
Comparing the Long-Term Success Rates of Tooth Preservation and Dental Implants: A Critical Review
 , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Definitions and Search Process
3. Survival of Endodontically Treated Teeth
4. Survival of Teeth Treated with Post-and-Core Restorations
5. Survival of Periodontal Treated Teeth
6. Survival of Dental Implants
7. Implications for Clinical Practice and Future Perspective
8. Conclusions
- The available evidence indicates similar long-term survival rates between endodontically treated teeth and dental implants.
- Regarding teeth treated with post-and-core restorations, the evidence suggests that decision-making to restore a tooth should be based on the amount of remaining tooth structure. This factor is usually more significant than the type of material used for post-and-core buildups.
- The long-term prognosis of teeth treated in the presence of periodontal disease is proportional to the disease stage, quality of treatment, biofilm control, and periodic maintenance.
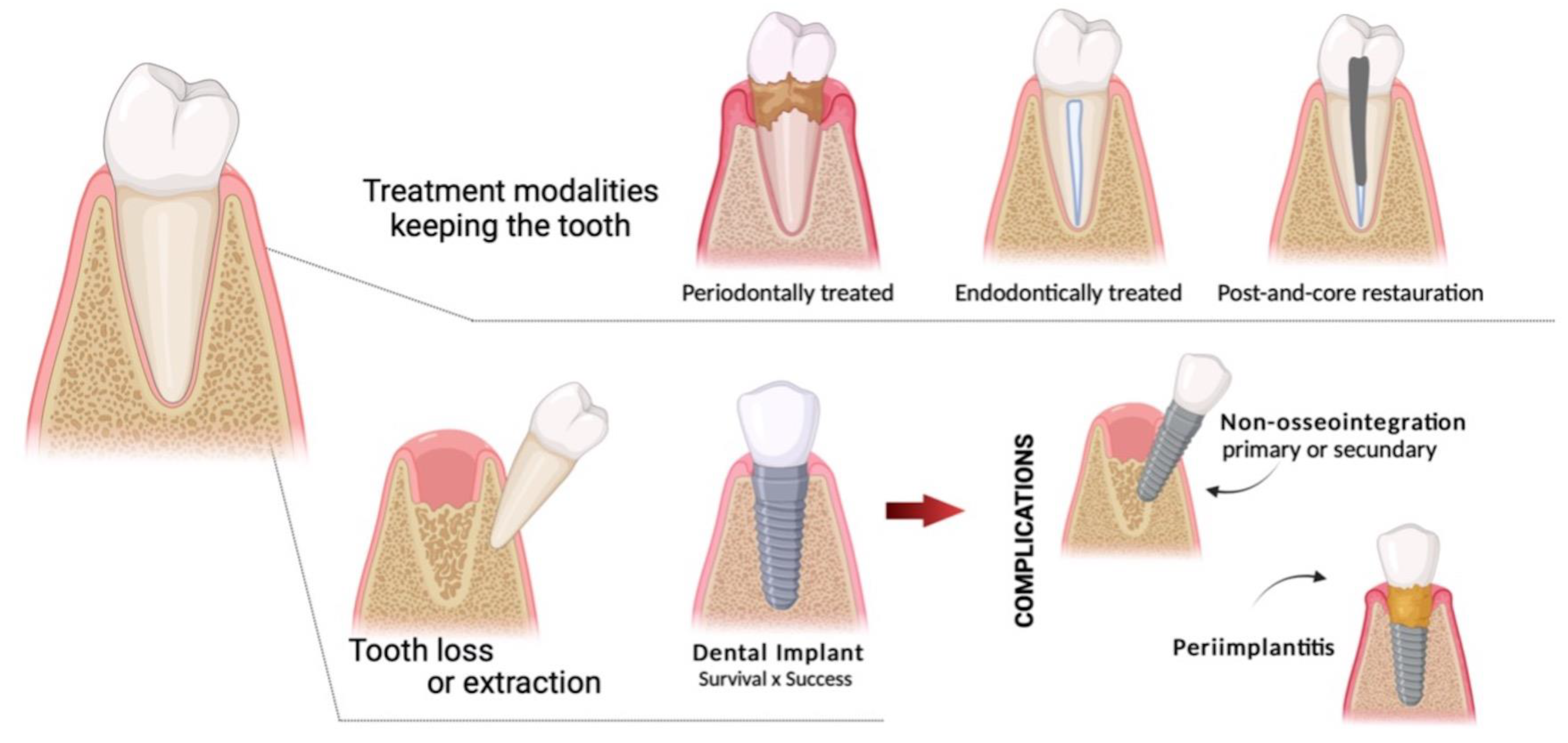
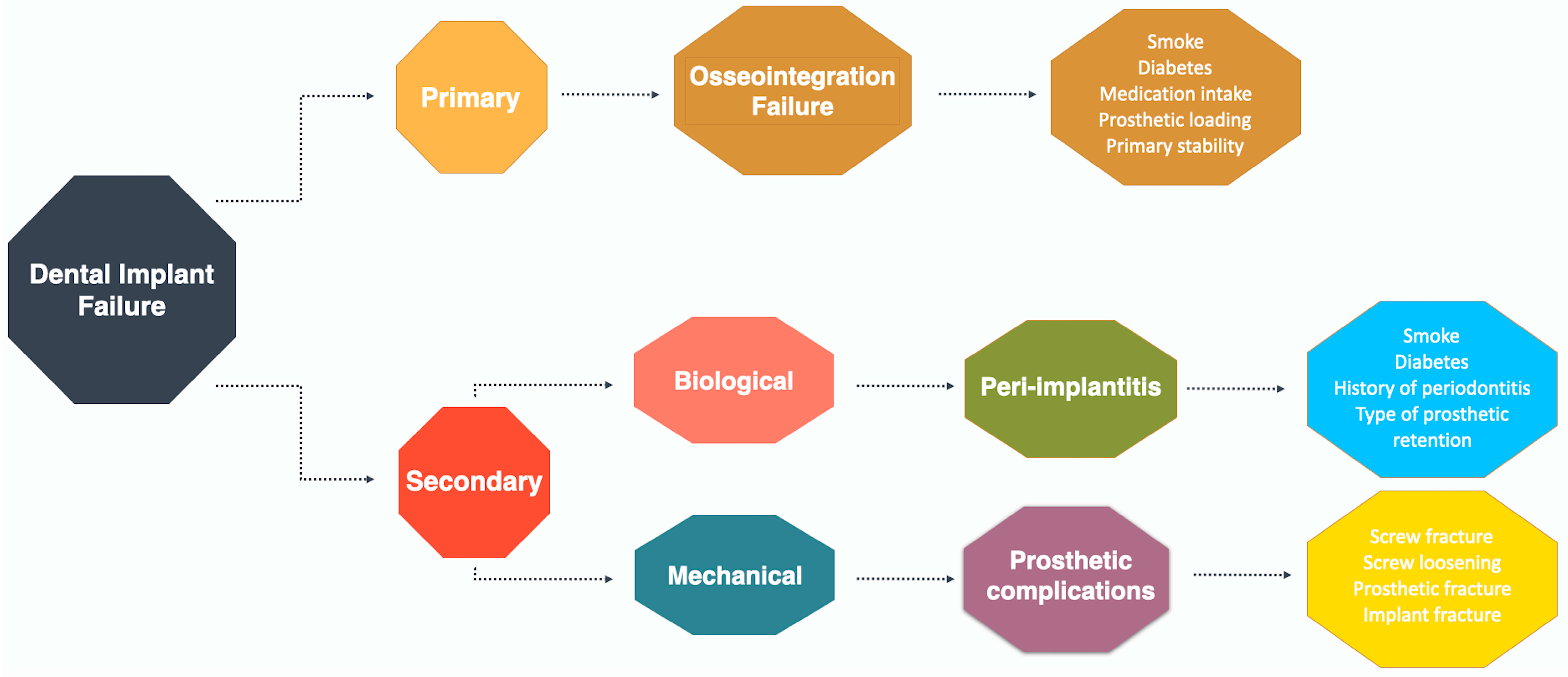
- Longitudinal studies show high success rates and long-term survival of dental implants. However, failures and complications are common.
- Overall, the evidence suggests that the decision between keeping a tooth or replacing it with an implant should be based on the condition of the tooth (e.g., amount of remaining tooth and degree of attachment loss and mobility), the systemic condition, and patient preference.
- Better attempts should be focused first on saving manageable teeth over the long-term, instead of immediately applying implant therapies.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marrone, A.; Lasserre, J.; Bercy, P.; Brecx, M.C. Prevalence and risk factors for peri-implant disease in Belgian adults. Clin. Oral Implant. Res. 2013, 24, 934–940. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.; Stadlinger, B.; Schwarz, F.; Beck-Broichsitter, B.; Jung, O.; Precht, C.; Kloss, F.; Grobe, A.; Heiland, M.; Ebker, T. Impact of Dental Implant Surface Modifications on Osseointegration. Biomed. Res. Int. 2016, 2016, 6285620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontol. 2000 2017, 73, 121–133. [Google Scholar] [CrossRef]
- Moraschini, V.; Poubel, L.A.; Ferreira, V.F.; Barboza Edos, S. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef]
- Duong, H.Y.; Roccuzzo, A.; Stahli, A.; Salvi, G.E.; Lang, N.P.; Sculean, A. Oral health-related quality of life of patients rehabilitated with fixed and removable implant-supported dental prostheses. Periodontol. 2000 2022, 88, 201–237. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Persson, L.; Klinge, B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J. Clin. Periodontol. 2002, 29 (Suppl. 3), 197–212; discussion 232–233. [Google Scholar] [CrossRef] [PubMed]
- Avila, G.; Galindo-Moreno, P.; Soehren, S.; Misch, C.E.; Morelli, T.; Wang, H.L. A novel decision-making process for tooth retention or extraction. J. Periodontol. 2009, 80, 476–491. [Google Scholar] [CrossRef]
- Ekelund, J.A.; Lindquist, L.W.; Carlsson, G.E.; Jemt, T. Implant treatment in the edentulous mandible: A prospective study on Branemark system implants over more than 20 years. Int. J. Prosthodont. 2003, 16, 602–608. [Google Scholar]
- Lindquist, L.W.; Carlsson, G.E.; Jemt, T. A prospective 15-year follow-up study of mandibular fixed prostheses supported by osseointegrated implants. Clinical results and marginal bone loss. Clin. Oral Implant. Res. 1996, 7, 329–336. [Google Scholar] [CrossRef]
- Schwarz, F.; Ramanauskaite, A. It is all about peri-implant tissue health. Periodontol. 2000 2022, 88, 9–12. [Google Scholar] [CrossRef]
- Moraschini, V.; Kischinhevsky, I.C.C.; Sartoretto, S.C.; de Almeida Barros Mourao, C.F.; Sculean, A.; Calasans-Maia, M.D.; Shibli, J.A. Does implant location influence the risk of peri-implantitis? Periodontol. 2000 2022, 90, 224–235. [Google Scholar] [CrossRef] [PubMed]
- Muller, F.; Srinivasan, M.; Krause, K.H.; Schimmel, M. Periodontitis and peri-implantitis in elderly people experiencing institutional and hospital confinement. Periodontol. 2000 2022, 90, 138–145. [Google Scholar] [CrossRef]
- Levin, L.; Halperin-Sternfeld, M. Tooth preservation or implant placement: A systematic review of long-term tooth and implant survival rates. J. Am. Dent. Assoc. 2013, 144, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Faggion, C.M., Jr.; Petersilka, G.; Lange, D.E.; Gerss, J.; Flemmig, T.F. Prognostic model for tooth survival in patients treated for periodontitis. J. Clin. Periodontol. 2007, 34, 226–231. [Google Scholar] [CrossRef] [PubMed]
- Priest, G. Single-tooth implants and their role in preserving remaining teeth: A 10-year survival study. Int. J. Oral Maxillofac. Implant. 1999, 14, 181–188. [Google Scholar]
- Van der Weijden, G.A.F.; Dekkers, G.J.; Slot, D.E. Success of non-surgical periodontal therapy in adult periodontitis patients: A retrospective analysis. Int. J. Dent. Hyg. 2019, 17, 309–317. [Google Scholar] [CrossRef] [Green Version]
- Lang NP, L.J. Clinical Periodontology and Implant Dentistry, 6th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2015; Volume 2. [Google Scholar]
- Ramfjord, S.P. Maintenance care for treated periodontitis patients. J. Clin. Periodontol. 1987, 14, 433–437. [Google Scholar] [CrossRef]
- Tavelli, L.; Barootchi, S.; Avila-Ortiz, G.; Urban, I.A.; Giannobile, W.V.; Wang, H.L. Peri-implant soft tissue phenotype modification and its impact on peri-implant health: A systematic review and network meta-analysis. J. Periodontol. 2021, 92, 21–44. [Google Scholar] [CrossRef]
- Torabinejad, M.; Anderson, P.; Bader, J.; Brown, L.J.; Chen, L.H.; Goodacre, C.J.; Kattadiyil, M.T.; Kutsenko, D.; Lozada, J.; Patel, R.; et al. Outcomes of root canal treatment and restoration, implant-supported single crowns, fixed partial dentures, and extraction without replacement: A systematic review. J. Prosthet. Dent. 2007, 98, 285–311. [Google Scholar] [CrossRef]
- Rinke, S.; Ohl, S.; Ziebolz, D.; Lange, K.; Eickholz, P. Prevalence of periimplant disease in partially edentulous patients: A practice-based cross-sectional study. Clin. Oral Implant. Res. 2011, 22, 826–833. [Google Scholar] [CrossRef]
- Kordbacheh Changi, K.; Finkelstein, J.; Papapanou, P.N. Peri-implantitis prevalence, incidence rate, and risk factors: A study of electronic health records at a U.S. dental school. Clin. Oral Implant. Res. 2019, 30, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Lindhe, J.; Meyle, J.; Group D of the European Workshop on Periodontology. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignoletti, F.; Di Domenico, G.L.; Di Martino, M.; Montero, E.; de Sanctis, M. Prevalence and risk indicators of peri-implantitis in a sample of university-based dental patients in Italy: A cross-sectional study. J. Clin. Periodontol. 2019, 46, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Torabinejad, M.; Landaez, M.; Milan, M.; Sun, C.X.; Henkin, J.; Al-Ardah, A.; Kattadiyil, M.; Bahjri, K.; Dehom, S.; Cortez, E.; et al. Tooth retention through endodontic microsurgery or tooth replacement using single implants: A systematic review of treatment outcomes. J. Endod. 2015, 41, 1–10. [Google Scholar] [CrossRef]
- Vozza, I.; Barone, A.; Quaranta, M.; De Paolis, G.; Covani, U.; Quaranta, A. A comparison between endodontics and implantology: An 8-year retrospective study. Clin. Implant. Dent. Relat. Res. 2013, 15, 29–36. [Google Scholar] [CrossRef]
- Iqbal, M.K.; Kim, S. A review of factors influencing treatment planning decisions of single-tooth implants versus preserving natural teeth with nonsurgical endodontic therapy. J. Endod. 2008, 34, 519–529. [Google Scholar] [CrossRef]
- Setzer, F.C.; Kim, S. Comparison of long-term survival of implants and endodontically treated teeth. J. Dent. Res. 2014, 93, 19–26. [Google Scholar] [CrossRef]
- Papaspyridakos, P.; Chen, C.J.; Singh, M.; Weber, H.P.; Gallucci, G.O. Success criteria in implant dentistry: A systematic review. J. Dent. Res. 2012, 91, 242–248. [Google Scholar] [CrossRef]
- Ng, Y.L.; Mann, V.; Gulabivala, K. Tooth survival following non-surgical root canal treatment: A systematic review of the literature. Int. Endod. J. 2010, 43, 171–189. [Google Scholar] [CrossRef]
- Vahdati, S.A.; Torabinejad, M.; Handysides, R.; Lozada, J. A Retrospective Comparison of Outcome in Patients Who Received Both Nonsurgical Root Canal Treatment and Single-tooth Implants. J. Endod. 2019, 45, 99–103. [Google Scholar] [CrossRef]
- Iqbal, M.K.; Kim, S. For teeth requiring endodontic treatment, what are the differences in outcomes of restored endodontically treated teeth compared to implant-supported restorations? Int. J. Oral Maxillofac. Implant. 2007, 22, 96–116. [Google Scholar]
- Prati, C.; Pirani, C.; Zamparini, F.; Gatto, M.R.; Gandolfi, M.G. A 20-year historical prospective cohort study of root canal treatments. A Multilevel analysis. Int. Endod. J. 2018, 51, 955–968. [Google Scholar] [CrossRef] [PubMed]
- Landys Boren, D.; Jonasson, P.; Kvist, T. Long-term survival of endodontically treated teeth at a public dental specialist clinic. J. Endod. 2015, 41, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, R.; Cardona, J.A.; Cadavid, D.; Alvarez, L.G.; Restrepo, F.A. Survival of Endodontically Treated Roots/Teeth Based on Periapical Health and Retention: A 10-year Retrospective Cohort Study. J. Endod. 2017, 43, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- Imura, N.; Pinheiro, E.T.; Gomes, B.P.; Zaia, A.A.; Ferraz, C.C.; Souza-Filho, F.J. The outcome of endodontic treatment: A retrospective study of 2000 cases performed by a specialist. J. Endod. 2007, 33, 1278–1282. [Google Scholar] [CrossRef]
- Ricucci, D.; Russo, J.; Rutberg, M.; Burleson, J.A.; Spangberg, L.S. A prospective cohort study of endodontic treatments of 1369 root canals: Results after 5 years. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 825–842. [Google Scholar] [CrossRef] [PubMed]
- Akbari, M.A.H.; Jamali, H.; Gholami, A.A.; Majidinia, S. One-Year Clinical Comparison of Survival of Endodontically Treated Premolar Restored with Different Direct Restoration Technique: A Prospective Cohort Study. Razavi Int. J. Med. Inpress 2016, 4, e39800. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, A.M.; Richards, L.C.; Berekally, T.L. Effect of remaining tooth structure on the fracture resistance of endodontically-treated maxillary premolars: An in vitro study. J. Prosthet. Dent. 2016, 115, 290–295. [Google Scholar] [CrossRef]
- Serin Kalay, T.; Yildirim, T.; Ulker, M. Effects of different cusp coverage restorations on the fracture resistance of endodontically treated maxillary premolars. J. Prosthet. Dent. 2016, 116, 404–410. [Google Scholar] [CrossRef]
- Balkenhol, M.; Wostmann, B.; Rein, C.; Ferger, P. Survival time of cast post and cores: A 10-year retrospective study. J. Dent. 2007, 35, 50–58. [Google Scholar] [CrossRef]
- Fokkinga, W.A.; Kreulen, C.M.; Bronkhorst, E.M.; Creugers, N.H. Up to 17-year controlled clinical study on post-and-cores and covering crowns. J. Dent. 2007, 35, 778–786. [Google Scholar] [CrossRef] [PubMed]
- Jung, R.E.; Kalkstein, O.; Sailer, I.; Roos, M.; Hammerle, C.H. A comparison of composite post buildups and cast gold post-and-core buildups for the restoration of nonvital teeth after 5 to 10 years. Int. J. Prosthodont. 2007, 20, 63–69. [Google Scholar] [PubMed]
- da Costa, R.G.; de Morais, E.C.; Leao, M.P.; Bindo, M.J.; Campos, E.A.; Correr, G.M. Three-year follow up of customized glass fiber esthetic posts. Eur. J. Dent. 2011, 5, 107–112. [Google Scholar] [CrossRef] [Green Version]
- Falcao Spina, D.R.; Goulart da Costa, R.; Farias, I.C.; da Cunha, L.G.; Ritter, A.V.; Gonzaga, C.C.; Correr, G.M. CAD/CAM post-and-core using different esthetic materials: Fracture resistance and bond strengths. Am. J. Dent. 2017, 30, 299–304. [Google Scholar]
- Coelho, C.S.; Biffi, J.C.; Silva, G.R.; Abrahao, A.; Campos, R.E.; Soares, C.J. Finite element analysis of weakened roots restored with composite resin and posts. Dent. Mater. J. 2009, 28, 671–678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maroulakos, G.; Nagy, W.W.; Kontogiorgos, E.D. Fracture resistance of compromised endodontically treated teeth restored with bonded post and cores: An in vitro study. J. Prosthet. Dent. 2015, 114, 390–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Naumann, M.; Blankenstein, F.; Kiessling, S.; Dietrich, T. Risk factors for failure of glass fiber-reinforced composite post restorations: A prospective observational clinical study. Eur. J. Oral Sci. 2005, 113, 519–524. [Google Scholar] [CrossRef]
- Sorrentino, R.; Di Mauro, M.I.; Ferrari, M.; Leone, R.; Zarone, F. Complications of endodontically treated teeth restored with fiber posts and single crowns or fixed dental prostheses-a systematic review. Clin. Oral Investig. 2016, 20, 1449–1457. [Google Scholar] [CrossRef] [Green Version]
- Soares, C.J.; Valdivia, A.D.; da Silva, G.R.; Santana, F.R.; de Souza Menezes, S. Longitudinal clinical evaluation of post systems: A literature review. Braz. Dent. J. 2012, 23, 135–740. [Google Scholar] [CrossRef] [Green Version]
- Lazari, P.C.; de Carvalho, M.A.; Del Bel Cury, A.A.; Magne, P. Survival of extensively damaged endodontically treated incisors restored with different types of posts-and-core foundation restoration material. J. Prosthet. Dent. 2018, 119, 769–776. [Google Scholar] [CrossRef]
- Naumann, M.; Schmitter, M.; Frankenberger, R.; Krastl, G. “Ferrule Comes First. Post Is Second!” Fake News and Alternative Facts? A Systematic Review. J. Endod. 2018, 44, 212–219. [Google Scholar] [CrossRef]
- Torabinejad, M.; Goodacre, C.J. Endodontic or dental implant therapy: The factors affecting treatment planning. J. Am. Dent. Assoc. 2006, 137, 973–977; quiz 1027–1028. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, R.; Bou Serhal, C.; van Steenberghe, D. The stereognostic ability of natural dentitions versus implant-supported fixed prostheses or overdentures. Clin. Oral Investig. 1997, 1, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Dorow, C.; Krstin, N.; Sander, F.G. Experiments to determine the material properties of the periodontal ligament. J. Orofac. Orthop. 2002, 63, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Marchionatti, A.M.E.; Wandscher, V.F.; Rippe, M.P.; Kaizer, O.B.; Valandro, L.F. Clinical performance and failure modes of pulpless teeth restored with posts: A systematic review. Braz. Oral Res. 2017, 31, e64. [Google Scholar] [CrossRef] [Green Version]
- Mancebo, J.C.; Jimenez-Castellanos, E.; Canadas, D. Effect of tooth type and ferrule on the survival of pulpless teeth restored with fiber posts: A 3-year clinical study. Am. J. Dent. 2010, 23, 351–356. [Google Scholar]
- Sarkis-Onofre, R.; Jacinto, R.C.; Boscato, N.; Cenci, M.S.; Pereira-Cenci, T. Cast metal vs. glass fibre posts: A randomized controlled trial with up to 3 years of follow up. J. Dent. 2014, 42, 582–587. [Google Scholar] [CrossRef]
- Garcia, P.P.; Wambier, L.M.; de Geus, J.L.; da Cunha, L.F.; Correr, G.M.; Gonzaga, C.C. Do anterior and posterior teeth treated with post-and-core restorations have similar failure rates? A systematic review and meta-analysis. J. Prosthet. Dent. 2019, 121, 887–894.e884. [Google Scholar] [CrossRef]
- Periodontology, A.A.O. Glossary of Periodontal Terms, 4th ed.; The American Academy of Periodontology: Chicago, IL, USA, 2001. [Google Scholar]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S173–S182. [Google Scholar] [CrossRef] [Green Version]
- Sedghi, L.; DiMassa, V.; Harrington, A.; Lynch, S.V.; Kapila, Y.L. The oral microbiome: Role of key organisms and complex networks in oral health and disease. Periodontol. 2000 2021, 87, 107–131. [Google Scholar] [CrossRef]
- Darveau, R.P.; Curtis, M.A. Oral biofilms revisited: A novel host tissue of bacteriological origin. Periodontol. 2000 2021, 86, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Joseph, S.; Curtis, M.A. Microbial transitions from health to disease. Periodontol. 2000 2021, 86, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Jakubovics, N.S.; Goodman, S.D.; Mashburn-Warren, L.; Stafford, G.P.; Cieplik, F. The dental plaque biofilm matrix. Periodontol. 2000 2021, 86, 32–56. [Google Scholar] [CrossRef] [PubMed]
- Di Benedetto, A.; Gigante, I.; Colucci, S.; Grano, M. Periodontal disease: Linking the primary inflammation to bone loss. Clin. Dev. Immunol. 2013, 2013, 503754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar]
- Machtei, E.E.; Hirsch, I. Retention of hopeless teeth: The effect on the adjacent proximal bone following periodontal surgery. J. Periodontol. 2007, 78, 2246–2252. [Google Scholar] [CrossRef] [Green Version]
- Graetz, C.; Dorfer, C.E.; Kahl, M.; Kocher, T.; Fawzy El-Sayed, K.; Wiebe, J.F.; Gomer, K.; Ruhling, A. Retention of questionable and hopeless teeth in compliant patients treated for aggressive periodontitis. J. Clin. Periodontol. 2011, 38, 707–714. [Google Scholar] [CrossRef] [Green Version]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S.; Participants, E.F.P.W.; Methodological, C. Treatment of stage I-III periodontitis-The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47 (Suppl. 22), 4–60. [Google Scholar] [CrossRef]
- Heasman, P.A.; McCracken, G.I.; Steen, N. Supportive periodontal care: The effect of periodic subgingival debridement compared with supragingival prophylaxis with respect to clinical outcomes. J. Clin. Periodontol. 2002, 29 (Suppl. 3), 163–172; discussion 195–196. [Google Scholar] [CrossRef]
- Supportive periodontal therapy (SPT) for maintaining the dentition in adults treated for periodontitis. J. Periodontol. 1998, 69, 502–506.
- Chambrone, L.A.; Chambrone, L. Tooth loss in well-maintained patients with chronic periodontitis during long-term supportive therapy in Brazil. J. Clin. Periodontol. 2006, 33, 759–764. [Google Scholar] [CrossRef]
- Fardal, O.; Johannessen, A.C.; Linden, G.J. Tooth loss during maintenance following periodontal treatment in a periodontal practice in Norway. J. Clin. Periodontol. 2004, 31, 550–555. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J.; Giordano, J.R.; Soehren, S.; Kaciroti, N. The nonsurgical treatment of patients with periodontal disease: Results after five years. J. Am. Dent. Assoc. 2002, 133, 311–320. [Google Scholar] [CrossRef] [PubMed]
- Wilson, T.G., Jr.; Glover, M.E.; Malik, A.K.; Schoen, J.A.; Dorsett, D. Tooth loss in maintenance patients in a private periodontal practice. J. Periodontol. 1987, 58, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Wood, W.R.; Greco, G.W.; McFall, W.T., Jr. Tooth loss in patients with moderate periodontitis after treatment and long-term maintenance care. J. Periodontol. 1989, 60, 516–520. [Google Scholar] [CrossRef]
- Loos, B.; Nylund, K.; Claffey, N.; Egelberg, J. Clinical effects of root debridement in molar and non-molar teeth. A 2-year follow-up. J. Clin. Periodontol. 1989, 16, 498–504. [Google Scholar] [CrossRef]
- D’Aiuto, F.; Ready, D.; Parkar, M.; Tonetti, M.S. Relative contribution of patient-, tooth-, and site-associated variability on the clinical outcomes of subgingival debridement. I. Probing depths. J. Periodontol. 2005, 76, 398–405. [Google Scholar] [CrossRef]
- Ehnevid, H.; Jansson, L.E. Effects of furcation involvements on periodontal status and healing in adjacent proximal sites. J. Periodontol. 2001, 72, 871–876. [Google Scholar] [CrossRef]
- Kathariya, R.; Devanoorkar, A.; Golani, R.; Shetty, N.; Vallakatla, V.; Bhat, M.Y. To Splint or Not to Splint: The Current Status of Periodontal Splinting. J. Int. Acad. Periodontol. 2016, 18, 45–56. [Google Scholar]
- Graetz, C.; Ostermann, F.; Woeste, S.; Salzer, S.; Dorfer, C.E.; Schwendicke, F. Long-term survival and maintenance efforts of splinted teeth in periodontitis patients. J. Dent. 2019, 80, 49–54. [Google Scholar] [CrossRef]
- Chambrone, L.; Chambrone, D.; Lima, L.A.; Chambrone, L.A. Predictors of tooth loss during long-term periodontal maintenance: A systematic review of observational studies. J. Clin. Periodontol. 2010, 37, 675–684. [Google Scholar] [CrossRef] [PubMed]
- Blatz, M.B.; Chiche, G.; Bahat, O.; Roblee, R.; Coachman, C.; Heymann, H.O. Evolution of Aesthetic Dentistry. J. Dent. Res. 2019, 98, 1294–1304. [Google Scholar] [CrossRef] [PubMed]
- Pjetursson, B.E.; Heimisdottir, K. Dental implants—Are they better than natural teeth? Eur. J. Oral Sci. 2018, 126 (Suppl. 1), 81–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, J.H.; Wang, H.L. Breaking the wave of peri-implantitis. Periodontol. 2000 2020, 84, 145–160. [Google Scholar] [CrossRef]
- Derks, J.; Schaller, D.; Hakansson, J.; Wennstrom, J.L.; Tomasi, C.; Berglundh, T. Effectiveness of Implant Therapy Analyzed in a Swedish Population: Prevalence of Peri-implantitis. J. Dent. Res. 2016, 95, 43–49. [Google Scholar] [CrossRef]
- Pesce, P.; Canullo, L.; Grusovin, M.G.; de Bruyn, H.; Cosyn, J.; Pera, P. Systematic review of some prosthetic risk factors for periimplantitis. J. Prosthet. Dent. 2015, 114, 346–350. [Google Scholar] [CrossRef]
- Sailer, I.; Karasan, D.; Todorovic, A.; Ligoutsikou, M.; Pjetursson, B.E. Prosthetic failures in dental implant therapy. Periodontol. 2000 2022, 88, 130–144. [Google Scholar] [CrossRef]
- Tomasi, C.; Derks, J. Etiology, occurrence, and consequences of implant loss. Periodontol. 2000 2022, 88, 13–35. [Google Scholar] [CrossRef]
- Ramanauskaite, A.; Sader, R. Esthetic complications in implant dentistry. Periodontol. 2000 2022, 88, 73–85. [Google Scholar] [CrossRef]
- Thoma, D.S.; Gil, A.; Hammerle, C.H.F.; Jung, R.E. Management and prevention of soft tissue complications in implant dentistry. Periodontol. 2000 2022, 88, 116–129. [Google Scholar] [CrossRef]
- Kotsakis, G.A.; Olmedo, D.G. Peri-implantitis is not periodontitis: Scientific discoveries shed light on microbiome-biomaterial interactions that may determine disease phenotype. Periodontol. 2000 2021, 86, 231–240. [Google Scholar] [CrossRef]
- Nibali, L.; Gkranias, N.; Mainas, G.; Di Pino, A. Periodontitis and implant complications in diabetes. Periodontol. 2000 2022, 90, 88–105. [Google Scholar] [CrossRef] [PubMed]
- Schliephake, H. The role of systemic diseases and local conditions as risk factors. Periodontol. 2000 2022, 88, 36–51. [Google Scholar] [CrossRef] [PubMed]
- De Backer, H.; Van Maele, G.; De Moor, N.; Van den Berghe, L. Long-term results of short-span versus long-span fixed dental prostheses: An up to 20-year retrospective study. Int. J. Prosthodont. 2008, 21, 75–85. [Google Scholar] [PubMed]
- Strindberg, L. The Dependence of the Results of Pulp Therapy on Certain Factors—An Analytical Study Based on Radiographic and Clinical Follow-up Examination. Acta Odontol. Scand. 1956, 14, 1–175. [Google Scholar]
- Orstavik, D.; Kerekes, K.; Eriksen, H.M. The periapical index: A scoring system for radiographic assessment of apical periodontitis. Endod. Dent. Traumatol. 1986, 2, 20–34. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.; Lang, N.P. Surgical and nonsurgical periodontal therapy. Learned and unlearned concepts. Periodontol. 2000 2013, 62, 218–231. [Google Scholar] [CrossRef]
- Feres, M.; Retamal-Valdes, B.; Faveri, M.; Duarte, P.; Shibli, J.; Soares, G.M.S.; Miranda, T.; Teles, F.; Goodson, M.; Hasturk, H.; et al. Proposal of a Clinical Endpoint for Periodontal Trials: The Treat-to-Target Approach. J. Int. Acad. Periodontol. 2020, 22, 41–53. [Google Scholar]
- Smith, D.E.; Zarb, G.A. Criteria for success of osseointegrated endosseous implants. J. Prosthet. Dent. 1989, 62, 567–572. [Google Scholar] [CrossRef]
- Albrektsson, T.; Zarb, G.; Worthington, P.; Eriksson, A.R. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int. J. Oral Maxillofac. Implant. 1986, 1, 11–25. [Google Scholar]
- Misch, C.E.; Perel, M.L.; Wang, H.L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant success, survival, and failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant. Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatavadekar, N. Helping the clinician make evidence-based implant selections. A systematic review and qualitative analysis of dental implant studies over a 20 year period. Int. Dent. J. 2010, 60, 359–369. [Google Scholar]
- Lindh, T.; Gunne, J.; Tillberg, A.; Molin, M. A meta-analysis of implants in partial edentulism. Clin. Oral Implant. Res. 1998, 9, 80–90. [Google Scholar] [CrossRef] [Green Version]
- Boioli, L.T.; Penaud, J.; Miller, N. A meta-analytic, quantitative assessment of osseointegration establishment and evolution of submerged and non-submerged endosseous titanium oral implants. Clin. Oral Implant. Res. 2001, 12, 579–588. [Google Scholar] [CrossRef] [PubMed]
- Lemos, C.A.; Ferro-Alves, M.L.; Okamoto, R.; Mendonca, M.R.; Pellizzer, E.P. Short dental implants versus standard dental implants placed in the posterior jaws: A systematic review and meta-analysis. J. Dent. 2016, 47, 8–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravida, A.; Wang, I.C.; Barootchi, S.; Askar, H.; Tavelli, L.; Gargallo-Albiol, J.; Wang, H.L. Meta-analysis of randomized clinical trials comparing clinical and patient-reported outcomes between extra-short (</=6 mm) and longer (>/=10 mm) implants. J. Clin. Periodontol. 2019, 46, 118–142. [Google Scholar] [CrossRef] [PubMed]
- Salinas, T.; Eckert, S. Implant-supported single crowns predictably survive to five years with limited complications. J. Evid. Based Dent. Pract. 2012, 12, 213–214. [Google Scholar] [CrossRef]
- Rodrigo, D.; Sanz-Sanchez, I.; Figuero, E.; Llodra, J.C.; Bravo, M.; Caffesse, R.G.; Vallcorba, N.; Guerrero, A.; Herrera, D. Prevalence and risk indicators of peri-implant diseases in Spain. J. Clin. Periodontol. 2018, 45, 1510–1520. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author (Year) | Study Design Follow-Up Time Primary Object of the Study | No. of Participants Gender Dropouts (%) | Age Range Mean Age | No. of Implants Implant System Implant Size (mm) | Dental Prosthesis |
|---|---|---|---|---|---|
| Lekholm et al. (1999) | Prospective 10 years Implant survival | 127 ♂54/♀73 30 | 18–70 50 | 461 NobelBiocare ∅7, 10, 13, 15, 18, 20 × 3.75–4.0 | FPD |
| Carlsson et al. (2000) | Prospective 15 years Bone level alteration | 60 ♂16/♀44 5 | 33–64 NR | 348 NobelBiocare ∅10–NR | FCDP |
| Van Steenberghe et al. (2001) | Retrospective 12 years Bone level alteration | 158 ♂114/♀44 2.5 | 32–82 59.2 | 316 NobelBiocare ∅7, 8, 10, 12, 13, 15, 18, 20 × 3.75, 4.0, 5.0 | IOD |
| Leonhardt et al. (2002) | Prospective 10 years Others | 15 ♂8/♀7 21 | 21–71 NR | 57 NobelBiocare ∅NR | FPD |
| Karoussis et al. (2004) | Prospective 12 years Survival and success | 89 ♂34/♀55 29.9 | 19–79 49.3 | 179 ITI ∅NR | SC/FPD |
| Telleman et al. (2006) | Retrospective 10 years Others | 38 ♂8/♀30 36.6 | 46–90 64 | 115 ITI ∅NR | IOD |
| Jemt and Johansson (2006) | Retrospective 15 years Others | 76 ♂48/♀28 56.6 | 32–76 61.1 | 450 NobelBiocare ∅7, 10, 13, 15, 18 × NR | FCDP |
| Romeo et al. (2006) | Retrospective 14 years Others | 129 ♂61/♀68 17.8 | NR 53 | 265 ITI ∅8, 10 × 3.75, 4.1, 4.8 | SC/FPD |
| Åstrand et al. (2008) | Retrospective 20 years Implant survival | 21 ♂7/♀14 56.2 | 40–74 54.3 | 123 NobelBiocare ∅NR | FCDP |
| Jemt (2008) | RCT 15 years Others | 114 ♂74/♀40 44 | NR 42.7 | 123 NobelBiocare ∅NR | SC |
| Pikner et al. (2009) | Retrospective 20 years Bone level alteration | 640 ♂255/♀385 NR | 18–83 52.3 | 3.462 NobelBiocare ∅NR | SC/FPD/FCDP |
| Simonis et al. (2010) | Retrospective 16 years Survival and success | 55 ♂21/♀34 28 | 29–88 68.7 | 131 ITI ∅6, 8, 10, 12 × NR | SC/FPD |
| Jacobs et al. (2010) | RCT 16 years Others | 18 ♂6/♀12 33.3 | 32–75 55.1 | 95 NobelBiocare/Astra Tech ∅7, 8, 9, 10, 11, 13, 15, 18, 19 × 3.75, 4.0 | FPD |
| Ma et al. (2010) | RCT 10 years Bone level alteration | 106 ♂40/♀66 25.4 | NR 65.3 | 212 NobelBiocare/Southern Implants/Steri-Oss ∅NR | IOD |
| Mertens et al. (2012) | Prospective 10 years Others | 14 ♂3/♀11 14.2 | 37–71 57.9 | 52 Astra Tech ∅8, 9 × 3.5, 4.0, 4.5 | SC/FPD/FCDP |
| Lops et al. (2012) | Retrospective 20 years Others | 121 ♂57/♀64 24.7 | 22–69 54 | 257 ITI ∅8, 10 × 3.75, 4.1, 4.8 | SC/FPD/FCDP |
| Gotfredsen (2012) | Prospective 10 years Others | 20 ♂10/♀10 5 | 18–59 33 | 20 Astra Tech ∅11, 13, 15 × 4.5 | SC |
| Degidi et al. (2012) | Prospective 10 years Others | 48 ♂21/♀27 18.6 | NR 49.9 | 158 NobelBiocare ∅10 to 15 × 3.3, 3.75, 4.0 | SC/FPD/FCDP |
| Deporter et al. (2012) | Prospective 10 years Survival and success | 24 ♂8/♀16 20.8 | 20–72 NR | 48 Sybron Implants Solution ∅7, 9 × 4.1 | SC/FPD |
| Deporter et al. (2014) | Prospective 20 years Others | 52 ♂17/♀35 32.7 | NR 55.3 | 156 Sybron Implants Solution ∅7, 8, 9, 10 × NR | IOD |
| Ravald et al. (2013) | RCT 15 years Implant survival | 46 ♂27/♀19 25.3 | 51–88 74.4 | 371 Astra Tech/NobelBiocare ∅9 to 19 × 3.5, 3.75, 4.0 | FCDP |
| Rocci et al. (2012) | Retrospective 10 years Others | 46 ♂26/♀20 NR | 24–77 51 | 97 NobelBiocare ∅8.5 to 18 × NR | SC/FPD |
| Mangano et al. (2014) | Prospective 10 years Others | 194 ♂104/♀90 25.7 | 24–74 49.1 | 215 Leone Implant System ∅8 × 3.3, 4.1, 4.8 | SC |
| Adler et al. (2019) | Retrospective 11 years Implant survival | 376 ♂207/♀169 NR | 20–81 54 | 1095 Astra Tech/NobelBiocare/Straumann ∅ < 10 and ≥10 × NR | SC/FPD/FCDP |
| Author (Year) | MPS (mm) | MPOM (mm) | Success Rate (%) Criterion of Success | Survival Rate (%) |
|---|---|---|---|---|
| Lekholm et al. (1999) | NR | 0.7 | NR Albrektsson et al. (1986) | 92.6 |
| Carlsson et al. (2000) | NR | 0.5 | 99 Albrektsson et al. (1986) | 96 |
| Van Steenberghe et al. (2001) | NR | 2.67 | 97.2 Albrektsson et al. (1986) | 98.5 |
| Leonhardt et al. (2002) | 1.9 | 1.7 | NR | 94.7 |
| Karoussis et al. (2004) | 2.87 | 0.98 | 85.5 Karoussis et al. (2003) | 92.4 |
| Telleman et al. (2006) | 3.3 | 2.2 | 92.2 Albrektsson et al. (1986) | 96.3 |
| Jemt and Johansson (2006) | NR | 2.1 | 86.8 Albrektsson et al. (1986) | 90.9 |
| Romeo et al. (2006) | 2.2 | 1.65 | NR Zarb and Albrektsson (1998) Roos et al. (1997) | 97.5 |
| Åstrand et al. (2008) | 3.4 | 2.33 | NR | 99.2 |
| Jemt (2008) | NR | 2 | NR Albrektsson and Isidor (1993) | 97.7 |
| Pikner et al. (2009) | NR | 2.5 | NR | 98.2 |
| Simonis et al. (2010) | 2.73 | 2.25 | 51.9 Simonis et al. (2010) | 83.7 |
| Jacobs et al. (2010) | 2.55 | 0.16 | 98.8 NR * | 93.9 |
| Ma et al. (2010) | NR | 0.29 | 100 Albrektsson and Isidor (1993) Roos et al. (1997) | 100 |
| Mertens et al. (2012) | 3.26 | 0.3 | 100 Albrektsson et al. (1986) | 100 |
| Lops et al. (2012) | 2.2 | 1.85 | 79.8 Albrektsson et al. (1986) Roos et al. (1997) | 94.1 |
| Gotfredsen (2012) | NR | 0.75 | NR Albrektsson and Isidor (1993) | 100 |
| Degidi et al. (2012) | 2.54 | 1.95 | 34.9 Misch et al. (2008) | 97.2 |
| Deporter et al. (2012) | NR | 1.21 | 95.5 NR * | 95.5 |
| Deporter et al. (2014) | NR | 0.67 | 73.4 Albrektsson et al. (1986) | 73.4 |
| Ravald et al. (2013) | 3.93 | 0.55 | NR | 95.1 |
| Rocci et al. (2012) | NR | 0.1 | NR | 91.1 |
| Mangano et al. (2014) | NR | 0.62 | 95.9 Zarb and Albrektsson (1998) | 98.5 |
| Adler et al. (2019) | NR | NR | NR | 82.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sartoretto, S.C.; Shibli, J.A.; Javid, K.; Cotrim, K.; Canabarro, A.; Louro, R.S.; Lowenstein, A.; Mourão, C.F.; Moraschini, V. Comparing the Long-Term Success Rates of Tooth Preservation and Dental Implants: A Critical Review. J. Funct. Biomater. 2023, 14, 142. https://doi.org/10.3390/jfb14030142
Sartoretto SC, Shibli JA, Javid K, Cotrim K, Canabarro A, Louro RS, Lowenstein A, Mourão CF, Moraschini V. Comparing the Long-Term Success Rates of Tooth Preservation and Dental Implants: A Critical Review. Journal of Functional Biomaterials. 2023; 14(3):142. https://doi.org/10.3390/jfb14030142
Chicago/Turabian StyleSartoretto, Suelen Cristina, Jamil Awad Shibli, Kayvon Javid, Khalila Cotrim, Antonio Canabarro, Rafael Seabra Louro, Adam Lowenstein, Carlos Fernando Mourão, and Vittorio Moraschini. 2023. "Comparing the Long-Term Success Rates of Tooth Preservation and Dental Implants: A Critical Review" Journal of Functional Biomaterials 14, no. 3: 142. https://doi.org/10.3390/jfb14030142