

Evaluation of Dosing Guidelines for Gentamicin in Neonates and Children
 , , and
, , and
Abstract
:1. Introduction
2. Results
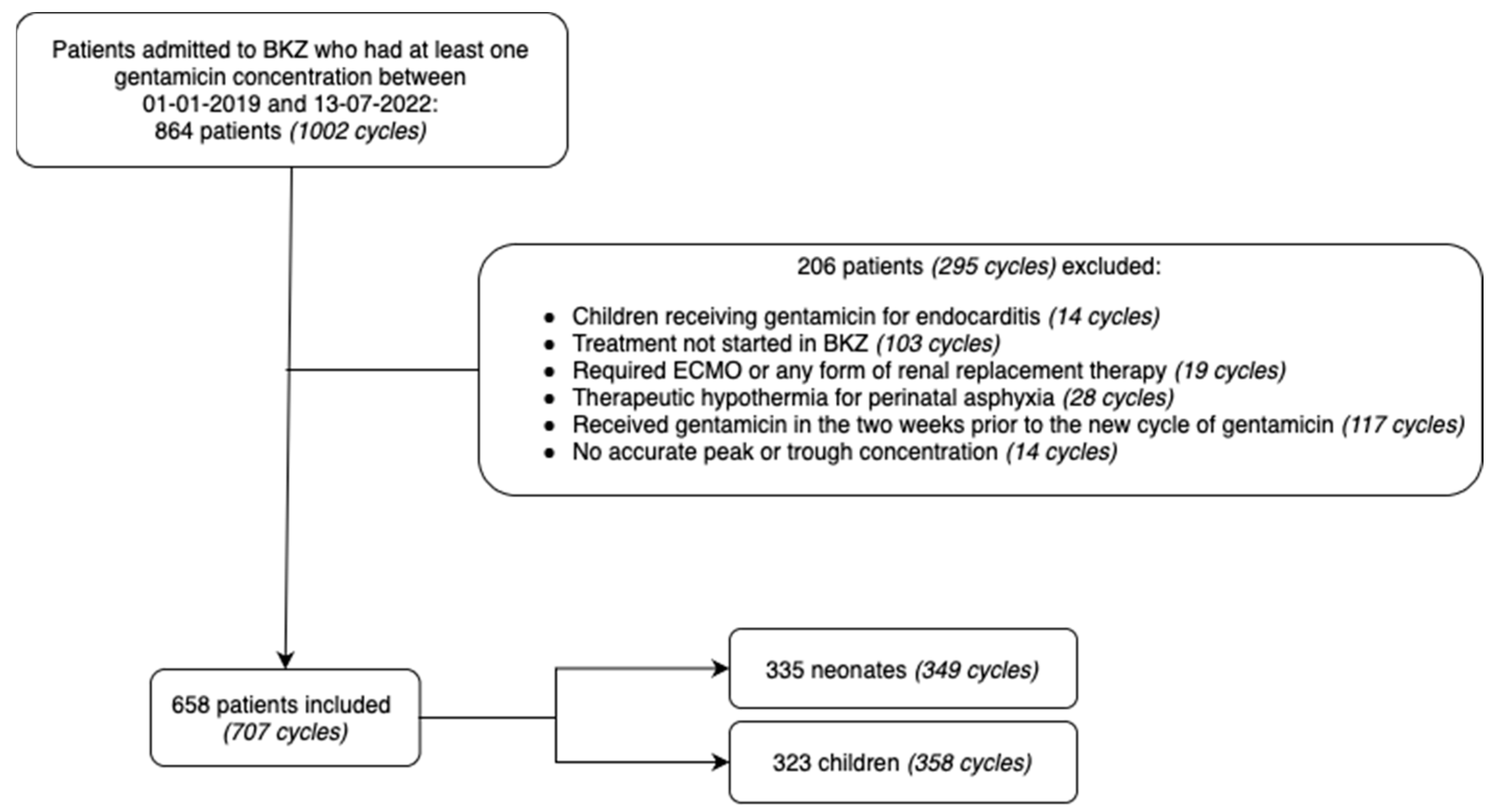
2.1. Patient Characteristics
2.2. Patient Cohorts
2.2.1. Neonates
2.2.2. Children
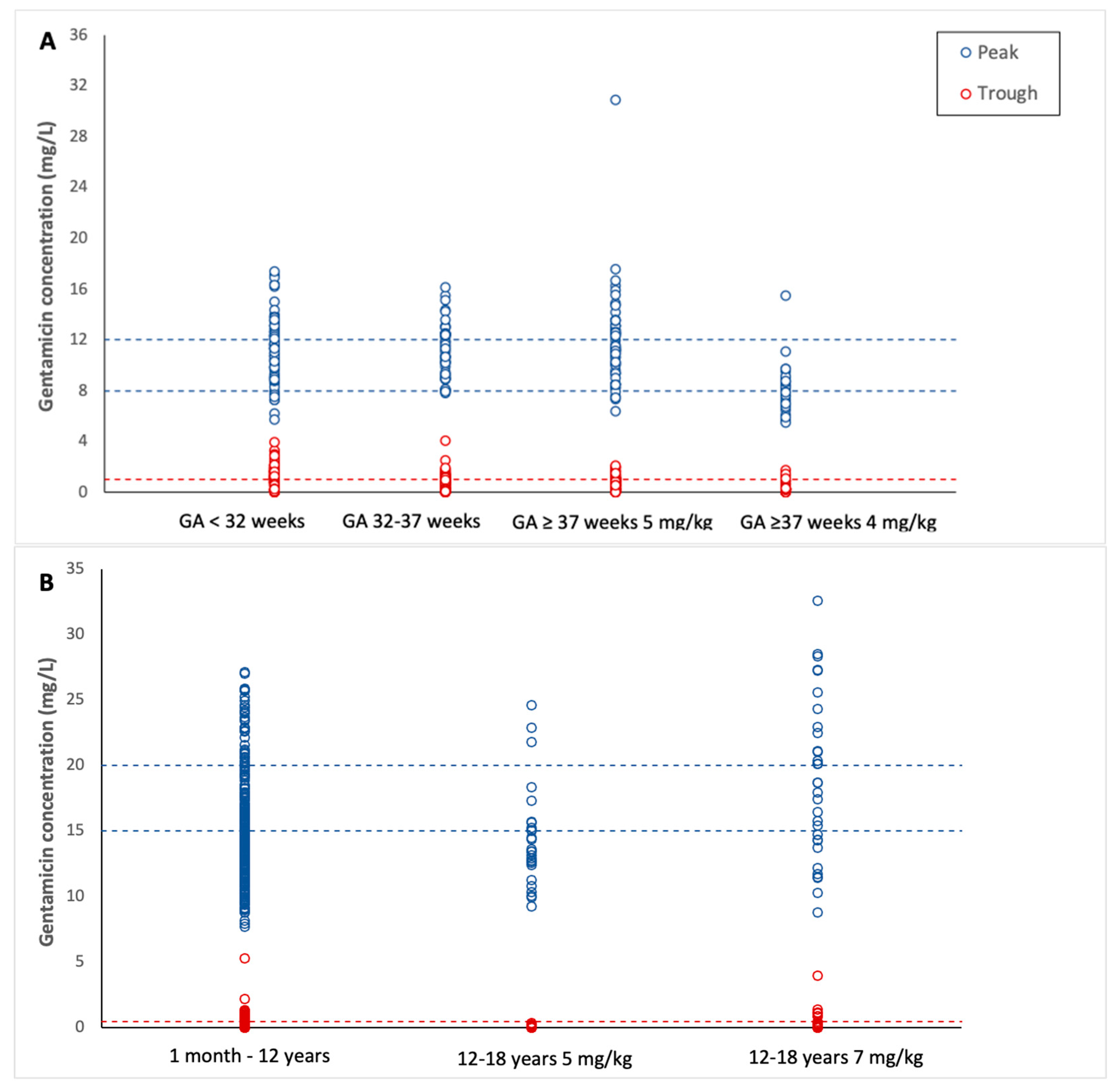
2.3. Target Attainment
2.3.1. Neonates
2.3.2. Children
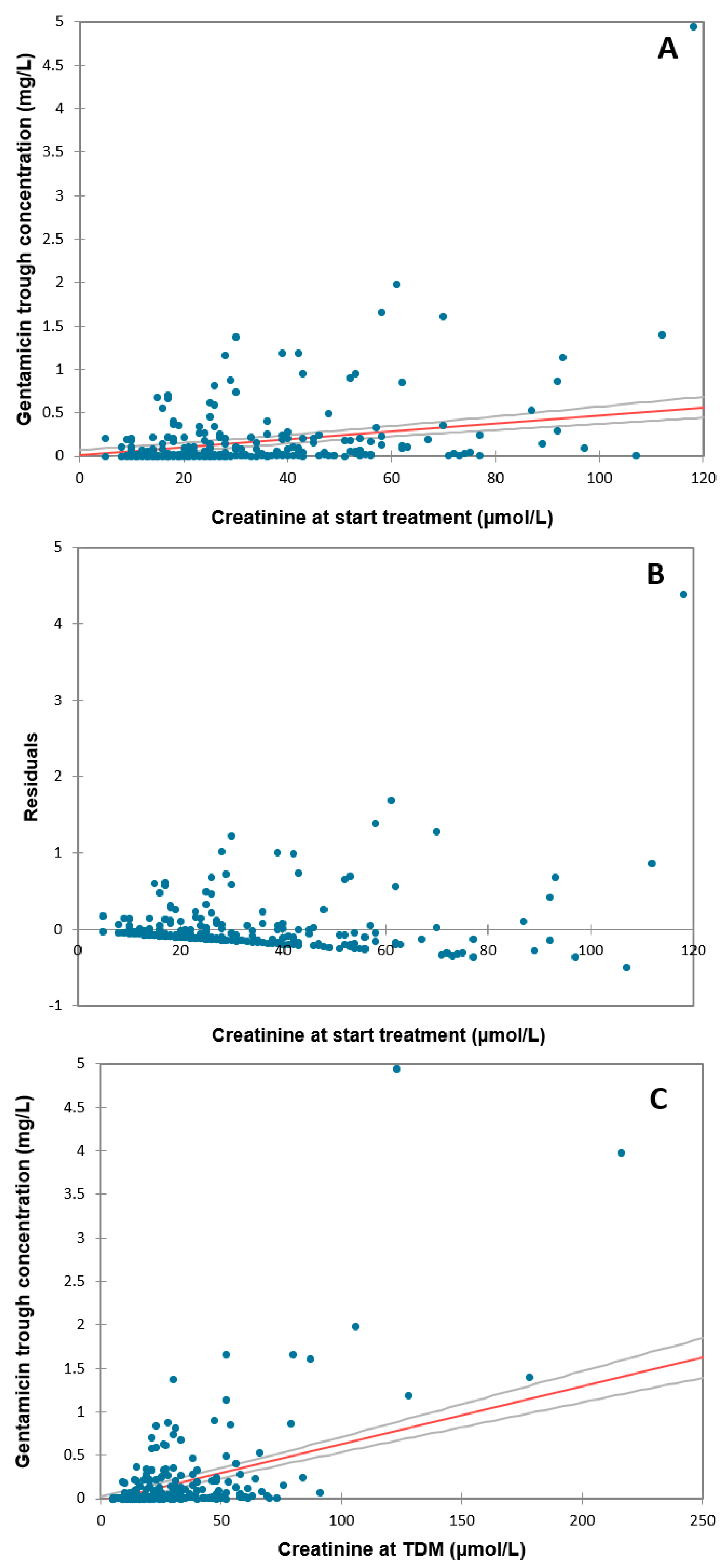
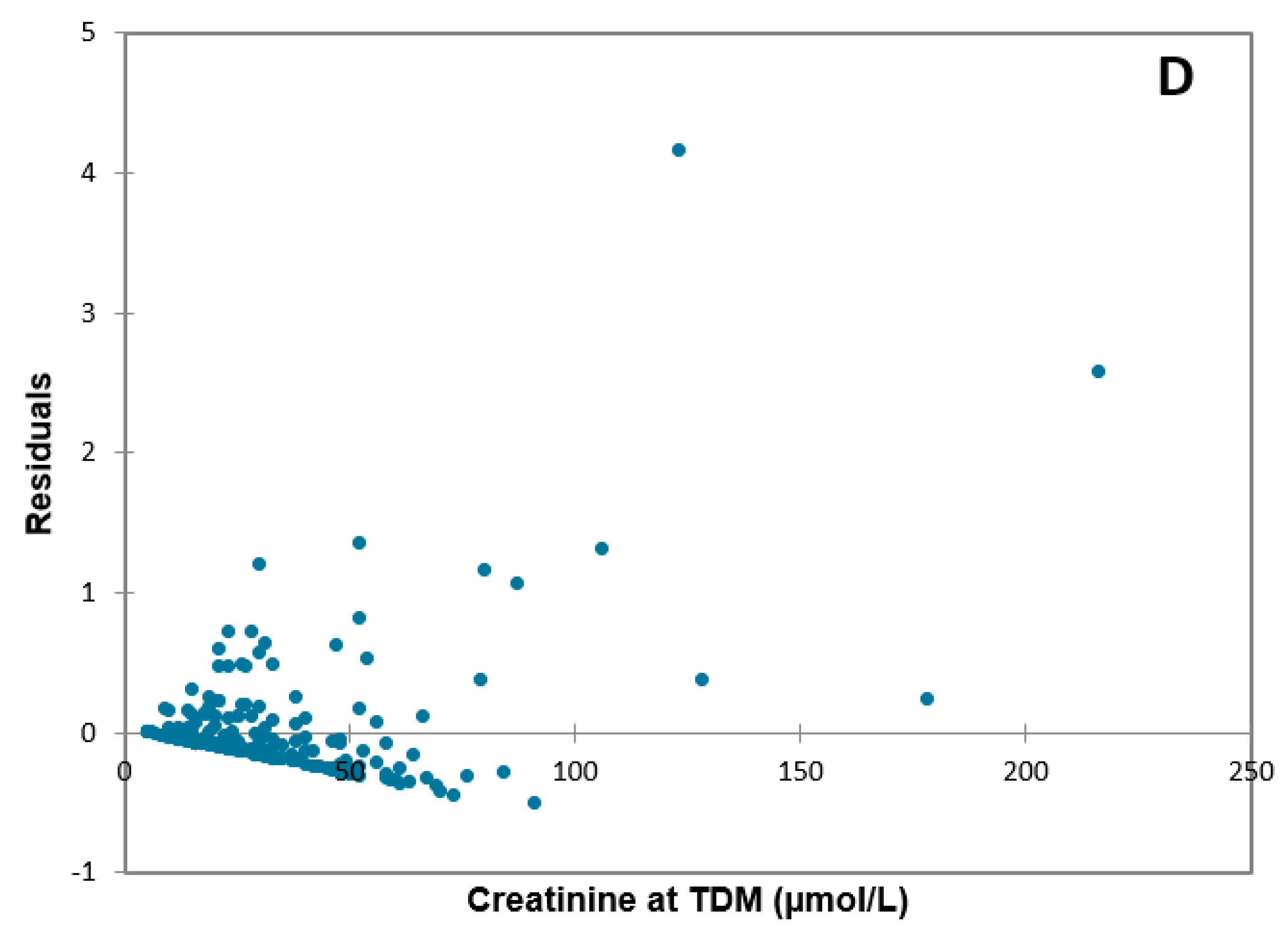
2.4. Correlation with Creatinine Concentration in Children above 1 Month of Age
3. Discussion
3.1. Preterm Neonates (<32 Weeks GA and 32–37 Weeks GA)
3.2. Term Neonates (>37 Weeks)
3.3. Children 1–12 Years
3.4. Children 12–18 Years
3.5. Recommendations
3.6. Limitations
4. Materials and Methods
4.1. Study Design
4.2. Inclusion and Exclusion Criteria
4.3. Data Collection
4.4. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Target | Dose | Age | Target Attainment Trough Concentration | Target Attainment Peak Concentration |
|---|---|---|---|---|---|
| Hartman (2020) [28] | Trough concentration: <1 mg/L Peak concentration: 8–12 mg/L | 5 mg/kg/48 h | <32 weeks GA, <7 days PNA | Within target range: 100% | Subtherapeutic: 44% Therapeutic: 56% Supratherapeutic: 0% |
| 4 mg/kg/24 h | <32 weeks GA, ≥7 days PNA | Within target range: 75% | Subtherapeutic: 100% Therapeutic: 0% Supratherapeutic: 0% | ||
| 5 mg/kg/36 h | 32–37 weeks GA, <7 days PNA | Within target range: 89% | Subtherapeutic: 56% Therapeutic: 33% Supratherapeutic: 11% | ||
| 4 mg/kg/24 h | 32–37 weeks GA, ≥7 days PNA | Within target range: 100% | Subtherapeutic: 100% Therapeutic: 0% Supratherapeutic: 0% | ||
| 4 mg/kg/24 h | >37 weeks GA, any PNA | Within target range: 71% | Subtherapeutic: 87% Therapeutic: 13% Supratherapeutic: 0% | ||
| Sum (2007) [30] | Trough concentration: <1 mg/L Peak concentration: 8–10 mg/L | 5 mg/kg/36 h | <35 weeks GA | Within target range: 91% | Therapeutic: 50% |
| ≥35 weeks GA | Within target range: 98% | Therapeutic: 47% | |||
| Van Maarseveen (2016) [56] | Trough concentration: <1 mg/L Peak concentration: >8 mg/L | 5 mg/kg/36 h | ≥32 weeks GA, ≤7 days PNA | Within target range: 100% | Therapeutic: 91% |
| O’Conner (2021) [52] | Trough concentration: <2 mg/L Peak concentration: 5–12 mg/L | 2.5 mg/kg/24 h | <30 weeks GA, ≤2 days PNA | Within target range: 100% | Subtherapeutic: 23% Therapeutic: 77% Supratherapeutic: 0% |
| ≥30 weeks GA, ≤2 days PNA | Within target range: 100% | Subtherapeutic: 13% Therapeutic: 88% Supratherapeutic: 0% | |||
| 3.5 mg/kg/24 h | <30 weeks GA, ≤2 days PNA | Within target range: 93% | Subtherapeutic: 2% Therapeutic: 98% Supratherapeutic: 0% | ||
| ≥30 weeks GA, ≤2 days PNA | Within target range: 80% | Subtherapeutic: 0% Therapeutic: 98% Supratherapeutic: 2% | |||
| Fullas (2011) [57] | Trough concentration: 0.5–2 mg/L Peak concentration: 5–10 mg/L | 4.5 mg/kg/48 h | ≤29 weeks GA | Within target range: 60% | Therapeutic: 60% |
| 3.5 mg/kg/36 h | 30–34 weeks GA | Within target range: 57% | Therapeutic: 97% | ||
| 4 mg/kg/36 h | Within target range: 73% | Therapeutic: 69% | |||
| 4.5 mg/kg/36 h | Within target range: 46% | Therapeutic: 46% | |||
| 3.5 mg/kg/24 h | ≥35 weeks GA PNA not reported | Within target range: 88% | Therapeutic: 91% | ||
| 4 mg/kg/24 h | Within target range: 93% | Therapeutic: 77% | |||
| Hansen (2003) [58] | Trough concentration: <2 mg/L Peak concentration: 6–12 mg/L | 3 mg/kg/24 h | < 35 weeks GA, ≤7 days PNA | Within target range: 100% | Therapeutic: 79% |
| 4 mg/kg/24 h | ≥35 weeks GA, ≤7 days PNA | Within target range: 100% | Therapeutic: 93% |
References
- Kinderformularium. Gentamicine. Available online: https://www.kinderformularium.nl/geneesmiddel/23/gentamicine (accessed on 30 November 2022).
- Mingeot-Leclercq, M.-P.; Glupczynski, Y.; Tulkens, P.M. Aminoglycosides: Activity and resistance. Antimicrob. Agents Chemother. 1999, 43, 727–737. [Google Scholar] [CrossRef]
- Zelenitsky, S.A.; Harding, G.K.; Sun, S.; Ubhi, K.; Ariano, R.E. Treatment and outcome of Pseudomonas aeruginosa bacteraemia: An antibiotic pharmacodynamic analysis. J. Antimicrob. Chemother. 2003, 52, 668–674. [Google Scholar] [CrossRef]
- Prayle, A.; Watson, A.; Fortnum, H.; Smyth, A. Side effects of aminoglycosides on the kidney, ear and balance in cystic fibrosis. Thorax 2010, 65, 654–658. [Google Scholar] [CrossRef]
- Stolk, L.M.; Degraeuwe, P.L.; Nieman, F.H.; de Wolf, M.C.; de Boer, A. Population Pharmacokinetics and Relationship Between Demographic and Clinical Variables and Pharmacokinetics of Gentamicin in Neonates. Ther. Drug Monit. 2002, 24, 527–531. [Google Scholar] [CrossRef]
- Lingvall, M.; Reith, D.; Broadbent, R. The effect of sepsis upon gentamicin pharmacokinetics in neonates. Br. J. Clin. Pharmacol. 2005, 59, 54–61. [Google Scholar] [CrossRef]
- Hodiamont, C.J.; van den Broek, A.K.; de Vroom, S.L.; Prins, J.M.; Mathôt RA, A.; van Hest, R.M. Clinical pharmacokinetics of gentamicin in various patient populations and consequences for optimal dosing for Gram-negative infections: An updated review. Clin. Pharmacokinet. 2002, 61, 1075–1094. [Google Scholar] [CrossRef]
- Rodieux, F.; Wilbaux, M.; van den Anker, J.N.; Pfister, M. Effect of Kidney Function on Drug Kinetics and Dosing in Neonates, Infants, and Children. Clin. Pharm. 2015, 54, 1183–1204. [Google Scholar] [CrossRef]
- Pacifici, G.M. Clinical pharmacology of gentamicin in neonates: Regimen, toxicology and pharmacokinetics. MedicalExpress 2015, 2, M150501. [Google Scholar] [CrossRef]
- Van Lent-Evers, N.A.; Mathot, R.A.; Geus, W.P.; van Hout, B.A.; Vinks, A.A. Impact of goal-oriented and model-based clinical pharmacokinetic dosing of aminoglycosides on clinical outcome: A cost-effectiveness analysis. Ther. Drug Monit. 1999, 21, 63–73. [Google Scholar] [CrossRef]
- Touw, D.J.; Westerman, E.M.; Sprij, A.J. Therapeutic Drug Monitoring of Aminoglycosides in Neonates. Clin. Pharm. 2009, 48, 71–88. [Google Scholar] [CrossRef]
- Nicolau, D.P.; Freeman, C.D.; Belliveau, P.P.; Nightingale, C.H.; Ross, J.W.; Quintiliani, R. Experience with a once-daily aminoglycoside program administered to 2,184 adult patients. Antimicrob. Agents Chemother. 1995, 39, 650–655. [Google Scholar] [CrossRef] [PubMed]
- NVZA. TDM Monografie Gentamicine. Available online: https://tdm-monografie.org/gentamicine/ (accessed on 4 December 2022).
- Miron, D. Once daily dosing of gentamicin in infants and children. Pediatr. Infect. Dis. J. 2001, 20, 1169–1173. [Google Scholar] [CrossRef] [PubMed]
- Grayson, M.L. Kucers’ The Use of Antibiotics, 6th ed.; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Prins, J.M.; Buller, H.R.; Kuijper, E.J.; Tange, R.A.; Speelman, P. Once versus thrice daily gentamicin in patients with serious infections. Lancet 1993, 341, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Drusano, G.L.; Ambrose, P.G.; Bhavnani, S.M.; Bertino, J.S.; Nafziger, A.N.; Louie, A. Back to the future: Using aminoglycosides again and how to dose them optimally. Clin. Infect. Dis. 2007, 45, 753–760. [Google Scholar]
- D’Agate, S.; Musuamba, F.T.; Jacqz-Aigrain, E.; Della Pasqua, O. Simplified dosing regimens for gentamicin in neonatal sepsis. Front. Pharmacol. 2021, 12, 624662. [Google Scholar] [CrossRef] [PubMed]
- Fjalstad, J.W.; Laukli, E.; van den Anker, J.N.; Klingenberg, C. High-dose gentamicin in newborn infants: Is it safe? Eur. J. Pediatr. 2013, 173, 489–495. [Google Scholar] [CrossRef]
- Alsultan, A.; Abouelkheir, M.; Elsharawy, Y.; Alkoraishi, A.; Osman, R.; Neely, M.N.; Mansy, W.; Algahtani, S. Optimizing gentamicin dosing in pediatrics using Monte Carlo simulations. Pediatr. Infect. Dis. J. 2019, 38, 390–395. [Google Scholar] [CrossRef]
- Ghoneim, R.H.; Thabit, A.K.; Lashkar, M.O.; Ali, A.S. Optimizing gentamicin dosing in different pediatric age groups using population pharmacokinetics and Monte Carlo simulation. Ital. J. Pediatr. 2021, 47, 167. [Google Scholar] [CrossRef]
- McDade, E.J.; Wagner, J.L.; Moffett, B.S.; Palazzi, D.L. Once-daily gentamicin dosing in pediatric patients without cystic fibrosis. Pharmacotherapy 2010, 30, 248–253. [Google Scholar] [CrossRef]
- Van der Zanden, T.M.; de Wildt, S.N.; Liem, Y.; Offringa, M.; de Hoog, M. Developing a paediatric drug formulary for the Netherlands. Arch. Dis. Child. 2017, 102, 357–361. [Google Scholar] [CrossRef]
- De Hoop-Sommen, M.A.; van der Zanden, T.M.; Allegaert, K.; Flint, R.B.; Simons SH, P.; de Wildt, S.N. Development of best evidence dosing recommendations for term and preterm neonates (NeoDose project). Neonatology 2023, 120, 196–207. [Google Scholar] [CrossRef]
- Inparajah, M.; Wong, C.; Sibbald, C.; Boodhan, S.; Atenafu, E.G.; Naqvi, A.; Dupuis, L.L. Once-daily gentamicin dosing in children with febrile neutropenia resulting from antineoplastic therapy. Pharmacotherapy 2010, 30, 43–51. [Google Scholar] [CrossRef]
- Bialkowski, S.; Staatz, C.E.; Clark, J.; Lawson, R.; Hennig, S. Gentamicin Pharmacokinetics and Monitoring in Pediatric Patients with Febrile Neutropenia. Ther. Drug Monit. 2018, 38, 693–698. [Google Scholar] [CrossRef]
- Van Donge, T.; Pfister, M.; Bielicki, J.; Csajka, C.; Rodieux, F.; van den Anker, J.; Fuchs, A. Quantitative Analysis of Gentamicin Exposure in Neonates and Infants Calls into Question Its Current Dosing Recommendations. Antimicrob. Agents Chemother. 2018, 62, e02004–e02017. [Google Scholar] [CrossRef]
- Hartman, S.J.F.; Orriëns, L.B.; Zwaag, S.M.; Poel, T.; de Hoop, M.; de Wildt, S.N. External Validation of Model-Based Dosing Guidelines for Vancomycin, Gentamicin, and Tobramycin in Critically Ill Neonates and Children: A Pragmatic Two-Center Study. Paediatr Drugs 2020, 22, 433–444. [Google Scholar] [CrossRef]
- Veltkamp, S.A.; Westerman, E.M.; Sprij, A.J.; Sum, B.L.; Touw, D.J. Gentamicin in preterm neonates: An extended interval dosing schedule. Eur. J. Hosp. Pharm. 2007, 13, 92–97. [Google Scholar]
- Sum, B.L.; Veltkamp, S.A.; Westerman, E.M.; Sprij, A.J.; Touw, D.J. An extended-ïnterval gentamïcin dosage regimen in newborns: A prospective study. Eur. J. Hosp. Pharm. Sci. 2007, 13, 98–104. [Google Scholar]
- Zakova, M.; Pong, S.; Trope, A.; Atenafu, E.G.; Papaioannou, V.; Bitnun, S.A.; Richardson, S.; Schwartz, S.; Cox, P.; Parshuram, C.; et al. Dose derivation of once-daily dosing guidelines for gentamicin in critically ill pediatric patients. Ther. Drug Monit. 2014, 36, 288–294. [Google Scholar] [CrossRef]
- Kearns, G.L.; Abdel-Rahman, S.M.; Alander, S.W.; Blowey, D.L.; Leeder, J.S.; Kauffman, R.E. Developmental pharmacology–drug disposition, action, and therapy in infants and children. N. Engl. J. Med. 2003, 349, 1157–1167. [Google Scholar] [CrossRef]
- Zhang, Y.; Mehta, N.; Muhari-Stark, E.; Burckart, G.J.; van den Anker, J.; Wang, J. Pediatric renal ontogeny and applications in drug development. J. Clin Pharmacol. 2019, 59 (Suppl. S1), 9–20. [Google Scholar] [CrossRef]
- Moore, R.D.; Smith, C.R.; Lietman, P.S. Association of aminoglycoside plasma levels with therapeutic outcome in gram-negative pneumonia. Am. J. Med. 1984, 77, 657–662. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.D.; Lietmand, P.S.; Smith, C.R. Clinical response to aminoglycoside therapy: Importance of the ratio of peak concentration to minimal inhibitory concentration. J. Infect. Dis. 1987, 155, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Kashuba, A.D.; Nafziger, A.N.; Drusano, G.L.; Bertino, J.S., Jr. Optimizing aminoglycoside therapy for nosocomial pneumonia caused by gram-negative bacteria. Antimicrob. Agents Chemother. 1999, 43, 623–629. [Google Scholar] [CrossRef] [PubMed]
- Best, E.J.; Gazarian, M.; Cohn, R.; Wilkinson, M.; Palasanthiran, P. Once-daily gentamicin in infants and children: A prospective cohort study evaluating safety and the role of therapeutic drug monitoring in minimizing toxicity. Pediatr. Infect. Dis. J. 2011, 30, 827–832. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 13.0. 2023. Available online: http://www.eucast.org. (accessed on 25 January 2023).
- Kent, A.; Kortsalioudaki, C.; Monahan, I.M.; Bielicki, J.; Planche, T.D.; Heath, P.T.; Sharland, M. Neonatal gram-negative infections, antibiotic susceptibility and clinical outcome: An observational study. Arch. Dis. Child.-Fetal Neonatal Ed. 2016, 101, F507–F512. [Google Scholar] [CrossRef]
- Zea-Vera, A.; Ochoa, T.J. Challenges in the diagnosis and management of neonatal sepsis. J. Trop. Pediatr. 2015, 61, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Blaabjerg, A.S.; Kofoed, P.E.; Dalegaard, M.C.; Fenger-Gron, J. A simple high-dose gentamicin regimen showed no side effects among neonates. Dan. Med. J. 2017, 64, A5387. [Google Scholar]
- Wang, H.; Sherwin, C.; Gobburu JV, S.; Ivaturi, V. Population pharmacokinetic modeling of gentamicin in pediatrics. J. Clin. Pharmacol. 2019, 59, 1584–1596. [Google Scholar] [CrossRef]
- Germovsek, E.; Kent, A.; Metsvaht, T.; Lutsar, I.; Klein, N.; Turner, M.A.; Sharland, M.; Nielsen, E.I.; Heath, P.T.; Standing, J.F. Development and evaluation of a gentamicin pharmacokinetic model that facilitates opportunistic gentamicin therapeutic drug monitoring in neonates and infants. Antimicrob. Agents Chemother. 2016, 60, 4869–4877. [Google Scholar] [CrossRef]
- Llanos-Paez, C.C.; Staatz, C.E.; Lawson, R.; Hennig, S. A population pharmacokinetic model of gentamicin in pediatric oncology patients to facilitate personalized dosing. Antimicrob. Agents Chemother. 2017, 61, e00205–e00217. [Google Scholar] [CrossRef]
- Thomson, A.H.; Way, S.; Bryson, S.M.; McGovern, E.M.; Kelman, A.W.; Whiting, B. Population pharmacokinetics of gentamicin in neonates. Dev. Pharmacol. Ther. 1988, 11, 173–179. [Google Scholar]
- Frymoyer, A.; Meng, L.; Bonifacio, S.L.; Verotta, D.; Guglielmo, B.J. Gentamicin pharmacokinetics and dosing in neonates with hypoxic ischemic encephalopathy receiving hypothermia. Pharmacotherapy 2013, 33, 718–726. [Google Scholar] [CrossRef]
- Guignard, J.-P.; Drukker, A. Why do newborn infants have a high plasma creatinine? Pediatrics 1999, 103, e49. [Google Scholar]
- Gallini, F.; Maggio, L.; Romagnoli, C.; Marrocco, G.; Tortorolo, G. Progression of renal function in preterm neonates with gestational age ≤32 weeks. Pediatr. Nephrol. 2000, 15, 119–124. [Google Scholar] [PubMed]
- Thayyil, S.; Sheik, S.; Kempley, S.T.; Sinha, A. A gestation- and postnatal age-based reference chart for assessing renal function in extremely premature infants. J. Perinatol. 2008, 28, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Miall, L.S.; Henderson, M.J.; Turner, A.J.; Brownlee, K.G.; Brocklebank, J.T.; Newell, S.J.; Allgar, V.L. Plasma creatinine rises dramatically in the first 48 hours of life in preterm infants. Pediatrics 1999, 104, e76. [Google Scholar] [CrossRef] [PubMed]
- Lopez, S.A.; Mulla, H.; Durward, A.; Tibby, S.M. Extended-interval gentamicin: Population pharmacokinetics in pediatric critical illness. Pediatr. Crit. Care Med. 2010, 11, 267–274. [Google Scholar] [CrossRef]
- O’Connor, K.; Davies, M.W.; Koorts, P.; Cartwright, D.W.; Whitfield, K. Gentamicin Dosing in Neonates with Normal Renal Function: Trough and Peak Levels. Eur. J. Drug Metab. Pharmacokinet. 2021, 46, 677–684. [Google Scholar] [CrossRef]
- Hartman SJ, F.; Brüggemann, R.J.; Orriëns, L.; Dia, N.; Schreuder, M.F.; de Wildt, S.N. Pharmacokinetics and target attainment of antibiotics in critically ill children: A systematic review of current literature. Clin. Pharmacokinet. 2020, 59, 173–205. [Google Scholar] [CrossRef]
- SOP Analyse: Gentamicine in Serum of Plasma m.b.v. Architect; Klinische Farmacie en Farmacologie UMCG: Groningen, The Netherlands, 2022.
- Abbott. ARCHITECT c8000 Clinical Chemistry. Available online: https://www.corelaboratory.abbott/us/en/offerings/brands/architect/architect-c8000.html (accessed on 16 December 2022).
- Van Maarseveen, E.M.; Sprij, A.; Touw, D.J. Extended-Interval Dosing of Gentamicin Aiming for a Drug-Free Period in Neonates: A Prospective Cohort Study. Ther. Drug Monit. 2016, 38, 402–406. [Google Scholar] [CrossRef]
- Fullas, F.; Padomek, M.T.; Thieman, C.J.; Van Gorp, A.E. Comparative evaluation of six extended-interval gentamicin dosing regimens in premature and full-term neonates. Am. J. Health-Syst. Pharm. 2011, 68, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Hansen, A.; Forbes, P.; Arnold, A.; O’Rourke, E. Once-daily gentamicin dosing for the preterm and term newborn: Proposal for a simple regimen that achieves target levels. J. Perinatol. 2003, 23, 635–639. [Google Scholar] [CrossRef] [PubMed]




| Cohort | BKZ | DPF | ||
|---|---|---|---|---|
| Daily Dose (mg/kg) | Dose Interval (hours) | Daily Dose (mg/kg) | Dose Interval (hours) | |
| Neonates | ||||
| GA < 32 weeks, <7 days PNA | 5 | 48 | 5 | 48 |
| GA < 32 weeks, ≥7 days PNA | 5 | 48 | 4 | 24 |
| GA 32–37 weeks, <7 days PNA | 5 | 36 | 5 | 36 |
| GA 32–37 weeks, ≥7 days PNA | 5 | 36 | 4 | 24 |
| GA > 37 weeks | 5 | 24 | 4 | 24 |
| Children | ||||
| 1 month–12 years | 7 | 24 | 7 | 24 |
| Adolescents | ||||
| 12–18 years (before 2021) | 7 | 24 | 7 | 24 |
| 12–18 years (after 2021) | 5 | 24 | 5 | 24 |
| Characteristics | Neonates | Children |
|---|---|---|
| Number of subjects | 335 | 323 |
| Number of cycles | 349 | 358 |
| PNA at treatment start | 1 day (0–7) | 2.21 years (0.51–9.69) |
| PNA < 7 days (n of cycles) | 260 | - |
| PNA ≥ 7 days (n of cycles) | 89 | - |
| GA at birth (weeks) | 38 (33–40) | - |
| GA < 32 weeks (n of cycles) | 80 | - |
| GA 32–37 weeks (n of cycles | 66 | - |
| GA ≥ 37 weeks (n of cycles) | 203 | - |
| 1 month–12 years (n of cycles) | - | 286 |
| 12–18 years (n of cycles) | - | 72 |
| Weight (kg) | 2.79 (1.75–3.60) | 12.8 (6.99–31.65) |
| Male/female | 62/38 | 55/45 |
| Creatinine concentration at start of treatment (µmol/L) | - | 25 (17–40), n = 258 |
| Creatinine concentration at TDM (µmol/L) | - | 24 (16–40), n = 236 |
| Gentamicin dose (mg/kg) | 5.00 (5.00–5.02) | 7.00 (6.96–7.02) |
| Gentamicin trough concentration (mg/L) | 0.92 (0.40–1.44)n=312 | 0.04 (0.00–0.22)n=334 |
| Gentamicin peak concentration (mg/L) | 11.14 (9.09–12.58)n=274 | 14.77 (12.43–17.80)n=317 |
| Safety (Trough Concentration) | Safe (%) | Toxic (%) | |
| Neonates total (n = 312) | 53.8 | 46.2 | |
| GA < 32 weeks (5 mg/kg per 48 h) (n = 76) | 68.4 | 31.6 | |
| PNA < 7 days (n = 63) | 63.5 | 36.5 | |
| PNA ≥ 7 days (n = 13) | 92.3 | 7.7 | |
| GA 32–37 weeks (5 mg/kg per 36 h) (n = 53) | 66.0 | 34.0 | |
| PNA < 7 days (n = 41) | 56.1 | 43.9 | |
| PNA ≥ 7 days (n = 12) | 100.0 | 0.0 | |
| GA > 37 weeks (5 mg/kg per 24 h) (n = 149) | 34.9 | 65.1 | |
| GA > 37 weeks (4 mg/kg per 24 h) (n = 34) | 85.3 | 14.7 | |
| Children total (n = 334) | 90.1 | 9.9 | |
| 1 month-12 years (7 mg/kg per 24 h) (n = 266) | 89.8 | 10.2 | |
| 12–18 years (5 mg/kg per 24 h) (n = 25) | 100.0 | 0.0 | |
| 12–18 years (7 mg/kg per 24 h) (n = 43) | 86.0 | 14.0 | |
| Efficacy (Peak Concentration) | Subtherapeutic (%) | Therapeutic (%) | Supratherapeutic (%) |
| Neonates total (n = 274) | 10.6 | 54.0 | 35.4 |
| GA < 32 weeks (5 mg/kg per 48 h) (n = 62) | 8.1 | 50.0 | 41.9 |
| PNA < 7 days (n = 50) | 4.0 | 46.0 | 50.0 |
| PNA ≥ 7 days (n = 12) | 25.0 | 66.7 | 8.3 |
| GA 32–37 weeks (5 mg/kg per 36 h) (n = 49) | 4.1 | 57.1 | 38.8 |
| PNA < 7 days (n = 37) | 0.0 | 48.6 | 51.4 |
| PNA ≥ 7 days (n = 12) | 16.7 | 83.3 | 0.0 |
| GA > 37 weeks (5 mg/kg per 24 h) (n = 130) | 6.2 | 54.6 | 39.2 |
| GA > 37 weeks (4 mg/kg per 24 h) (n = 33) | 42.4 | 54.5 | 3.0 |
| Children total (n = 317) | 51.7 | 31.2 | 17.0 |
| 1 month-12 years (7 mg/kg per 24 h) (n = 254) | 53.5 | 33.1 | 13.4 |
| 12–18 years (5 mg/kg per 24 h) (n = 27) | 63.0 | 25.9 | 11.1 |
| 12–18 years (7 mg/kg per 24 h) (n = 36) | 30.6 | 22.2 | 47.2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hollander, E.M.; van Tuinen, E.L.; Schölvinck, E.H.; Bergman, K.A.; Bourgonje, A.R.; Gracchi, V.; Kneyber, M.C.J.; Touw, D.J.; Mian, P. Evaluation of Dosing Guidelines for Gentamicin in Neonates and Children. Antibiotics 2023, 12, 810. https://doi.org/10.3390/antibiotics12050810
Hollander EM, van Tuinen EL, Schölvinck EH, Bergman KA, Bourgonje AR, Gracchi V, Kneyber MCJ, Touw DJ, Mian P. Evaluation of Dosing Guidelines for Gentamicin in Neonates and Children. Antibiotics. 2023; 12(5):810. https://doi.org/10.3390/antibiotics12050810
Chicago/Turabian StyleHollander, Esther M., Eline L. van Tuinen, Elisabeth H. Schölvinck, Klasien A. Bergman, Arno R. Bourgonje, Valentina Gracchi, Martin C. J. Kneyber, Daan J. Touw, and Paola Mian. 2023. "Evaluation of Dosing Guidelines for Gentamicin in Neonates and Children" Antibiotics 12, no. 5: 810. https://doi.org/10.3390/antibiotics12050810