Approaches and Challenges for Biosensors for Acute and Chronic Heart Failure


 and
and 
Abstract
:1. Introduction
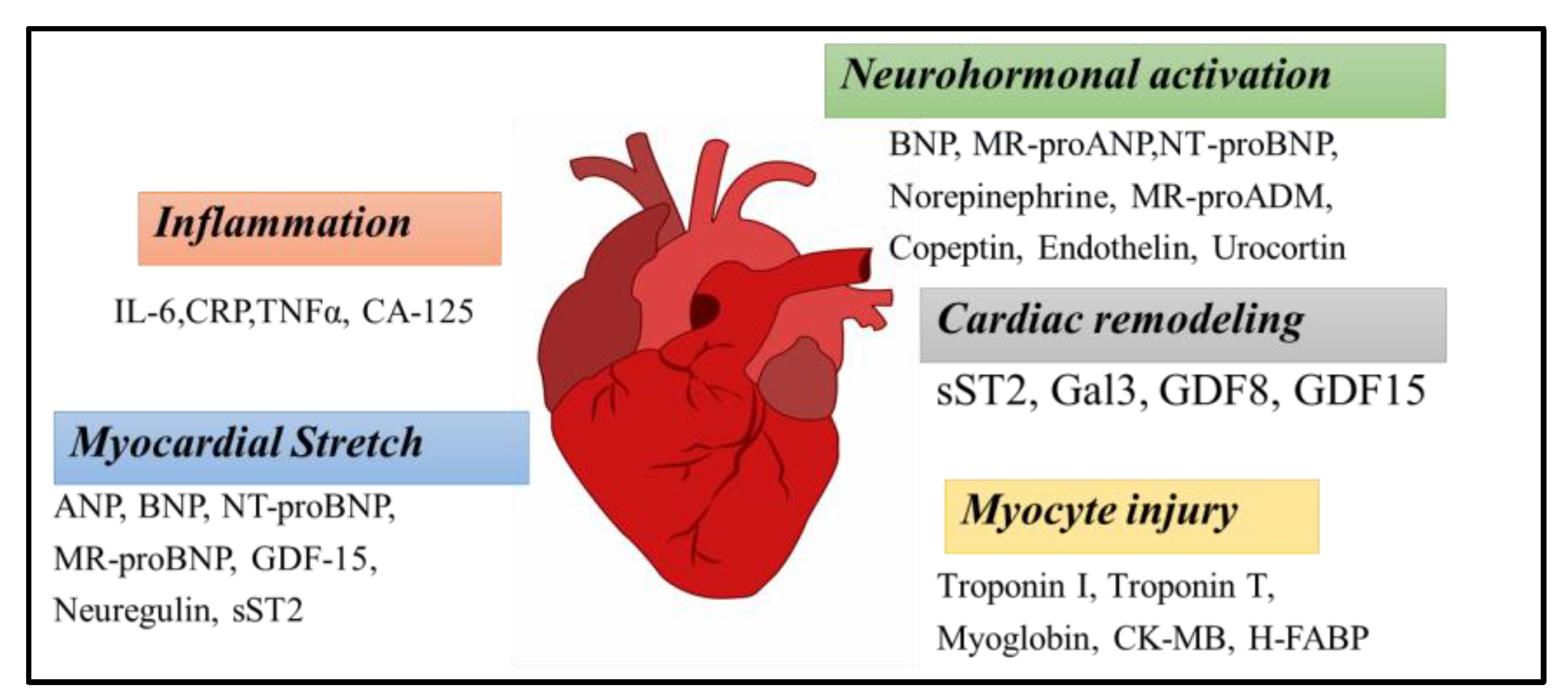
2. Heart Failure Biomarkers for Diagnosis and Therapy
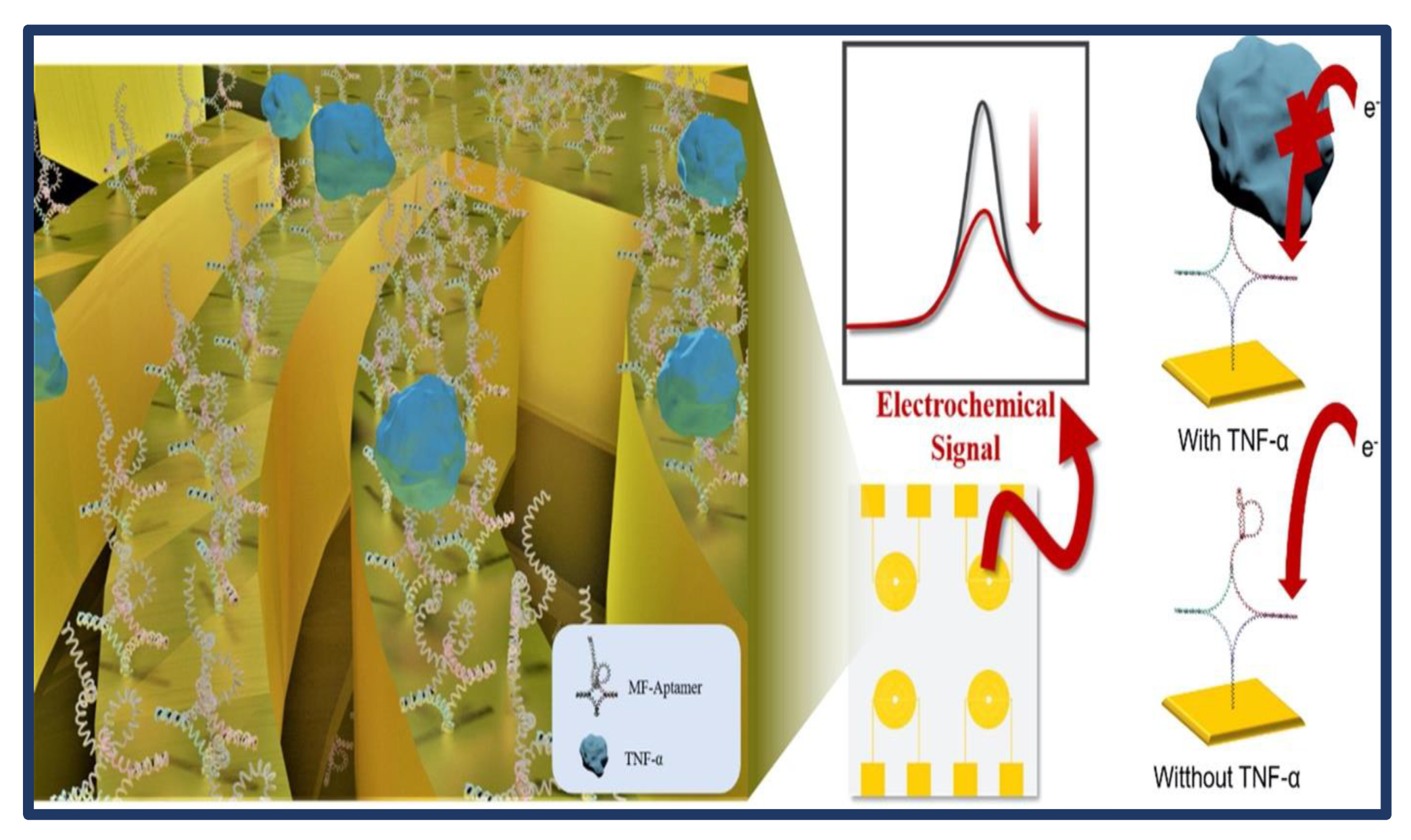
3. Applications of Biosensors for Acute and Chronic Heart Failure
4. Future Prospects
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Luo, Q.; Qian, X.; Mi, X.; Tu, Y. A Novel Electrochemiluminescent Immunosensor for the Detection of NT-ProBNP Based on a Au/ZIF-67 Nanocomposite. J. Electroanal. Chem. 2022, 912, 116260. [Google Scholar] [CrossRef]
- Ouyang, M.; Tu, D.; Tong, L.; Sarwar, M.; Bhimaraj, A.; Li, C.; Coté, G.L.; Di Carlo, D. A Review of Biosensor Technologies for Blood Biomarkers toward Monitoring Cardiovascular Diseases at the Point-of-Care. Biosens. Bioelectron. 2021, 171. [Google Scholar] [CrossRef] [PubMed]
- Ghantous, C.M.; Kamareddine, L.; Farhat, R.; Zouein, F.A.; Mondello, S.; Kobeissy, F.; Zeidan, A. Advances in Cardiovascular Biomarker Discovery. Biomedicines 2020, 8, 552. [Google Scholar] [CrossRef]
- Ataklte, F.; Vasan, R.S. Heart Failure Risk Estimation Based on Novel Biomarkers. Expert Rev. Mol. Diagn. 2021, 21, 655–672. [Google Scholar] [CrossRef] [PubMed]
- Maalouf, R.; Bailey, S. A Review on B-Type Natriuretic Peptide Monitoring: Assays and Biosensors. Heart Fail. Rev. 2016, 21, 567–578. [Google Scholar] [CrossRef] [Green Version]
- Sodeman, W.A., Jr.; Sodeman, T.C. Heart Failure: Patient and Caregiver’s Guide. In Instructions for Geriatric Patients; Saunders: Newberg, OR, USA, 2005; pp. 202–203. [Google Scholar]
- Teerlink, J.R.; Sliwa, K.; Opie, L.H. Heart Failure. In Drugs for the Heart; Opie, L.H., Gersh, B.J., Eds.; Saunders: Newberg, OR, USA, 2013; pp. 169–223. [Google Scholar]
- Correale, M.; Monaco, I.; Brunetti, N.D.; Di Biase, M.; Metra, M.; Nodari, S.; Butler, J.; Gheorghiade, M. Redefining Biomarkers in Heart Failure. Heart Fail. Rev. 2018, 23, 237–253. [Google Scholar] [CrossRef]
- Derosa, G.; Maffioli, P. Testing Pharmacological Profiles with Biomarkers Relevant to Cardiovascular Profiles. In Biomarkers in Cardiovascular Disease; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1–24. ISBN 9789400776777. [Google Scholar]
- Dhingra, R.; Vasan, R.S. Biomarkers in Cardiovascular Disease: Statistical Assessment and Section on Key Novel Heart Failure Biomarkers. Trends Cardiovasc. Med. 2017, 27, 123–133. [Google Scholar] [CrossRef] [Green Version]
- Puggia, I.; Rowland, T.J.; Miyamoto, S.D.; Sinagra, G.; Mestroni, L. Molecular and Cellular Mechanisms in Heart Failure. In Heart Failure in the Child and Young Adult: From Bench to Bedside; Elsevier Inc.: Amsterdam, The Netherlands, 2017; pp. 3–19. ISBN 9780128026137. [Google Scholar]
- Wettersten, N.; Maisel, A.S. Biomarker Developments in Heart Failure: 2016 and Beyond. Curr. Opin. Cardiol. 2019, 34, 218–224. [Google Scholar] [CrossRef]
- Joury, A.; Ventura, H.; Krim, S.R. Biomarkers in Heart Failure: Relevance in the Clinical Practice. Int. J. Cardiol. 2022, 363, 196–201. [Google Scholar] [CrossRef]
- Munief, W.M.; Lu, X.; Teucke, T.; Wilhelm, J.; Britz, A.; Hempel, F.; Lanche, R.; Schwartz, M.; Law, J.K.Y.; Grandthyll, S.; et al. Reduced Graphene Oxide Biosensor Platform for the Detection of NT-ProBNP Biomarker in Its Clinical Range. Biosens. Bioelectron. 2019, 126, 136–142. [Google Scholar] [CrossRef]
- Bellagambi, F.G.; Baraket, A.; Longo, A.; Vatteroni, M.; Zine, N.; Bausells, J.; Fuoco, R.; Di Francesco, F.; Salvo, P.; Karanasiou, G.S.; et al. Electrochemical Biosensor Platform for TNF-α Cytokines Detection in Both Artificial and Human Saliva: Heart Failure. Sens. Actuators B Chem. 2017, 251, 1026–1033. [Google Scholar] [CrossRef]
- Pourali, A.; Rashidi, M.R.; Barar, J.; Pavon-Djavid, G.; Omidi, Y. Voltammetric Biosensors for Analytical Detection of Cardiac Troponin Biomarkers in Acute Myocardial Infarction. TrAC Trends Anal. Chem. 2021, 134, 116123. [Google Scholar] [CrossRef]
- Azzouz, A.; Hejji, L.; Sonne, C.; Kim, K.H.; Kumar, V. Nanomaterial-Based Aptasensors as an Efficient Substitute for Cardiovascular Disease Diagnosis: Future of Smart Biosensors. Biosens. Bioelectron. 2021, 193, 113617. [Google Scholar] [CrossRef] [PubMed]
- Nadar, S.K.; Shaikh, M.M. Biomarkers in Routine Heart Failure Clinical Care. Card. Fail. Rev. 2019, 5, 50–56. [Google Scholar] [CrossRef] [Green Version]
- Yeboah, J.; Rodrigues, C.J.; Qureshi, W.; Liu, S.; Car, J.J.; Lima, J.A.; Hundley, W.G.; Herrington, D.M. Prognosis of Low Normal Left Ventricular Ejection Fraction in an Asymptomatic Population-Based Adult Cohort. J. Card. Fail. 2016, 22, 763–768. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, N.E.; Januzzi, J.L. Established and Emerging Roles of Biomarkers in Heart Failure. Circ. Res. 2018, 123, 614–629. [Google Scholar] [CrossRef]
- Chia, Y.C.; Kieneker, L.M.; van Hassel, G.; Binnenmars, S.H.; Nolte, I.M.; van Zanden, J.J.; van der Meer, P.; Navis, G.; Voors, A.A.; Bakker, S.J.L.; et al. Interleukin 6 and Development of Heart Failure with Preserved Ejection Fraction in the General Population. J. Am. Heart Assoc. 2021, 10. [Google Scholar] [CrossRef]
- Prasad, S.; Tyagi, A.K.; Aggarwal, B.B. Detection of Inflammatory Biomarkers in Saliva and Urine: Potential in Diagnosis, Prevention, and Treatment for Chronic Diseases. Exp. Biol. Med. 2016, 241, 783–799. [Google Scholar] [CrossRef] [Green Version]
- Aydin, S.; Ugur, K.; Aydin, S.; Sahin, İ.; Yardim, M. Biomarkers in Acute Myocardial Infarction: Current Perspectives. Vasc. Health Risk Manag. 2019, 15, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Biasucci, L.M.; Maino, A.; Grimaldi, M.C.; Cappannoli, L.; Aspromonte, N. Novel Biomarkers in Heart Failure: New Insight in Pathophysiology and Clinical Perspective. J. Clin. Med. 2021, 10, 2771. [Google Scholar] [CrossRef]
- Badianyama, M.; Mpanya, D.; Adamu, U.; Sigauke, F.; Nel, S.; Tsabedze, N. New Biomarkers and Their Potential Role in Heart Failure Treatment Optimisation—An African Perspective. J. Cardiovasc. Dev. Dis. 2022, 9, 335. [Google Scholar] [CrossRef] [PubMed]
- Kanukurti, J.; Mohammed, N.; Sreedevi, N.N.; Khan, S.A.; Baba, K.S.S.S.; Bhaskar, M.V.; Satish, O.S.; Naushad, S.M.; Mohan, I.K. Evaluation of Galectin-3 as a Novel Diagnostic Biomarker in Patients with Heart Failure with Preserved Ejection Fraction. J. Lab. Physicians 2020, 12, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Dou, Y.H.; Haswell, S.J.; Greenman, J.; Wadhawan, J. Voltammetric Immunoassay for the Detection of Protein Biomarkers. Electroanalysis 2012, 24, 264–272. [Google Scholar] [CrossRef]
- Sato, Y.; Kita, T.; Takatsu, Y.; Kimura, T. Biochemical Markers of Myocyte Injury in Heart Failure. Heart 2004, 90, 1110–1113. [Google Scholar] [CrossRef]
- Mallick, A.; Januzzi, J.L. Biomarkers in Acute Heart Failure. Rev. Española Cardiol. Engl. Ed. 2015, 68, 514–525. [Google Scholar] [CrossRef]
- Shrivastava, A.; Haase, T.; Zeller, T.; Schulte, C. Biomarkers for Heart Failure Prognosis: Proteins, Genetic Scores and Non-Coding RNAs. Front. Cardiovasc. Med. 2020, 7, 601364. [Google Scholar] [CrossRef]
- Castiglione, V.; Aimo, A.; Vergaro, G.; Saccaro, L.; Passino, C.; Emdin, M. Biomarkers for the Diagnosis and Management of Heart Failure. Heart Fail. Rev. 2022, 625–643. [Google Scholar] [CrossRef]
- Komarova, N.; Panova, O.; Titov, A.; Kuznetsov, A. Aptamers Targeting Cardiac Biomarkers as an Analytical Tool for the Diagnostics of Cardiovascular Diseases: A Review. Biomedicines 2022, 10, 1085. [Google Scholar] [CrossRef]
- Razmshoar, P.; Bahrami, S.H.; Rabiee, M.; Hangouet, M.; Martin, M.; Errachid, A.; Jaffrezic-renault, N. A Novel Electrochemical Immunosensor for Ultrasensitive Detection of Tumor Necrosis Factor α Based on Polystyrene—PAMAM Dendritic Polymer Blend Nanofibers. Microchem. J. 2022, 175, 107206. [Google Scholar] [CrossRef]
- Mayer, M.D.; Lai, R.Y. Eff Ects of Redox Label Location on the Performance of an Electrochemical Aptamer-Based Tumor Necrosis Factor-Alpha Sensor. Talanta 2018, 189, 585–591. [Google Scholar] [CrossRef]
- Yola, M.L.; Atar, N. Novel Voltammetric Tumor Necrosis Factor-Alpha (TNF-α) Immunosensor Based on Gold Nanoparticles Involved in Thiol-Functionalized Multi-Walled Carbon Nanotubes and Bimetallic Ni/Cu-MOFs. Anal. Bioanal. Chem. 2021, 413, 2481–2492. [Google Scholar] [CrossRef] [PubMed]
- Ghalehno, M.H.; Mirzaei, M.; Torkzadeh-mahani, M. Aptamer-Based Determination of Tumor Necrosis Factor α Using a Screen-Printed Graphite Electrode Modified with Gold Hexacyanoferrate. Microchim. Acta 2018, 185, 165. [Google Scholar] [CrossRef]
- Aydin, E.B.; Aydin, M.; Sezgintürk, M.K. A Label-Free Electrochemical Immunosensor for Highly Sensitive Detection of TNF α, Based on Star Polymer-Modified Disposable ITO Electrode. Curr. Pharm. Anal. 2021, 17, 450–459. [Google Scholar] [CrossRef]
- Kim, J.; Woo, S.; Park, C.; Lee, J.; Cho, H.; Min, J.; Lee, T. Fabrication of Electrochemical Biosensor Composed of Multi-Functional DNA 4 Way Junction for TNF- a Detection in Human Serum. Bioelectrochemistry 2021, 142, 107939. [Google Scholar] [CrossRef] [PubMed]
- Aydın, E.B. A Label-Free and Sensitive Impedimetric Immunosensor for TNF α Biomarker Detection Based on Epoxysilane-Modified Disposable ITO-PET Electrode. Int. J. Environ. Anal. Chem. 2020, 100, 363–377. [Google Scholar] [CrossRef]
- Longo, A.; Baraket, A.; Vatteroni, M.; Zine, N.; Di Francesco, F.; Karanasiou, G.S.; Dimitrios, I.; Menciassi, A.; Errachid, A. Highly Sensitive Electrochemical BioMEMS for TNF- Į Detection in Humansaliva: Heart Failure. Procedia Eng. 2016, 168, 97–100. [Google Scholar] [CrossRef]
- Meftah, M.; Habel, A.; Baachaoui, S.; Yaacoubi, B.; Noureddine, L. Sensitive Electrochemical Detection of Polymorphisms in IL6 and TGFβ1 Genes from Ovarian Cancer DNA Patients Using EcoRI and DNA Hairpin—Modified Gold Electrodes. Microchim. Acta 2023, 190, 15. [Google Scholar] [CrossRef]
- Zhao, C.; Xiao, J.; Liu, T.; Shi, H.; Li, Q.; Ruan, Z. Electrochemical Sensor Based on Glass Carbon Electrode Modified With Graphene Quantum Dots ( GQDs ) for Detection of Uric Acid. Int. J. Electrochem. Sci. 2022, 17, 2. [Google Scholar] [CrossRef]
- Cerqueira, S.M.V.; Fernandes, R.; Moreira, F.T.C.; Sales, M.G.F. Development of an Electrochemical Biosensor for Galectin-3 Detection in point-of-care. Microchem. J. 2021, 164, 105992. [Google Scholar] [CrossRef]
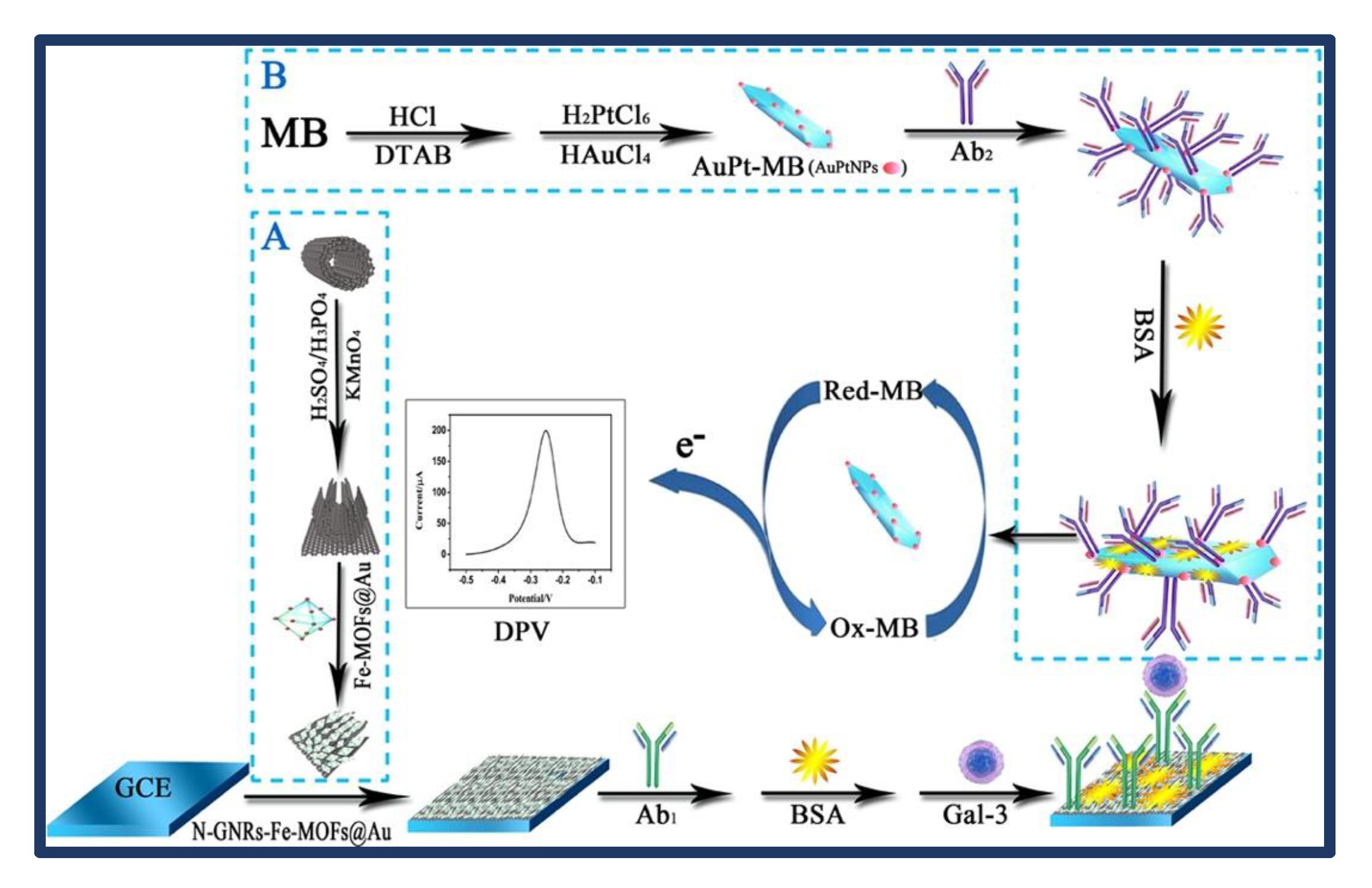
- Tang, Z.; He, J.; Chen, J.; Niu, Y.; Zhao, Y.; Zhang, Y.; Yu, C. A Sensitive Sandwich-Type Immunosensor for the Detection of Galectin-3 Based on N-GNRs-Fe-MOFs @ AuNPs Nanocomposites and a Novel AuPt- Methylene Blue Nanorod. Biosens. Bioelectron. 2018, 101, 253–259. [Google Scholar] [CrossRef]
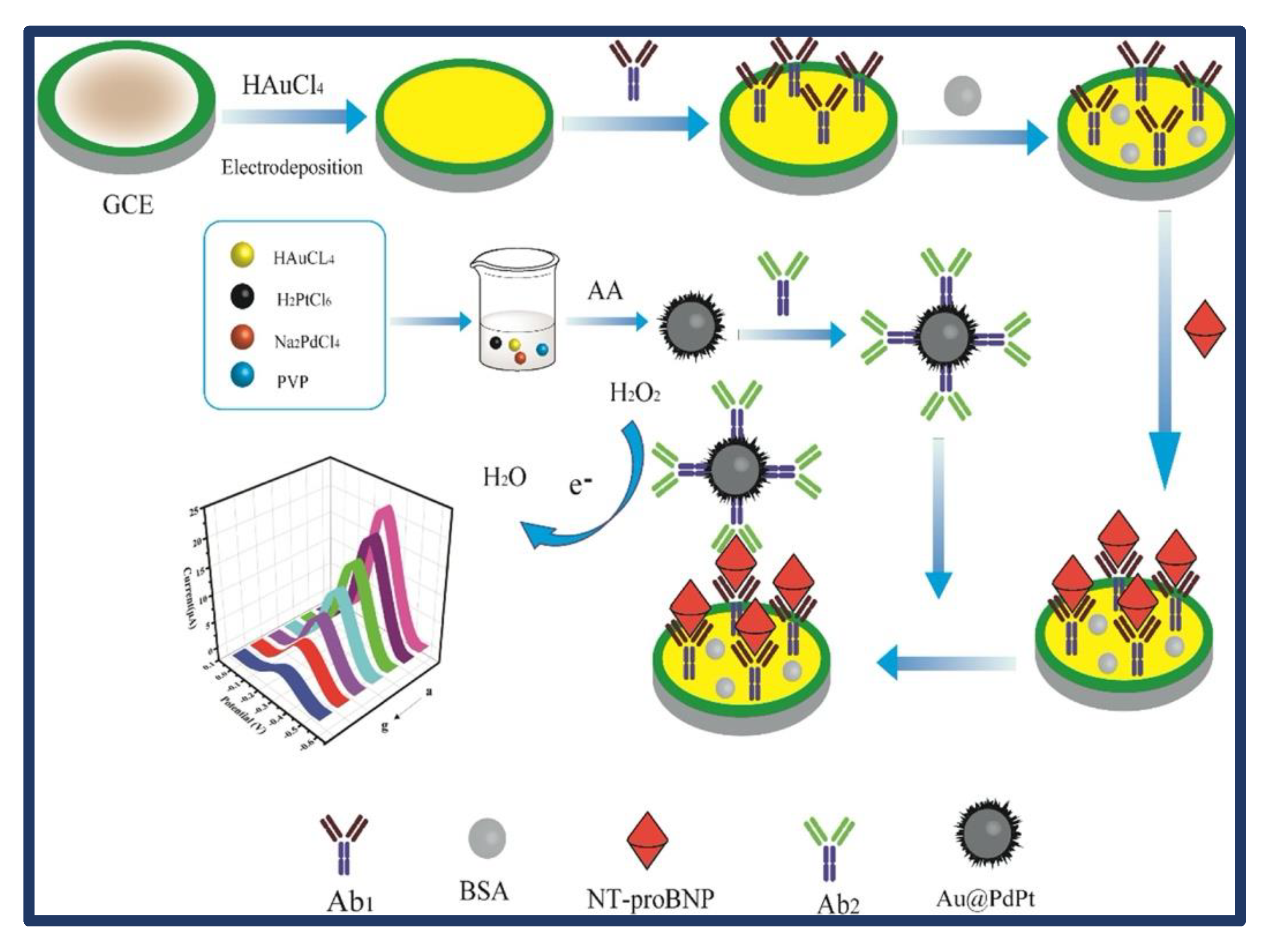
- Zhang, B.; Li, F.; Han, F.; Yang, H.; Jiang, C.; Tan, S.; Tu, J.; Qiao, B.; Wang, X.; Wu, Q. A Sandwich-Type Electrochemical Immunosensor Using Trimetallic Nanozyme as Signal Amplification for NT-ProBNP Sensitive Detection. Bioelectrochemistry 2022, 145, 108075. [Google Scholar] [CrossRef] [PubMed]
- Ben, H.; Bellagambi, F.G.; Hangou, M.; Alcacer, A.; Pfeiffer, N.; Heuberger, A.; Zine, N.; Bausells, J.; Elaissari, A.; Errachid, A. Talanta A Novel Electrochemical Strategy for NT-ProBNP Detection Using IMFET for Monitoring Heart Failure by Saliva Analysis. Talanta 2023, 251, 123759. [Google Scholar] [CrossRef]
- Demirbakan, B.; Sezgintürk, M.K. An Impedimetric Biosensor System Based on Disposable Graphite Paper Electrodes: Detection of ST2 as a Potential Biomarker for Cardiovascular Disease in Human Serum. Anal. Chim. Acta 2021, 1144, 43–52. [Google Scholar] [CrossRef]
- Shrestha, B.K.; Ahmad, R.; Shrestha, S.; Park, C.H.; Kim, C.S. In Situ Synthesis of Cylindrical Spongy Polypyrrole Doped Protonated Graphitic Carbon Nitride for Cholesterol Sensing Application. Biosens. Bioelectron. 2017, 94, 686–693. [Google Scholar] [CrossRef] [PubMed]
- Verma, N.V.; Tiwari, B.S.; Pandya, A. Paper Disc Interfaced Prussian Blue Nanocube Modified Immunodevice for Electrochemical Detection of Diverse Biomarker at Point of Care. Bioelectrochemistry 2023, 150, 108346. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Liu, Z.; Yan, Y.; Chen, J.; Yang, R.; Huang, Q.; Jin, M.; Shui, L. Triple Signal-Enhancing Electrochemical Aptasensor Based on Rhomboid Dodecahedra Carbonized-ZIF 67 for Ultrasensitive CRP Detection. Biosens. Bioelectron. 2022, 207, 114129. [Google Scholar] [CrossRef]
- Dong, S.; Zhang, D.; Cui, H.; Huang, T. ZnO/Porous Carbon Composite from a Mixed-Ligand MOF for Ultrasensitive Electrochemical Immunosensing of C-Reactive Protein. Sensors Actuators B Chem. 2019, 284, 354–361. [Google Scholar] [CrossRef]
- Pinyorospathum, C.; Chaiyo, S.; Sae-ung, P.; Hoven, V.P.; Damsongsang, P. Disposable Paper-Based Electrochemical Sensor Using for the Label-Free Detection of C-Reactive Protein. Microchim. Acta 2019, 186, 1–3. [Google Scholar] [CrossRef]
- Kowalczyk, A.; Jakub, P.S.; Kasprzak, A.; Poplawska, M.; Grudzinski, I.P.; Nowicka, A.M. Occlusion Phenomenon of Redox Probe by Protein as a Way of Voltammetric Detection of Non-Electroactive C-Reactive Protein. Biosens. Bioelectron. 2018, 117, 232–239. [Google Scholar] [CrossRef]
- Sun, S.; Luo, J.; Zhu, Y.; Kong, F.; Mao, G.; Ming, T.; Xing, Y.; Liu, J.; Dai, Y.; Yan, S.; et al. Multifunctional Self-Driven Origami Paper-Based Integrated Microfluidic Chip to Detect CRP and PAB in Whole Blood. Biosens. Bioelectron. 2022, 208, 114225. [Google Scholar] [CrossRef]
- Cheng, Y.; Zhan, T.; Feng, X.; Han, G. A Synergistic Effect of Gold Nanoparticles and Melamine with Signal Ampli Fi Cation for C-Reactive Protein Sensing. J. Electroanal. Chem. 2021, 895, 115417. [Google Scholar] [CrossRef]
- Arruza, L.; Angel, M. On-the-Fly Rapid Immunoassay for Neonatal Sepsis Diagnosis: C-Reactive Protein Accurate Determination Using Magnetic Graphene-Based Micromotors. Biosens. Bioelectron. 2020, 158, 112156. [Google Scholar] [CrossRef]
- Jang, Y.; Kim, H.; Yang, S.Y.; Jung, J.; Oh, J. Bioactive Multiple-Bent MWCNTs for Sensitive and Reliable Electrochemical Detection of Picomolar- Level C-Reactive Proteins. Nanoscale 2020, 12, 9980–9990. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, S.H.D.; Alves, L.M.; Flauzino, J.M.R.; Moço, A.C.R.; Segatto, M.S. Reusable Immunosensor for Detection of C-Reactive Protein in Human Serum. Electroanalysis 2020, 32, 2316–2322. [Google Scholar] [CrossRef]
- Vilian, A.T.E.; Kim, W.; Park, B.; Yeong, S.; Kim, T.; Suk, Y.; Kwon, C.; Han, Y. Efficient Electron-Mediated Electrochemical Biosensor of Gold Wire for the Rapid Detection of C-Reactive Protein: A Predictive Strategy for Heart Failure. Biosens. Bioelectron. 2019, 142, 111549. [Google Scholar] [CrossRef]
- Gür, B.; Emre, M.; Gür, F.; Kalita, G.; Tanemura, M.; Hakkı, M. Silver Nanoparticle Doped Graphene-Based Impedimetric Biosensor towards Sensitive Detection of Procalcitonin. Mater. Chem. Phys. 2023, 297, 127339. [Google Scholar] [CrossRef]
- Au, M.; Liu, J.; Quan, L.; Yu, X.; Wang, L. Quantitative Detection of Procalcitonin Using an Electrochemical Immunosensor Based On. Analyst 2019, 144, 6968–6974. [Google Scholar] [CrossRef]
- Xu, X.; Li, X.; Miao, J.; Liu, L.; Huang, X.; Wei, Q.; Cao, W. A Dual-Mode Label-Free Electrochemical Immunosensor for Ultrasensitive Detection of Procalcitonin Based on g-C3N4-NiCo2S4-CNTs-Ag NPs. Analyst 2021, 146, 3169–3176. [Google Scholar] [CrossRef]
- Raj, N.; Crooks, R.M. Detection Efficiency of Ag Nanoparticle Labels for a Heart Failure Marker Using Linear and Square-Wave Anodic Stripping Voltammetry. Biosensors 2022, 12, 203. [Google Scholar] [CrossRef]
- Serafín, V.; Torrente-Rodríguez, R.M.; González-Cortés, A.; García de Frutos, P.; Sabaté, M.; Campuzano, S.; Yáñez-Sedeño, P.; Pingarrón, J.M. An Electrochemical Immunosensor for Brain Natriuretic Peptide Prepared with Screen-Printed Carbon Electrodes Nanostructured with Gold Nanoparticles Grafted through Aryl Diazonium Salt Chemistry. Talanta 2018, 179, 131–138. [Google Scholar] [CrossRef]
- Hu, X.; Zhang, N.; Shen, L.; Yu, L.; Huang, L.; Wang, A.; Shan, D.; Yuan, P.; Feng, J. The Enhanced Photoelectrochemical Platform Constructed by N-Doped ZnO Nanopolyhedrons and Porphyrin for Ultrasensitive Detection of Brain Natriuretic Peptide. Anal. Chim. Acta 2021, 1183, 338870. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Liu, L.; Dong, X.; Zhao, G.; Li, Y.; Miao, J.; Fang, J.; Cui, M.; Wei, Q.; Cao, W. Dual Mode Competitive Electrochemical Immunoassay for B-Type Natriuretic Peptide Based on GS/SnO 2 /Polyaniline-Au and ZnCo 2 O 4 /N-CNTs. Biosens. Bioelectron. 2019, 126, 448–454. [Google Scholar] [CrossRef] [PubMed]
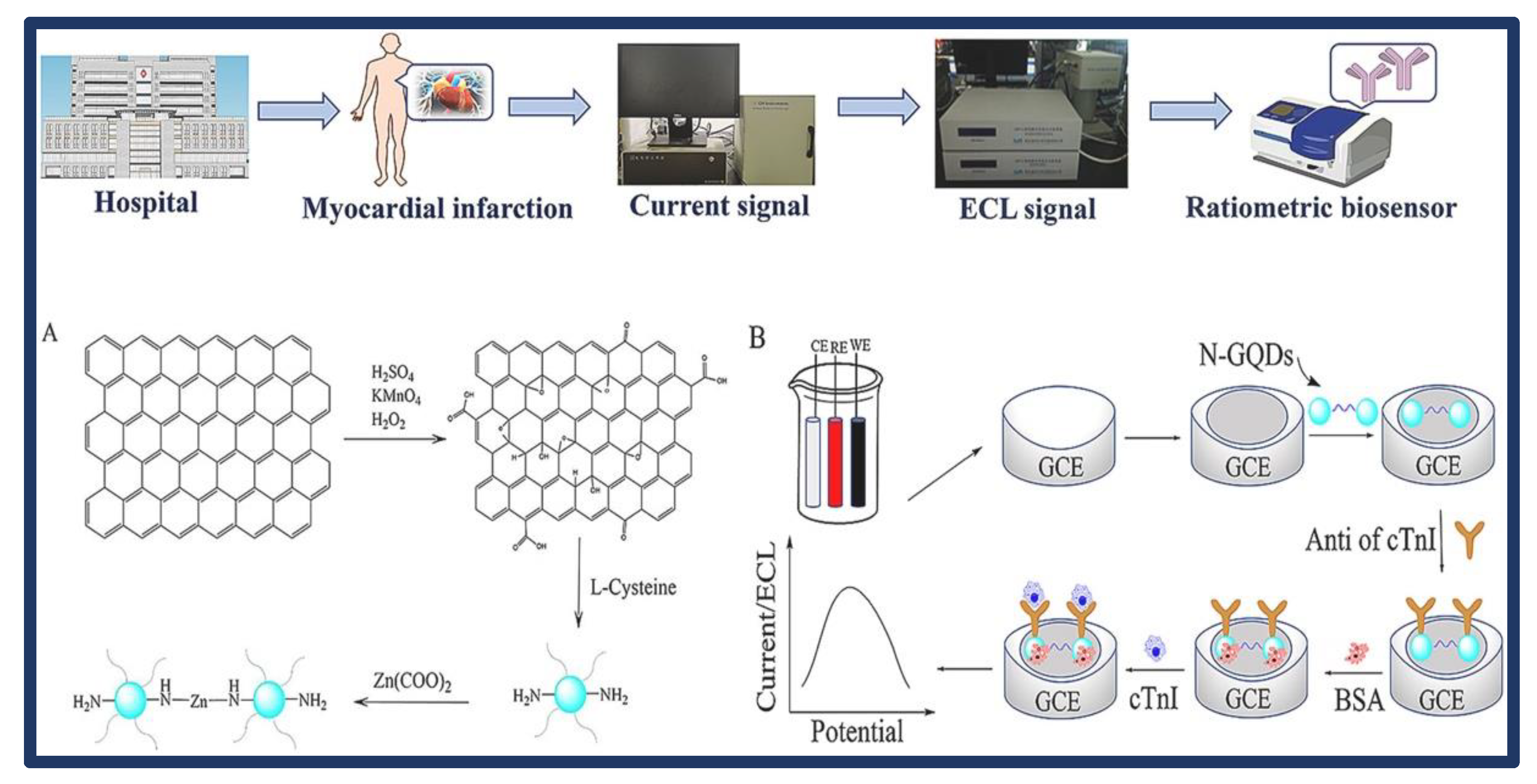
- Liu, M.; Jiang, R.; Zheng, M.; Li, M.; Yu, Q. A Sensitive Ratiometric Biosensor for Determination Cardiac Troponin I of Myocardial Infarction Markers Based on N, Zn-GQDs. Talanta 2022, 249, 123577. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari, Z.; Khajehshari, H.; Hashemnia, S.; Solati, Z.; Azimpanah, R. Evaluation of Molecular Imprinted Polymerized Methylene Blue/Aptamer as a Novel Hybrid Receptor for Cardiac Troponin I ( CTnI ) Detection at Glassy Carbon Electrodes Modi Fi Ed with New Biosynthesized ZnONPs. Sensors Actuators B Chem. 2020, 320, 128316. [Google Scholar] [CrossRef]
- Song, Z.; Song, J.; Gao, F.; Chen, X.; Wang, Q.; Zhao, Y.; Huang, X.; Yang, C.; Wang, Q. Novel Electroactive Ferrocene-Based Covalent Organic Frameworks towards Electrochemical Label-Free Aptasensors for the Detection of Cardiac Troponin I. Sens. Actuators B Chem. 2022, 368, 132205. [Google Scholar] [CrossRef]
- Khushaim, W.; Peramaiah, K.; Beduk, T.; Teja, M.; Filho, D.O.; Huang, K.; Mani, V.; Nabil, K. Porous Graphitic Carbon Nitrides Integrated Biosensor for Sensitive Detection of Cardiac Troponin I. Biosens. Bioelectron. X 2022, 12, 100234. [Google Scholar] [CrossRef]
- Ahmadi, A.; Mehdi, S.; Mirzaeizadeh, Z.; Kabiri, S.; Rezaie, J.; Omidfar, K. Electrochemical Immunosensor for Determination of Cardiac Troponin I Using Two-Dimensional Metal-Organic Framework/Fe3O4—COOH Nanosheet Composites Loaded with Thionine and p CTAB/DES Modified Electrode. Talanta 2022, 237, 122911. [Google Scholar] [CrossRef]
- Chekin, F.; Vasilescu, A.; Jijie, R.; Singh, S.K.; Kurungot, S.; Iancu, M.; Badea, G.; Boukherroub, R.; Szunerits, S. Sensitive Electrochemical Detection of Cardiac Troponin I in Serum and Saliva by Nitrogen-Doped Porous Reduced Graphene Oxide Electrode. Sens. Actuators B Chem. 2018, 262, 180–187. [Google Scholar] [CrossRef]
- Yan, H.; Tang, X.; Zhu, X.; Zeng, Y.; Lu, X.; Yin, Z.; Lu, Y.; Yang, Y.; Li, L. Sandwich-Type Electrochemical Immunosensor for Highly Sensitive Determination of Cardiac Troponin I Using Carboxyl-Terminated Ionic Liquid and Helical Carbon Nanotube Composite as Platform and Ferrocenecarboxylic Acid as Signal Label. Sens. Actuators B Chem. 2018, 277, 234–240. [Google Scholar] [CrossRef]
- Lopa, N.S.; Rahman, M.M.; Ahmed, F.; Ryu, T.; Sutradhar, S.C.; Lei, J.; Kim, J.; Kim, D.H.; Lee, Y.H.; Kim, W. Simple, Low-Cost, Sensitive and Label-Free Aptasensor for the Detection of Cardiac Troponin I Based on a Gold Nanoparticles Modified Titanium Foil. Biosens. Bioelectron. 2019, 126, 381–388. [Google Scholar] [CrossRef]
- Lee, T.; Lee, Y.; Park, S.Y.; Hong, K.; Kim, Y.; Park, C.; Chung, Y.H.; Lee, M.H.; Min, J. Fabrication of Electrochemical Biosensor Composed of Multi-Functional DNA Structure/Au Nanospike on Micro-Gap/PCB System for Detecting Troponin I in Human Serum. Colloids Surf. B Biointerfaces 2019, 175, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Yola, M.L.; Atar, N. Development of Cardiac Troponin-I Biosensor Based on Boron Nitride Quantum Dots Including Molecularly Imprinted Polymer. Biosens. Bioelectron. 2019, 126, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.; Rabiee, M.; Tahriri, M.; Salarian, R.; Tayebi, L. A Graphene Based–Biomimetic Molecularly Imprinted Polyaniline Sensor for Ultrasensitive Detection of Human Cardiac Troponin T (CTnT). Synth. Met. 2019, 256, 116136. [Google Scholar] [CrossRef]
- Phonklam, K.; Wannapob, R.; Sriwimol, W.; Thavarungkul, P.; Phairatana, T. A Novel Molecularly Imprinted Polymer PMB/MWCNTs Sensor for Highly-Sensitive Cardiac Troponin T Detection. Sens. Actuators B Chem. 2020, 308, 127630. [Google Scholar] [CrossRef]
- Karaman, C.; Bölükbaşı, Ö.S.; Bankoğlu Yola, B.; Karaman, O.; Atar, N.; Yola, M.L. Electrochemical Neuron-Specific Enolase (NSE) Immunosensor Based on CoFe2O4@Ag Nanocomposite and AuNPs@ MoS2/RGO. Anal. Chim. Acta 2022, 1200, 339609. [Google Scholar] [CrossRef]
- Yu, X.; Li, Y.; Li, Y.; Liu, S.; Wu, Z.; Dong, H.; Xu, Z. An Electrochemical Amplification Strategy Based on the Ferrocene Functionalized Cuprous Oxide Superparticles for the Detection of NSE. Talanta 2022, 236, 122865. [Google Scholar] [CrossRef]
- Dong, H.; Liu, S.; Liu, Q.; Li, Y.; Li, Y.; Zhao, Z. A Dual-Signal Output Electrochemical Immunosensor Based on Au–MoS2/MOF Catalytic Cycle Amplification Strategy for Neuron-Specific Enolase Ultrasensitive Detection. Biosens. Bioelectron. 2022, 195, 113648. [Google Scholar] [CrossRef]
- Sadrjavadi, K.; Taran, M.; Fattahi, A.; Khoshroo, A. A Microelectrode System for Simple Measurement of Neuron Specific Enolase with Photolithography Technique. Microchem. J. 2022, 182, 107889. [Google Scholar] [CrossRef]
- Chen, M.; Zhao, L.; Wu, D.; Tu, S.; Chen, C.; Guo, H.; Xu, Y. Highly Sensitive Sandwich-Type Immunosensor with Enhanced Electrocatalytic Durian-Shaped MoS2/AuPtPd Nanoparticles for Human Growth Differentiation Factor-15 Detection. Anal. Chim. Acta 2022, 1223, 340194. [Google Scholar] [CrossRef]
- Fang, D.; Tang, S.; Wu, Z.; Chen, C.; Wan, M.; Mao, C.; Zhou, M. Electrochemical Sensor Based on Micromotor Technology for Detection of Ox-LDL in Whole Blood. Biosens. Bioelectron. 2022, 217, 114682. [Google Scholar] [CrossRef]
- Liu, H.; Cheng, Y.; Chen, Y.; Xiao, H.; Sui, Y.; Xie, Q.; Liu, R.; Yang, X. Dual-Signal Sandwich-Type Electrochemical Immunoassay of Galectin-3 Using Methylene Blue and Gold Nanoparticles Biolabels. J. Electroanal. Chem. 2020, 861, 113952. [Google Scholar] [CrossRef]
- Roger, V.L. Heart Failure. In International Encyclopedia of Public Health; Academic Press: Cambridge, MA, USA, 2016; Volume 3, pp. 520–526. ISBN 9780128037089. [Google Scholar]
- DeVore, A.D.; Wosik, J.; Hernandez, A.F. The Future of Wearables in Heart Failure Patients. JACC Hear. Fail. 2019, 7, 922–932. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Analyte | Sensor | Technique | Linear Range | LOD | RSD (%) | Real Sample | Recovery | Ref |
|---|---|---|---|---|---|---|---|---|
| TNFα | Anti-TNFα/BSA/PAMAM/ NFs-AuE | CV EIS | 10–200 pg/mL | 669 fg/mL | NR | Human serum Saliva | NR | [33] |
| TNFα | AuE | ACV | 0.1–500 nM | 100 pM | NR | Urine Saliva | NR | [34] |
| TNFα | TNFα/anti-TNFα-Ab1/AuNPs/S-MWCNTs/GCE | CV EIS | 0.01–1.0 pg/mL | 2.00 fg/mL | 0.61 | Human plasma | 100 | [35] |
| TNFα | AuHCF-AuNPs/SPE | DPV | 10 pg/mL–40μg/mL | 5.5 pg/mL | 0.46 | Human serum | NR | [36] |
| TNFα | ITO Electrode | EIS CV | 0.02–4 pg/mL | 6 fg/mL | NR | Human serum | 97.07–100.19 | [37] |
| TNFα | PDMS/AuE- ITO | CV | 0.15 pg/mL–15 ng/mL | 0.07 pg/mL | NR | Human serum | NR | [38] |
| TNFα | GPTES-ITO-PET | CV EIS | 0.01–1.5 pg/mL | 3.1 fg/mL | 0.87 | Human Serum | 96.51–100.90 | [39] |
| TNFα α | AuE (microelectrodes) | CV EIS | NR | 1–15 pg/mL | NR | Human Saliva | NR | [40] |
| IL6 TGFβ1 | AuNP-SPE | DPV | 102−108 fM 50−105 fM | 47.9 fM 16.6 fM | NR | Human DNA | NR | [41] |
| Uric acid | GCE | DPV CV | 10–1000 μmol/L | 107 nmol/L | 0.3–8.5 | Human serum | 95.8–104 | [42] |
| Gal-3 | MIPs/SPE | CV EIS | 0.5−5000 ng/mL | NR | NR | Human Serum | NR | [43] |
| Gal-3 | N-GNRs-Fe-MOFs@AuNPs/GCE | DPV | 100 fg/mL−50 ng/mL | 33.33 fg/mL | 2.75 | Human plasma | 98.91–104.84 | [44] |
| NT-proBNP | Au@PdPtRTNs/GCE | Amperometry CV EIS | 0.1 pg/mL–100 ng/mL | 0.046 pg/mL | 3–5.4 | Human Serum | 98.7–101.3 | [45] |
| NT-proBNP | SPE, Pt counter electrode | EIS | 0.02–1 pg/mL | 0.02 pg/mL | NR | Saliva | 99 ± 8 | [46] |
| ST2 | GP Electrode | EIS CV | 0.1 fg/mL−100 fg/mL | 0.124 fg/mL | 1.16–15.59 | Human Serum | 100–113.46 | [47] |
| Cholesterol | ChOx- CSPPy-g-C3N4H+/GCE | CV | 0.02–5.0 Mm | 8.0 µM | 1.8–2.7 | Human Serum | 97–101 | [48] |
| CRP | SPCE | CV EIS DPV | 800,000−0.008 µM | 0.92 nM | NR | Leaf | 106.11–107.05 | [49] |
| CRP | GCE | CV DPV | 10 pg/mL–10 μg/mL | 0.44 pg/mL | 5.93–12.02 | Human Serum | NR | [50] |
| CRP | BSA/ZnO/MPC/IL/anti-CRP/CPE | EIS DPV | 0.01–1000 ng/mL | 0.005 ng/mL | <6 | Human Serum | 94.5–107.0 | [51] |
| CRP | PMPC-SH/SAM/AuNPs/SPCE | DPV | 5–5000 ng/mL | 1.6 ng/mL | <1.34 | Human Serum | NR | [52] |
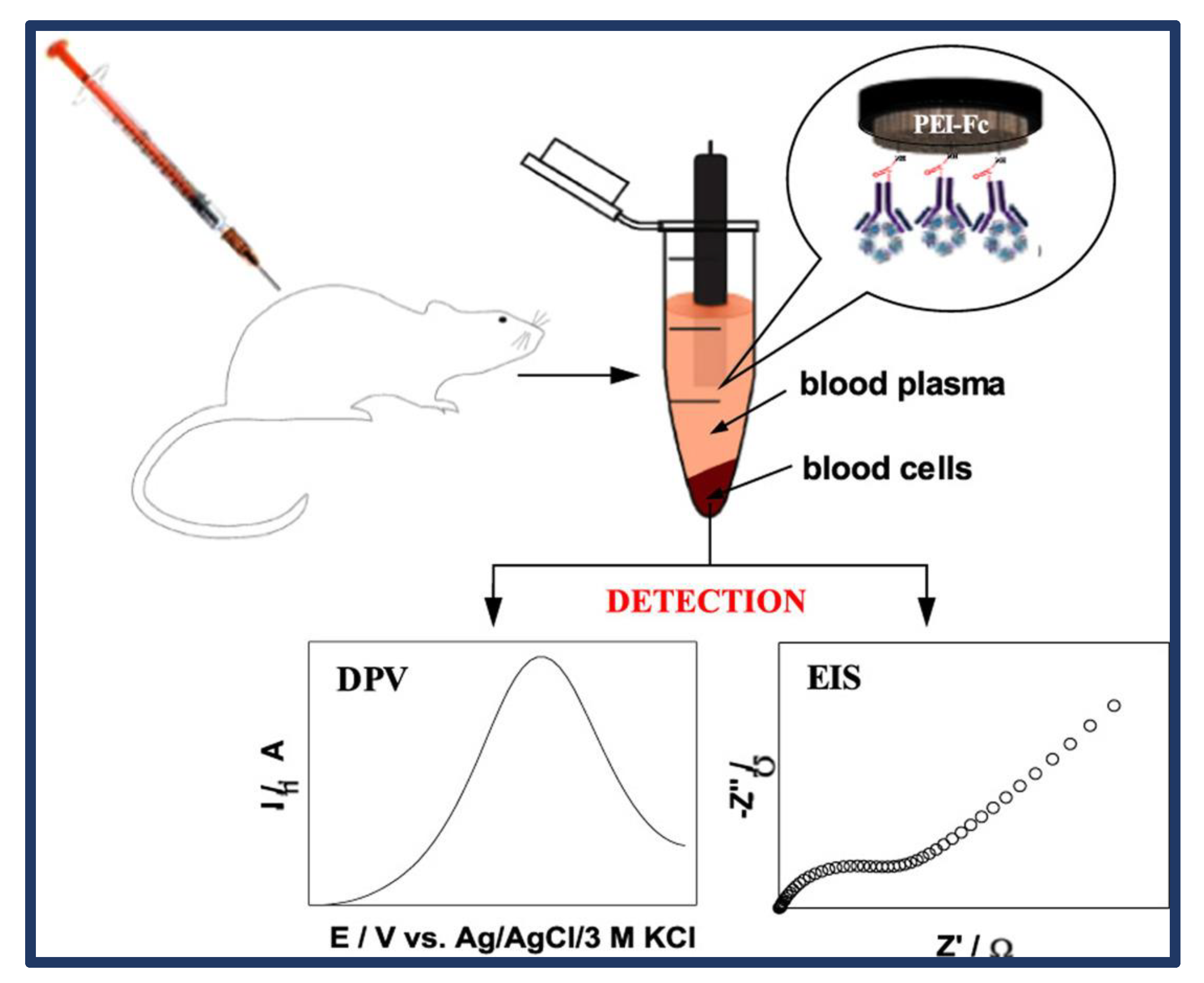
| CRP | PEI-Fc /anti-CRP/GCE | DPV EIS | 10–50,000 ng/mL | 0.5 ng/mL | 8.5 | Blood sample | NR | [53] |
| CRP | MB-NH2-SWCNT-AuNPs/SPE | CV DPV EIS | 5 pg/mL–1 μg/mL | 5 pg/mL | >13.38 | Blood sample | 80 | [54] |
| CRP | Fc-ECG/MEL/AuNPs/SPE | CV EIS DPV | 0.001–1000 μg/mL | 0.30 μg/mL | 6.59 | Human Serum | 98.69–102.43 | [55] |
| CRP | anti-CRP rGO/Ni/PtN/SPCE | Amperometry | 2–100 μg/mL | 0.80 μg/mL | 8.0 | Human Serum | NR | [56] |
| CRP | MWCNTs/AuE | EIS CV | 0.084–0.84 nM | 4\0 pM | 3.15 | Human Serum | NR | [57] |
| CRP | ERGO/PTyr/ | DPV EIS | 1.09–100 μg/L | 0.375 μg/L | NR | Human Serum | NR | [58] |
| CRP | BSA/anti-CRP/MPA/Au | CV SWV | 5–220 fg/mL | 2.25 fg/mL | 3.12 | Human Serum | NR | [59] |
| PCT | PCT-Ab-AgNp-SLG/ITO | CV EIS | 2–25 ng /mL | 0.55 ng/mL | NR | Human serum | NR | [60] |
| PCT | MoO3-Au-rGO-Ab2/GCE | CV | 0.01 pg/mL−10 ng/mL | 0.002 pg/mL | 2.30 | BSA | NR | [61] |
| PCT | g-C3N4-NiCo2S4-CNTs-AgNPs /GCE | DPV | 0.05–50 ng/mL | 16.70 pg/mL | 3–5 | Human serum | 98.40–102.74 | [62] |
| NT-proBNP | Paper Electrode | LASV SWASV | 53–590 pM | 300.0 pM | NR | Human Serum | NR | [63] |
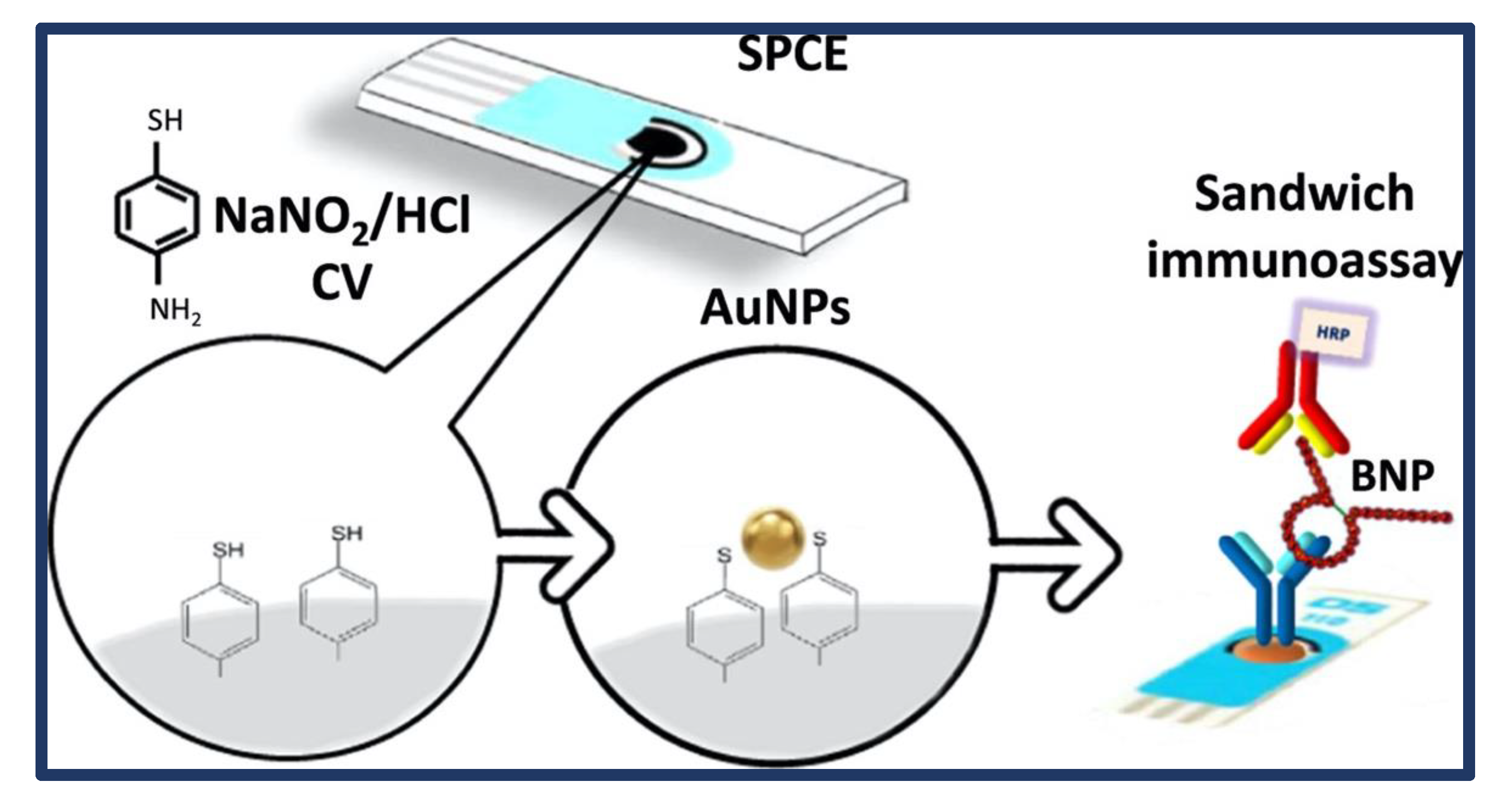
| BNP | AuNPs-S-Phe/SPCE | EIS CV | 0.014–15 ng/mL | 4 pg/Ml | 6.4 | Human Serum | NR | [64] |
| BNP | PPIX/N–ZnO NP/ITO | EIS | 1 pg/mL–0.1 μg/ mL | 0.14 pg/mL | 2.6–5.9 | Human Serum | 90.0–102 | [65] |
| BNP | ZnCo2O4/N-CNTs-Ab/GCE | Amperometry DPV CV | 0.01 pg/mL−1 ng/mL | 3.34 fg/mL | 2.9–3.5 | Human Serum | 97.0–102.1 | [66] |
| cTnI | N, Zn-GQDs/GCE | DPV | 10–106 pg/mL | 4.59 pg/L | 9.09–11.1 | Human Serum | 92–97.1 | [67] |
| cTnI | COOH-ZnONPs/GCE | EIS DPV | 0.50 pM–3.3 × 105 pM | 1.04 pM | 3.06–4.5 | Human Serum | 93.40−114.28 | [68] |
| cTnI | CSA/MCH/Fc-COFNs-MBA/Au | CV DPV | 10 fg/mL–10 ng/mL | 2.6 fg/Ml | 4.2 | Human Serum | 97.2–102.9 | [69] |
| cTnI | PCN-AuNPs/LSGE | CV SWV | 0.0001–1000 ng/mL | 0.01 pg/mL | 2.25 | Human Serum | NR | [70] |
| cTnI | pCTAB/DES/Au-SPE and pCTAB/DES/Ab2/Au-SPE | DPV CV | 0.04 ng/mL−50 ng/mL | 0.0009 ng/Ml | 0.37–1.94 | Human Serum | NR | [71] |
| cTnI | N-prGO/COOH/PEG-aptamer/GCE | DPV | 0.001–100 pg/L | 1 pg/mL | 4.3 | Human Seum | 98.2–101.7 | [72] |
| cTnI | Fc-COOH-CIL-HCNTs/GCE | DPV | 0.01–60 ng/mL | 0.006 ng/mL | 4.3–6.0 | Human serum | 96.4–103.3 | [73] |
| cTnI | Ti disc/AuNPs/Apt | DPV | 1–1100 pM | 0.18 pM | 3.28 | Human serum | 100.2–101.8 | [74] |
| cTnI | DNA 3WJ/MB/Apt | CV | 0 pM−100 nM | 1.0 pM | NR | Human serum | NR | [75] |
| cTnI | MIP/BNQDs/GCE | DPV | 0.01–5.0 ng/mL | 0.0005 ng/mL | 0.17–0.47 | Human Plasma | NR | [76] |
| cTnT | N-MIP/SPCE | DPV | 0.02–0.09 ng/mL | 0.008 ng/mL | NR | Human Serum | NR | [77] |
| cTnT | cTnT-PANI/PMB/f-MWCNTs/ SPCE | DPV CV | 0.10–8.0 pg/mL | 0.040 pg/mL | 1.3 | Human Blood Plasma | 91–112 | [78] |
| NSE | AuNPs@MoS2/rGO/GCE | SWV EIS | 0.01–1.0 pg/mL | 3.00 fg/Ml | 0.48 | Human Serum | 99.80–100.52 | [79] |
| NSE | Ab2-Au/Fc@CuxO SPs/ HCNs-GR/GCE | Amperometry | 500 fg/mL−100 ng/mL | 25.7 fg/mL | 4.6–7.6 | Human Serum | 87.8–95.4 | [80] |
| NSE | Au–MoS2/MOF/GCE | SWV CV EIS | 1.00 pg/mL−100.0 ng/mL | 0.37 pg/mL | 0.57–3.95 | Human Serum | 99–105.2 | [81] |
| NSE | Ab/AuNPs/MES | CV DPV | 1.0–750 ng/mL | 0.34 ng/mL | 3.1 | Human Serum Saliva | NR | [82] |
| GDF15 | MoS2/AuPtPd-Ab2/GCE | CV EIS | 1.5 pg/mL−1.5 μg/mL | 0.9 pg/mL | 4.5 | BSA | 94.0–110.0 | [83] |
| Ox-LDL | Mg–Fe3O4/PB/Ab/BSA MGCE | Chronoamperometry | 10−2 μg/mL −10 μg/mL | 9.80 × 10−4 μg/mL | 2.10–4.95 | BSA | NR | [84] |
| Gal-3 | Ab2/AuNPs/MB/MSN/ GCE | DPV ASV | 50 fg/mL−500 ng/mL | 2.0 fg/mL | −2.8–4.6 | Human Serum | 95.2–107 | [85] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaya, S.I.; Cetinkaya, A.; Ozcelikay, G.; Samanci, S.N.; Ozkan, S.A. Approaches and Challenges for Biosensors for Acute and Chronic Heart Failure. Biosensors 2023, 13, 282. https://doi.org/10.3390/bios13020282
Kaya SI, Cetinkaya A, Ozcelikay G, Samanci SN, Ozkan SA. Approaches and Challenges for Biosensors for Acute and Chronic Heart Failure. Biosensors. 2023; 13(2):282. https://doi.org/10.3390/bios13020282
Chicago/Turabian StyleKaya, Sariye Irem, Ahmet Cetinkaya, Goksu Ozcelikay, Seyda Nur Samanci, and Sibel A. Ozkan. 2023. "Approaches and Challenges for Biosensors for Acute and Chronic Heart Failure" Biosensors 13, no. 2: 282. https://doi.org/10.3390/bios13020282