
Immediate and Long-Term Effects of Hyperbaric Oxygenation in Patients with Long COVID-19 Syndrome Using SF-36 Survey and VAS Score: A Clinical Pilot Study
 , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Background
1.2. Hypothesis and Objectives
2. Materials and Methods
2.1. Study Design
2.2. Patient Characteristics
2.3. HBO Treatment
2.4. Patient Evaluation
2.5. Statistical Analysis
3. Results
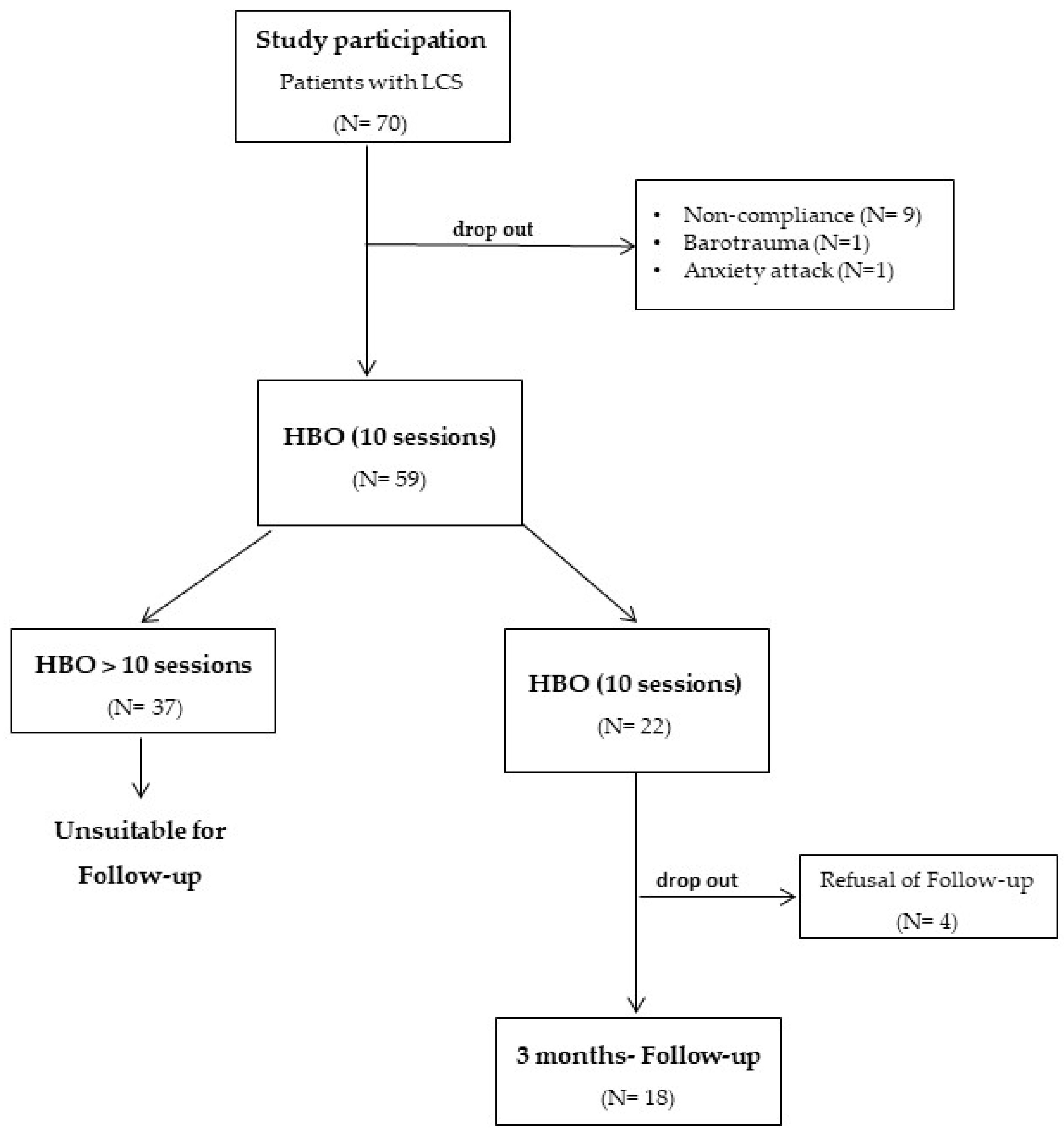
3.1. Study Population
3.2. Severity of COVID-19 Infection
3.3. Biometrical Data and Co-Morbidity
3.4. Collective of Patients Finishing HBO Treatment (10 Sessions) without Follow-Up
3.5. Collective of Patients Finishing HBO Treatment (10 Sessions) without Follow-Up
3.6. Collective of Patients Finishing HBO Treatment (10 Sessions) with Follow-Up
3.7. Collective of Patients Exceeding 10 HBO Sessions without Follow-Up
3.8. Side Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yong, S.J. Long COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors, and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef] [PubMed]
- Wulf Hanson, S.; Abbafati, C.; Aerts, J.G.; Al-Aly, Z.; Ashbaugh, C.; Ballouz, T.; Blyuss, O.; Bobkova, P.; Bonsel, G.; Borzakova, S.; et al. Estimated Global Proportions of Individuals with Persistent Fatigue, Cognitive, and Respiratory Symptom Clusters Following Symptomatic COVID-19 in 2020 and 2021. JAMA 2022, 328, 1604–1615. [Google Scholar] [PubMed]
- Aiyegbusi, O.L.; Hughes, S.E.; Turner, G.; Rivera, S.C.; McMullan, C.; Chandan, J.S.; Haroon, S.; Price, G.; Davies, E.H.; Nirantharakumar, K.; et al. Symptoms, complications and management of long COVID: A review. J. R. Soc. Med. 2021, 114, 428–442. [Google Scholar] [CrossRef] [PubMed]
- Joli, J.; Buck, P.; Zipfel, S.; Stengel, A. Post-COVID-19 fatigue: A systematic review. Front. Psychiatry 2022, 13, 947973. [Google Scholar] [CrossRef]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; Maertens de Noordhout, C.; Primus-de Jong, C.; Cleemput, I.; Van den Heede, K. Pathophysiology and mechanism of long COVID: A comprehensive review. Ann. Med. 2022, 54, 1473–1487. [Google Scholar] [CrossRef]
- Lindenmann, J.; Smolle, C.; Kamolz, L.P.; Smolle-Juettner, F.M.; Graier, W.F. Survey of Molecular Mechanisms of Hyperbaric Oxygen in Tissue Repair. Int. J. Mol. Sci. 2021, 22, 11754. [Google Scholar] [CrossRef]
- Guo, D.; Pan, S.; Wang, M.; Guo, Y. Hyperbaric oxygen therapy may be effective to improve hypoxemia in patients with severe COVID-2019 pneumonia: Two case reports. Undersea Hyperb. Med. 2020, 47, 181–187. [Google Scholar] [CrossRef]
- Thibodeaux, K.; Speyrer, M.; Raza, A.; Yaakov, R.; Serena, T.E. Hyperbaric oxygen therapy in preventing mechanical ventilation in COVID-19 patients: A retrospective case series. J. Wound Care 2020, 29, S4–S8. [Google Scholar] [CrossRef]
- Cannellotto, M.; Duarte, M.; Keller, G.; Larrea, R.; Cunto, E.; Chediack, V.; Mansur, M.; Brito, D.M.; García, E.; Di Salvo, H.E.; et al. Hyperbaric oxygen as an adjuvant treatment for patients with COVID-19 severe hypoxaemia: A randomised controlled trial. Emerg. Med. J. 2022, 39, 88–93. [Google Scholar] [CrossRef]
- Gorenstein, S.A.; Castellano, M.L.; Slone, E.S.; Gillette, B.; Liu, H.; Alsamarraie, C.; Jacobson, A.M.; Wall, S.P.; Adhikari, S.; Swartz, J.L.; et al. Hyperbaric oxygen therapy for COVID-19 patients with respiratory distress: Treated cases versus propensity-matched controls. Undersea Hyperb. Med. 2020, 47, 405–413. [Google Scholar] [CrossRef]
- Jansen, D.; Dickstein, D.R.; Erazo, K.; Stacom, E.; Lee, D.C.; Wainwright, S.K. Hyperbaric oxygen for COVID-19 patients with severe hypoxia prior to vaccine availability. Undersea Hyperb. Med. 2022, 49, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Bhaiyat, A.M.; Sasson, E.; Wang, Z.; Khairy, S.; Ginzarly, M.; Qureshi, U.; Fikree, M.; Efrati, S. Hyperbaric oxygen treatment for long coronavirus disease-19: A case report. J. Med. Case Rep. 2022, 16, 80. [Google Scholar] [CrossRef] [PubMed]
- Zant, A.E.; Figueroa, X.A.; Paulson, C.P.; Wright, J.K. Hyperbaric oxygen therapy to treat lingering COVID-19 symptoms. Undersea Hyperb. Med. 2022, 49, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Robbins, T.; Gonevski, M.; Clark, C.; Baitule, S.; Sharma, K.; Magar, A.; Patel, K.; Sankar, S.; Kyrou, I.; Ali, A.; et al. Hyperbaric oxygen therapy for the treatment of long COVID: Early evaluation of a highly promising intervention. Clin. Med. 2021, 21, e629–e632. [Google Scholar] [CrossRef]
- Turova, E.A.; Shchikota, A.M.; Pogonchenkova, I.V.; Golovach, A.V.; Tagirova, D.I.; Gusakova, E.V. Hyperbaric oxygenation in outpatient rehabilitation of COVID-19 convalescents. Vopr. Kurortol. Fizioter. Lech. Fiz. Kult. 2021, 98, 16–21. [Google Scholar] [CrossRef]
- Zilberman-Itskovich, S.; Catalogna, M.; Sasson, E.; Elman-Shina, K.; Hadanny, A.; Lang, E.; Finci, S.; Polak, N.; Fishlev, G.; Korin, C.; et al. Hyperbaric oxygen therapy improves neurocognitive functions and symptoms of post-COVID condition: Randomized controlled trial. Sci. Rep. 2022, 12, 11252. [Google Scholar] [CrossRef]
- Catalogna, M.; Sasson, E.; Hadanny, A.; Parag, Y.; Zilberman-Itskovich, S.; Efrati, S. Effects of hyperbaric oxygen therapy on functional and structural connectivity in post-COVID-19 condition patients: A randomized, sham-controlled trial. Neuroimage Clin. 2022, 36, 103218. [Google Scholar] [CrossRef]
- Hussain, R.; Wark, S.; Dillon, G.; Ryan, P. Self-reported physical and mental health of Australian carers: A cross-sectional study. BMJ Open 2016, 6, e011417. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Lins, L.; Carvalho, F.M. SF-36 total score as a single measure of health-related quality of life: Scoping review. SAGE Open Med. 2016, 4, 2050312116671725. [Google Scholar] [CrossRef]
- Poudel, A.N.; Zhu, S.; Cooper, N.; Roderick, P.; Alwan, N.; Tarrant, C.; Ziauddeen, N.; Yao, G.L. Impact of Covid-19 on health-related quality of life of patients: A structured review. PLoS ONE 2021, 16, e0259164. [Google Scholar] [CrossRef]
- Weigl, K.; Forstner, T. Design of Paper-Based Visual Analogue Scale Items. Educ. Psychol. Meas. 2021, 81, 595–611. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Mathieu, D.; Marroni, A.; Kot, J. Tenth European Consensus Conference on Hyperbaric Medicine: Recommendations for accepted and non-accepted clinical indications and practic of hyperbaric oxygten treatment. Diving Hyperb. Med. 2017, 47, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Manganotti, P.; Michelutti, M.; Furlanis, G.; Deodato, M.; Buoite Stella, A. Deficient GABABergic and glutamatergic excitability in the motor cortex of patients with long-COVID and cognitive impairment. Clin. Neurophysiol. 2023, 151, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Ortelli, P.; Ferrazzoli, D.; Sebastianelli, L.; Maestri, R.; Dezi, S.; Spampinato, D.; Saltuari, L.; Alibardi, A.; Engl, M.; Kofler, M.; et al. Altered motor cortex physiology and dysexecutive syndrome in patients with fatigue and cognitive difficulties after mild COVID-19. Eur. J. Neurol. 2022, 29, 1652–1662. [Google Scholar] [CrossRef] [PubMed]
- Ajčević, M.; Iscra, K.; Furlanis, G.; Michelutti, M.; Miladinović, A.; Buoite Stella, A.; Ukmar, M.; Cova, M.A.; Accardo, A.; Manganotti, P. Cerebral hypoperfusion in post-COVID-19 cognitively impaired subjects revealed by arterial spin labeling MRI. Sci. Rep. 2023, 13, 5808. [Google Scholar] [CrossRef]
- Guedj, E.; Campion, J.Y.; Dudouet, P.; Kaphan, E.; Bregeon, F.; Tissot-Dupont, H.; Guis, S.; Barthelemy, F.; Habert, P.; Ceccaldi, M.; et al. 18F-FDG brain PET hypometabolism in patients with long COVID. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2823–2833. [Google Scholar] [CrossRef]
- Rosenberg, K. Hyperbaric Oxygen Improves Neurocognitive Function and Symptoms of Post-COVID Condition. Am. J. Nurs. 2022, 122, 61–62. [Google Scholar] [CrossRef]
- Nopp, S.; Moik, F.; Klok, F.A.; Gattinger, D.; Petrovic, M.; Vonbank, K.; Koczulla, A.R.; Ay, C.; Zwick, R.H. Outpatient Pulmonary Rehabilitation in Patients with Long COVID Improves Exercise Capacity, Functional Status, Dyspnea, Fatigue, and Quality of Life. Respiration 2022, 101, 593–601. [Google Scholar] [CrossRef]
- Raman, B.; Bluemke, D.A.; Lüscher, T.F.; Neubauer, S. Long COVID: Post-acute sequelae of COVID-19 with a cardiovascular focus. Eur. Heart J. 2022, 43, 1157–1172. [Google Scholar] [CrossRef] [PubMed]
- Choutka, J.; Jansari, V.; Hornig, M.; Iwasaki, A. Unexplained post-acute infection syndromes. Nat. Med. 2022, 28, 911–923. [Google Scholar] [CrossRef] [PubMed]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol. Sci. 2022, 434, 120162. [Google Scholar] [CrossRef]
- Shanthanna, H.; Nelson, A.M.; Kissoon, N.; Narouze, S. The COVID-19 pandemic and its consequences for chronic pain: A narrative review. Anaesthesia 2022, 77, 1039–1050. [Google Scholar] [CrossRef] [PubMed]
- Hadanny, A.; Bechor, Y.; Catalogna, M.; Daphna-Tekoah, S.; Sigal, T.; Cohenpour, M.; Lev-Wiesel, R.; Efrati, S. Hyperbaric Oxygen Therapy Can Induce Neuroplasticity and Significant Clinical Improvement in Patients Suffering from Fibromyalgia with a History of Childhood Sexual Abuse-Randomized Controlled Trial. Front. Psychol. 2018, 9, 2495. [Google Scholar] [CrossRef]
- Curtis, K.; Katz, J.; Djaiani, C.; O’Leary, G.; Uehling, J.; Carroll, J.; Santa Mina, D.; Clarke, H.; Gofeld, M.; Katznelson, R. Evaluation of a Hyperbaric Oxygen Therapy Intervention in Individuals with Fibromyalgia. Pain. Med. 2021, 22, 1324–1332. [Google Scholar] [CrossRef]
- Leitman, M.; Fuchs, S.; Tyomkin, V.; Hadanny, A.; Zilberman-Itskovich, S.; Efrati, S. The effect of hyperbaric oxygen therapy on myocardial function in post-COVID-19 syndrome patients: A randomized controlled trial. Sci. Rep. 2023, 13, 9473. [Google Scholar] [CrossRef]


{kind=link}
| Pre-HBO (N = 59) | Post-HBO (N = 59) | p Compared with Pre | |
|---|---|---|---|
| Mean systolic blood pressure (mm Hg) | 131.9 +/− 20.0 | 130.6 +/− 15.8 | 0.46 |
| Mean diastolic blood pressure (mm Hg) | 81.3 +/− 12.1 | 79.3 +/− 10.2 | 0.09 |
| Mean heart rate (bpm) | 80.3 +/− 12.9 | 76.8 +/− 11.4 | 0.03 |
| Peripheral oxygen saturation (%) | 96.0 +/− 1.5 | 96.2 +/− 1.5 | 0.35 |
| Physical functioning | 43.9 +/− 24.6 | 52.4 +/− 24.6 | <0.001 |
| Physical role | 10+/− 27.4 | 16.8 +/− 30.4 | 0.01 (0.02) |
| Energy | 22.3 +/− 20.2 | 30.4 +/− 20.4 | <0.001 (<0.001) |
| Emotional role | 45.0 +/− 48.1 | 51.2 +/− 46.5 | 0.26 |
| Emotional well-being | 54.0 +/− 18.5 | 64.0 +/− 18 | <0.001 |
| Social functioning | 32.6 +/− 26.6 | 43.7 +/− 25.9 | <0.001 |
| Pain | 42.7 +/− 25.0 | 50.1 +/− 22.1 | 0.01 |
| General perception of health | 39.5 +/− 16.8 | 42.9 +/− 16.3 | 0.07 |
| Limitation of activities | 12.8 +/− 5.5 | 9.4 +/− 7.9 | <0.001 |
| VAS score | 5.85 +/− 2.01 | 3.79 +/− 2.11 | <0.001 |
| Pre-HBO (N = 22) | Post-HBO (N = 22) | p Compared with Pre | Pre-HBO (N = 18) | After 3 Months (N = 18) | p Compared with Pre | |
|---|---|---|---|---|---|---|
| Mean systolic blood pressure (mm Hg) | 135.3 +/− 23.8 | 131.5 +/− 15.6 | 0.25 | 141.4 +/− 24.1 | 131.3 +/− 11.8 | 0.06 |
| Mean diastolic blood pressure (mm Hg) | 82.8 +/− 10.9 | 82.5 +/− 10.3 | 0.79 | 86.1 +/− 10.9 | 81.4 +/− 8.9 | 0.09 |
| Mean heart rate (bpm) | 82.2 +/− 12.7 | 80.7 +/− 12.4 | 0.47 | 81.9 +/− 13.0 | 80.1 +/− 10.4 | 0.45 |
| Peripheral oxygen saturation (%) | 96.0 +/− 1.4 | 95.7 +/− 1.5 | 0.38 | 96.1 +/− 1.7 | 96.7 +/− 1.7 | 0.41 |
| Physical functioning | 46.8 +/− 25.6 | 57.3 +/− 26.4 | <0.001 | 44.1 +/− 26.7 | 58.3 +/− 24.7 | <0.001 |
| Physical role | 14.4 +/− 32.6 | 21.0 +/− 35.6 | 0.14 (0.25) | 16.1 +/− 34.7 | 30.9 +/− 41.9 | 0.07 (0.13) |
| Energy | 26.8 +/− 25.1 | 36.5 +/− 20.9 | 0.02 (0.01) | 30.8 +/− 26.0 | 38.0 +/− 25.9 | 0.15 (0.13) |
| Emotional role | 41.6 +/− 48.2 | 50 +/− 48.9 | 0.06 | 42.6 +/− 49.6 | 50.0 +/− 46.1 | 0.16 |
| Emotional well-being | 54.1 +/− 22.4 | 61.4 +/− 21.1 | 0.07 | 58.3 +/− 46.7 | 64.4 +/− 24.5 | 0.09 |
| Social functioning | 38.1 +/− 31.2 | 48.1 +/− 29.3 | 0.02 | 39.6 +/− 32.7 | 60.4 +/− 32.4 | <0.001 |
| Pain | 49.3 +/− 28.1 | 53.5 +/− 24.0 | 0.42 | 52.9 +/− 28.2 | 58.2 +/− 30.2 | 0.17 |
| General perception of health | 38.3 +/− 20.7 | 42.7 +/− 20.3 | 0.17 | 43.2 +/− 19.6 | 46.2 +/− 23.9 | 0.49 |
| Limitation of activities | 13.0 +/− 6.9 | 9.2 +/− 5.7 | <0.001 | 12.2 +/− 7.1 | 9.2 +/− 6.8 | 0.02 |
| VAS score | 5.5 +/− 2.3 | 3.3 +/− 2.4 | <0.001 | 5.2 +/− 2.3 | 2.6 +/− 1.9 | <0.001 |
| Pre-HBO (N = 37) | Post-HBO (N = 37) | p Compared with Pre | |
|---|---|---|---|
| Mean systolic blood pressure (mm Hg) | 129.9 +/− 17.3 | 130.1 +/− 16.1 | 0.94 |
| Mean diastolic blood pressure (mm Hg) | 80.4 +/− 12.8 | 77.4 +/− 9.8 | 0.08 |
| Mean heart rate (bpm) | 79.2 +/− 13.1 | 74.4 +/− 10.2 | 0.04 |
| Peripheral oxygen saturation (%) | 96.1 +/− 1.5 | 96.6 +/− 1.5 | 0.09 |
| Physical functioning | 42.2 +/− 24.2 | 49.5 +/− 23.3 | <0.001 |
| Physical role | 7.6 +/− 24.5 | 14.6 +/− 27.6 | 0.05 (0.05) |
| Energy | 19.8 +/− 16.8 | 27.1 +/− 19.7 | <0.001 (<0.001) |
| Emotional role | 47.0 +/− 48.6 | 51.9 +/− 45.8 | 0.56 |
| Emotional well-being | 54.0 +/− 16.3 | 65.6 +/− 15.9 | <0.001 |
| Social functioning | 29.4 +/− 23.4 | 41.2 +/− 23.7 | <0.001 |
| Pain | 38.9 +/− 22.6 | 48.2 +/− 21.1 | <0.001 |
| General perception of health | 40.1 +/− 14.7 | 43 +/− 14.1 | 0.22 |
| Limitation of activities | 12.6 +/− 4.6 | 9.6 +/− 5.7 | <0.001 |
| VAS score | 6.06 +/− 1.84 | 4.08 +/− 1.9 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lindenmann, J.; Porubsky, C.; Okresa, L.; Klemen, H.; Mykoliuk, I.; Roj, A.; Koutp, A.; Kink, E.; Iberer, F.; Kovacs, G.; et al. Immediate and Long-Term Effects of Hyperbaric Oxygenation in Patients with Long COVID-19 Syndrome Using SF-36 Survey and VAS Score: A Clinical Pilot Study. J. Clin. Med. 2023, 12, 6253. https://doi.org/10.3390/jcm12196253
Lindenmann J, Porubsky C, Okresa L, Klemen H, Mykoliuk I, Roj A, Koutp A, Kink E, Iberer F, Kovacs G, et al. Immediate and Long-Term Effects of Hyperbaric Oxygenation in Patients with Long COVID-19 Syndrome Using SF-36 Survey and VAS Score: A Clinical Pilot Study. Journal of Clinical Medicine. 2023; 12(19):6253. https://doi.org/10.3390/jcm12196253
Chicago/Turabian StyleLindenmann, Joerg, Christian Porubsky, Lucija Okresa, Huberta Klemen, Iurii Mykoliuk, Andrej Roj, Amir Koutp, Eveline Kink, Florian Iberer, Gabor Kovacs, and et al. 2023. "Immediate and Long-Term Effects of Hyperbaric Oxygenation in Patients with Long COVID-19 Syndrome Using SF-36 Survey and VAS Score: A Clinical Pilot Study" Journal of Clinical Medicine 12, no. 19: 6253. https://doi.org/10.3390/jcm12196253