
Cone-Beam Computed Tomography and Histological Findings for Socket Preservation Techniques Using Different Grafting Materials: A Systematic Review
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
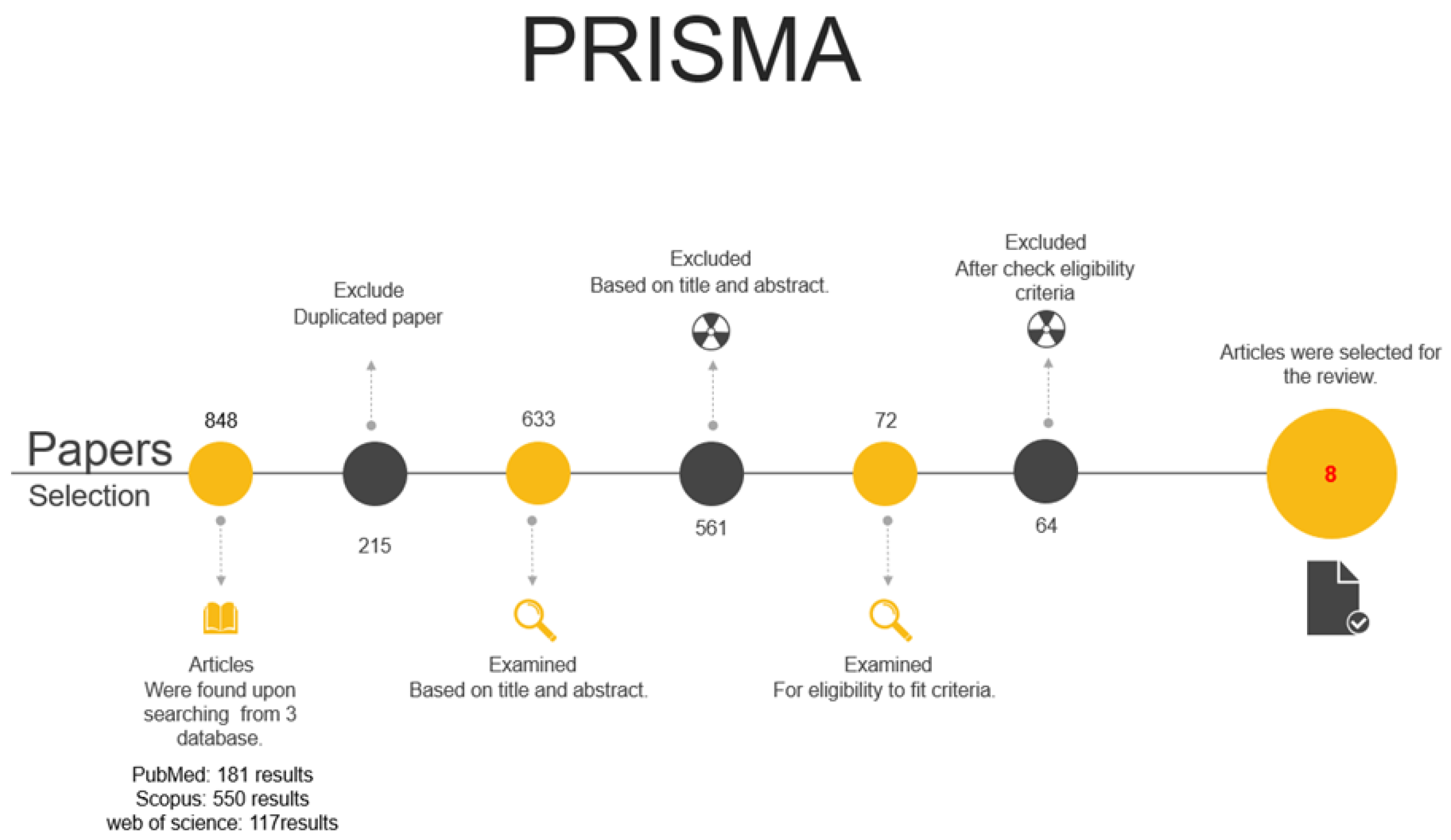
2.1. Search Strategy
2.1.1. Protocol
2.1.2. Eligibility Criteria
- P: Medically healthy individuals with an indication for teeth extraction.
- I: In socket preservation procedures, the use of graft materials affects both the quantity and quality of newly formed bone.
- C: Different graft materials.
- O: More effective in socket preservation.
- S: Randomized controlled trials (RCTs) and Clinical studies.
2.1.3. Primary Focus Question
2.1.4. Main Outcome
2.2. Inclusion Criteria and Exclusion Criteria
2.3. Data Collection
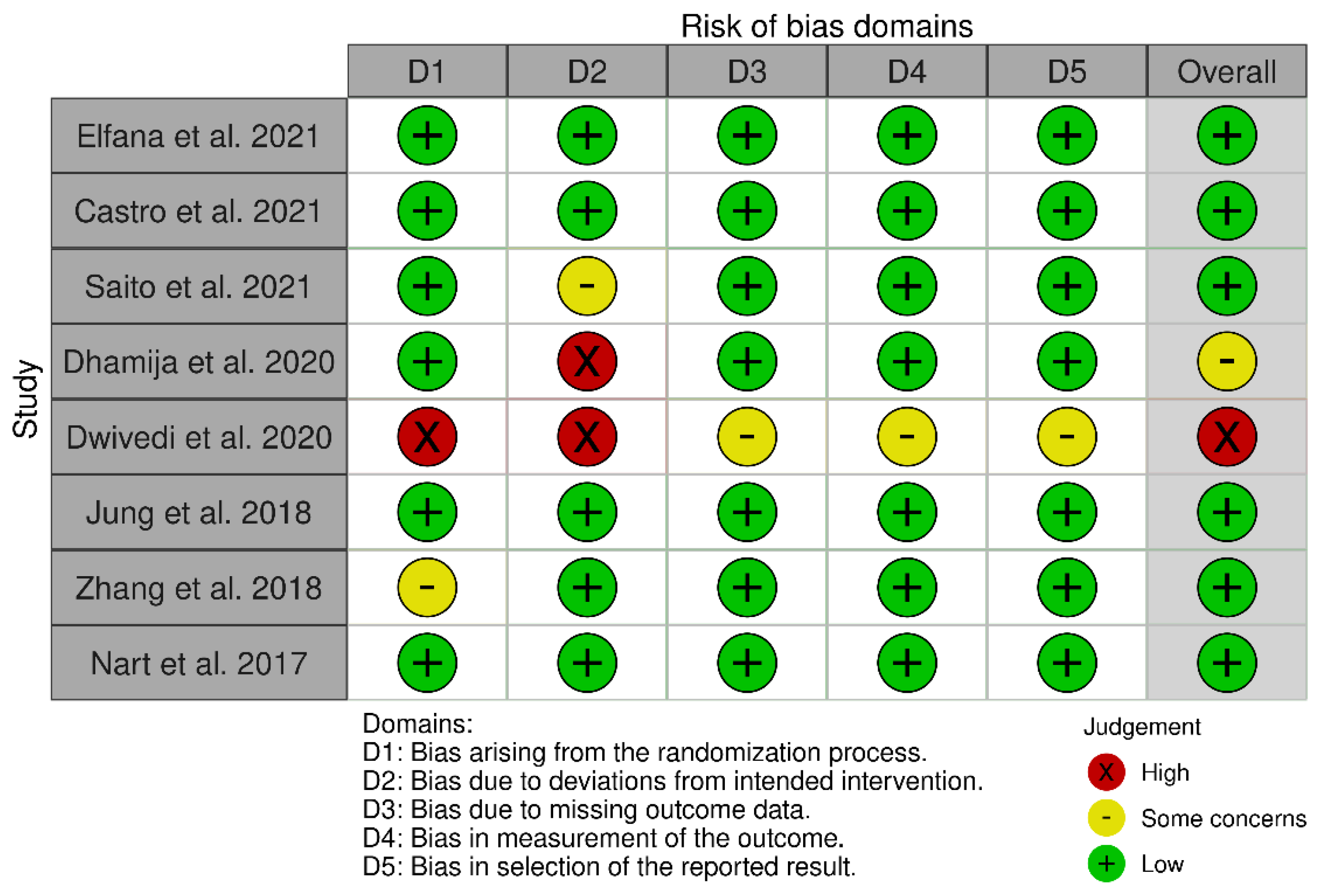
2.4. Risk of Bias (Quality) Assessment
3. Results
3.1. Excluded Studies
3.2. Characteristics of the Outcome Measures
3.3. Data Regarding the First Outcome (The Percentage of the Newly Formed Bone)
3.4. Data Regarding the Second Outcome (The Percentage of the Residual Graft Materials)
3.5. Data Regarding the Third Outcome (The Changes in Horizontal Width at the Follow-Up Period)
3.6. Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chapple, I.L.; Wilson, N.H. Manifesto for a paradigm shift: Periodontal health for a better life. Br. Dent. J. 2014, 216, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.; Baker, S.R.; Shahrbaf, S.; Martin, N.; Vettore, M.V. Oral health-related quality of life after prosthodontic treatment for patients with partial edentulism: A systematic review and meta-analysis. J. Prosthet. Dent. 2019, 121, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Wolleb, K.; Sailer, I.; Thoma, A.; Menghini, G.; Hammerle, C.H. Clinical and radiographic evaluation of patients receiving both tooth- and implant-supported prosthodontic treatment after 5 years of function. Int. J. Prosthodont. 2012, 25, 252–259. [Google Scholar]
- Atwood, D.A. Reduction of residual ridges: A major oral disease entity. J. Prosth. Dent. 1971, 27, 266–279. [Google Scholar] [CrossRef] [PubMed]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent. 2003, 23, 313–323. [Google Scholar]
- Paolantonio, M.; Dolci, M.; Scarano, A.; d’Archivio, D.; di Placido, G.; Tumini, V.; Piattelli, A. Immediate implantation in fresh extraction sockets: A controlled clinical and histological study in man. J. Periodontol. 2001, 72, 1560–1571. [Google Scholar] [CrossRef]
- Araujo, M.G.; Lindhe, J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J. Clin. Periodontol. 2005, 32, 212–218. [Google Scholar] [CrossRef]
- Araujo, M.G.; Sukekava, F.; Wennström, J.L.; Lindhe, J. Tissue modeling following implant placement in fresh extraction sockets. Clin. Oral Implant. Res. 2006, 17, 615–624. [Google Scholar] [CrossRef]
- Chen, S.T.; Buser, D. Clinical and esthetic outcomes of implants placed in postextraction sites. Int. J. Oral Maxillofac. Implant. 2009, 24, 186–217. [Google Scholar]
- Sanz, M.; Cecchinato, D.; Ferrus, J.; Pjetursson, E.B.; Lang, N.P.; Lindhe, J. A prospective, randomized-controlled clinical trial to evaluate bone preservation using implants with different geometry placed into extraction sockets in the maxilla. Clin. Oral Implant. Res. 2010, 21, 13–21. [Google Scholar] [CrossRef]
- Cirmeni, M.; Fedele, O.; Giammarinaro, E.; Marconcini, S.; Covani, U.; Caso, G. Immediate implant and socket preservation using sticky bone and leukocyte-platelet-rich fibrin in the anterior maxilla: A 3-year case report. Clin. Adv. Periodontics, 2022; epub ahead of print. [Google Scholar] [CrossRef]
- Eskow, A.J.; Mealey, B.L. Evaluation of healing following tooth extraction with ridge preservation using cortical versus cancellous freeze-dried bone allograft. J. Periodontol. 2014, 85, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Becker, W. Treatment of small defects adjacent to oral implants with various biomaterials. Periodontol 2000 2003, 33, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Vance, G.S.; Greenwell, H.; Miller, R.L.; Hill, M.; Johnston, H.; Scheetz, J.P. Comparison of an allograft in an experimental putty carrier and a bovine-derived xenograft used in ridge preservation: A clinical and histologic study in humans. Int. J. Oral Maxillofac. Implant. 2004, 19, 491–497. [Google Scholar]
- Darby, I.; Chen, S.T.; Buser, D. Ridge preservation techniques for implant therapy. Int. J. Oral Maxillofac. Implant. 2009, 24, 260–271. [Google Scholar]
- Chisci, G.; Fredianelli, L. Therapeutic Efficacy of Bromelain in Alveolar Ridge Preservation. Antibiotics. 2022, 11, 1542–1546. [Google Scholar] [CrossRef]
- Barone, A.; Aldini, N.N.; Fini, M.; Giardino, R.; Guirado, J.L.C.; Covani, U. Xenograft versus Extraction Alone for Ridge Preservation after Tooth Removal: A Clinical and Histomorphometric Study. J. Periodontol. 2008, 79, 1370–1377. [Google Scholar] [CrossRef]
- Araújo, M.G.; da Silva, J.C.C.; de Mendonça, A.F.; Lindhe, J. Ridge alterations following grafting of fresh extraction sockets in man. A randomized clinical trial. Clin. Oral Implant. Res. 2015, 26, 407–412. [Google Scholar] [CrossRef]
- Becker, W.; Cameron, C.; Sennerby, L.; Urist, M.R.; Becker, B.E. Histologic findings after implantation and evaluation of different grafting materials and titanium micro screws into extraction sockets: Case reports. J. Periodontol. 1998, 69, 414–421. [Google Scholar] [CrossRef]
- Araujo, M.G.; Lindhe, J. Ridge preservation with the use of Bio-Oss Collagen: A 6-month study in the dog. Clin. Oral Implant. Res. 2009, 20, 433–440. [Google Scholar] [CrossRef]
- Park, J.Y.; Koo, K.T.; Kim, T.I.; Seol, Y.J.; Lee, Y.M.; Ku, Y. Socket preservation using deproteinized horse-derived bone mineral. J. Periodontal Implant Sci. 2010, 40, 227–231. [Google Scholar] [CrossRef]
- Heberer, S.; Al-Chawaf, B.; Jablonski, C.; Nelson, J.J.; Lage, H.; Nelson, K. Healing of ungrafted and grafted extraction sockets after 12 weeks: A prospective clinical study. Int. J. Oral Maxillofac. Implant. 2011, 26, 385–392. [Google Scholar]
- Barone, A.; Ricci, M.; Tonelli, P.; Santini, S.; Covani, U. Tissue changes of extraction sockets in humans: A comparison of spontaneous healing vs. ridge preservation with secondary soft tissue healing. Clin. Oral Implants Res. 2013, 24, 1231–1237. [Google Scholar] [CrossRef]
- Chisci, G.; Hatia, A.; Chisci, E.; Chisci, D.; Gennaro, P.; Gabriele, G. Socket Preservation after Tooth Extraction: Particulate Autologous Bone vs. Deproteinized Bovine Bone. Bioengineering 2023, 10, 421. [Google Scholar] [CrossRef] [PubMed]
- Vignoletti, F.; Matesanz, P.; Rodrigo, D.; Figuero, E.; Martin, C.; Sanz, M. Surgical protocols for ride preservation after tooth extraction. A systematic review. Clin. Oral Implant. Res. 2012, 23, 22–38. [Google Scholar] [CrossRef] [PubMed]
- Avila-Ortiz, G.; Chambrone, L.; Vignoletti, F. Effect of alveolar ridge preservation interventions following tooth extraction: A systematic review and meta-analysis. J. Clin. Periodontol. 2019, 46, 195–223. [Google Scholar] [CrossRef]
- Um, I.W.; Hwang, S.H.; Kim, Y.K.; Kim, M.Y.; Jun, S.H.; Ryu, J.J.; Jang, H.S. Demineralized dentin matrix combined with recombinant human bone morphogenetic protein-2 in rabbit calvarial defects. J. Korean Assoc. Oral Maxillofac. 2016, 42(2), 90–98. [Google Scholar] [CrossRef]
- Moher, D.; Altman, D.G.; Liberati, A.; Tetzlaff, J. PRISMA statement. Epidemiology 2011, 22, 128. [Google Scholar] [CrossRef]
- Higgins, J.P. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0. Updated March 2011; The Cochrane Collaboration: London, UK, 2011; Available online: www.cochrane-handbook.Org (accessed on 9 September 2022).
- Elfana, A.; El-Kholy, S.; Saleh, H.A.; Fawzy El-Sayed, K. Alveolar ridge preservation using autogenous whole-tooth versus demineralized dentin grafts: A randomized controlled clinical trial. Clin. Oral Implant. Res. 2021, 32, 539–548. [Google Scholar] [CrossRef]
- Castro, A.B.; Van Dessel, J.; Temmerman, A.; Jacobs, R.; Quirynen, M. Effect of different platelet-rich fibrin matrices for ridge preservation in multiple tooth extractions: A split-mouth randomized controlled clinical trial. J. Clin. Periodontol. 2021, 48, 984–995. [Google Scholar] [CrossRef]
- Saito, H.; Couso-Queiruga, E.; Shiau, H.J.; Stuhr, S.; Prasad, H.; Allareddy, T.V.; Reynolds, M.A.; Avila-Ortiz, G. Evaluation of poly lactic-co-glycolic acid-coated β-tricalcium phosphate for alveolar ridge preservation: A multicenter randomized controlled trial. J. Periodontol. 2021, 92, 524–535. [Google Scholar] [CrossRef]
- Dhamija, R.; Shetty, V.; Vineeth, K.; Nagaraju, R.; Rao, R.S. Socket preservation with demineralized freeze-dried bone allograft and platelet-rich fibrin for implant site development: A randomized controlled trial. J. Indian Prosthodont. Soc. 2020, 20, 304. [Google Scholar] [CrossRef] [PubMed]
- Dwivedi, A.; Kour, M. A neoteric procedure for alveolar ridge preservation using autogenous fresh mineralized tooth graft prepared at chair side. J. Oral Biol. Craniofac. Res. 2020, 10, 535–541. [Google Scholar] [CrossRef] [PubMed]
- Jung, G.U.; Jeon, T.H.; Kang, M.H.; Um, I.W.; Song, I.S.; Ryu, J.J.; Jun, S.H. Volumetric, radiographic, and histologic analyses of demineralized dentin matrix combined with recombinant human bone morphogenetic protein-2 for ridge preservation: A prospective randomized controlled trial in comparison with xenograft. Appl. Sci. 2018, 8, 1288. [Google Scholar] [CrossRef]
- Zhang, Y.; Ruan, Z.; Shen, M.; Tan, L.; Huang, W.; Wang, L.; Huang, Y. Clinical effect of platelet-rich fibrin on the preservation of the alveolar ridge following tooth extraction. Exp. Ther. Med. 2018, 15, 2277–2286. [Google Scholar] [CrossRef] [PubMed]
- Nart, J.; Barallat, L.; Jimenez, D.; Mestres, J.; Gómez, A.; Carrasco, M.A.; Violant, D.; Ruíz-Magaz, V. Radiographic and histological evaluation of deproteinized bovine bone mineral vs. deproteinized bovine bone mineral with 10% collagen in ridge preservation. A randomized controlled clinical trial. Clin. Oral Implant. Res. 2017, 28, 840–848. [Google Scholar] [CrossRef] [PubMed]
- Iorio-Siciliano, V.; Blasi, A.; Nicolò, M.; Iorio-Siciliano, A.; Riccitiello, F.; Ramaglia, L. Clinical Outcomes of Socket Preservation Using Bovine-Derived Xenograft Collagen and Collagen Membrane Post-Tooth Extraction: A 6-Month Randomized Controlled Clinical Trial. Int. J. Periodontics Restor. Dent. 2017, 37, e290–e296. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani, A.A.; Murriky, A.; Shafik, S. Influence of platelet rich fibrin on post-extraction socket healing: A clinical and radiographic study. Saudi Dent. J. 2017, 29, 149–155. [Google Scholar] [CrossRef]
- Adam, S.A.; Elarab, A.E.; Rahman, A.R.; Rahim, D.A. Evaluation of implant stability and marginal bone loss in immediate implant using “nano bone” versus “autogenous bone” for the treatment of patients with unrestorable single tooth: A randomized controlled trial. J. Osseointegration 2020, 12, 8–17. [Google Scholar]
- Gkikas, G.; McLaughlin, M.; Renvert, S.; Polyzois, I. A Prospective Study Comparing the Effect of L-PRF and Porous Titanium Granules on the Preservation of the Buccal Bone Plate Following Immediate Implant Placement. Int. J. Periodontics Restor. Dent. 2020, 40, 767–774. [Google Scholar] [CrossRef]
- Giuliani, A.; Iezzi, G.; Mazzoni, S.; Piattelli, A.; Perrotti, V.; Barone, A. Regenerative properties of collagenated porcine bone grafts in human maxilla: Demonstrative study of the kinetics by synchrotron radiation microtomography and light microscopy. Clin. Oral Investig. 2018, 22, 505–513. [Google Scholar] [CrossRef]
- Kakar, A.; Rao, B.H.; Hegde, S.; Deshpande, N.; Lindner, A.; Nagursky, H.; Patney, A.; Mahajan, H. Ridge preservation using an in situ hardening biphasic calcium phosphate (β-TCP/HA) bone graft substitute—A clinical, radiological, and histological study. Int. J. Implant Dent. 2017, 3, 25. [Google Scholar] [CrossRef]
- Kivovics, M.; Szabó, B.T.; Németh, O.; Tari, N.; Dőri, F.; Nagy, P.; Dobó-Nagy, C.; Szabó, G. Microarchitectural study of the augmented bone following ridge preservation with a porcine xenograft and a collagen membrane: Preliminary report of a prospective clinical, histological, and micro-computed tomography analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 250–260. [Google Scholar] [CrossRef] [PubMed]
- Min, B.M. Oral Biochemistry; Daehan Narae Publishing: Seoul, Republic of Korea, 2007; pp. 8–73. ISBN 978-897-089-146-0. [Google Scholar]
- Wood, R.A.; Mealey, B.L. Histologic comparison of healing after tooth extraction with ridge preservation using mineralized versus demineralized freeze-dried bone allograft. J. Periodontol. 2012, 83, 329–336. [Google Scholar] [CrossRef]
- Beck, T.M.; Mealey, B.L. Histologic analysis of healing after tooth extraction with ridge preservation using mineralized human bone allograft. J. Periodontol. 2010, 81, 1765–1772. [Google Scholar] [CrossRef] [PubMed]
- Froum, S.; Cho, S.C.; Rosenberg, E.; Rohrer, M.; Tarnow, D. Histological comparison of healing extraction sockets implanted with bioactive glass or demineralized freeze-dried bone allograft: A pilot study. J. Periodontol. 2002, 73, 94–102. [Google Scholar] [CrossRef] [PubMed]
- Koga, T.; Minamizato, T.; Kawai, Y.; Miura, K.I.; Nakatani, Y.; Sumita, Y.; Asahina, I. Bone regeneration using dentin matrix depends on the degree of demineralization and particle size. PLoS ONE 2016, 11, e0147235. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Mah, Y.J.; Kim, D.H.; Kim, E.S.; Park, E.J. Demineralized deciduous tooth as a source of bone graft material: Its biological and physicochemical characteristics. Oral Surg. Oral Med. Oral Radiol. 2015, 120, 307–314. [Google Scholar] [CrossRef]
- Li, R.; Guo, W.; Yang, B.; Guo, L.; Sheng, L.; Chen, G.; Li, Y.; Zou, Q.; Xie, D.; An, X.; et al. Human treated dentin matrix as a natural scaffold for complete human dentin tissue regeneration. Biomaterials 2011, 32, 4525–4538. [Google Scholar] [CrossRef]
- Castro, A.B.; Cortellini, S.; Temmerman, A.; Li, X.; Pinto, N.; Teughels, W.; Quirynen, M. Characterization of the leukocyte- and platelet-rich fibrin block: Release of growth factors, cellular content, and structure. Int. J. Oral Maxillofac. Implant. 2019, 34, 855–864. [Google Scholar] [CrossRef]
- Hachim, D.; Whittaker, T.E.; Kim, H.; Stevens, M.M. Glycosaminoglycan-based biomaterials for growth factor and cytokine delivery: Making the right choices. J. Control. Release 2019, 313, 131–147. [Google Scholar] [CrossRef]
- Geurs, N.; Ntounis, A.; Vassilopoulos, P.; Van der Velden, U.; Loos, B.G.; Reddy, M. Using growth factors in human extraction sockets: A histologic and histomorphometric evaluation of short-term healing. Int. J. Oral Maxillofac. Implant. 2014, 29, 485–496. [Google Scholar] [CrossRef]
- Leventis, M.D.; Fairbairn, P.; Kakar, A.; Leventis, A.D.; Margaritis, V.; Lückerath, W.; Horowitz, R.A.; Rao, B.H.; Lindner, A.; Nagursky, H. Minimally invasive alveolar ridge preservation utilizing an in situ hardening β-tricalcium phosphate bone substitute: A multicenter case series. Int. J. Dent. 2016, 2016, 5406736. [Google Scholar] [CrossRef]
- Kargarpour, Z.; Nasirzade, J.; Strauss, F.J.; Di Summa, F.; Hasannia, S.; Müller, H.D.; Gruber, R. Platelet-rich fibrin suppresses in vitro osteoclastogenesis. J. Periodontol. 2020, 91, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Strauss, F.J.; Nasirzade, J.; Kargarpoor, Z.; Stähli, A.; Gruber, R. Effect of platelet-rich fibrin on cell proliferation, migration, differentiation, inflammation, and osteoclastogenesis: A systematic review of in vitro studies. Clin. Oral Investig. 2020, 24, 569–584. [Google Scholar] [CrossRef]
- Castro, A.B.; Meschi, N.; Temmerman, A.; Pinto, N.; Lambrechts, P.; Teughels, W.; Quirynen, M. Regenerative potential of leucocyte- and platelet-rich fibrin. Part B: Sinus floor elevation, alveolar ridge preservation and implant therapy. A systematic review. J. Clin. Periodontol. 2017, 44, 225–234. [Google Scholar] [CrossRef]
- Strauss, F.J.; Stähli, A.; Gruber, R. The use of platelet-rich fibrin to enhance the outcomes of implant therapy: A systematic review. Clin. Oral Implant. Res. 2018, 29, 6–19. [Google Scholar] [CrossRef]
- Temmerman, A.; Vandessel, J.; Castro, A.; Jacobs, R.; Teughels, W.; Pinto, N.; Quirynen, M. The use of leucocyte and platelet-rich fibrin in socket management and ridge preservation: A split-mouth, randomized, controlled clinical trial. J. Clin. Periodontol. 2016, 43, 990–999. [Google Scholar] [CrossRef]
- Canellas, J.; da Costa, R.C.; Breves, R.C.; de Oliveira, G.P.; Figueredo, C.; Fischer, R.G.; Thole, A.A.; Medeiros, P.J.D.; Ritto, F.G. Tomographic and histomorphometric evaluation of socket healing after tooth extraction using leukocyte- and platelet-rich fibrin: A randomized, single-blind, controlled clinical trial. J. Cranio-Maxillofac. Surg. 2020, 48, 24–32. [Google Scholar] [CrossRef]
- Dragonas, P.; Katsaros, T.; Avila-Ortiz, G.; Chambrone, L.; Schiavo, J.H.; Palaiologou, A. Effects of leukocyte–platelet-rich fibrin (L-PRF) in different intraoral bone grafting procedures: A systematic review. Int. J. Oral Maxillofac. Surg. 2019, 48, 250–262. [Google Scholar] [CrossRef] [PubMed]
- Mourão, C.F.; de Mello-Machado, R.C.; Javid, K.; Moraschini, V. The use of leukocyte-and platelet-rich fibrin in the management of soft tissue healing and pain in post-extraction sockets: A randomized clinical trial. J. Cranio-Maxillofac. Surg. 2020, 48, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Abad, C.E.; Sanz-Sanchez, I.; Serrano, V.; Sanz Esporrin, J.; Sanz-Martin, I.; Sanz, M. Efficacy of the application of leukocyte and platelet-rich fibrin (L-PRF) on alveolar ridge preservation. A randomized controlled clinical trial. Clin. Implant Dent. Relat. Res, 2023; epub ahead of print. [Google Scholar] [CrossRef]
- Pang, K.M.; Um, I.W.; Kim, Y.K.; Woo, J.M.; Kim, S.M.; Lee, J.H. Autogenous demineralized dentin matrix from extracted tooth for the augmentation of alveolar bone defect: A prospective randomized clinical trial in comparison with anorganic bovine bone. Clin. Oral Implant. Res. 2017, 28, 809–815. [Google Scholar] [CrossRef] [PubMed]
- MacBeth, N.D.; Donos, N.; Mardas, N. Alveolar ridge preservation with guided bone regeneration or socket seal technique. A randomized, single-blind controlled clinical trial. Clin. Oral Implant. Res. 2022, 33, 681–699. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, M.T.; Guillen, G.A.; Macêdo, F.G.; Goulart, D.R.; Nóia, C.F. Comparative Effects of Different Materials on Alveolar Preservation. J. Oral Maxillofac. Surg. 2023, 81, 213–223. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study Type | Author/Year | Extraction Teeth | Study Groups | Membrane | Graft Quantity and Size | Follow-Up Period | Outcome 1 The Percentage of the Newly Formed Bone | Outcome 2 The Percentage of the Residual Graft Materials | Outcome 3 The Changes in Horizontal Width at the Follow-Up Period |
|---|---|---|---|---|---|---|---|---|---|
| RCT | Elfana et al., 2021 [30] | Singles rooted teeth | n = 10 Test: AWTG group Control: ADDG | Bioabsorbable collagen membrane. Open membrane approach | 6 months | AWTG group 37.55 ± 8.94% ADDG group 48.40 ± 11.56% | AWTG: 18.07 ± 5.58% ADDG: 11.45 ± 4.13% | AWTG group (test) : 6.80 ± 2.61% : 0.61 ± 0.20 mm ADDG group (control) : 8.43 ± 3.66% : 0.72 ± 0.27 mm | |
| RCT | Castro et al., 2021 [31] | Singles rooted teeth | n = 10 Test: L-PRF or A-PRF+ Control: unassisted socket healing. | L-PRF/A-PRF+ | 3 months | L-PRF: 47.7 ± 7.9% A-PRF+: 54.5 ± 5.6% | none | L-PRF group HW-1 mm: −2.2 + 1 HW-3 mm: −1.8 + −1.7 HW-5 mm: −1.2 + 0.8 A-PRF+ group HW-1 mm: −2.2 + 0.9 HW-3 mm: −1.6 + 0.9 HW-5 mm: −1.2 + 0.8 | |
| RCT | Saito et al., 2021 [32] | Multi-rooted and single Posterior teeth | n = 43 Group 20 Control: 23 | Group1/ moldable PLGA-β-TCP Group2/ FDBA material covered with a RACD | The socket was filled with the graft material up to the bone crest | 16 weeks (4 m) | Group A = 27.0 ± 22.1% Group B = 38.2 ± 12.5% | Group A = 20.5 ± 16.8% Group B = 15.7 ± 7.0%. | Group A At 3 mm: 0.61 ± 0.92 At 5 mm: 0.29 ± 0.56 Group B At 3 mm: 0.68 ± 1.59 At 5 mm: 0.56 ± 0.75 |
| RCT | Dhamija et al., 2020 [33] | Multi rooted teeth | n = 15/group Test: socket preservation using DFDBA + PRF Control: no graft was placed. | DFDBA + PRF | 0.5 cc vial for each test group socket DFDBA 500–1000 μ particulate | 16 weeks for the histological analysis 3–6 months for CBCT | Control: 53.05 ± 15.43% Test: 57.32 ± 19.94% | 1.5% | The ridge width differences before extraction and implant placement. At 2 mm and Control: 2.6 ± 0.62 Test: 3.27 ± 0.48 At 6 mm Control: 2.07 ± 0.43 Test: 3.26 ± 0.41 No significant difference was observed between the groups. |
| Dwivedi et al., 2020 [34] | Single and multirooted teeth | n = 30 Control: autogenous bone graft Test: autogenous tooth graft | No membrane | No | 3 years | 34–66% of new bone formation in 40% of cases. 67–100% of bone formation in 60% of cases. | None | - Alveolar width Pre(mm.): 11.652 mm. - Alveolar Width Post (mm): 12.330 | |
| RCT | Jung et al., 2018 [35] | one or more (premolar and molar). | n = 10 1st Group: Bio-Oss® Collagen 2nd group: DDM graft 3rd group: rhBMP-2 + DDM | DBBC and DDM | DDM ranged from 0.5 mm to 1 mm in diameter. | 4 months | Ist group: 22.00 ± 11.01% 2nd group: 32.88 ± 14.48% 3rd group: 39.09 ± 15.30% | Ist group: 13.20 ± 9.79 2nd group: 10.72 ± 9.83 3rd group: 11.02 ± 12.72 | Ist group: 1.14 ± 0.81 2nd group: 0.97 ± 0.39 3rd group: 0.82 ± 0.36 Alveolar bone heights and widths in the three groups (1, 2, 3) at baseline and 4 months following ridge preservation. |
| Zhang et al., 2018 [36] | Multirooted teeth | n = 14 Control: Naturally healing sockets Tests: PRF membrane | PRF membrane | No | CBCT and histology after 3 months | Test: 9.7624 ± 4.0121% Control: 2.8056 ± 1.2094% | None | Test: 1.0500 ± 0.77862 Control: 2.0760 ± 1.67149 | |
| RCT | Nart et al., 2017 [37] | extraction of non-molar tooth | n = 11 Group 1: DBBM Group 2: DBBM +10% collagen (DBBM-C) | collagen membrane | No | 5 months | DBBM group: 33.44 ± 17.82% DBBM-C group: 37.68 ± 13.38% | DBBM group (group 1): 13.14 ± 8.32% DBBM-C group (group 2): 16.00 ± 11.60% | DBBM group: Ridge width reduction of 9.42% at 1 mm 3.21% at 3 mm 2.53% at 5 mm DBBM-C group: Ridge width reduction of 13.83% at 1 mm 6.43% at 3 mm 4.16% at 5 mm |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Madi, M.; Almindil, I.; Alrassasi, M.; Alramadan, D.; Zakaria, O.; Alagl, A.S. Cone-Beam Computed Tomography and Histological Findings for Socket Preservation Techniques Using Different Grafting Materials: A Systematic Review. J. Funct. Biomater. 2023, 14, 282. https://doi.org/10.3390/jfb14050282
Madi M, Almindil I, Alrassasi M, Alramadan D, Zakaria O, Alagl AS. Cone-Beam Computed Tomography and Histological Findings for Socket Preservation Techniques Using Different Grafting Materials: A Systematic Review. Journal of Functional Biomaterials. 2023; 14(5):282. https://doi.org/10.3390/jfb14050282
Chicago/Turabian StyleMadi, Marwa, Ibrahim Almindil, Maria Alrassasi, Doha Alramadan, Osama Zakaria, and Adel S Alagl. 2023. "Cone-Beam Computed Tomography and Histological Findings for Socket Preservation Techniques Using Different Grafting Materials: A Systematic Review" Journal of Functional Biomaterials 14, no. 5: 282. https://doi.org/10.3390/jfb14050282