

Beta-Lactam Probability of Target Attainment Success: Cefepime as a Case Study

Abstract
:1. Introduction
2. Results
2.1. Description of PTA Studies
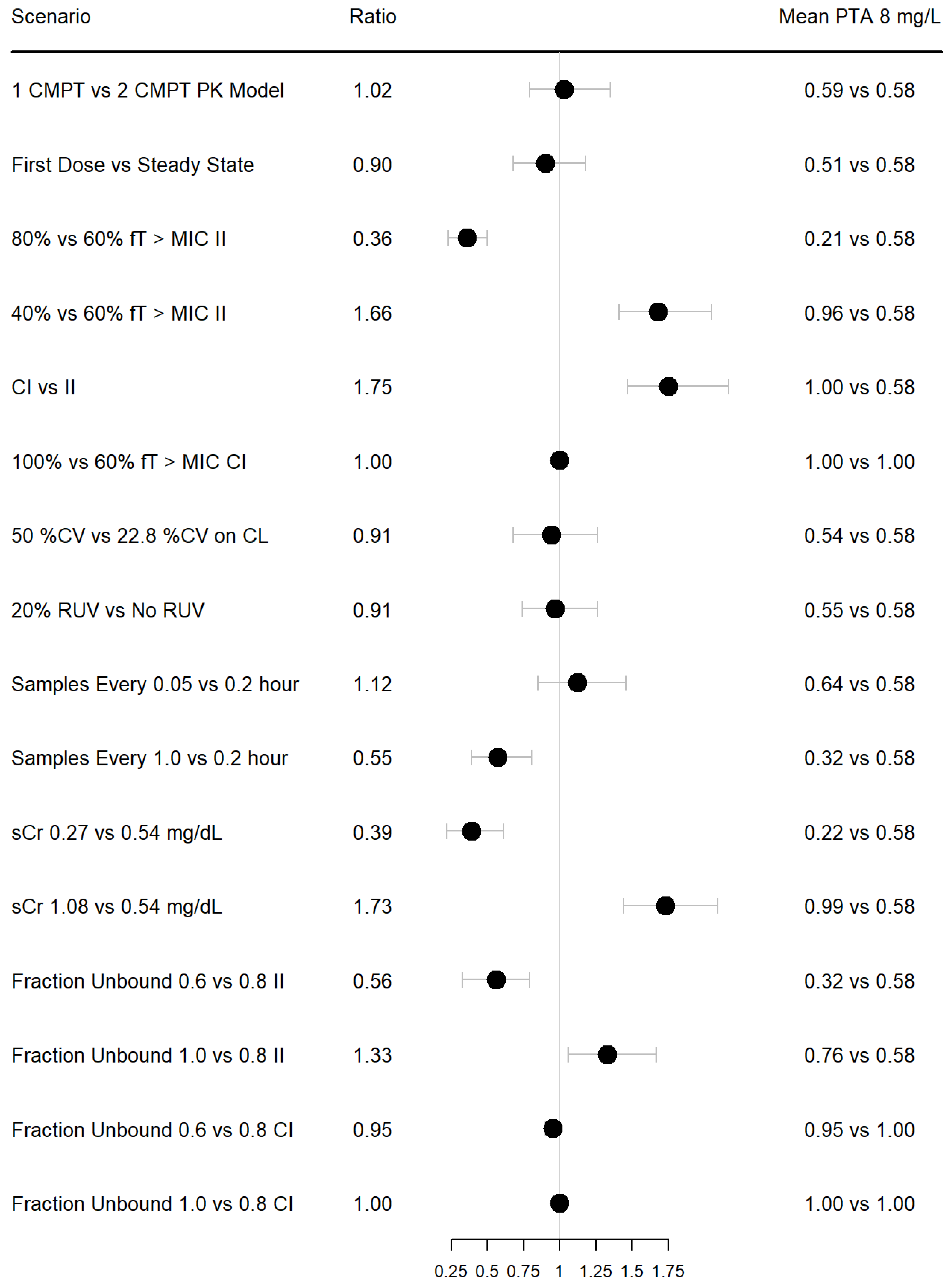
2.2. Results of PTA Simulations
3. Discussion
4. Materials and Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sherwin, C.M.; Kiang, T.K.; Spigarelli, M.G.; Ensom, M.H. Fundamentals of population pharmacokinetic modelling: Validation methods. Clin. Pharmacokinet. 2012, 51, 573–590. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.S.; Yuan, M.; Zhu, H.; Yang, Y.; Wang, H.; Zhou, H.; Xu, J.; Zhang, L.; Pinheiro, J. Full covariate modelling approach in population pharmacokinetics: Understanding the underlying hypothesis tests and implications of multiplicity. Br. J. Clin. Pharmacol. 2018, 84, 1525–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Zhu, H.; Madabushi, R.; Liu, Q.; Huang, S.; Zineh, I. Model-informed drug development: Current US regulatory practice and future considerations. Clin. Pharmacol. Ther. 2019, 105, 899–911. [Google Scholar] [CrossRef]
- Onufrak, N.J.; Forrest, A.; Gonzalez, D. Pharmacokinetic and pharmacodynamic principles of anti-infective dosing. Clin. Ther. 2016, 38, 1930–1947. [Google Scholar] [CrossRef] [Green Version]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients-guidelines from the French Society of Pharmacology and Therapeutics (Societe Francaise de Pharmacologie et Therapeutique-SFPT) and the French Society of Anaesthesia and Intensive Care Medicine (Societe Francaise d’Anesthesie et Reanimation-SFAR). Crit. Care 2019, 23, 104. [Google Scholar] [PubMed] [Green Version]
- Póvoa, P.; Moniz, P.; Pereira, J.; Coelho, L. Optimizing antimicrobial drug dosing in critically ill patients. Microorganisms 2021, 9, 1401. [Google Scholar] [CrossRef] [PubMed]
- Scharf, C.; Liebchen, U.; Paal, M.; Taubert, M.; Vogeser, M.; Irlbeck, M.; Zoller, M.; Schroeder, I. The higher the better? Defining the optimal beta-lactam target for critically ill patients to reach infection resolution and improve outcome. J. Intensiv. Care 2020, 8, 86. [Google Scholar] [CrossRef]
- Mouton, J.W.; Dudley, M.N.; Cars, O.; Derendorf, H.; Drusano, G.L. Standardization of pharmacokinetic/pharmacodynamic (PK/PD) terminology for anti-infective drugs: An update. J. Antimicrob. Chemother. 2005, 55, 601–607. [Google Scholar] [CrossRef] [Green Version]
- Shorr, A.F.; Bruno, C.J.; Zhang, Z.; Jensen, E.; Gao, W.; Feng, H.-P.; Huntington, J.A.; Yu, B.; Rhee, E.G.; De Anda, C.; et al. Ceftolozane/tazobactam probability of target attainment and outcomes in participants with augmented renal clearance from the randomized phase 3 ASPECT-NP trial. Crit. Care 2021, 25, 354. [Google Scholar] [CrossRef]
- Por, E.D.; Akers, K.S.; Chung, K.K.; Livezey, J.R.; Selig, D.J. Population pharmacokinetic modeling and simulations of imipenem in burn patients with and without continuous venovenous hemofiltration in the military health system. J. Clin. Pharmacol. 2021, 61, 1182–1194. [Google Scholar] [CrossRef]
- Selig, D.J.; Akers, K.S.; Chung, K.K.; Pruskowski, K.A.; Livezey, J.R.; Por, E.D. Meropenem pharmacokinetics in critically ill patients with or without burn treated with or without continuous veno-venous haemofiltration. Br. J. Clin. Pharmacol. 2021, 88, 2156–2168. [Google Scholar] [CrossRef] [PubMed]
- Bakdach, D.; Elajez, R.; Bakdach, A.R.; Awaisu, A.; De Pascale, G.; Ait Hssain, A. Pharmacokinetics, pharmacodynamics, and dosing considerations of novel beta-lactams and beta-lactam/beta-lactamase inhibitors in critically ill adult patients: Focus on obesity, augmented renal clearance, renal replacement therapies, and extracorporeal membrane oxygenation. J. Clin. Med. 2022, 11, 6898. [Google Scholar] [PubMed]
- Kidd, J.M.; Stein, G.E.; Nicolau, D.P.; Kuti, J.L. Monte Carlo Simulation methodologies for beta-lactam/beta-lactamase inhibitor combinations: Effect on probability of target attainment assessments. J. Clin. Pharmacol. 2020, 60, 172–180. [Google Scholar] [CrossRef] [PubMed]
- Sember, A.M.; LoFaso, M.E.; Lewis, S.J. An optimal extended-infusion dosing of cefepime and ceftazidime in critically ill patients with continuous renal replacement therapy. J. Crit Care 2022, 69, 154011. [Google Scholar] [CrossRef]
- Jang, S.-M.; Shaw, A.R.; Mueller, B.A. Size matters: The influence of patient size on antibiotics exposure profiles in critically ill patients on continuous renal replacement therapy. Antibiotics 2021, 10, 1390. [Google Scholar] [CrossRef]
- Lau, C.; Marriott, D.; Schultz, H.B.; Gould, M.; Andresen, D.; Wicha, S.G.; Alffenaar, J.-W.; Penm, J.; Reuter, S.E. Assessment of cefepime toxicodynamics: Comprehensive examination of pharmacokinetic/pharmacodynamic targets for cefepime-induced neurotoxicity and evaluation of current dosing guidelines. Int. J. Antimicrob. Agents 2021, 58, 106443. [Google Scholar] [CrossRef]
- Álvarez, J.C.; Cuervo, S.I.; Silva, E.; Díaz, J.A.; Jiménez, L.L.; Parra, D.S.; Gómez, J.C.; Sánchez, R.; Cortés, J.A. Pharmacokinetics and pharmacodynamics of cefepime in adults with hematological malignancies and febrile neutropenia after chemotherapy. Antibiotics 2021, 10, 504. [Google Scholar] [CrossRef]
- Liu, J.; Rhodes, N.J.; Roberts, J.A.; Pais, G.M.; Turner, B.; Kiel, P.J.; Scheetz, M.H. β-lactam dosing strategies: Think before you push. Int. J. Antimicrob. Agents 2020, 56, 106151. [Google Scholar] [CrossRef]
- Delattre, I.K.; Hites, M.; Laterre, P.-F.; Dugernier, T.; Spapen, H.; Wallemacq, P.E.; Jacobs, F.; Taccone, F.S. What is the optimal loading dose of broad-spectrum β-lactam antibiotics in septic patients? Results from pharmacokinetic simulation modelling. Int. J. Antimicrob. Agents 2020, 56, 106113. [Google Scholar] [CrossRef]
- Wang, C.; Bai, Y.; Li, R.; Shen, C.; Zhang, J. Use of Monte Carlo simulation to optimize antibiotic selection for bloodstream infections caused by Enterobacteriaceae in Shandong Province, China. Diagn. Microbiol. Infect. Dis. 2020, 97, 115039. [Google Scholar] [CrossRef]
- Huang, C.; Shi, Q.; Zheng, B.; Ji, J.; Ying, C.; Yu, X.; Wang, H.; Xiao, Y. Simulating moxalactam dosage for extended-spectrum β-lactamase-producing Enterobacteriaceae using blood antimicrobial surveillance network data. Infect. Drug Resist. 2019, 12, 1199–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaijamorn, W.; Charoensareerat, T.; Srisawat, N.; Pattharachayakul, S.; Boonpeng, A. Cefepime dosing regimens in critically ill patients receiving continuous renal replacement therapy: A Monte Carlo simulation study. J. Intensiv. Care 2018, 6, 61. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.R.; Mueller, B.A. Antibiotic dosing in continuous renal replacement therapy. Adv. Chronic Kidney Dis. 2017, 24, 219–227. [Google Scholar] [CrossRef]
- Rhodes, N.J.; Grove, M.E.; Kiel, P.J.; O’Donnell, J.N.; Whited, L.K.; Rose, D.T.; Jones, D.R.; Scheetz, M.H. Population pharmacokinetics of cefepime in febrile neutropenia: Implications for dose-dependent susceptibility and contemporary dosing regimens. Int. J. Antimicrob. Agents 2017, 50, 482–486. [Google Scholar] [CrossRef] [PubMed]
- Butterfield-Cowper, J.M.; Burgner, K. Effects of i.v. push administration on β-lactam pharmacodynamics. Am. J. Health Syst. Pharm. 2017, 74, e170–e175. [Google Scholar] [CrossRef] [PubMed]
- Koomanachai, P.; Yungyuen, T.; Disthaporn, P.; Kiratisin, P.; Nicolau, D.P. Application of pharmacodynamic profiling for the selection of optimal β-lactam regimens in a large university hospital. Int. J. Infect. Dis. 2016, 46, 22–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, R.Z.; Martin, C.A.; Burgess, D.R.; Rutter, W.C.; Burgess, D.S. Optimizing beta-lactam pharmacodynamics against Pseudomonas aeruginosa in adult cystic fibrosis patients. J. Cyst. Fibros. 2016, 15, 660–663. [Google Scholar] [CrossRef] [Green Version]
- Das, S.; Fitzgerald, R.; Ullah, A.; Bula, M.; Collins, A.M.; Mitsi, E.; Reine, J.; Hill, H.; Rylance, J.; Ferreira, D.M.; et al. Intrapulmonary pharmacokinetics of cefepime and enmetazobactam in healthy volunteers: Towards new treatments for nosocomial pneumonia. Antimicrob. Agents Chemother. 2020, 65, e01468-20. [Google Scholar] [CrossRef]
- Jang, S.M.; Pai, M.P.; Shaw, A.R.; Mueller, B.A. Antibiotic Exposure profiles in trials comparing intensity of continuous renal replacement therapy. Crit. Care Med. 2019, 47, e863–e871. [Google Scholar] [CrossRef]
- Jang, S.M.; Gharibian, K.N.; Lewis, S.J.; Fissell, W.H.; Tolwani, A.J.; Mueller, B.A. A Monte Carlo simulation approach for beta-lactam dosing in critically ill patients receiving prolonged intermittent renal replacement therapy. J. Clin. Pharmacol. 2018, 58, 1254–1265. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.B.; Lusk, K.A.; Cota, J.M. The role of cefepime in the treatment of extended-spectrum beta-lactamase infections. J. Pharm. Pract. 2017, 32, 458–463. [Google Scholar] [CrossRef]
- Hirai, K.; Ishii, H.; Shimoshikiryo, T.; Shimomura, T.; Tsuji, D.; Inoue, K.; Kadoiri, T.; Itoh, K. Augmented renal clearance in patients with febrile neutropenia is associated with increased risk for subtherapeutic concentrations of vancomycin. Ther. Drug Monit. 2016, 38, 706–710. [Google Scholar] [CrossRef]
- Alzahrani, A.M.; Hakami, A.Y.; AlAzmi, A.; Karim, S.; Ali, A.S.; Burzangi, A.S.; Alkreathy, H.M.; Khan, M.A.; Alzhrani, R.M.; Basudan, S.S.; et al. Augmented renal clearance and hypoalbuminemia-induced low vancomycin trough concentrations in febrile neutropenic patients with hematological malignancies. Cureus 2022, 14, e29568. [Google Scholar] [CrossRef]
- Nelson, N.R.; Mendoza, C.; Rhoney, D.H. Augmented renal clearance in the hematology and oncology populations: A scoping review for pharmacists. J. Pharm. Pract. 2022, 08971900221121362. [Google Scholar] [CrossRef]
- CLSI M100-ED32; Performance Standards for Antimicrobial Susceptibility Testing. 32nd ed. Institute CaLS: Gainesville, FL, USA, 2022. Available online: http://em100.edaptivedocs.net/GetDoc.aspx?doc=CLSI%20M100%20ED32,2022&sbssok=CLSI%20M100%20ED32,2022%20TABLE%202B-1&format=HTML#CLSI%20M100%20ED32,2022%20TABLE%202B-1 (accessed on 16 January 2023).
- Hospira. Cefepime [Package Insert]; Hospira Inc.: Lake Forest, IL, USA, 1996. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/050679s042lbl.pdf (accessed on 16 January 2023).
- Barbhaiya, R.H.; Knupp, C.A.; Forgue, S.T.; Matzke, G.R.; Guay, D.R.P.; Pittman, K.A. Pharmacokinetics of cefepime in subjects with renal insufficiency. Clin. Pharmacol. Ther. 1990, 48, 268–276. [Google Scholar] [CrossRef]
- Masich, A.M.; Heavner, M.S.; Gonzales, J.P.; Claeys, K.C. Pharmacokinetic/pharmacodynamic considerations of beta-lactam antibiotics in adult critically ill patients. Curr. Infect. Dis. Rep. 2018, 20, 9. [Google Scholar] [CrossRef]
- Kollef, M.H.; Shorr, A.F.; Bassetti, M.; Timsit, J.-F.; Micek, S.T.; Michelson, A.P.; Garnacho-Montero, J. Timing of antibiotic therapy in the ICU. Crit. Care 2021, 25, 360. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.A.; Paul, S.K.; Akova, M.; Bassetti, M.; De Waele, J.J.; Dimopoulos, G.; Kaukonen, K.M.; Koulenti, D.; Martin, C.; Montravers, P.; et al. DALI: Defining antibiotic levels in intensive care unit patients: Are current beta-lactam antibiotic doses sufficient for critically ill patients? Clin. Infect. Dis. 2014, 58, 1072–1083. [Google Scholar] [CrossRef] [PubMed]
- Jean-Michel, V.; Homey, C.; Devos, P.; Delannoy, P.-Y.; Boussekey, N.; Caulier, T.; Leroy, O.; Georges, H. Continuous infusion of high doses of cefepime in intensive care unit: Assessment of steady-state plasma level and incidence on neurotoxicity. Antibiotics 2022, 12, 69. [Google Scholar] [CrossRef]
- Laboratory, J. SENTRY MVP Microbiology Visualization Platform 2023. Available online: https://sentry-mvp.jmilabs.com/ (accessed on 17 January 2023).
- Rackauckas, C.; Ma, Y.; Noack, A.; Dixit, V.; Mogensen, P.K.; Byrne, S.; Maddhashiya, S.; Santiago Calderón, J.B.; Nyberg, J.; Gobburu, J.V.; et al. Accelerated predictive healthcare analytics with pumas, a high performance pharmaceutical modeling and simulation platform. bioRxiv 2020. [Google Scholar] [CrossRef]


{kind=link}
| Study | Simulated Population | tvCL in Model | Simulated Doses | PD Target and Definition of Success | TD Target | Assumed Fraction Unbound | Simulation of PK Parameters | Simulated Time Intervals | Final Dose Recommendation |
|---|---|---|---|---|---|---|---|---|---|
| Álvarez | 2500 patients with hematologic malignancy | 13.6 L/h scaled to sCR of 0.47 | 4–8 G/day as 30-min infusions, extended infusions or continuous infusions | fT 60% or 100% > MIC = 4 mg/L or 8 mg/L. PTA 90% | Toxicity not analyzed | 0.8, fixed | Pop PK model developed from plasma samples of 15 patients | Not specified, first 24 h and at steady state | 2 G q 8 with extended 4-h infusions achieves lenient PD target and 6 g/day CI achieves all targets. |
| Butterfield-Cowper | 5000 patients | 5.43 L/h scaled to CrCl of 80 mL/min | 30-min and 5-min infusions of 1 G q 6 h and 2 G q 8 h | 70% fT 70% > 1 × MIC at hour 24 of therapy | Toxicity not analyzed | 0.8, fixed | 2-cmpt pop PK model developed by Tam et al. | Not specified | Minimal difference in PK profile from 30-min to. 5-min infusion. |
| Chaijamorn | 5000 anuric CKRT patients | 1.46 L/h (patients assumed to be anuric) | 1 to 2 g every 12 h to 2 g loading dose followed by 1 g every 8 h or 2 g every 12 h | ≥70% fT > 4 × MIC = 8 mg/L in a 48-h time period. PTA 90% | Probability of trough >= 70 mg/L at end of 48-h interval | 0.79, simulated with mean and SD | Log-normal distribution based on 1-compartment PK model developed via a literature search | Not specified, initial 48 h | 1.75–2 G loading dose followed by 1.5–2 G q 8 h. |
| Delattre | 1000 patients per group | 4.5 L/h scaled to CrCl of 100 mL/min and weight of 70 kg | 4 g or 6 g administered as a 0.5-h, 2-h or 3-h infusion every 8 h | 70%T > 4 × MIC ≤8 mg/L within a dosing interval. PTA 90% | Toxicity not analyzed | 1, fixed | Pop PK developed from 88 critically ill patients | Not stated | 4 G loading dose infused over 3 h followed by 4 G q 6 h. |
| Huang | 10,000 healthy patients | 5.3 L/h corresponds to CrCl of 100–120 mL/min (need to follow up on Nye et al.) | 1 g every 12 h (q 12 h), 1 g every 8 h (q 8 h), 2 g q 12 h, and 2 g q 8 h as an IV bolus (an assumption for the equation to generate %fT > MIC) | fT 50% ≥ MIC based on observed MIC distribution and 90% CFR defined as success | Toxicity not analyzed | 0.8–0.9 uniformly distributed. | CL estimated from a study of healthy volunteers Nye et al., %fT generated from an equation. | Equation used, steady state | 2 G q 8 h IV bolus PTA achieved > 90% to MIC 16 mg/L; however, adequate for non-esbls, not adequate for esbl based on CFR |
| Jang | 10,000 patients receiving CRRT | 1.46 L/h (assumed to be anuric) | Cefepime 1 and 2-g q 8 or q 12 h over 30-min infusion | fT 60% ≥ MIC of 8 mg/L (also 4XMIC tested) in 72-h time period. PTA 90% | Toxicity not analyzed | 0.79, fixed | Log-normal distribution based on 1-compartment PK model developed via a literature search | Not stated, 72 h of initial therapy | No dose recommendation, 2 G q 8 achieved > 90% PTA in all simulated subgroups. |
| Lau | 12,000 patients | 2.29 L/h scaled to CrCl 60 mL/min with linear model | Per Australian dosing guidelines | Cmin > 32 mg/L. PTA 90% | 49 mg/L derived via ROC analysis | Not specified, assumed to be 1 | Via population PK model developed by Jonckheere et al. | Cmin at steady state | No recommendation, 89% of patients with CrCl > 50 mL/min would achieve PTA dosing of 2 G q 8 h. |
| Liu | 1000 patients per group, fixed at 70 kg and varied CrCl | 5.65 L/h scaled to CrCL 120 mL/min and 70 kg | 1–2 G q 8–12 as 2-, 5- or 30-min infusions | 70%fT > MIC. CFR based on SENTRY database of MIC distributions. PTA 90%, CFR 90% | Toxicity not analyzed | 0.8, fixed | Pop PK model developed from 70 patients and 604 cefepime concentrations | Not specified, evaluated 1st dose | IVP is not likely to be as good as intermittent infusion. No regimen meets the 90% threshold for MIC > 8 mg/L in patients with CrCl > 60, but CFR is > 90% for 2 G q 8 h based on MIC distributions. |
| Koomanachai | 5000 patients | 6.04 L/h scaled to CrCl 103.74 mL/min per equation in Tam et al. | 2 g every 12 h (0.5-h infusion) or 2 g every 8 h (0.5-h and 3-h infusion) | ≥50% fT > MIC. CFR >= 90% against observed MIC distribution | Toxicity not analyzed | Not stated | Simulated used Tam et al. | Not stated, steady state | 2 g q 8 h infused over 3 h achieved CFR > 80–90% |
| Rhodes | 10,000 patients with CrCl simulated range 108–220 mL/min | 6.33 L/h scaled to CrCl of 120 m/min | 3–8 G/day infused over 0.5–24 h q6–12 h or CI | ≥68% fT > 1 × MIC in first 24 h of therapy. PTA 90% | Toxicity not analyzed | 0.8, fixed | 2-cmpt Pop PK model developed via cefepime concentration data from 9 patients | Simulated every 0.5 h, first 24 h of therapy | 3–4 g/day as continuous infusions and doses of 2 g administered q 6 h (0.5-h infusion) to q 8 h (2-h infusion) |
| Sember | 5000 anuric patients receiving CRRT | 1.46 L/h (patients assumed to be anuric) | 2-g loading dose (LD) infused over 0.5 h, followed by 1 or 2-g every 8 or 12 h with a 4-h extended-infusion. | ≥60% fT > 4 × MIC = 8 mg/L in a 48-h time period. PTA 90% | Probability of trough >= 20 mg/L at end of 48-h interval | 0.79, fixed | Log-normal distribution based on 1-compartment PK model developed via a literature search | Every 0.1 h for initial 48 h | 2 G load followed by 2 G q 8 h |
| Shaw | 5000 anuric patients receiving CRRT | 1.49 L/h (patients assumed to be anuric) | 1 to 2 g every 8–12 h to 2 g with or without load 2 G loading dose | ≥60% fT > 1 × MIC or 4 × MIC = 8 mg/L in a 48-h time period. PTA 90% | Toxicity not analyzed | 0.79, fixed | Log-normal distribution based on 1-compartment PK model developed via a literature search | Not specified, initial 72 h | No recommendation, but 2 G q 12 achieved 100% PTA in lenient target and 88.58% in strict target. |
| Thompson | 10,000 patients with Cystic Fibrosis | 8.47 L/h scaled to CrCl of 111.11 mL/min | 2 g every 8 h (bolus and prolonged infusion) | ≥60% or 100% fT > MIC against observed MIC distribution in CF patients (MIC50 = 16 mg/L). PTA 90%. | Toxicity not analyzed | 0.8, fixed | Simulated via equations using steady state CL from Huls et al. | Equations used N/A | 2 G CI achieves 66% PTA success and therefore is not adequate to cover resistant pseudomonal strains in CF population |
| Wang | 5000 patients with CrCl >= 50 mL/min | 9.18 L/h, which scales to a CrCl of 166.25 mL/min as calculated from Nicasio’s equation for CLT = 0.048 × CLCR + 1.2 | 1 g q 12 h or 2 g q 12 h as 30-min infusion or 2 g q 12 h as 3-h infusion | 50% fT > MIC within dosing interval based on observed MIC distribution with CFR 90% defined as success | Toxicity not analyzed | 0.85, fixed | Used Pop PK developed by Nicasio et al. | Not stated, evaluated at steady state | 2 g q 12 h, 3 h; and cefepime 2 g q 12 h, 0.5 h had CFR of 80–90% which was considered suboptimal and therefore other antibiotics were recommended. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Selig, D.J.; Kress, A.T.; Nadeau, R.J.; DeLuca, J.P. Beta-Lactam Probability of Target Attainment Success: Cefepime as a Case Study. Antibiotics 2023, 12, 444. https://doi.org/10.3390/antibiotics12030444
Selig DJ, Kress AT, Nadeau RJ, DeLuca JP. Beta-Lactam Probability of Target Attainment Success: Cefepime as a Case Study. Antibiotics. 2023; 12(3):444. https://doi.org/10.3390/antibiotics12030444
Chicago/Turabian StyleSelig, Daniel J., Adrian T. Kress, Robert J. Nadeau, and Jesse P. DeLuca. 2023. "Beta-Lactam Probability of Target Attainment Success: Cefepime as a Case Study" Antibiotics 12, no. 3: 444. https://doi.org/10.3390/antibiotics12030444