossRef] [Green Version]
- Barletta, J.F.; Mangram, A.J.; Byrne, M.; Sucher, J.F.; Hollingworth, A.K.; Ali-Osman, F.R.; Dzandu, J.K. Identifying augmented renal clearance in trauma patients: Validation of the Augmented Renal Clearance in Trauma Intensive Care scoring system. J. Trauma Acute Care Surg. 2017, 82, 665–671. [Google Scholar] [CrossRef]
- Gijsen, M.; Huang, C.-Y.; Flechet, M.; Van Daele, R.; Declercq, P.; Debaveye, Y.; Meersseman, P.; Meyfroidt, G.; Wauters, J.; Spriet, I. Development and External Validation of an Online Clinical Prediction Model for Augmented Renal Clearance in Adult Mixed Critically Ill Patients: The Augmented Renal Clearance Predictor. Crit. Care Med. 2020, 48, e1260–e1268. [Google Scholar] [CrossRef]
- Jabamikos, C.; Fang, Y.T.; Nguyen, K.; Sananikone, A.; Archambault, K.; Bing, E.; Chagnon, M.; Husainalamoodi, O.; Marsot, A.; Duceppe, M.; et al. Validation of the Augmented Renal Clearance in Trauma Intensive Care scoring system for augmented renal clearance prediction in a trauma subgroup of a mixed ICU population. J. Clin. Pharm. Ther. 2022, 47, 1517–1524. [Google Scholar] [CrossRef] [PubMed]
- ARC Prediction. Available online: https://www.arcpredictor.com/ (accessed on 13 April 2022).
- Steyerberg, E.W.; Harrell, F.E., Jr. Prediction models need appropriate internal, internal–external, and external validation. J. Clin. Epidemiol. 2016, 69, 245–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- COVID19-Map–Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 19 May 2022).
- Silver, S.A.; Beaubien-Souligny, W.; Shah, P.S.; Harel, S.; Blum, D.; Kishibe, T.; Meraz-Munoz, A.; Wald, R.; Harel, Z. The Prevalence of Acute Kidney Injury in Patients Hospitalized With COVID-19 Infection: A Systematic Review and Meta-analysis. Kidney Med. 2021, 3, 83–98.e1. [Google Scholar] [CrossRef] [PubMed]
- Rhoney, D.H.P.; Brooks, A.B.; Nelson, N.R. Augmented Renal Clearance: An Under-Recognized Phenomenon Associated With COVID-19. Crit. Care Explor. 2022, 4, e0617. [Google Scholar] [CrossRef]
- Beunders, R.; van de Wijgert, I.H.; Berg, M.V.D.; van der Hoeven, J.G.; Abdo, W.F.; Pickkers, P. Late augmented renal clearance in patients with COVID-19 in the intensive care unit. A prospective observational study. J. Crit. Care 2021, 64, 7–9. [Google Scholar] [CrossRef]
- Nelson, N.; Brooks, A.; Rhoney, D. A Rapid Review of Augmented Renal Clearance in Patients with Covid-19. Crit. Care Med. 2022, 50, 110. [Google Scholar] [CrossRef]
- Dhaese, S.; Peperstraete, H.; Hoste, E.; Van Biesen, W.; De Waele, J. Augmented renal clearance in critically ill COVID-19 patients: Forewarned is forearmed. J. Crit. Care 2021, 66, 93–95. [Google Scholar] [CrossRef]
- Murt, A.; Dincer, M.T.; Karaca, C. Augmented Renal Clearance in COVID-19. Nephron 2021, 145, 386–387. [Google Scholar] [CrossRef]
- Higgins, T.L.; Stark, M.M.; Henson, K.N.; Freeseman-Freeman, L. Coronavirus Disease 2019 ICU Patients Have Higher-Than-Expected Acute Physiology and Chronic Health Evaluation–Adjusted Mortality and Length of Stay Than Viral Pneumonia ICU Patients. Crit. Care Med. 2021, 49, e701–e706. [Google Scholar] [CrossRef]
- Nei, A.M.; Kashani, K.B.; Dierkhising, R.; Barreto, E.F. Predictors of Augmented Renal Clearance in a Heterogeneous ICU Population as Defined by Creatinine and Cystatin C. Nephron 2020, 144, 313–320. [Google Scholar] [CrossRef]
- Udy, A.A.; Dulhunty, J.M.; Roberts, J.A.; Davis, J.S.; Webb, S.A.R.; Bellomo, R.; Gomersall, C.; Shirwadkar, C.; Eastwood, G.M.; Myburgh, J.; et al. Association between augmented renal clearance and clinical outcomes in patients receiving beta-lactam antibiotic therapy by continuous or intermittent infusion: A nested cohort study of the BLING-II randomised, placebo-controlled, clinical trial. Int. J. Antimicrob. Agents 2017, 49, 624–630. [Google Scholar] [CrossRef] [PubMed]
- Kawano, Y.; Maruyama, J.; Hokama, R.; Koie, M.; Nagashima, R.; Hoshino, K.; Muranishi, K.; Nakashio, M.; Nishida, T.; Ishikura, H. Outcomes in patients with infections and augmented renal clearance: A multicenter retrospective study. PLoS ONE 2018, 13, e0208742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulder, M.B.; Eidelson, S.A.; Sussman, M.S.; Schulman, C.I.; Lineen, E.B.; Iyenger, R.S.; Namias, N.; Proctor, K.G. Risk Factors and Clinical Outcomes Associated with Augmented Renal Clearance in Trauma Patients. J. Surg. Res. 2019, 244, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Nazer, L.H.; AbuSara, A.K.; Kamal, Y. Augmented renal clearance in critically ill patients with cancer (ARCCAN Study): A prospective observational study evaluating prevalence and risk factors. Pharmacol. Res. Perspect. 2021, 9, e00747. [Google Scholar] [CrossRef]
- Johnston, B.W.; Perry, D.; Habgood, M.; Joshi, M.; Krige, A. Augmented renal clearance: A retrospective, cohort study of urinary creatinine clearance in critically ill patients in the United Kingdom. J. Int. Med. Res. 2021, 49, 19–32. [Google Scholar] [CrossRef]
- Baptista, J.P.; Martins, P.J.; Marques, M.; Pimentel, J.M. Prevalence and Risk Factors for Augmented Renal Clearance in a Population of Critically Ill Patients. J. Intensiv. Care Med. 2020, 35, 1044–1052. [Google Scholar] [CrossRef]
- Dickerson, R.N.; Crawford, C.N.; Tsiu, M.K.; Bujanowski, C.E.; Van Matre, E.T.; Swanson, J.M.; Filiberto, D.M.; Minard, G. Augmented Renal Clearance Following Traumatic Injury in Critically Ill Patients Requiring Nutrition Therapy. Nutrients 2021, 13, 1681. [Google Scholar] [CrossRef]
- Wu, C.-C.; Tai, C.H.; Liao, W.-Y.; Wang, C.-C.; Kuo, C.-H.; Lin, S.-W.; Ku, S.-C. Augmented renal clearance is associated with inadequate antibiotic pharmacokinetic/pharmacodynamic target in Asian ICU population: A prospective observational study. Infect. Drug Resist. 2019, 12, 2531–2541. [Google Scholar] [CrossRef] [Green Version]
- De Waele, J.J.; Dumoulin, A.; Janssen, A.; Hoste, E.A.J. Epidemiology of augmented renal clearance in mixed ICU patients. Minerva Anestesiol. 2015, 81, 1079–1085. [Google Scholar]
- Udy, A.A.; Baptista, J.P.; Lim, N.L.; Joynt, G.M.; Jarrett, P.; Wockner, L.; Boots, R.J.; Lipman, J. Augmented Renal Clearance in the ICU: Results of a Multicenter Observational Study of Renal Function in Critically Ill Patients with Normal Plasma Creatinine Concentrations. Crit. Care Med. 2014, 42, 520–527. [Google Scholar] [CrossRef]
- Bing, E.; Archambault, K.; Sananikone, A.; Nguyen, K.-D.; Fang, Y.T.; Jabamikos, C.; Gras, C.; Marsot, A.; Duceppe, M.-A.; Perreault, M.M. Risk factors associated with augmented renal clearance in a mixed intensive care unit population: A retrospective study. Int. J. Clin. Pharm. 2022, 44, 1277–1286. [Google Scholar] [CrossRef] [PubMed]
- Twohig, A.K.; Nyberg, T.; Zaidi, A.; Thelwall, S.; Sinnathamby, A.M.; Aliabadi, S.; Seaman, S.R.; Harris, R.J.; Hope, R.; Lopez-Bernal, J.; et al. Hospital admission and emergency care attendance risk for SARS-CoV-2 delta (B.1.617.2) compared with alpha (B.1.1.7) variants of concern: A cohort study. Lancet Infect. Dis. 2022, 22, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Chadeau-Hyam, M.; Wang, H.; Eales, O.; Haw, D.; Bodinier, B.; Whitaker, M.; Walters, E.C.; Ainslie, K.E.C.; Atchison, C.; Fronterre, C.; et al. SARS-CoV-2 infection and vaccine effectiveness in England (REACT-1): A series of cross-sectional random community surveys. Lancet Respir. Med. 2022, 10, 355–366. [Google Scholar] [CrossRef] [PubMed]
- Steyerberg, E.W.; Vergouwe, Y. Towards better clinical prediction models: Seven steps for development and an ABCD for validation. Eur. Heart J. 2014, 35, 1925–1931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moons, K.G.M.; Altman, D.G.; Reitsma, J.B.; Ioannidis, J.P.A.; Macaskill, P.; Steyerberg, E.W.; Vickers, A.J.; Ransohoff, D.F.; Collins, G.S. Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD): Explanation and Elaboration. Ann. Intern. Med. 2015, 162, W1–W73. [Google Scholar] [CrossRef] [Green Version]
- Steyerberg, E.W. Clinical Prediction Models. Statistics for Biology and Health; Springer: New York, NY, USA, 2009; pp. 255–280. [Google Scholar]
- Vickers, A.J.; Elkin, E.B. Decision Curve Analysis: A Novel Method for Evaluating Prediction Models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Random Forests. Available online: https://www.stat.berkeley.edu/~breiman/RandomForests/ (accessed on 19 May 2022).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 120) | ARC (n = 57, 47.50%) | Not ARC (n = 63, 52.50%) | p-Value |
|---|---|---|---|---|
| Age, years, median (IQR) | 67 (59–75) | 61 (57–67) | 73 (65–78) | <0.01 |
| Sex male, number (%) | 87 (72.5) | 40 (70.2) | 47 (74.6) | 0.59 |
| Height, m, median (IQR) | 1.7 (1.6–1.8) | 1.8 (1.7–1.8) | 1.7 (1.6–1.8) | 0.03 |
| Weight, kg, median (IQR) | 85.0 (71.5–104.0) | 86.0 (70.0–104.0) | 85.0 (73.5–101.5) | 0.63 |
| BMI, median (IQR) | 28.7 (25.8–33.1) | 28.1 (26.1–32.8) | 29.0 (25.8–34.3) | 0.71 |
| Baseline serum creatinine, mg/dL, median (IQR) | 0.9 (0.8–1.0) | 0.9 (0.7–0.9) | 0.9 (0.9–1.1) | <0.01 |
| APACHE II score, median (IQR) | 19 (15–25) | 18 (13–23) | 19 (17–27) | <0.01 |
| Day from ICU admission, day, median (IQR) | 6.0 (3.5–10.0) | 6.5 (4.0–10.0) | 6.0 (3.2–10.5) | 0.73 |
| Creatinine clearance, mL/min/1.73 m2, median (IQR) | 91.3 (54.7–132.5) | 133.8 (106.4–165.0) | 55.9 (27.8–81.9) | <0.01 |
| Length of stay in ICU, days, median (IQR) | 14 (9–24) | 15 (8–24) | 14 (10–24) | 0.11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, C.-Y.; Güiza, F.; Gijsen, M.; Spriet, I.; Dauwe, D.; Debaveye, Y.; Peetermans, M.; Wauters, J.; Van den Berghe, G.; Meyfroidt, G.; et al. External Validation of the Augmented Renal Clearance Predictor in Critically Ill COVID-19 Patients. Antibiotics 2023, 12, 698. https://doi.org/10.3390/antibiotics12040698
Huang C-Y, Güiza F, Gijsen M, Spriet I, Dauwe D, Debaveye Y, Peetermans M, Wauters J, Van den Berghe G, Meyfroidt G, et al. External Validation of the Augmented Renal Clearance Predictor in Critically Ill COVID-19 Patients. Antibiotics. 2023; 12(4):698. https://doi.org/10.3390/antibiotics12040698
Chicago/Turabian StyleHuang, Chao-Yuan, Fabian Güiza, Matthias Gijsen, Isabel Spriet, Dieter Dauwe, Yves Debaveye, Marijke Peetermans, Joost Wauters, Greet Van den Berghe, Geert Meyfroidt, and et al. 2023. "External Validation of the Augmented Renal Clearance Predictor in Critically Ill COVID-19 Patients" Antibiotics 12, no. 4: 698. https://doi.org/10.3390/antibiotics12040698