
Effectiveness and Safety of Linezolid Versus Vancomycin, Teicoplanin, or Daptomycin against Methicillin-Resistant Staphylococcus aureus Bacteremia: A Systematic Review and Meta-Analysis
 ,
,
Abstract
:1. Introduction
2. Results
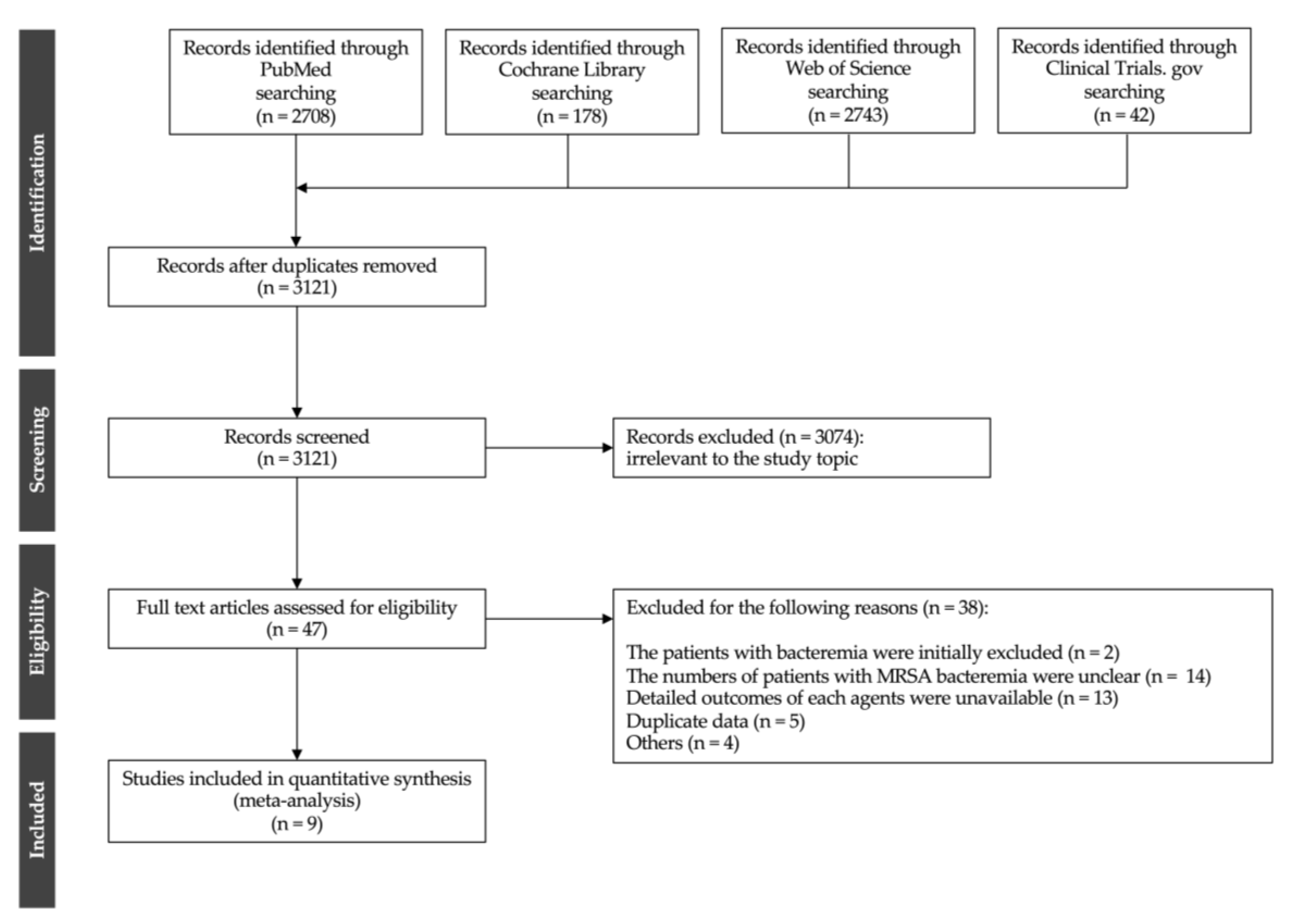
2.1. Literature Search Results
2.1.1. Systematic Review
2.1.2. Meta-Analysis
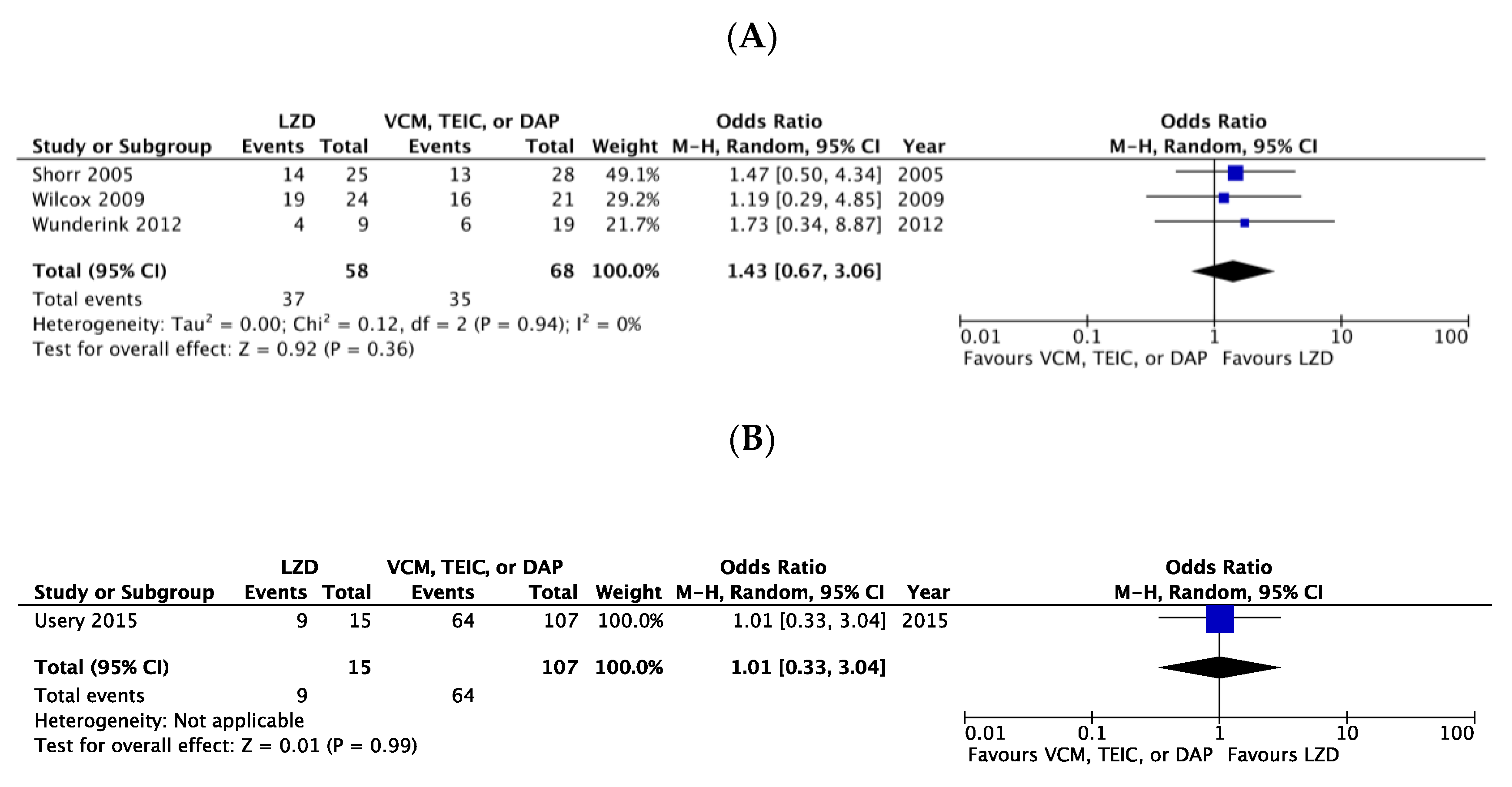
Primary Effectiveness Outcomes
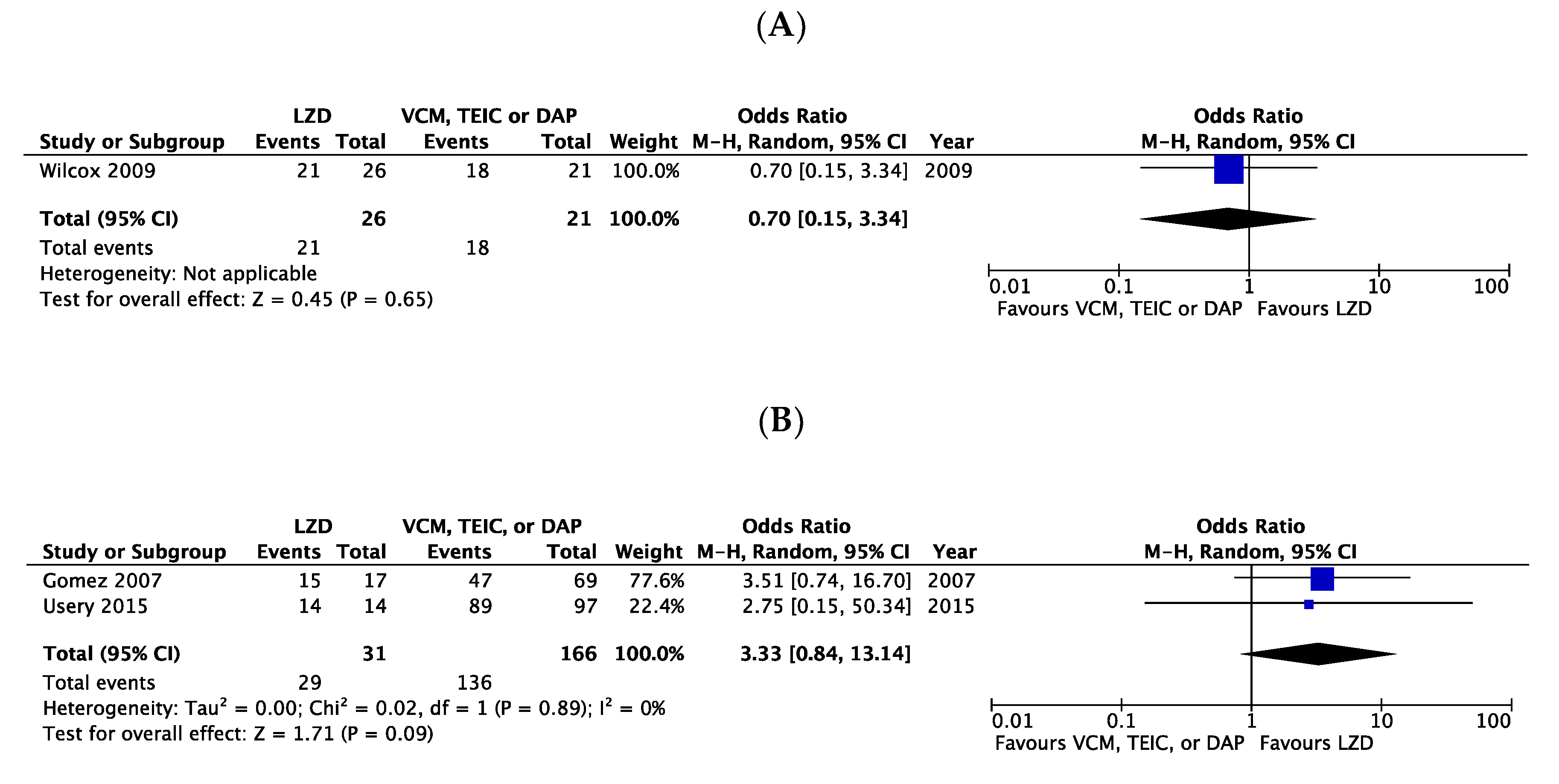
Secondary Effectiveness Outcomes
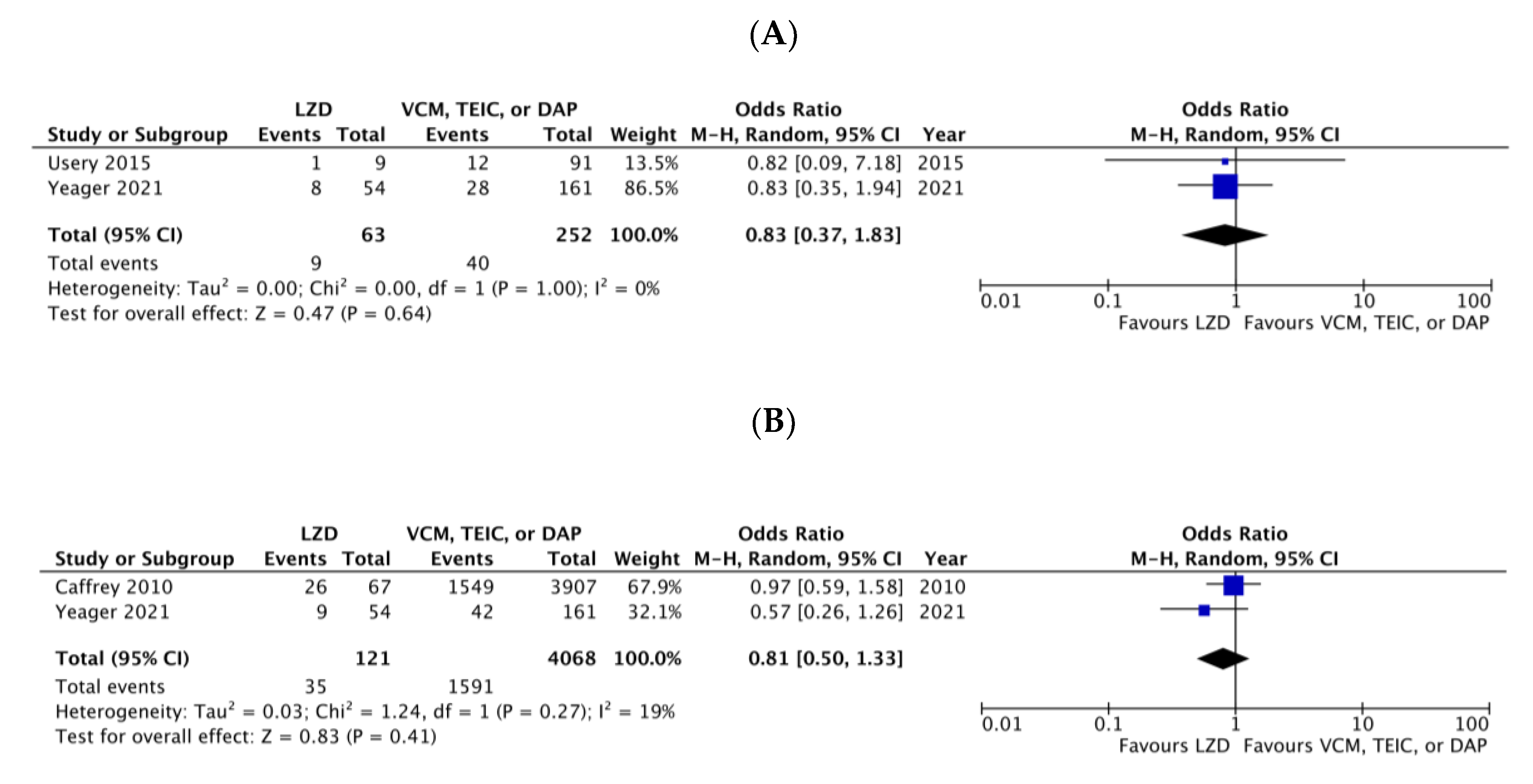
Primary Safety Outcome
2.2. Risk of Bias
2.3. Quality of Evidence
3. Discussion
4. Materials and Methods
4.1. Search Strategy and Study Selection Criteria
4.2. Data Extraction
4.3. Assessment for the Risk of Bias
4.4. Assessment of Quality of Evidence
4.5. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bai, A.D.; Lo, C.K.L.; Komorowski, A.S.; Suresh, M.; Guo, K.; Garg, A.; Tandon, P.; Senecal, J.; Del Corpo, O.; Stefanova, I.; et al. Staphylococcus aureus bacteraemia mortality: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 1076–1084. [Google Scholar] [CrossRef] [PubMed]
- Hassoun, A.; Linden, P.K.; Friedman, B. Incidence, prevalence, and management of MRSA bacteremia across patient populations-a review of recent developments in MRSA management and treatment. Crit. Care 2017, 21, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gómez, J.; García-Vázquez, E.; Baños, R.; Canteras, M.; Ruiz, J.; Baños, V.; Herrero, J.A.; Valdés, M. Predictors of mortality in patients with methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia: The role of empiric antibiotic therapy. Eur. J. Clin. Microbiol. Infect. Dis. 2007, 26, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Bayer, A.; Cosgrove, S.E.; Daum, R.S.; Fridkin, S.K.; Gorwitz, R.J.; Kaplan, S.L.; Karchmer, A.W.; Levine, D.P.; Murray, B.E.; et al. Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clin. Infect. Dis. 2011, 52, e18–e55. [Google Scholar] [CrossRef] [Green Version]
- Wilcox, M.; Nathwani, D.; Dryden, M. Linezolid compared with teicoplanin for the treatment of suspected or proven Gram-positive infections. J. Antimicrob. Chemother. 2004, 53, 335–344. [Google Scholar] [CrossRef]
- Shorr, A.F.; Kunkel, M.J.; Kollef, M. Linezolid versus vancomycin for Staphylococcus aureus bacteraemia: Pooled analysis of randomized studies. J. Antimicrob. Chemother. 2005, 56, 923–929. [Google Scholar] [CrossRef]
- Wilcox, M.H.; Tack, K.J.; Bouza, E.; Herr, D.L.; Ruf, B.R.; IJzerman, M.M.; Croos-Dabrera, R.V.; Kunkel, M.J.; Knirsch, C. Complicated skin and skin-structure infections and catheter-related bloodstream infections: Noninferiority of linezolid in a phase 3 study. Clin. Infect. Dis. 2009, 48, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Usery, J.B.; Vo, N.H.; Finch, C.K.; Cleveland, K.O.; Gelfand, M.S.; Self, T.H. Evaluation of the treatment of methicillin-resistant Staphylococcus aureus bacteremia. Am. J. Med. Sci. 2015, 349, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Yeager, S.D.; Oliver, J.E.; Shorman, M.A.; Wright, L.R.; Veve, M.P. Comparison of linezolid step-down therapy to standard parenteral therapy in methicillin-resistant Staphylococcus aureus bloodstream infections. Int. J. Antimicrob. Agents 2021, 57, 106329. [Google Scholar] [CrossRef]
- MacGowan, A.P. Pharmacokinetic and pharmacodynamic profile of linezolid in healthy volunteers and patients with Gram-positive infections. J. Antimicrob. Chemother. 2003, 51 (Suppl. S2), ii17–ii25. [Google Scholar] [CrossRef] [Green Version]
- Moellering, R.C. Linezolid: The first oxazolidinone antimicrobial. Ann. Intern. Med. 2003, 138, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Wald-Dickler, N.; Holtom, P.; Spellberg, B. Busting the myth of “Static vs. Cidal”: A systemic literature review. Clin. Infect. Dis. 2018, 66, 1470–1474. [Google Scholar] [CrossRef] [PubMed]
- Stevens, D.L.; Dotter, B.; Madaras-Kelly, K. A review of linezolid: The first oxazolidinone antibiotic. Expert. Rev. Anti-Infect. Ther. 2004, 2, 51–59. [Google Scholar] [CrossRef]
- Kato, H.; Hagihara, M.; Asai, N.; Shibata, Y.; Koizumi, Y.; Yamagishi, Y.; Mikamo, H. Meta-analysis of vancomycin versus linezolid in pneumonia with proven methicillin-resistant Staphylococcus aureus. J. Glob. Antimicrob. Resist. 2021, 24, 98–105. [Google Scholar] [CrossRef]
- Feng, J.; Xiang, F.; Cheng, J.; Gou, Y.; Li, J. Comparative efficacy and safety of vancomycin, linezolid, tedizolid, and daptomycin in treating patients with suspected or proven complicated skin and soft tissue infections: An updated network meta-analysis. Infect. Dis. Ther. 2021, 10, 1531–1547. [Google Scholar] [CrossRef]
- Park, H.J.; Kim, S.H.; Kim, M.J.; Lee, Y.M.; Park, S.Y.; Moon, S.M.; Park, K.H.; Chong, Y.P.; Lee, S.O.; Choi, S.H.; et al. Efficacy of linezolid-based salvage therapy compared with glycopeptide-based therapy in patients with persistent methicillin-resistant Staphylococcus aureus bacteremia. J. Infect. 2012, 65, 505–512. [Google Scholar] [CrossRef]
- Kullar, R.; Sakoulas, G.; Deresinski, S.; van Hal, S.J. When sepsis persists: A review of MRSA bacteraemia salvage therapy. J. Antimicrob. Chemother. 2016, 71, 576–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caffrey, A.R.; Quilliam, B.J.; LaPlante, K.L. Comparative effectiveness of linezolid and vancomycin among a national cohort of patients infected with methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 2010, 54, 4394–4400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, N.M.; Goodman, A.L.; Horner, C.; Jenkins, A.; Brown, E.M. Treatment of methicillin-resistant Staphylococcus aureus (MRSA): Updated guidelines from the UK. JAC Antimicrob. Resist. 2021, 3, dlaa114. [Google Scholar] [CrossRef]
- Wunderink, R.G.; Niederman, M.S.; Kollef, M.H.; Shorr, A.F.; Kunkel, M.J.; Baruch, A.; McGee, W.T.; Reisman, A.; Chastre, J. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: A randomized, controlled study. Clin. Infect. Dis. 2012, 54, 621–629. [Google Scholar] [CrossRef] [Green Version]
- Rose, H.R.; Holzman, R.S.; Altman, D.R.; Smyth, D.S.; Wasserman, G.A.; Kafer, J.M.; Wible, M.; Mendes, R.E.; Torres, V.J.; Shopsin, B. Cytotoxic virulence predicts mortality in nosocomial pneumonia due to methicillin-resistant Staphylococcus aureus. J. Infect. Dis. 2015, 211, 1862–1874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, Y.P.; Park, K.H.; Kim, E.S.; Kim, M.N.; Kim, S.H.; Lee, S.O.; Choi, S.H.; Jeong, J.Y.; Woo, J.H.; Kim, Y.S. Clinical and microbiologic analysis of the risk factors for mortality in patients with heterogeneous vancomycin-intermediate Staphylococcus aureus bacteremia. Antimicrob. Agents Chemother. 2015, 59, 3541–3547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rubinstein, E.; Cammarata, S.; Oliphant, T.; Wunderink, R.; Linezolid Nosocomial Pneumonia Study Group. Linezolid (PNU-100766) versus vancomycin in the treatment of hospitalized patients with nosocomial pneumonia: A randomized, double-blind, multicenter study. Clin. Infect. Dis. 2001, 32, 402–412. [Google Scholar] [CrossRef] [Green Version]
- Wunderink, R.G.; Cammarata, S.K.; Oliphant, T.H.; Kollef, M.H.; Linezolid Nosocomial Pneumonia Study Group. Continuation of a randomized, double-blind, multicenter study of linezolid versus vancomycin in the treatment of patients with nosocomial pneumonia. Clin. Ther. 2003, 25, 980–992. [Google Scholar] [CrossRef]
- Stevens, D.L.; Herr, D.; Lampiris, H.; Hunt, J.L.; Batts, D.H.; Hafkin, B. Linezolid versus vancomycin for the treatment of methicillin-resistant Staphylococcus aureus infections. Clin. Infect. Dis. 2002, 34, 1481–1490. [Google Scholar] [CrossRef] [Green Version]
- Yoon, Y.K.; Park, D.W.; Sohn, J.W.; Kim, H.Y.; Kim, Y.S.; Lee, C.S.; Lee, M.S.; Ryu, S.Y.; Jang, H.C.; Choi, Y.J.; et al. Multicenter prospective observational study of the comparative efficacy and safety of vancomycin versus teicoplanin in patients with health care-associated methicillin-resistant Staphylococcus aureus bacteremia. Antimicrob. Agents Chemother. 2014, 58, 317–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Britt, N.S.; Potter, E.M.; Patel, N.; Steed, M.E. Comparison of the Effectiveness and Safety of Linezolid and Daptomycin in Vancomycin-Resistant Enterococcal Bloodstream Infection: A National Cohort Study of Veterans Affairs Patients. Clin. Infect. Dis. 2015, 61, 871–878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yue, J.; Dong, B.R.; Yang, M.; Chen, X.; Wu, T.; Liu, G.J. Linezolid versus vancomycin for skin and soft tissue infections. Cochrane Database Syst. Rev. 2013, 12, CD008056. [Google Scholar] [CrossRef] [Green Version]
- Mohammad, H.; Mayhoub, A.S.; Cushman, M.; Seleem, M.N. Anti-biofilm activity and synergism of novel thiazole compounds with glycopeptide antibiotics against multidrug-resistant Staphylococci. J. Antibiot. 2015, 68, 259–266. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.C.; Sy, C.L.; Huang, Y.C.; Shie, S.S.; Shu, J.C.; Hsieh, P.H.; Hsiao, C.H.; Chen, C.J. Risk factors of treatment failure and 30-day mortality in patients with bacteremia due to MRSA with reduced vancomycin susceptibility. Sci. Rep. 2018, 8, 7868. [Google Scholar] [CrossRef] [Green Version]
- Pfaller, M.A.; Cormican, M.; Flamm, R.K.; Mendes, R.E.; Jones, R.N. Temporal and geographic variation in antimicrobial susceptibility and resistance patterns of enterococci: Results from the SENTRY antimicrobial surveillance program, 1997–2016. Open Forum Infect. Dis. 2019, 6 (Suppl. S1), S54–S62. [Google Scholar] [CrossRef] [Green Version]
- Patel, J.B.; Jevitt, L.A.; Hageman, J.; McDonald, L.C.; Tenover, F.C. An association between reduced susceptibility to daptomycin and reduced susceptibility to vancomycin in Staphylococcus aureus. Clin. Infect. Dis. 2006, 42, 1652–1653. [Google Scholar] [CrossRef]
- Humphries, R.M.; Pollett, S.; Sakoulas, G. A current perspective on daptomycin for the clinical microbiologist. Clin. Microbiol. Rev. 2013, 26, 759–780. [Google Scholar] [CrossRef] [Green Version]
- Sakoulas, G.; Alder, J.; Thauvin-Eliopoulos, C.; Moellering, R.C., Jr.; Eliopoulos, G.M. Induction of daptomycin heterogeneous susceptibility in Staphylococcus aureus by exposure to vancomycin. Antimicrob. Agents Chemother. 2006, 50, 1581–1585. [Google Scholar] [CrossRef] [Green Version]
- Vinh, D.C.; Rubinstein, E. Linezolid: A review of safety and tolerability. J. Infect. 2009, 59 (Suppl. S1), S59–S74. [Google Scholar] [CrossRef]
- Conte, J.E., Jr.; Golden, J.A.; Kipps, J.; Zurlinden, E. Intrapulmonary pharmacokinetics of linezolid. Antimicrob. Agents Chemother. 2002, 46, 1475–1480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamer, C.; de Beco, V.; Soler, P.; Calvat, S.; Fagon, J.Y.; Dombret, M.C.; Farinotti, R.; Chastre, J.; Gibert, C. Analysis of vancomycin entry into pulmonary lining fluid by bronchoalveolar lavage in critically ill patients. Antimicrob. Agents Chemother. 1993, 37, 281–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gee, T.; Ellis, R.; Marshall, G.; Andrews, J.; Ashby, J.; Wise, R. Pharmacokinetics and tissue penetration of linezolid following multiple oral doses. Antimicrob. Agents Chemother. 2001, 45, 1843–1846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wise, R.; Gee, T.; Andrews, J.M.; Dvorchik, B.; Marshall, G. Pharmacokinetics and inflammatory fluid penetration of intravenous daptomycin in volunteers. Antimicrob. Agents Chemother. 2002, 46, 31–33. [Google Scholar] [CrossRef] [Green Version]
- Lovering, A.M.; Zhang, J.; Bannister, G.C.; Lankester, B.J.; Brown, J.H.; Narendra, G.; MacGowan, A.P. Penetration of linezolid into bone, fat, muscle and haematoma of patients undergoing routine hip replacement. J. Antimicrob. Chemother. 2002, 50, 73–77. [Google Scholar] [CrossRef] [Green Version]
- Daschner, F.D.; Frank, U.; Kümmel, A.; Schmidt-Eisenlohr, E.; Schlosser, V.; Spillner, H.; Schuster, B.; Schindler, M. Pharmacokinetics of vancomycin in serum and tissue of patients undergoing open-heart surgery. J. Antimicrob. Chemother. 1987, 19, 359–362. [Google Scholar] [CrossRef]
- Rana, B.; Butcher, I.; Grigoris, P.; Murnaghan, C.; Seaton, R.A.; Tobin, C.M. Linezolid penetration into osteo-articular tissues. J. Antimicrob. Chemother. 2002, 50, 747–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graziani, A.L.; Lawson, L.A.; Gibson, G.A.; Steinberg, M.A.; MacGregor, R.R. Vancomycin concentrations in infected and noninfected human bone. Antimicrob. Agents Chemother. 1988, 32, 1320–1322. [Google Scholar] [CrossRef] [Green Version]
- Montange, D.; Berthier, F.; Leclerc, G.; Serre, A.; Jeunet, L.; Berard, M.; Muret, P.; Vettoretti, L.; Leroy, J.; Hoen, B.; et al. Penetration of daptomycin into bone and synovial fluid in joint replacement. Antimicrob. Agents Chemother. 2014, 58, 3991–3996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villani, P.; Regazzi, M.B.; Marubbi, F.; Viale, P.; Pagani, L.; Cristini, F.; Cadeo, B.; Carosi, G.; Bergomi, R. Cerebrospinal fluid linezolid concentrations in postneurosurgical central nervous system infections. Antimicrob. Agents Chemother. 2002, 46, 936–937. [Google Scholar] [CrossRef] [Green Version]
- Albanèse, J.; Léone, M.; Bruguerolle, B.; Ayem, M.L.; Lacarelle, B.; Martin, C. Cerebrospinal fluid penetration and pharmacokinetics of vancomycin administered by continuous infusion to mechanically ventilated patients in an intensive care unit. Antimicrob. Agents Chemother. 2000, 44, 1356–1358. [Google Scholar] [CrossRef] [Green Version]
- Piva, S.; Di Paolo, A.; Galeotti, L.; Ceccherini, F.; Cordoni, F.; Signorini, L.; Togni, T.; De Nicolò, A.; Rasulo, F.A.; Fagoni, N.; et al. Daptomycin plasma and CSF levels in patients with healthcare-associated meningitis. Neurocrit. Care 2019, 31, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Nau, R.; Djukic, M.; Spreer, A.; Ribes, S.; Eiffert, H. Bacterial meningitis: An update of new treatment options. Expert. Rev. Anti-Infect. Ther. 2015, 13, 1401–1423. [Google Scholar] [CrossRef]
- Senior, K. FDA issue linezolid warning. Lancet Infect. Dis. 2007, 7, 310. [Google Scholar] [CrossRef]
- Shariati, A.; Dadashi, M.; Chegini, Z.; van Belkum, A.; Mirzaii, M.; Khoramrooz, S.S.; Darban-Sarokhalil, D. The global prevalence of Daptomycin, Tigecycline, Quinupristin/Dalfopristin, and Linezolid-resistant Staphylococcus aureus and coagulase–negative staphylococci strains: A systematic review and meta-analysis. Antimicrob. Resist. Infect. Control 2020, 9, 56. [Google Scholar] [CrossRef] [Green Version]
- An, M.M.; Shen, H.; Zhang, J.D.; Xu, G.T.; Jiang, Y.Y. Linezolid versus vancomycin for meticillin-resistant Staphylococcus aureus infection: A meta-analysis of randomised controlled trials. Int. J. Antimicrob. Agents 2013, 41, 426–433. [Google Scholar] [CrossRef]
- Heidari, S.; Khalili, H. Linezolid pharmacokinetics: A systematic review for the best clinical practice. Eur. J. Clin. Pharmacol. 2023, 79, 195–206. [Google Scholar] [CrossRef] [PubMed]
- Tsuji, Y.; Holford, N.H.G.; Kasai, H.; Ogami, C.; Heo, Y.A.; Higashi, Y.; Mizoguchi, A.; To, H.; Yamamoto, Y. Population pharmacokinetics and pharmacodynamics of linezolid-induced thrombocytopenia in hospitalized patients. Br. J. Clin. Pharmacol. 2017, 83, 1758–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawasuji, H.; Tsuji, Y.; Ogami, C.; Kimoto, K.; Ueno, A.; Miyajima, Y.; Kawago, K.; Sakamaki, I.; Yamamoto, Y. Proposal of initial and maintenance dosing regimens with linezolid for renal impairment patients. BMC Pharmacol. Toxicol. 2021, 22, 13. [Google Scholar] [CrossRef]
- Kawasuji, H.; Tsuji, Y.; Ogami, C.; Kaneda, M.; Murai, Y.; Kimoto, K.; Ueno, A.; Miyajima, Y.; Fukui, Y.; Sakamaki, I.; et al. Initially reduced linezolid dosing regimen to prevent thrombocytopenia in hemodialysis patients. Antibiotics 2021, 10, 496. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists Pharmacists. Am. J. Health Syst. Pharm. 2020, 77, 835–864. [Google Scholar] [CrossRef] [Green Version]
- Matsumoto, K.; Oda, K.; Shoji, K.; Hanai, Y.; Takahashi, Y.; Fujii, S.; Hamada, Y.; Kimura, T.; Mayumi, T.; Ueda, T.; et al. Clinical practice guidelines for therapeutic drug monitoring of vancomycin in the framework of model-informed precision dosing: A consensus review by the Japanese society of chemotherapy and the Japanese society of therapeutic drug monitoring. Pharmaceutics 2022, 14, 489. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y.; Park, J.E.; Lee, Y.J.; Seo, H.J.; Sheen, S.S.; Hahn, S.; Jang, B.H.; Son, H.J. Testing a tool for assessing the risk of bias for nonrandomized studies showed moderate reliability and promising validity. J. Clin. Epidemiol. 2013, 66, 408–414. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Study Period | Country | Age (Years) | No. of Eligible Patients | Drug Regimen | VCM trough (mg/L) | Treatment Duration (days) | Bacteremia Source | Outcomes | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| LZD | VCM, TEIC, or DAP | LZD | VCM | TEIC | DAP | |||||||||
| Shorr 2005 [6] | Pooled analysis of five RCTs [23,24,25] | July 1998 to March 2003 | North and South America, Latin America, Europe, Israel, South Africa, Australia, and Asia (MC) | ≥13 | 36 | VCM 37 | 600 mg every 12 h iv, po | 1 g every 12 h iv a | - | - | NR | NR | Pneumonia [23,24], SSTI [25], UTI [25], other d [25] | MO, CC |
| Gómez 2007 [3] | Prospective observational study | January 2000 to December 2014 | Spain (SC) | Mean (range), LZD: 66 (15–95), VCM and TEIC: 58 (14–90) | 17 | VCM 49, TEIC 20 | NR | NR | NR | - | NR | NR | Overall (both LZD, VCM, and TEIC groups): venous catheters (40%), cutaneous (27%), unclear (28%), other (respiratory and urinary) (5%) | MO, MC, LOS |
| Wilcox 2009 [7] | RCT | May 2002 to August 2005 | Argentina, Australia, Austria, Belgium, Brazil, Chile, Colombia, Czech Republic, Germany, Greece, Guatemala, Hungary, India, Italy, Mexico, Pakistan, Peru, Philippines, Russian Federation, Slovakia, South Africa, Spain, Thailand, Turkey, United States, and Venezuela (MC) | ≥13 | 26 | VCM 21 | 600 mg every 12 h iv, po | 1 g every 12 h iv b | - | - | NR | NR | CRBSI | CC, MC |
| Caffrey 2010 [18] | Retrospective cohort study | January 2002 to June 2008 | Iceland (MC) | ≥18 | 82 | VCM 4498 | NR | NR | - | - | NR | NR | NR | MO, 90dRA |
| Wunderink 2012 [20] | RCT | October 2004 to January 2010 | United States, Europe, Asia, South America, and other (MC) | ≥18 | 9 | VCM 19 | 600 mg every 12 h iv | 15 mg/kg every 12 h c | - | - | Overall (not only bacteremia): median 12.3 (Day 3), 14.7 (Day 6), 16.1 (Day 9) | Overall (not only bacteremia): median 10 days in both LZD and VCM groups | Pneumonia | CC |
| Rose 2014 [21] | Subgroup analysis of one RCT [20] | October 2004 to January 2010 | United States, Europe, Asia, South America, and other (MC) | ≥18 | 22 | VCM 34 | 600 mg every 12 h iv | 15 mg/kg every 12 h c | - | - | Overall (not only bacteremia): median 12.3 (Day 3), 14.7 (Day 6), 16.1 (Day 9) | Overall (not only bacteremia): median 10 days in both LZD and VCM groups | Pneumonia | MO |
| Chong 2015 [22] | Prospective observational cohort study | August 2008 to April 2011 | Republic of Korea (SC) | Adult | 32 | VCM 82, TEIC 7 | NR | NR | NR | - | <15 mg/L 33/94 (35.1%) | NR | LZD: metastatic infection 10 (31.3%), IE 6 (18.8%), CRBSI 17 (53.1%), pneumonia 3 (9.4%), SSTI 1 (3.1%), BJI 3 (9.4%), POWI 1 (3.1%), PB 2 (6.3%); VCM and TEIC: metastatic infection 16 (18.0%), IE 6 (6.7%), CRBSI 42 (47.2%), pneumonia 8 (9.0%), SSTI 5 (5.6%), BJI 3 (3.4%), POWI 8 (9.0%), PB 11 (12.4%) | MO |
| Usery 2015 [8] | Retrospective cohort study | June 2008 to November 2010 | United States (SC) | Mean ± SD, LZD: 53.2 ± 18, VCM: 58.7 ± 15.5, DAP: 59.5 ± 16.2 | 15 | VCM 54, DAP 53 | 600 mg every 12 h | Mean ± SD, 13.6 ± 4 mg/kg/dose | - | Mean ± SD, 6.7 ± 1.8 mg/kg/day | > 15 mg/L 26/46 (56.5%) | Mean ± SD, LZD: 10.1 ± 3.2, VCM: 13.6 ± 7.1, DAP: 16.4 ± 9.6 | LZD: osteomyelitis 2 (13.3%), IE 0, pneumonia 5 (33.3%), VCM: osteomyelitis 7 (13.0%), IE 6 (11.1%), pneumonia 11 (20.4%), DAP: osteomyelitis 11 (20.8%), IE 6 (11.3%), pneumonia 3 (5.7%) | MO, CC, MC, 90dRA, LOS, recurrence |
| Yeager 2021 [9] | Retrospective cohort study | January 2011 to December 2019 | United States (SC) | Median (IQR), LZD: 56 (46–69), VCM and DAP: 48 (38–65) | 54 | VCM 100, DAP 61 | NR | NR | - | NR | NR | median (IQR) duration of total antibiotic therapy, LZD: 22 (17–35), VCM and DAP: 45 (29–49); definitive therapy, LZD: 14 (10–19), VCM and DAP: 39 (24–45) | LZD: BJI 3 (6%), IE 2 (4%), SSTI 24 (44%), CRBSI 3 (6%), pneumonia 13 (24%), other 6 (11%), multiple 3 (6%), VCM and DAP: BJI 29 (18%), IE 25 (16%), SSTI 50 (31%), CRBSI 22 (14%), pneumonia 12 (7%), other 13 (8%), multiple 10 (6%) | MO, LOS, recurrence, AEs |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawasuji, H.; Nagaoka, K.; Tsuji, Y.; Kimoto, K.; Takegoshi, Y.; Kaneda, M.; Murai, Y.; Karaushi, H.; Mitsutake, K.; Yamamoto, Y. Effectiveness and Safety of Linezolid Versus Vancomycin, Teicoplanin, or Daptomycin against Methicillin-Resistant Staphylococcus aureus Bacteremia: A Systematic Review and Meta-Analysis. Antibiotics 2023, 12, 697. https://doi.org/10.3390/antibiotics12040697
Kawasuji H, Nagaoka K, Tsuji Y, Kimoto K, Takegoshi Y, Kaneda M, Murai Y, Karaushi H, Mitsutake K, Yamamoto Y. Effectiveness and Safety of Linezolid Versus Vancomycin, Teicoplanin, or Daptomycin against Methicillin-Resistant Staphylococcus aureus Bacteremia: A Systematic Review and Meta-Analysis. Antibiotics. 2023; 12(4):697. https://doi.org/10.3390/antibiotics12040697
Chicago/Turabian StyleKawasuji, Hitoshi, Kentaro Nagaoka, Yasuhiro Tsuji, Kou Kimoto, Yusuke Takegoshi, Makito Kaneda, Yushi Murai, Haruka Karaushi, Kotaro Mitsutake, and Yoshihiro Yamamoto. 2023. "Effectiveness and Safety of Linezolid Versus Vancomycin, Teicoplanin, or Daptomycin against Methicillin-Resistant Staphylococcus aureus Bacteremia: A Systematic Review and Meta-Analysis" Antibiotics 12, no. 4: 697. https://doi.org/10.3390/antibiotics12040697