
In Vitro Evaluation of Lithium Disilicate Endocrowns and Post and Core Crowns—A Systematic Review

Abstract
:1. Introduction
2. Materials and Methods
2.1. Focused Question
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Data Extraction
2.6. Quality Assessment
3. Results
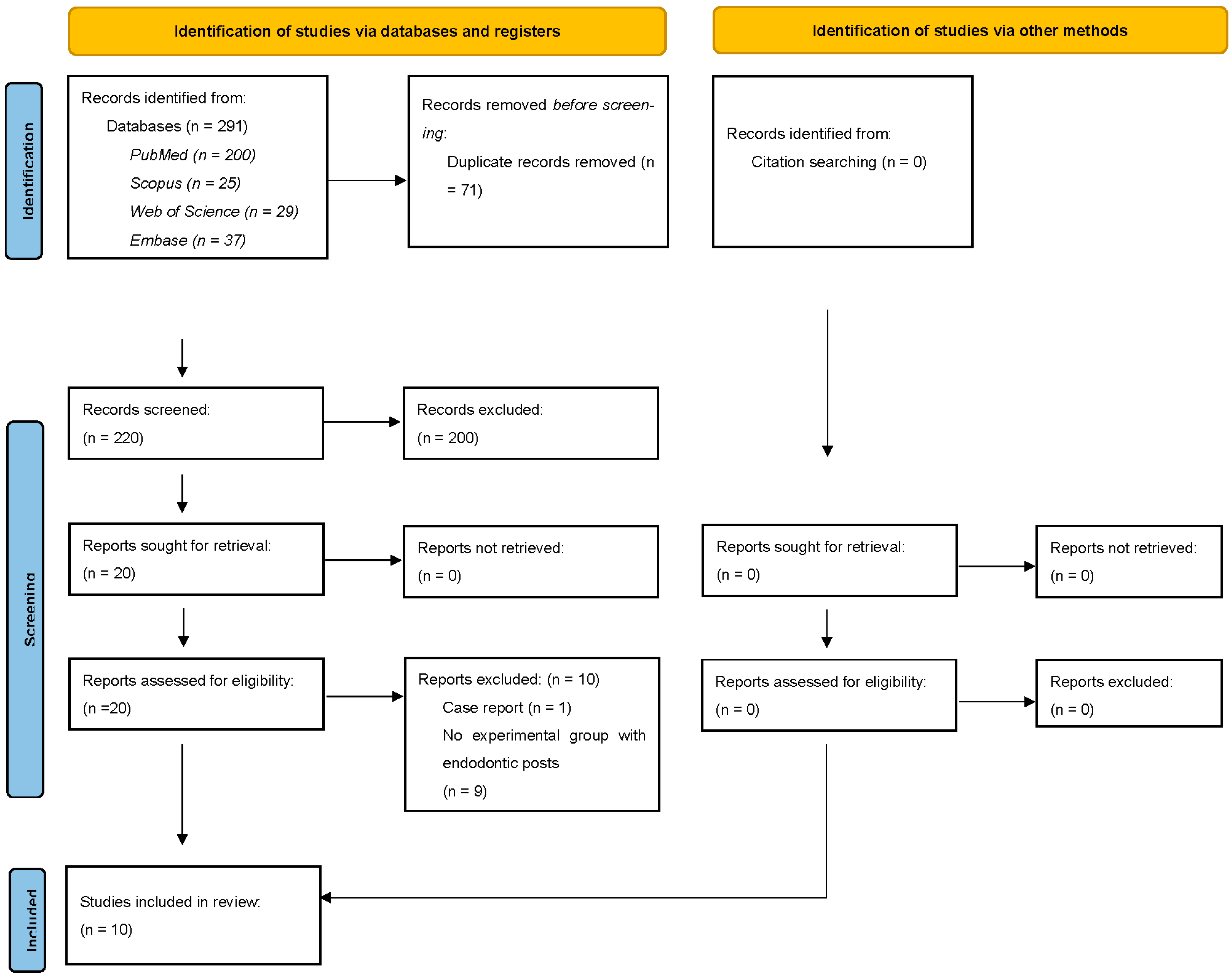
3.1. Literature Search
3.2. General Characteristics of the Studies
3.3. Fracture Strength Outcomes
3.4. Failure Patterns
3.5. Marginal Adaptation
3.6. Results of Bias Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Saeed, F.; Muhammad, N.; Khan, A.S.; Sharif, F.; Rahim, A.; Ahmad, P.; Irfan, M. Prosthodontics Dental Materials: From Conventional to Unconventional. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 106, 110167. [Google Scholar] [CrossRef] [PubMed]
- Naumann, M.; Schmitter, M.; Krastl, G. Postendodontic Restoration: Endodontic Post-and-Core or No Post At All? J. Adhes. Dent. 2018, 20, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Falcão Spina, D.R.; Goulart da Costa, R.; Farias, I.C.; da Cunha, L.G.; Ritter, A.V.; Gonzaga, C.C.; Correr, G.M. CAD/CAM Post-and-Core Using Different Esthetic Materials: Fracture Resistance and Bond Strengths. Am. J. Dent. 2017, 30, 299–304. [Google Scholar]
- Hendi, A.R.; Moharrami, M.; Siadat, H.; Hajmiragha, H.; Alikhasi, M. The Effect of Conventional, Half-Digital, and Full-Digital Fabrication Techniques on the Retention and Apical Gap of Post and Core Restorations. J. Prosthet. Dent. 2019, 121, 364-e1–364-e6. [Google Scholar] [CrossRef]
- Pang, J.; Feng, C.; Zhu, X.; Liu, B.; Deng, T.; Gao, Y.; Li, Y.; Ke, J. Fracture Behaviors of Maxillary Central Incisors with Flared Root Canals Restored with CAD/CAM Integrated Glass Fiber Post-and-Core. Dent. Mater. J. 2019, 38, 114–119. [Google Scholar] [CrossRef]
- Hsiao, L.-T.; Ho, J.-C.; Huang, C.-F.; Hung, W.-C.; Chang, C.-W. Analysis of Clinical Associated Factors of Vertical Root Fracture Cases Found in Endodontic Surgery. J. Dent. Sci. 2020, 15, 200–206. [Google Scholar] [CrossRef] [PubMed]
- Papalexopoulos, D.; Samartzi, T.-K.; Sarafianou, A. A Thorough Analysis of the Endocrown Restoration: A Literature Review. J. Contemp. Dent. Pract. 2021, 22, 422–426. [Google Scholar] [CrossRef] [PubMed]
- Gulec, L.; Ulusoy, N. Effect of Endocrown Restorations with Different CAD/CAM Materials: 3D Finite Element and Weibull Analyses. BioMed Res. Int. 2017, 2017, 5638683. [Google Scholar] [CrossRef]
- Elagra, D.M.E. Endocrown Preparation: Review. Int. J. Appl. Dent. Sci. 2019, 5, 253–256. [Google Scholar]
- Altier, M.; Erol, F.; Yildirim, G.; Dalkilic, E.E. Fracture Resistance and Failure Modes of Lithium Disilicate or Composite Endocrowns. Niger. J. Clin. Pract. 2018, 21, 821–826. [Google Scholar] [CrossRef]
- Forberger, N.; Göhring, T.N. Influence of the Type of Post and Core on in Vitro Marginal Continuity, Fracture Resistance, and Fracture Mode of Lithia Disilicate-Based All-Ceramic Crowns. J. Prosthet. Dent. 2008, 100, 264–273. [Google Scholar] [CrossRef] [PubMed]
- Pedrollo Lise, D.; Van Ende, A.; De Munck, J.; Umeda Suzuki, T.Y.; Cardoso Vieira, L.C.; Van Meerbeek, B. Biomechanical Behavior of Endodontically Treated Premolars Using Different Preparation Designs and CAD/CAM Materials. J. Dent. 2017, 59, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Altman, D.G.; Liberati, A.; Tetzlaff, J. PRISMA Statement. Epidemiology 2011, 22, 128. [Google Scholar] [CrossRef]
- Sheth, V.H.; Shah, N.P.; Jain, R.; Bhanushali, N.; Bhatnagar, V. Development and Validation of a Risk-of-Bias Tool for Assessing in Vitro Studies Conducted in Dentistry: The QUIN. J. Prosthet. Dent. 2022, 3913, 345–346. [Google Scholar] [CrossRef] [PubMed]
- Biacchi, G.R.; Mello, B.; Basting, R.T. The Endocrown: An Alternative Approach for Restoring Extensively Damaged Molars. J. Esthet. Restor. Dent. 2013, 25, 383–390. [Google Scholar] [CrossRef]
- El-Damanhoury, H.M.; Haj-Ali, R.N.; Platt, J.A. Fracture Resistance and Microleakage of Endocrowns Utilizing Three CAD-CAM Blocks. Oper. Dent. 2015, 40, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Gresnigt, M.M.M.; Özcan, M.; van den Houten, M.L.A.; Schipper, L.; Cune, M.S. Fracture Strength, Failure Type and Weibull Characteristics of Lithium Disilicate and Multiphase Resin Composite Endocrowns under Axial and Lateral Forces. Dent. Mater. 2016, 32, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Belleflamme, M.M.; Geerts, S.O.; Louwette, M.M.; Grenade, C.F.; Vanheusden, A.J.; Mainjot, A.K. No Post-No Core Approach to Restore Severely Damaged Posterior Teeth: An up to 10-Year Retrospective Study of Documented Endocrown Cases. J. Dent. 2017, 63, 1–7. [Google Scholar] [CrossRef]
- Hayes, A.; Duvall, N.; Wajdowicz, M.; Roberts, H. Effect of Endocrown Pulp Chamber Extension Depth on Molar Fracture Resistance. Oper. Dent. 2017, 42, 327–334. [Google Scholar] [CrossRef]
- Dartora, G.; Rocha Pereira, G.K.; Varella de Carvalho, R.; Zucuni, C.P.; Valandro, L.F.; Cesar, P.F.; Caldas, R.A.; Bacchi, A. Comparison of Endocrowns Made of Lithium Disilicate Glass-Ceramic or Polymer-Infiltrated Ceramic Networks and Direct Composite Resin Restorations: Fatigue Performance and Stress Distribution. J. Mech. Behav. Biomed. Mater. 2019, 100, 103401. [Google Scholar] [CrossRef]
- El Makawi, Y.; Khattab, N. In Vitro Comparative Analysis of Fracture Resistance of Lithium Disilicate Endocrown and Prefabricated Zirconium Crown in Pulpotomized Primary Molars. Open Access Maced. J. Med. Sci. 2019, 7, 4094–4100. [Google Scholar] [CrossRef]
- Elashmawy, Y.; Aboushelib, M.; Elshahawy, W. Retention of Different CAD/CAM Endocrowns Bonded to Severely Damaged Endodontically Treated Teeth: An in Vitro Study. J. Indian Prosthodont. Soc. 2021, 21, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Frankenberger, R.; Winter, J.; Dudek, M.-C.; Naumann, M.; Amend, S.; Braun, A.; Krämer, N.; Roggendorf, M.J. Post-Fatigue Fracture and Marginal Behavior of Endodontically Treated Teeth: Partial Crown vs. Full Crown vs. Endocrown vs. Fiber-Reinforced Resin Composite. Materials 2021, 14, 7733. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Wang, Z.; Li, X.; Sun, C.; Gao, E.; Li, H. A Comparison of the Fracture Resistances of Endodontically Treated Mandibular Premolars Restored with Endocrowns and Glass Fiber Post-Core Retained Conventional Crowns. J. Adv. Prosthodont. 2016, 8, 489–493. [Google Scholar] [CrossRef] [PubMed]
- Rocca, G.T.; Daher, R.; Saratti, C.M.; Sedlacek, R.; Suchy, T.; Feilzer, A.J.; Krejci, I. Restoration of Severely Damaged Endodontically Treated Premolars: The Influence of the Endo-Core Length on Marginal Integrity and Fatigue Resistance of Lithium Disilicate CAD-CAM Ceramic Endocrowns. J. Dent. 2018, 68, 41–50. [Google Scholar] [CrossRef] [PubMed]
- El Ghoul, W.; Özcan, M.; Silwadi, M.; Salameh, Z. Fracture Resistance and Failure Modes of Endocrowns Manufactured with Different CAD/CAM Materials under Axial and Lateral Loading. J. Esthet. Restor. Dent. 2019, 31, 378–387. [Google Scholar] [CrossRef]
- de Kuijper, M.; Gresnigt, M.; van den Houten, M.; Haumahu, D.; Schepke, U.; Cune, M.S. Fracture Strength of Various Types of Large Direct Composite and Indirect Glass Ceramic Restorations. Oper. Dent. 2019, 44, 433–442. [Google Scholar] [CrossRef]
- Rayyan, M.R.; Alauti, R.Y.; Abanmy, M.A.; AlReshaid, R.M.; Bin Ahmad, H.A. Endocrowns versus Post-Core Retained Crowns for Restoration of Compromised Mandibular Molars: An in Vitro Study. Int. J. Comput. Dent. 2019, 22, 39–44. [Google Scholar]
- Sedrez-Porto, J.A.; Münchow, E.A.; Cenci, M.S.; Pereira-Cenci, T. Which Materials Would Account for a Better Mechanical Behavior for Direct Endocrown Restorations? J. Mech. Behav. Biomed. Mater. 2020, 103, 103592. [Google Scholar] [CrossRef]
- Hassouneh, L.; Jum’ah, A.A.; Ferrari, M.; Wood, D.J. Post-Fatigue Fracture Resistance of Premolar Teeth Restored with Endocrowns: An in Vitro Investigation. J. Dent. 2020, 100, 103426. [Google Scholar] [CrossRef]
- Ahmed, M.A.A.; Kern, M.; Mourshed, B.; Wille, S.; Chaar, M.S. Fracture Resistance of Maxillary Premolars Restored with Different Endocrown Designs and Materials after Artificial Ageing. J. Prosthodont. Res. 2022, 66, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Mavriqi, L.; Valente, F.; Murmura, G.; Sinjari, B.; Macrì, M.; Trubiani, O.; Caputi, S.; Traini, T. Lithium Disilicate and Zirconia Reinforced Lithium Silicate Glass-Ceramics for CAD/CAM Dental Restorations: Biocompatibility, Mechanical and Microstructural Properties after Crystallization. J. Dent. 2022, 119, 104054. [Google Scholar] [CrossRef] [PubMed]
- Elshahawy, W.; Ajlouni, R.; James, W.; Abdellatif, H.; Watanabe, I. Elemental Ion Release from Fixed Restorative Materials into Patient Saliva. J. Oral. Rehabil. 2013, 40, 381–388. [Google Scholar] [CrossRef]
- Kourtis, S.; Damanaki, M.; Kaitatzidou, S.; Kaitatzidou, A.; Roussou, V. Loosening of the Fixing Screw in Single Implant Crowns: Predisposing Factors, Prevention and Treatment Options. J. Esthet. Restor. Dent. 2017, 29, 233–246. [Google Scholar] [CrossRef] [PubMed]
- Glossary of Prosthodontic Terms. J. Prosthet. Dent. 2005, 94, 10–92. [CrossRef] [PubMed]
- Jacobs, M.S.; Windeler, A.S. An investigation of dental luting cement solubility as a function of the marginal gap. J. Prosthet. Dent. 1991, 65, 436–442. [Google Scholar] [CrossRef]
- Knoernschild, K.L.; Campbell, S.D. Periodontal tissue responses after insertion of artificial crowns and fixed partial dentures. J. Prosthet. Dent. 2000, 84, 492–498. [Google Scholar] [CrossRef]
- Sailer, I.; Fehér, A.; Filser, F.; Gauckler, L.J.; Lüthy, H.; Hämmerle, C.H. Five-year clinical results of zirconia frameworks for posterior fixed partial dentures. Int. J. Prosthodont. 2007, 20, 383–388. [Google Scholar]
- Taha, D.; Spintzyk, S.; Sabet, A.; Wahsh, M.; Salah, T. Assessment of marginal adaptation and fracture resistance of endocrown restorations utilizing different machinable blocks subjected to thermomechanical aging. J. Esthet. Restor. Dent. 2018, 30, 319–328. [Google Scholar] [CrossRef]
- Govare, N.; Contrepois, M. Endocrowns: A Systematic Review. J. Prosthet. Dent. 2020, 123, 411–418. [Google Scholar] [CrossRef]
- Rathke, A.; Frehse, H.; Hrusa, B. Vertical Root Fracture Resistance and Crack Formation of Root Canal-Treated Teeth Restored with Different Post-Luting Systems. Odontology 2022, 110, 719–725. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, H.; Cong, Q.; Zhang, Z.; Du, A.; Wang, Y. Correction: Effect of proximal box elevation on fracture resistance and microleakage of premolars restored with ceramic endocrowns. PLoS ONE 2021, 16, e0258038. [Google Scholar] [CrossRef] [PubMed]
- Cacciafesta, V.; Sfondrini, M.F.; Lena, A.; Scribante, A.; Vallittu, P.K.; Lassila, L.V. Flexural strengths of fiber-reinforced composites polymerized with conventional light-curing and additional postcuring. Am. J. Orthod. Dentofacial. Orthop. 2007, 132, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, T.; Nourizadeh, A.; Shafiei, E.; Mahboub, F.; Kalantari, A.R. Compressive Strength of Temporary Crowns Made from Default design in Two Types of Software. J. Dent. 2023, 24, 47–52. [Google Scholar]


{kind=link}
| Domain | Keywords |
|---|---|
| posterior teeth | (Bicuspids) OR (Premolar) OR (Premolars) OR (Molars, Third) OR (Third Molar *) OR (Tooth, Wisdom) OR (Wisdom Tooth) OR (Teeth, Wisdom) OR (Wisdom Teeth) OR (posterior tooth) OR (teeth, posterior) OR (molar *, first) OR (molar *, second) |
| Lithium disilicate | (lithia disilicate) OR (lithium Disilicate) |
| endocrowns | (endocrown *) |
| post and core | (Post-Core Technic *) OR (Technic *, Post-Core) OR (Post and Core Technic *) OR (Post Technique *) OR (Technique *, Post) OR (Post Technic *) OR (Technic *, Post) OR (Dental Dowel *) OR (Dowel *, Dental) |
| physical properties | (Propert *, Surface) OR (Surface Propert *) OR (mechanical, properties) OR (Mechanical Phenomenon) OR (Phenomena, Mechanical) OR (Mechanical Concepts) OR (Concept, Mechanical) OR (Processes, Mechanical) OR (Mechanical Process) OR (Flexural Strength *) OR (Resistance *, Flexural) OR (Bend Strengths) OR (Propert *, Flexural) OR (Strength *, Fracture) |
| Domain | Keywords |
| posterior teeth | dens molaris’ OR ‘dentes molares’ OR ‘molar’ OR ‘tooth, molar’ OR ‘molar tooth’ OR ‘bicuspid’ OR ‘bicuspids’ OR ‘dens premolaris’ OR ‘dentes premolares’ OR ‘pre-molar’ OR ‘pre-molars’ OR ‘premolar’ OR ‘premolar teeth’ OR ‘premolars’ OR ‘tooth, premolar’ OR ‘premolar tooth’ |
| Lithium disilicate | lithia disilicate’ OR ‘lithium Disilicate’ |
| endocrowns | ceramic dental crown’ OR ‘ceramic tooth crown’ OR ‘clinical tooth crown’ OR ‘corona clinica’ OR ‘corona dentis’ OR ‘crown’ OR ‘crown work, pulp’ OR ‘crown, dental’ OR ‘crown, tooth’ OR ‘crowns’ OR ‘crownwork, pulp’ OR ‘dental crown’ OR ‘dental crown, ceramic’ OR ‘dental crown, metal’ OR ‘dental crown, metal/polymer’ OR ‘dental crowns’ OR ‘dental prosthetic crown’ OR ‘permanent preformed dental crown’ OR ‘post and core technique’ OR ‘preformed dental crown, permanent’ OR ‘pulp crown work’ OR ‘pulp crownwork’ OR ‘tooth crown margin’ OR ‘tooth pulp crownwork’ OR ‘tooth crown’ |
| post and core | Post and Core’ OR ‘Dental Dowel *’ OR ‘Dowel *, Dental’ |
| physical properties | tiredness’ OR ‘fatigue’ OR ‘bone fracture, stress’ OR ‘fatigue fracture’ OR ‘fracture, fatigue’ OR ‘fractures, stress’ OR ‘stress bone fracture’ OR ‘stress fractures’ OR ‘stress fracture’ OR |
| Author/Year of Publication | Type(s) of Teeth Restored/Population Details (n) | Groups/Materials Used (n) | Tooth Preparation/Post Details | Fracture Resistance | Margin Outcomes | Failure Patterns/Modes | Outcomes |
|---|---|---|---|---|---|---|---|
| Forberger & Gohring, 2008 [11] | Mandibular premolars (n = 48) | No treatment Composite only (n = 8) EC (LDS) (n = 8) LDS crown + Variolink GFP (n = 8) RC + Variolink Zirconia (n = 8) Zr crown + variolink cement Gold post + crown (n = 8) Gold crown + Ketac Cem | Shoulder: 0.8 mm Axial dentine: 2 mm Posts: GFP: 15 mm; Gold: 15 mm; Zr: 10 mm; | No treatment: 849 ± 94.0 N (control) Composite only: 1031.9 ± 266.7 N Endocrown: 1107.3 ± 217.1 N GFP: 1092 ± 307.8 N Zirconia: 1253.7 ± 226.5 N Gold: 1101.2 ± 182.9 N | Marginal continuity EC: 74% GFP: 94.8% | 50% of samples had root fractures, irrespective of groups | No significant difference between fracture strengths of endocrowns vs. post-and-core. |
| Guo et al. 2016 [24] | Mandibular premolars (n = 30) | No treatment (n = 10) EC (LDS) (n = 10) GFP + LDS crown (n = 10) | EC: Depth 5 mm, shoulder 2 mm GFP: Core height 3 mm, ferrule 1.5 mm | No treatment: 997.1 ± 166.3 N EC: 479.1 ± 180.6 N GFP + LDS crown: 510 ± 191 N | NA | Intact teeth had more favourable fractures EC and GFP had more root fractures | Fracture resistance of EC (LDS) and GFP + LDS crowns was lower than that of unprepared teeth (p < 0.05). No difference between GFP + LDS and EC (LDS) (p > 0.5) |
| Lise et al. 2017 [12] | Premolars (n = 48) | EC (LDS/RC)–2.5 mm depth (n = 16) EC (LDS/RC))–5.0 mm depth (n = 16) GFP + LDS/RC Crown (n = 16) Each group restored with LDS or indirect RC (subgroup) (n = 8) All groups subjected to chewing cycles (1,200,000). | EC (2.5 mm): 2.5 mm deep, 1 mm wide margin EC (5.0 mm): 5.0 mm deep, 1 mm wide margin GFP: Post with 1.6 mm diameter and 10 mm length | No numerical values provided. | NA | Predominantly root fractures in all experimental groups | 100% survival rate of all specimens after 1,200,000 chewing cycles EC (RC) with 2.5 mm depth had highest fracture/load-to-failure resistance (p < 0.05). No difference between GFP and 5.0 mm deep ECs. |
| Rocca et al. 2017 [25] | Premolars (n = 48) | Overlays (n = 12) EC + (LDS) (2 mm depth) (n = 12) EC (LDS) (4 mm depth) (n = 12) GFP + LDS crown (n = 12) All specimens subjected to thermocycling | EC (2 mm depth): 2 mm depth EC (4 mm depth): 4 mm depth GFP: 5 mm length, core 3.5 mm depth | No numerical values provided. | No difference between margin outcomes of ECs and post-retained crowns. ECs and post-retained higher than overlays. | NA | No difference between 2 mm-deep ECs, 4 mm-deep ECs and post-and-core (p > 0.05) Groups 1–3 performed better than overlay controls. |
| Ghoul et al. 2019 [26] | Mandibular molars (n = 80) | GFP + LDS crown (n = 20) EC (LDS) (n = 20) EC (Zr-LDS) (n = 20) EC (Resin nanoceramic) (n = 20) Each group subjected to axial and lateral loading, n = 10. | 1 mm chamfer, 2 mm ferrule, 2 mm occlusal reduction EC depth: 4 mm | GFP: 1347 ± 185 N (axial), 788 ± 92 N (lateral) EC (LDS): 2914 ± 205 N (axial), 1516 ± 205 N EC (Zr LDS): 2279 ± 290 N (axial), 1074 ± 153 N (lateral) EC (Resin nanoceramic): 2752 ± 242 N (axial), 1210 ± 92 N (lateral) | NA | More irreparable (below CEJ) fractures in ECs. | Resin nanoceramic, LDS and Zr-LDS had significant higher fracture strength than post-and-core (p < 0.05). LDS had higher axial fracture strength than Zr-LDS and similar to resin. LDS crowns had the highest lateral fracture strength. |
| de Kuijper et al. 2019 [27] | Molars (n = 105) | Endo access cavity only (control) (n = 15) GFC crown (n = 15) Direct Microhybrid RC crown (n = 15) Direct Microhybrid RC crown + GFP (n = 15) RC buildup + LDS crown (n = 15) LDS/RC core + GFP (n = 15) EC (LDS) (n = 15) | 1 mm chamfer, 2 m ferrule, occlusal reduction 1.5 mm 5 mm apical GP left intact for post No endocrown depth provided | Control: 1890 ± 774 N GFC: 1823 ± 911 N RC crown: 2192 ± 752 N RC crown + GFP: 1830 ± 590 N LDS: 3217 ± 1052 N LDS + GFP: 2697 ± 993 N EC (LDS): 2425 ± 993 N | NA | Glass-fiber reinforcing resulted in more repairable fractures. | LDS with no post had the highest fracture strength (p < 0.05), followed by LDS + GFP and EC. |
| Rayyan et al. 2019 [28] | Premolars (n = 27) | EC (LDS) (n = 9) LDS/RC core + GFP (no (ferrule) (n = 9) LDS/RC core + GFP (ferrule) (n = 9) All groups subjected to thermocycling and oblique compressive loading. | EC: 3 mm depth Post: 5 mm of apical GP left intact for post | EC: 594 ± 5.8 N LDS/RC no ferrule: 458.57 ± 5.26 N LDS/RC (ferrule): 491.13 ± 6.93 N | NA | Root fractures observed predominant in all groups. | Endocrowns had highest oblique fracture strength compared to other groups (p < 0.05) |
| Sedrez-Porto et al. 2019 [29] | Molars (n = 63) | Endocrowns LDS Filtek 350 XT RC Filtek 2350 XT RC + Multipurpose adhesive 2350 XT + Universal adhesive Bulkfill (Filtek) Post-retained Filtek 2350 (incremental) Filtek 2350 (bulk-fill) | EC: 2 mm distal root depth, 1 mm depth for other roots | Sound tooth: 2149.9 ± 13.8 N LDS: 1748.5 ± 559.3 N Filtek 2530: 2292.3 ± 716.8 N Filtek + Multipurpose adhesive: 2546.3 ± 216.8 N Filtek 2350 + Universal adhesive: 2583.7 ± 612.2 N Bulkfill: 3363.1 ± 123.9 N Post-retained Filtek 2350: 2451.6 ± 484.5 N Filtek 2350 + Multipurpose adhesive: 2774 ± 578.8 N Bulkfill: 2861.2 ± 424.1 N | NA | Irreprable fractures: Natural teeth: 14% EC repairable fractures: 21% Post-retained: 57–81% | The bulk-filled endocrowns exhibited highest fracture strength compared to all other groups (p 0.05). |
| Hassouneh et al. 2020 [30] | Premolars (n = 70) | EC (n = 30) RC (n = 10) LDS (n = 10) Zr (n = 10) Post-retained (n = 30) RC (n = 10) LDS (n = 10) Zr (n = 10) No treatment (n = 10) | EC retention depth: 4 mm Post length: 3 mm projection in the post-build up, 3–5 mm of GP left intact | EC RC: 758.1 ± 105.2 N LDS: 547.4 ± 141.5 N Zr: 460 ± 112 N Post-retained RC: 477 ± 134.4 N LDS: 534.1 ± 119.1 N Zr: 815.6 ± 87.6 N No treatment: 947.4 ± 223 N | NA | Zr crowns had higher % of catastrophic fractures | Post-retained Zr crowns and resin composite ECs exhibited higher fracture strength compared to other materials (p < 0.001). Zr crowns had the highest unrepairable fractures (p < 0.05). |
| Ahmed et al. 2022 [31] | Premolars (n = 56) | EC (LDS/Zr) Flat occlusal table (no ferrule) (n = 16) EC + 1.5 mm circumferential ferrule (n = 16) EC + 1.5 mm buccal ferrule (n = 16) Post-retained: LDS/Zr crowns + Zr post (n = 16) | Ferrule: 1.5 mm (buccal and circumferential) EC retention depth: 2 mm | LDS 661 ± 143 N (buccal ferrule), 870 ± 167 N (no ferrule), 1225 ± 172 N (circumferential ferrule) Zr 1165 ± 172 N (circumferential ferrule), 1391 ± 309 N (no ferrule), 857 ± 136 N (buccal ferrule) Post and core 1440 ± 316 N (LDS and LDS) | NA | Only two post-and-core crown specimens (25%) with a favourable failure mode. | Post-retained crowns, Zr/LDS ECs with 1.5 circumferential ferrule and Zr with flat occlusal table had higher fracture strengths than other groups (p < 0.05), with no difference between them (p > 0.05). |
| Study | Aims & Objectives | Sample Size | Comparison Group | Methodology | Sampling Technique | Operator Details | Randomization | Outcomes Measurement | Outcomes Assessor Details | Blinding | Statistical Analysis | Results | Overall Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Forberger & Gohring, 2008 [11] | Yes | No | Yes | Yes | No | No | No | Yes | No | Yes | Yes | Yes | High |
| Guo et al. 2016 [24] | Yes | No | Yes | Yes | No | No | Yes | Yes | No | No | Yes | Yes | High |
| Lise et al. 2017 [12] | Yes | No | Yes | Yes | No | No | Yes | Yes | No | No | Yes | Yes | High |
| Rocca et al. 2017 [25] | Yes | No | Yes | Yes | No | No | Yes | Yes | No | No | Yes | Yes | High |
| Ghoul et al. 2019 [26] | Yes | No | Yes | Yes | No | No | No | Yes | No | No | Yes | Yes | Medium |
| de Kuijper et al. 2019 [27] | Yes | No | Yes | Yes | No | No | Yes | Yes | No | No | Yes | Yes | High |
| Rayyan et al. 2019 [28] | Yes | No | Yes | Yes | No | No | Yes | Yes | No | No | Yes | Yes | High |
| Sedrez-Porto et al. 2019 [29] | Yes | No | Yes | Yes | No | No | Yes | Yes | No | No | Yes | Yes | High |
| Hassouneh et al. 2020 [30] | Yes | No | Yes | Yes | No | No | Yes | Yes | No | No | Yes | Yes | High |
| Ahmed et al. 2022 [31] | Yes | No | Yes | Yes | No | No | Yes | Yes | No | No | Yes | Yes | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qamar, Z.; Alghamdi, A.M.S.; Haydarah, N.K.B.; Balateef, A.A.; Alamoudi, A.A.; Abumismar, M.A.; Mathur, A.; Minervini, G. In Vitro Evaluation of Lithium Disilicate Endocrowns and Post and Core Crowns—A Systematic Review. J. Funct. Biomater. 2023, 14, 276. https://doi.org/10.3390/jfb14050276
Qamar Z, Alghamdi AMS, Haydarah NKB, Balateef AA, Alamoudi AA, Abumismar MA, Mathur A, Minervini G. In Vitro Evaluation of Lithium Disilicate Endocrowns and Post and Core Crowns—A Systematic Review. Journal of Functional Biomaterials. 2023; 14(5):276. https://doi.org/10.3390/jfb14050276
Chicago/Turabian StyleQamar, Zeeshan, Ahmed Mohammed Saad Alghamdi, Naji Khaled Bin Haydarah, Abdulateef Ahmed Balateef, Ahmed Aydhah Alamoudi, Munther Amer Abumismar, Ankita Mathur, and Giuseppe Minervini. 2023. "In Vitro Evaluation of Lithium Disilicate Endocrowns and Post and Core Crowns—A Systematic Review" Journal of Functional Biomaterials 14, no. 5: 276. https://doi.org/10.3390/jfb14050276