Noncontact Cardiac Activity Detection Based on Single-Channel ISM Band FMCW Radar


Abstract
:1. Introduction
2. Measurement Method
2.1. Single Out-Channel FMCW Radar Displacement Measurement Method
2.2. Harmonic Analysis of Respiratory Signals
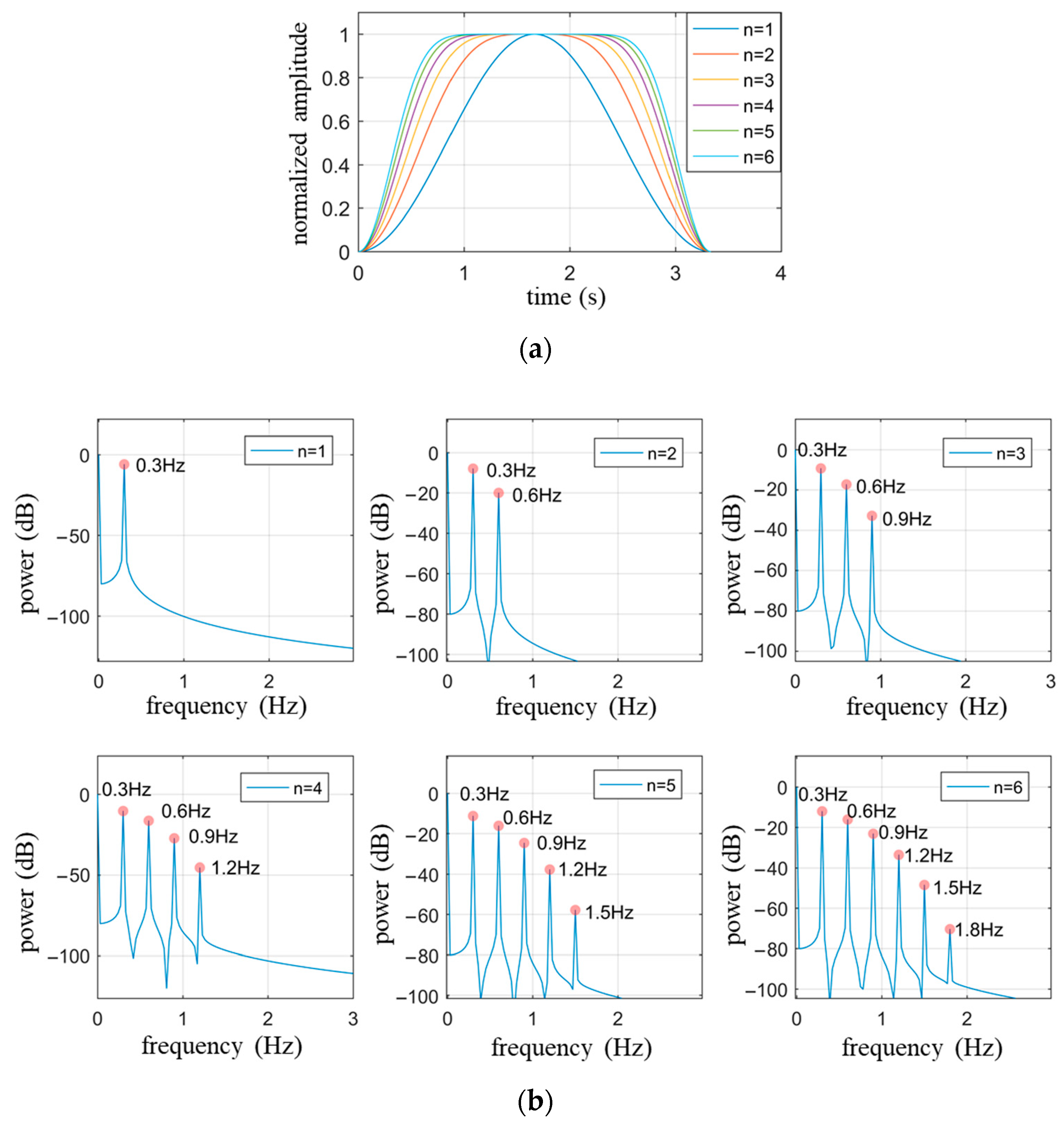
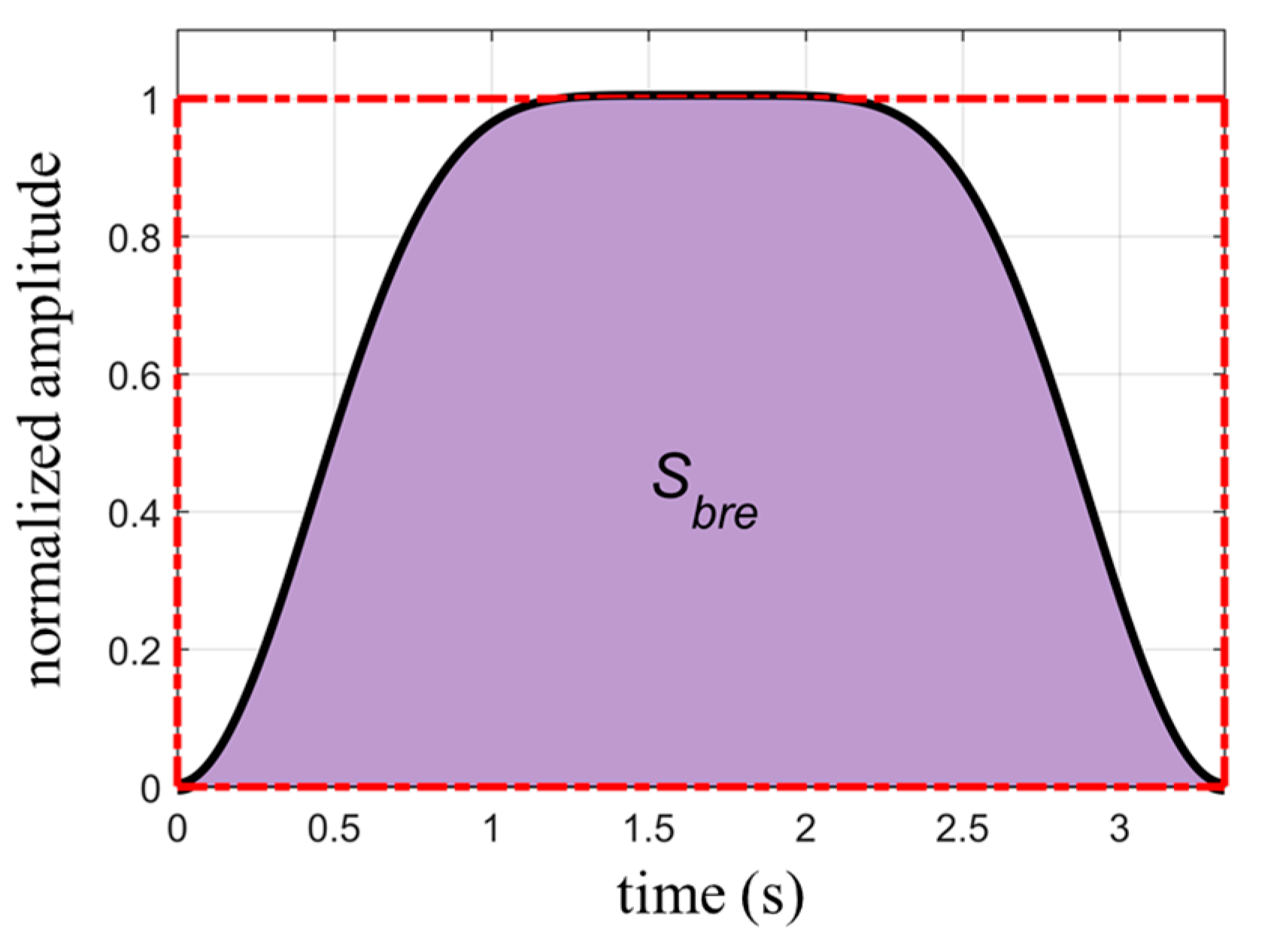
2.2.1. Empirical Formulas for Breathing Signals
2.2.2. Determination of the Number of Harmonics in Respiratory Waveforms
2.3. Estimation of Heartbeat Signals
3. Simulation
4. Experimental Measurements
4.1. Experimental Setup
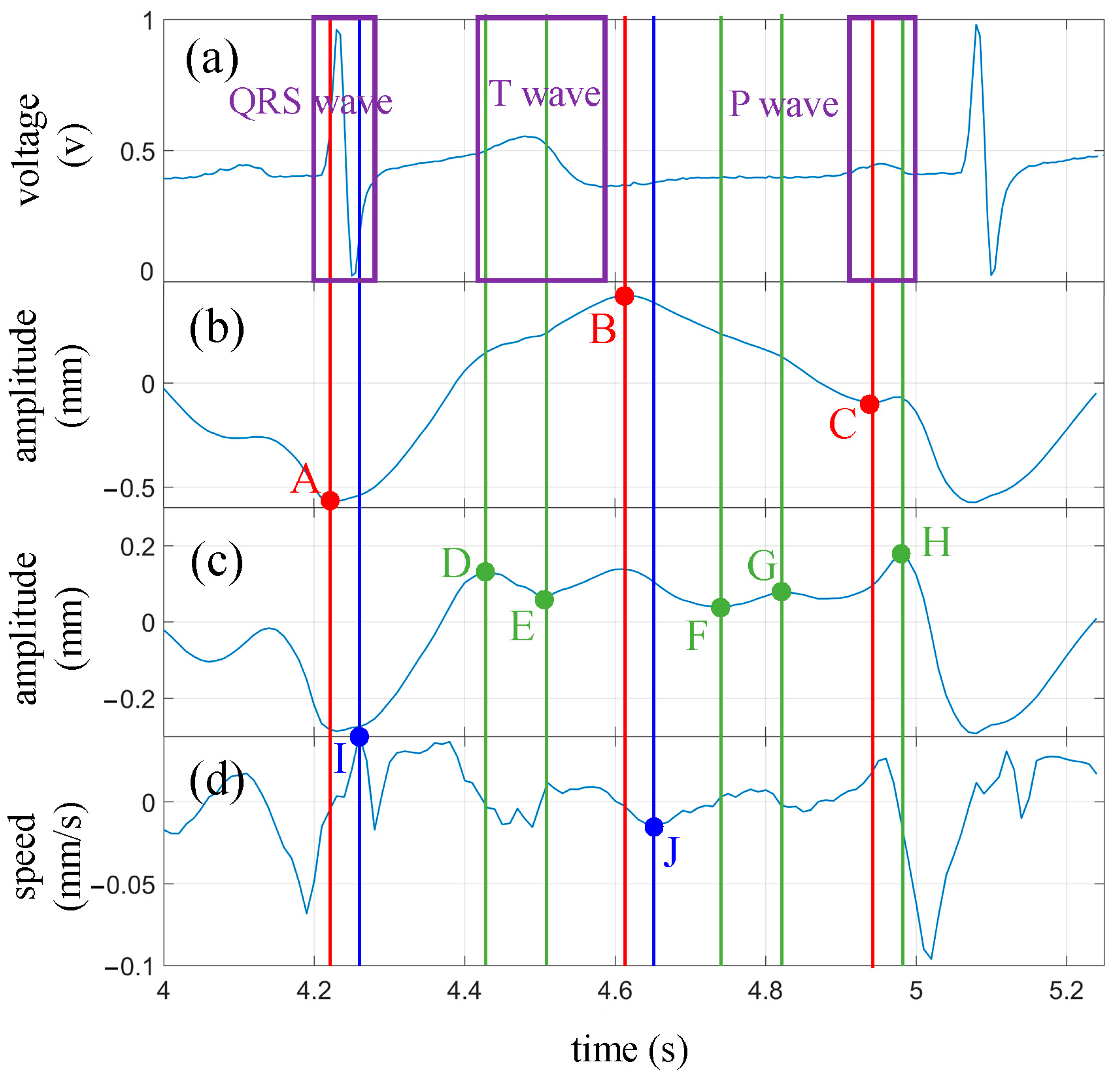
4.2. Cardiac Activity Detection
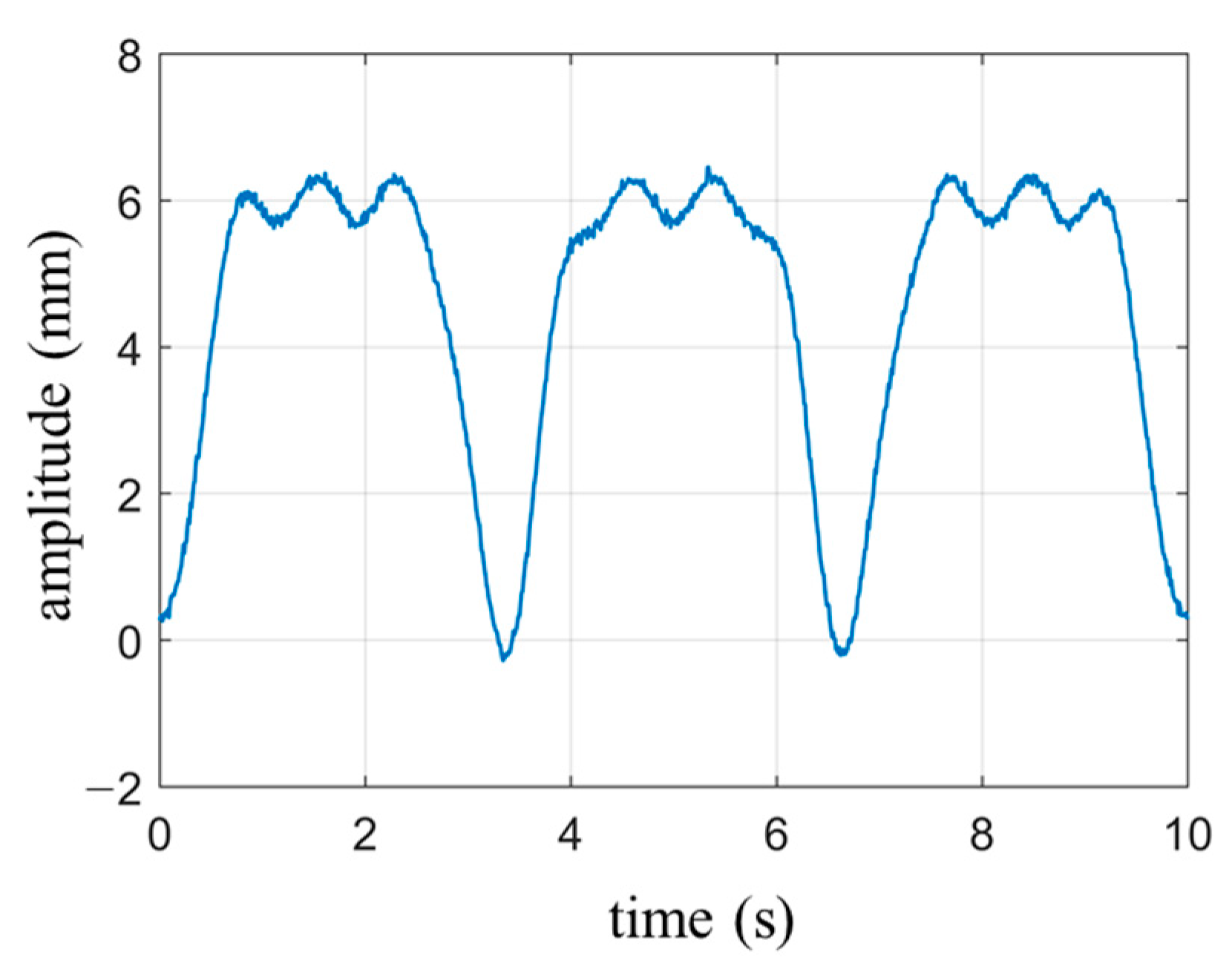
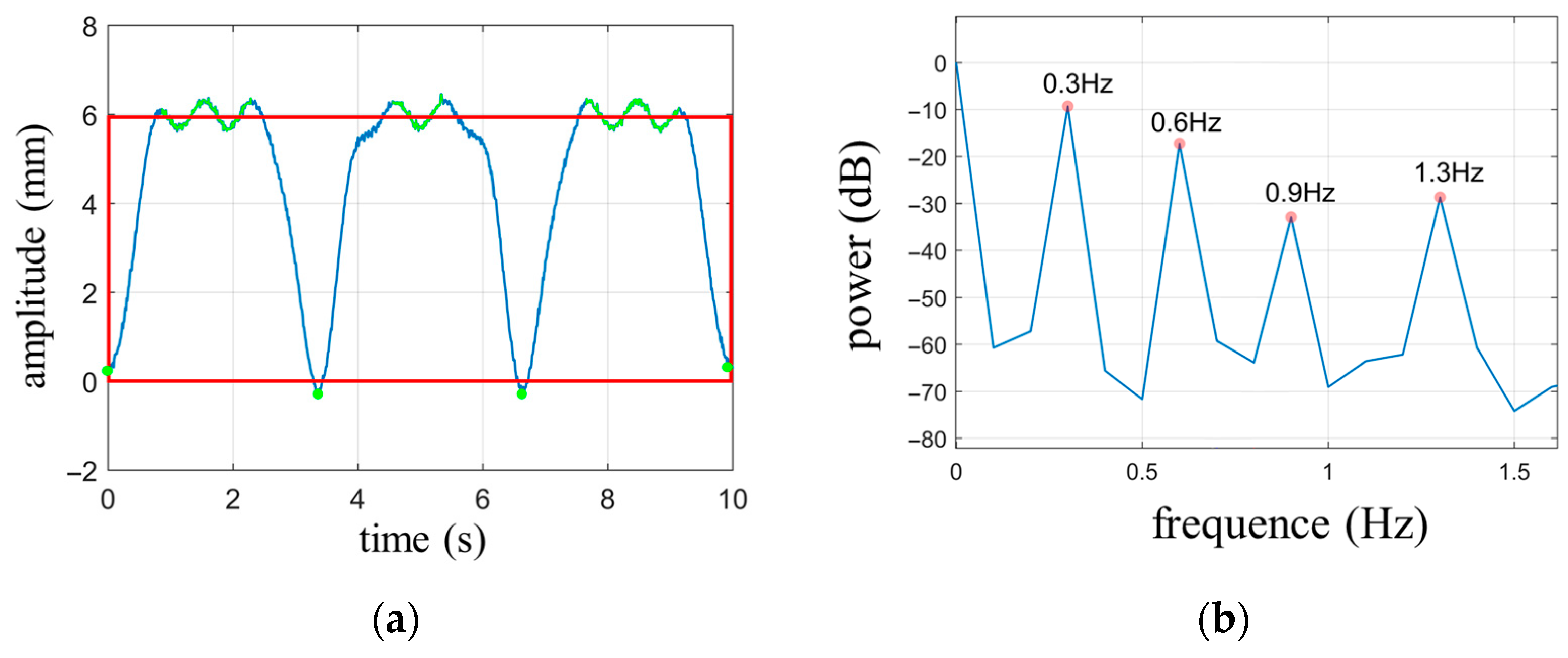
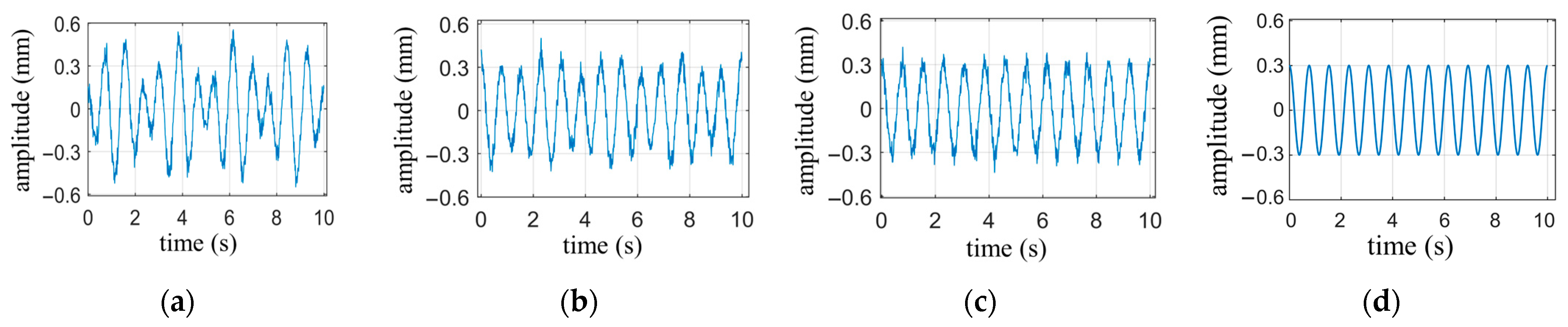
4.2.1. The Heartbeat Waveform under Breath-Holding Condition
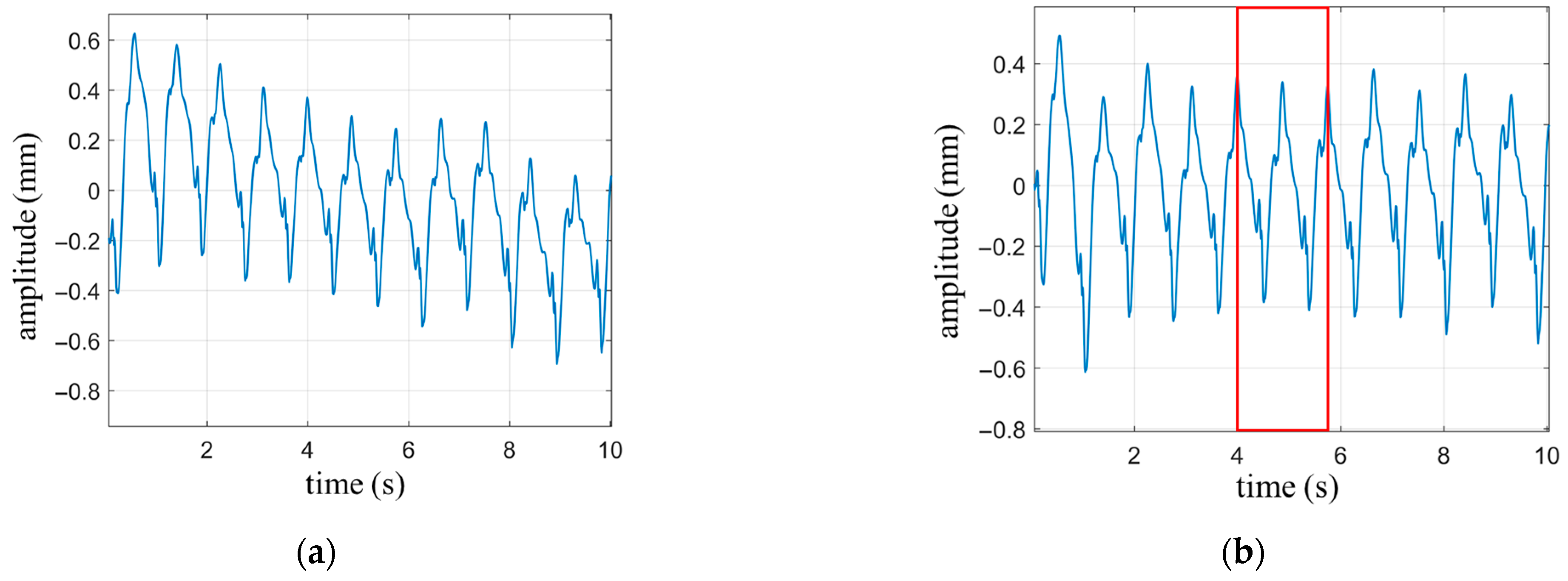
4.2.2. The Heartbeat Waveform under Normal Breathing State
4.3. Comparison of Performance with Other Works
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhang, T.; Sarrazin, J.; Valerio, G.; Istrate, D. Estimation of Human Body Vital Signs Based on 60 GHz Doppler Radar Using a Bound-Constrained Optimization Algorithm. Sensors 2018, 18, 2254. [Google Scholar] [CrossRef] [PubMed]
- Kao, T.Y.J.; Yan, Y.; Shen, T.M.; Chen, A.Y.K.; Lin, J.S. Design and Analysis of a 60-GHz CMOS Doppler Micro-Radar System-in-Package for Vital-Sign and Vibration Detection. IEEE Trans. Microw. Theory Tech. 2013, 61, 1649–1659. [Google Scholar] [CrossRef]
- Wang, S.; Pohl, A.; Jaeschke, T.; Czaplik, M.; Kony, M.; Leonhardt, S.; Pohl, N. A novel ultra-wideband 80 GHz FMCW radar system for contactless monitoring of vital signs. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 4978–4981. [Google Scholar] [CrossRef]
- Edanami, K.; Sun, G. Medical Radar Signal Dataset for Non-Contact Respiration and Heart Rate Measurement. Data Brief 2022, 40, 107724. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.C.; Lai, W.C.; Hsiao, Y.K.; Chuang, H.R. 60-GHz CMOS Doppler Radar Sensor with Integrated V-Band Power Detector for Clutter Monitoring and Automatic Clutter-Cancellation in Noncontact Vital-Signs Sensing. IEEE Trans. Microw. Theory Tech. 2018, 66, 1635–1643. [Google Scholar] [CrossRef]
- Wu, P.-H.; Chung, F.-H.; Hsu, P. A 5.8 GHz phase-and self-injection-locked CMOS radar sensor chip for vital sign detector miniaturization. In Proceedings of the 2016 IEEE MTT-S International Microwave Symposium (IMS), San Francisco, CA, USA, 22–27 May 2016; pp. 1–3. [Google Scholar]
- Ma, X.J.; Wang, Y.Y.; Lu, L.; Zhang, X.X.; Chen, Q.; You, X.H.; Lin, J.S.; Li, L.M. Design of a 100-GHz Double-Sideband Low-IF CW Doppler Radar Transceiver for Micrometer Mechanical Vibration and Vital Sign Detection. IEEE Trans. Microw. Theory Tech. 2020, 68, 2876–2890. [Google Scholar] [CrossRef]
- Su, Y.-S.; Chang, C.-C.; Guo, J.-J.; Chang, S.-F. 2-D wireless human subjects positioning system based on respiration detections. In Proceedings of the 2012 IEEE/MTT-S International Microwave Symposium Digest, Montreal, QC, Canada, 17–22 June 2012; pp. 1–3. [Google Scholar]
- Lin, J.C.; Salinger, J. Microwave measurement of respiration. In Proceedings of the 1975 IEEE-MTT-S International Microwave Symposium, Palo Alto, CA, USA, 12–14 May 1975; pp. 285–287. [Google Scholar]
- Lohman, B.; Boric-Lubecke, O.; Lubecke, V.M.; Ong, P.W.; Sondhi, M.M. A digital signal processor for Doppler radar sensing of vital signs. IEEE Eng. Med. Biol. Mag. 2002, 21, 161–164. [Google Scholar] [CrossRef]
- Park, B.-K.; Boric-Lubecke, O.; Lubecke, V.M. Arctangent demodulation with DC offset compensation in quadrature Doppler radar receiver systems. IEEE Trans. Microw. Theory Tech. 2007, 55, 1073–1079. [Google Scholar] [CrossRef]
- Tribolet, J. A new phase unwrapping algorithm. IEEE Trans. Acoust. Speech Signal Process. 1977, 25, 170–177. [Google Scholar] [CrossRef]
- Schadt, F.; Mohr, F.; Holzer, M. Application of Kalman filters as a tool for phase and frequency demodulation of IQ signals. In Proceedings of the 2008 IEEE Region 8 International Conference on Computational Technologies in Electrical and Electronics Engineering, Novosibirsk, Russia, 21–25 July 2008; pp. 421–424. [Google Scholar]
- Wang, J.Y.; Wang, X.; Chen, L.; Huangfu, J.T.; Li, C.Z.; Ran, L.X. Noncontact Distance and Amplitude-Independent Vibration Measurement Based on an Extended DACM Algorithm. IEEE Trans. Instrum. Meas. 2014, 63, 145–153. [Google Scholar] [CrossRef]
- Qu, K.; Zhang, R.; Fang, Z. High Accuracy Motion Detection Algorithm via ISM Band FMCW Radar. Remote Sens. 2022, 14, 58. [Google Scholar] [CrossRef]
- Regev, N.; Wulich, D. Remote sensing of vital signs using an ultra-wide-band radar. Int. J. Remote Sens. 2019, 40, 6596–6606. [Google Scholar] [CrossRef]
- Rahman, M.; NaghshvarianJahromi, M.; Mirjavadi, S.S.; Hamouda, A.M. Bandwidth Enhancement and Frequency Scanning Array Antenna Using Novel UWB Filter Integration Technique for OFDM UWB Radar Applications in Wireless Vital Signs Monitoring. Sensors 2018, 18, 3155. [Google Scholar] [CrossRef] [PubMed]
- Hu, W.; Zhao, Z.; Wang, Y.; Zhang, H.; Lin, F. Noncontact Accurate Measurement of Cardiopulmonary Activity Using a Compact Quadrature Doppler Radar Sensor. IEEE Trans. Biomed. Eng. 2014, 61, 725–735. [Google Scholar] [CrossRef] [PubMed]
- Shi, Q.; Hu, B.; Tian, F.; Zhao, Q. Noncontact Doppler Radar-based Heart Rate Detection on the SVD and ANC. In Proceedings of the 2022 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Las Vegas, NV, USA, 6–8 December 2022; pp. 1710–1713. [Google Scholar]
- Hu, Y.; Toda, T. Remote heart-rate estimation based on phase accumulation-linear interpolation method for mm-wave FMCW radar. IEICE Commun. Express 2021, 10, 56–61. [Google Scholar] [CrossRef]
- Xu, D.; Yu, W.; Deng, C.; He, Z.S. Non-Contact Detection of Vital Signs Based on Improved Adaptive EEMD Algorithm (July 2022). Sensors 2022, 22, 6423. [Google Scholar] [CrossRef] [PubMed]
- Dong, S.; Li, Y.; Lu, J.; Zhang, Z.; Gu, C.; Mao, J. Accurate Detection of Doppler Cardiograms with a Parameterized Respiratory Filter Technique Using a K-Band Radar Sensor. IEEE Trans. Microw. Theory Tech. 2023, 71, 71–82. [Google Scholar] [CrossRef]
- Mikhelson, I.V.; Bakhtiari, S.; Elmer, T.W., II; Sahakian, A.V. Remote Sensing of Heart Rate and Patterns of Respiration on a Stationary Subject Using 94-GHz Millimeter-Wave Interferometry. IEEE Trans. Biomed. Eng. 2011, 58, 1671–1677. [Google Scholar] [CrossRef]
- Kuutti, J.; Paukkunen, M.; Aalto, M.; Eskelinen, P.; Sepponen, R.E. Evaluation of a Doppler radar sensor system for vital signs detection and activity monitoring in a radio-frequency shielded room. Measurement 2015, 68, 135–142. [Google Scholar] [CrossRef]
- Yu, Z.; Zhao, D.; Zhang, Z. Doppler Radar Vital Signs Detection Method Based on Higher Order Cyclostationary. Sensors 2018, 18, 47. [Google Scholar] [CrossRef]
- Sakamoto, T.; Aubry, P.J.; Okumura, S.; Taki, H.; Sato, T.; Yarovoy, A.G. Noncontact Measurement of the Instantaneous Heart Rate in a Multi-Person Scenario Using X-Band Array Radar and Adaptive Array Processing. IEEE J. Emerg. Sel. Top. Circuits Syst. 2018, 8, 280–293. [Google Scholar] [CrossRef]
- Yang, Z.-K.; Shi, H.; Zhao, S.; Huang, X.-D.; Guan, Z. Fast heart rate extraction using CW Doppler radar with interpolated discrete Fourier transform algorithm. AIP Adv. 2020, 10, 075113. [Google Scholar] [CrossRef]
- Ren, W.; Qi, F.; Foroughian, F.; Kvelashvili, T.; Liu, Q.; Kilic, O.; Long, T.; Fathy, A.E. Vital Sign Detection in Any Orientation Using a Distributed Radar Network via Modified Independent Component Analysis. IEEE Trans. Microw. Theory Tech. 2021, 69, 4774–4790. [Google Scholar] [CrossRef]
- Aubert, A.E.; Welkenhuysen, L.; Montald, J.; de Wolf, L.; Geivers, H.; Minten, J.; Kesteloot, H.; Geest, H. Laser method for recording displacement of the heart and chest wall. J. Biomed. Eng. 1984, 6, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Sekine, M.; Maeno, K. Non-contact heart rate detection using periodic variation in Doppler frequency. In Proceedings of the 2011 IEEE Sensors Applications Symposium, San Antonio, TX, USA, 22–24 February 2011; pp. 318–322. [Google Scholar]
- Gao, X.M.; Aditya, S.; Ehsan, Y.; Victor, L.; Olga, B.L. Noncontact displacement estimation using Doppler radar. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012. [Google Scholar] [CrossRef]
- Morgan, D.R.; Zierdt, M.G. Novel signal processing techniques for Doppler radar cardiopulmonary sensing. Signal Process. 2009, 89, 45–66. [Google Scholar] [CrossRef]
- Varghese, J. Adaptive threshold based frequency domain filter for periodic noise reduction. Aeu-Int. J. Electron. Commun. 2016, 70, 1692–1701. [Google Scholar] [CrossRef]
- Zhang, B.; Tang, C.M. A method for defect detection of yarn-dyed fabric based on frequency domain filtering and similarity measurement. Autex Res. J. 2019, 19, 257–262. [Google Scholar] [CrossRef]
- Yan, W.Q.; He, B.; Zhao, J.; Wu, Y.C.; Du, C.H.; Xu, G.H. Frequency Domain Filtering Method for SSVEP-EEG Preprocessing. IEEE Trans. Neural Syst. Rehabil. Eng. 2023, 31, 2079–2089. [Google Scholar] [CrossRef]
- Kim, C.; Bae, J.; Han, H.; Park, S.; Kim, H. High frequency arbitrary waveform generator using a nonlinear transmission line. Microw. Opt. Technol. Lett. 2020, 62, 1204–1208. [Google Scholar] [CrossRef]
- Brunetti, G.; Armenise, M.N.; Ciminelli, C. Chip-Scaled Ka-Band Photonic Linearly Chirped Microwave Waveform Generator. Front. Phys. 2022, 10, 158. [Google Scholar] [CrossRef]
- He, Y.B.; Bahr, B.; Si, M.W.; Ye, P.D.; Weinstein, D. A tunable ferroelectric based unreleased RF resonator. Microsyst. Nanoeng. 2020, 6, 8. [Google Scholar] [CrossRef]
- Costa, J.D.; Figeys, B.; Sun, X.; Van Hoovels, N.; Tilmans, H.A.C.; Ciubotaru, F.; Adelmann, C. Compact tunable YIG-based RF resonators. Appl. Phys. Lett. 2021, 118, 162406. [Google Scholar] [CrossRef]
- Yu, Y.P.; Shang, Q.H.; An, S.H.; Zhang, Y.; Su, Y.K.; Yao, J.P. Tunable Silicon Photonic RF Phase Shifter with Low RF Power Variation Based on Constructive Interference of an Add-Drop Ring Resonator. IEEE Photonics J. 2018, 10, 1–8. [Google Scholar] [CrossRef]
- Sattin, M.; Burhani, Z.; Jaidka, A.; Millington, S.J.; Arntfield, R.T. Stroke Volume Determination by Echocardiography. Chest 2022, 161, 1598–1605. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.N.; Miyoshi, T.; Addetia, K.; Henry, M.P.; Citro, R.; Daimon, M.; Fajardo, P.G.; Kasliwal, R.R.; Kirkpatrick, J.N.; Monaghan, M.J.; et al. Normal Values of Cardiac Output and Stroke Volume According to Measurement Technique, Age, Sex, and Ethnicity: Results of the World Alliance of Societies of Echocardiography Study. J. Am. Soc. Echocardiogr. 2021, 34, 1077–1085. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.G.; Liu, D.D.; Avolio, A.P.; Chen, K.; Li, D.C.; Hu, B.; Butlin, M. Estimation of cardiac stroke volume from radial pulse waveform by artificial neural network. Comput. Methods Programs Biomed. 2022, 218, 106738. [Google Scholar] [CrossRef]
- Gagnon, D.; Romero, S.A.; Ngo, H.; Sarma, S.; Cornwell, W.K.; Poh, P.Y.S.; Stoller, D.; Levine, B.D.; Crandall, C.G. Healthy aging does not compromise the augmentation of cardiac function during heat stress. J. Appl. Physiol. 2016, 121, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.T.; Li, Y.C.; Li, C.Z.; Gu, C.Z.; Mao, J.F. Accurate Measurement of Human Vital Signs with Linear FMCW Radars Under Proximity Stationary Clutters. IEEE Trans. Biomed. Circuits Syst. 2021, 15, 1393–1404. [Google Scholar] [CrossRef]
- Zheng, P.W.; Zheng, C.D.; Li, X.X.; Chen, H.H.; Wang, A.G.; Luo, Y.H. Second Harmonic Weighted Reconstruction for Non-Contact Monitoring Heart Rate. IEEE Sens. J. 2022, 22, 5815–5823. [Google Scholar] [CrossRef]
- Yang, Z.; Bao, Z. Short-time Heart Rate Estimation Based on 60-GHz FMCW Radar. In Proceedings of the 2023 IEEE MTT-S International Wireless Symposium (IWS), Qingdao, China, 14–17 May 2023; pp. 1–3. [Google Scholar] [CrossRef]
- Dong, S.Q.; Zhang, Y.; Ma, C.; Zhu, C.K.; Gu, Z.T.; Lv, Q.Y.; Zhang, B.; Li, C.Z.; Ran, L.X. Doppler Cardiogram: A Remote Detection of Human Heart Activities. IEEE Trans. Microw. Theory Tech. 2020, 68, 1132–1141. [Google Scholar] [CrossRef]
- Zhu, C.K.; Balle, M.; Zhang, B.; Lv, Q.Y.; Li, Y.; Zhu, Z.B.; Wang, X.B.; Li, X.J.; Ran, L.X. Doppler Cardiogram Detected by a V-Band Doppler Radar Sensor. IEEE Trans. Microw. Theory Tech. 2022, 70, 521–531. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Fundamental Frequency Range (Hz) | Frequency per Minute (Hz/min) | Amplitude of Chest Wall (mm) |
|---|---|---|---|
| Respiration | 0.13~0.4 | 7.8~24 | 4~12 |
| Heartbeat | 0.83~3.3 | 49.8~198 | <0.6 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 0.5 | 0.625 | 0.688 | 0.727 | 0.754 | 0.774 | 0.791 | 0.804 | 0.815 | 0.824 |
| Ref. | Waveform | Single-Channel | ISM Band | The Detection Content of Cardiac Activity | Number of Feature Points | Type of Waveform Used |
|---|---|---|---|---|---|---|
| [26] | CW | NO | NO | Periodicity | None | HW 1 |
| [27] | CW | NO | NO | Periodicity | None | HW |
| [28] | SFCW | NO | NO | Periodicity | None | HW |
| [45] | FMCW | YES | NO | Periodicity | None | HW |
| [46] | FMCW | NO | NO | Periodicity | None | HW |
| [47] | FMCW | NO | NO | Periodicity | None | HW |
| [22] | CW | NO | YES | Periodicity and Feature Points | 3 | HW and SW 2 and AW 3 |
| [48] | CW | NO | YES | Periodicity and Feature Points | 5 | HW and SW and AW |
| [49] | CW | NO | YES | Periodicity and Feature Points | 8 | HW and SW and AW |
| This work | FMCW | YES | YES | Periodicity and Feature Points | 10 | HW and SW and HWRFW 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qu, K.; Wei, L.; Zhang, R. Noncontact Cardiac Activity Detection Based on Single-Channel ISM Band FMCW Radar. Biosensors 2023, 13, 982. https://doi.org/10.3390/bios13110982
Qu K, Wei L, Zhang R. Noncontact Cardiac Activity Detection Based on Single-Channel ISM Band FMCW Radar. Biosensors. 2023; 13(11):982. https://doi.org/10.3390/bios13110982
Chicago/Turabian StyleQu, Kui, Lei Wei, and Rongfu Zhang. 2023. "Noncontact Cardiac Activity Detection Based on Single-Channel ISM Band FMCW Radar" Biosensors 13, no. 11: 982. https://doi.org/10.3390/bios13110982