
Influence of Clinical and Sociodemographic Variables on Health-Related Quality of Life in the Adult Population with Long COVID

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
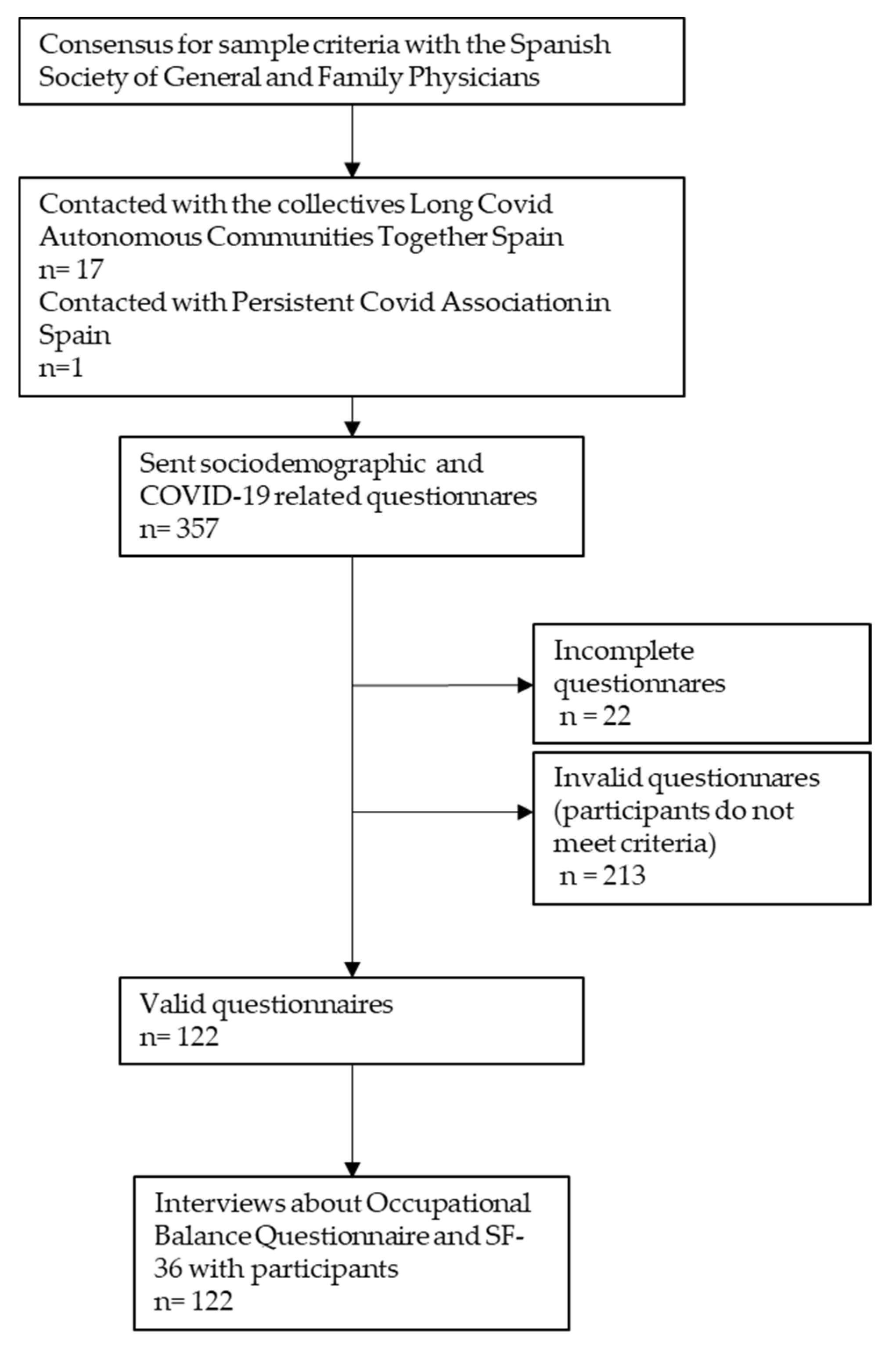
2.2. Sample
2.3. Procedure
2.4. Measures
2.5. Data Analysis
3. Results
4. Discussion
Practical Implications and Future Lines of Investigation
5. Strengths and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mehandru, S.; Merad, M. Pathological sequelae of long-haul COVID. Nat. Immunol. 2022, 23, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. COVID-19: What Do We Know about “Long COVID”? BMJ 2020, 370, m2815. [Google Scholar] [CrossRef] [PubMed]
- Cirulli, E.T.; Barrett, K.M.S.; Riffle, S.; Bolze, A.; Neveux, I.; Dabe, S.; Grzymski, J.J.; Lu, J.T.; Washington, N.L. Long-Term COVID-19 Symptoms in a Large Unselected Population. medRxiv 2020. [Google Scholar] [CrossRef]
- Sadat Larijani, M.; Ashrafian, F.; Bagheri Amiri, F.; Banifazl, M.; Bavand, A.; Karami, A.; Asgari Shokooh, F.; Ramezani, A. Characterization of long COVID-19 manifestations and its associated factors: A prospective cohort study from Iran. Microb. Pathog. 2022, 169, 105618. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of Post-Acute COVID-19 in Primary Care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Yong, S.J. Long COVID or Post-COVID-19 Syndrome: Putative Pathophysiology, Risk Factors, and Treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.; Ni, Z.; Hu, Y.; Liang, W.; Ou, C.; He, J.; Liu, L.; Shan, H.; Lei, C.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Moldofsky, H.; Patcai, J. Chronic Widespread Musculoskeletal Pain, Fatigue, Depression and Disordered Sleep in Chronic Post-SARS Syndrome; a Case-Controlled Study. BMC Neurol. 2011, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- Notarte, K.I.; de Oliveira, M.H.S.; Peligro, P.J.; Velasco, J.V.; Macaranas, I.; Ver, A.T.; Pangilinan, F.C.; Pastrana, A.; Goldrich, N.; Kavteladze, D.; et al. Age, Sex and Previous Comorbidities as Risk Factors Not Associated with SARS-CoV-2 Infection for Long COVID-19: A Systematic Review and Meta-Analysis. J. Clin. Med. 2022, 11, 7314. [Google Scholar] [CrossRef]
- Guo, L.; Lin, J.; Ying, W.; Zheng, C.; Tao, L.; Ying, B.; Cheng, B.; Jin, S.; Hu, B. Correlation Study of Short-Term Mental Health in Patients Discharged After Coronavirus Disease 2019 (COVID-19) Infection without Comorbidities: A Prospective Study. Neuropsychiatr. Dis. Treat. 2020, 16, 2661–2667. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Boon, G.J.A.M.; Barco, S.; Endres, M.; Geelhoed, J.J.M.; Knauss, S.; Rezek, S.A.; Spruit, M.A.; Vehreschild, J.; Siegerink, B. The Post-COVID-19 Functional Status Scale: A Tool to Measure Functional Status over Time after COVID-19. Eur. Respir. J. 2020, 56, 2001494. [Google Scholar] [CrossRef]
- Carfì, A.; Bernabei, R.; Landi, F. Persistent Symptoms in Patients After Acute COVID-19. JAMA 2020, 324, 603. [Google Scholar] [CrossRef] [PubMed]
- Neufeld, K.J.; Leoutsakos, J.-M.S.; Yan, H.; Lin, S.; Zabinski, J.S.; Dinglas, V.D.; Hosey, M.M.; Parker, A.M.; Hopkins, R.O.; Needham, D.M. Fatigue Symptoms During the First Year Following ARDS. Chest 2020, 158, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Wagman, P.; Håkansson, C. Introducing the Occupational Balance Questionnaire (OBQ). Scand. J. Occup. Ther. 2014, 21, 227–231. [Google Scholar] [CrossRef]
- Backman, C.L. Occupational Balance: Exploring the Relationships among Daily Occupations and Their Influence on Well-Being. Can. J. Occup. Ther. 2004, 71, 202–209. [Google Scholar] [CrossRef]
- Jandhyala, R. Design, Validation and Implementation of the Post-Acute (Long) COVID-19 Quality of Life (PAC-19QoL) Instrument. Health Qual. Life Outcomes 2021, 19, 229. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-las-Peñas, C.; Notarte, K.I.; Peligro, P.J.; Velasco, J.V.; Ocampo, M.J.; Henry, B.M.; Arendt-Nielsen, L.; Torres-Macho, J.; Plaza-Manzano, G. Long-COVID Symptoms in Individuals Infected with Different SARS-CoV-2 Variants of Concern: A Systematic Review of the Literature. Viruses 2022, 14, 2629. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-Year Outcomes in Hospital Survivors with COVID-19: A Longitudinal Cohort Study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Rodríguez-Pérez, M.P.; Sánchez-Herrera-Baeza, P.; Rodríguez-Ledo, P.; Serrada-Tejeda, S.; García-Bravo, C.; Pérez-de-Heredia-Torres, M. Headaches and Dizziness as Disabling, Persistent Symptoms in Patients with Long COVID—A National Multicentre Study. J. Clin. Med. 2022, 11, 5904. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association Declaration of Helsinki. JAMA 2013, 310, 2191. [CrossRef] [PubMed] [Green Version]
- Graham, E.L.; Clark, J.R.; Orban, Z.S.; Lim, P.H.; Szymanski, A.L.; Taylor, C.; DiBiase, R.M.; Jia, D.T.; Balabanov, R.; Ho, S.U.; et al. Persistent Neurologic Symptoms and Cognitive Dysfunction in Non-hospitalized COVID-19 “Long Haulers”. Ann. Clin. Transl. Neurol. 2021, 8, 1073–1085. [Google Scholar] [CrossRef] [PubMed]
- Håkansson, C.; Wagman, P.; Hagell, P. Construct Validity of a Revised Version of the Occupational Balance Questionnaire. Scand. J. Occup. Ther. 2020, 27, 441–449. [Google Scholar] [CrossRef]
- Peral-Gómez, P.; López-Roig, S.; Pastor-Mira, M.Á.; Abad-Navarro, E.; Valera-Gran, D.; Håkansson, C.; Wagman, P. Cultural Adaptation and Psychometric Properties of the Spanish Version of the Occupational Balance Questionnaire: An Instrument for Occupation-Based Research. Int. J. Environ. Res. Public Health 2021, 18, 7506. [Google Scholar] [CrossRef]
- Brazier, J.E.; Harper, R.; Jones, N.M.; O’Cathain, A.; Thomas, K.J.; Usherwood, T.; Westlake, L. Validating the SF-36 Health Survey Questionnaire: New Outcome Measure for Primary Care. BMJ 1992, 305, 160–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, G.D.; Hockey, R.; Dobson, A.J. A comparison of SF-36 summary measures of physical and mental health for women across the life course. Qual. Life Res. 2014, 23, 1515–1521. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Kosinski, M.; Keller, S.D. SF-36 Physical and Mental Health Summary Scales: A Manual for Users of Version 1, 2nd ed.; Quality Metric Incorporated: Lincoln, RI, USA, 2005. [Google Scholar]
- Alonso, J.; Prieto, L.; Antó, J.M. Adaptación Versión Española de SF-36v2TM Health Survey©. Med. Clin. 1995, 104, 771–776. [Google Scholar]
- Arnold, D.T.; Hamilton, F.W.; Milne, A.; Morley, A.J.; Viner, J.; Attwood, M.; Noel, A.; Gunning, S.; Hatrick, J.; Hamilton, S.; et al. Patient Outcomes after Hospitalisation with COVID-19 and Implications for Follow-up: Results from a Prospective UK Cohort. Thorax 2021, 76, 399–401. [Google Scholar] [CrossRef]
- Taft, C.; Karlsson, J.; Sullivan, M. Do SF-36 summary component scores accurately summarize subscale scores? Qual. Life Res. 2001, 10, 395–404. [Google Scholar] [CrossRef]
- Mills, S.D.; Fox, R.S.; Bohan, S.; Roesch, S.C.; Sadler, G.R.; Malcarne, V.L. Psychosocial and Neighborhood Correlates of Health-Related Quality of Life: A Multi-Level Study among Hispanic Adults. Cult. Divers. Ethn. Minor Psychol. 2020, 26, 1–10. [Google Scholar] [CrossRef]
- Fernández-de-las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef] [PubMed]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-Discharge Persistent Symptoms and Health-Related Quality of Life after Hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.-Y.; Li, T.; Gong, F.-H.; Zhang, J.-S.; Li, X.-K. Predictors of Health-Related Quality of Life and Influencing Factors for COVID-19 Patients, a Follow-Up at One Month. Front. Psychiatry 2020, 11, 668. [Google Scholar] [CrossRef] [PubMed]
- Poudel, A.N.; Zhu, S.; Cooper, N.; Roderick, P.; Alwan, N.; Tarrant, C.; Ziauddeen, N.; Yao, G.L. Impact of COVID-19 on Health-Related Quality of Life of Patients: A Structured Review. PLoS ONE 2021, 16, e0259164. [Google Scholar] [CrossRef] [PubMed]
- Meys, R.; Delbressine, J.M.; Goërtz, Y.M.J.; Vaes, A.W.; Machado, F.V.C.; van Herck, M.; Burtin, C.; Posthuma, R.; Spaetgens, B.; Franssen, F.M.E.; et al. Generic and Respiratory-Specific Quality of Life in Non-Hospitalized Patients with COVID-19. J. Clin. Med. 2020, 9, 3993. [Google Scholar] [CrossRef]
- Håkansson, C.; Lissner, L.; Björkelund, C.; Sonn, U. Engagement in Patterns of Daily Occupations and Perceived Health among Women of Working Age. Scand. J. Occup. Ther. 2009, 16, 110–117. [Google Scholar] [CrossRef]
- Meseguer de Pedro, M.; Fernández-Valera, M.M.; García-Izquierdo, M.; Soler Sánchez, M.I. Burnout, Psychological Capital and Health during COVID-19 Social Isolation: A Longitudinal Analysis. Int. J. Environ. Res. Public Health 2021, 18, 1064. [Google Scholar] [CrossRef]
- Park, S.; Lee, H.J.; Jeon, B.-J.; Yoo, E.-Y.; Kim, J.-B.; Park, J.-H. Effects of Occupational Balance on Subjective Health, Quality of Life, and Health-Related Variables in Community-Dwelling Older Adults: A Structural Equation Modeling Approach. PLoS ONE 2021, 16, e0246887. [Google Scholar] [CrossRef] [PubMed]
- Belhan Çelik, S.; Özkan, E.; Bumin, G. Effects of Occupational Therapy via Telerehabilitation on Occupational Balance, Well-Being, Intrinsic Motivation and Quality of Life in Syrian Refugee Children in COVID-19 Lockdown: A Randomized Controlled Trial. Children 2022, 9, 485. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, B.; Fong, K.N.K.; Meena, S.K.; Prasad, P.; Tong, R.K.Y. Impact of COVID-19 Pandemic Lockdown on Occupational Therapy Practice and Use of Telerehabilitation—A Cross Sectional Study. Eur. Rev. Med. Pharmacol. 2021, 25, 3614–3622. [Google Scholar]
- Fridman, A.; Gershon, R.; Gneezy, A. COVID-19 and Vaccine Hesitancy: A Longitudinal Study. PLoS ONE 2021, 16, e0250123. [Google Scholar] [CrossRef] [PubMed]
- Hay, J.W.; Gong, C.L.; Jiao, X.; Zawadzki, N.K.; Zawadzki, R.S.; Pickard, A.S.; Xie, F.; Crawford, S.A.; Gu, N.Y. A US Population Health Survey on the Impact of COVID-19 Using the EQ-5D-5L. J. Gen. Intern. Med. 2021, 36, 1292–1301. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sociodemographic Variables | n |
|---|---|
| Sex (n (%)) | |
| Women | 95 (77.9) |
| Men | 27 (22.1) |
| Age (range) | 30-50 |
| Age (mean (SD)) | 43.5 (5.8) |
| Time since infection (min.–max. months (SD)) | 4–16 (3.33) |
| Mean (SD) | |
|---|---|
| Physical Functioning (PF) | 27.50 (20.40) |
| Role of Physical Limitations (RP) | 5.12 (16.99) |
| General Health (GH) | 29.51 (16.23) |
| Bodily Pain (BP) | 36.52 (22.04) |
| Physical Component Summary (Pcs) | 24.66(4.45) |
| Vitality (V) | 22.25 (20.71) |
| Mental Health (Mh) | 59.30 (14.94) |
| Social Functioning (SF) | 39.45 (17.53) |
| Role of Emotional Limitations (RE) | 62.81 (46.98) |
| Mental Component Summary (MCS) | 45.95 (8.65) |
| Health Transition | 7.17 (11.35) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | |||||||||
| 0.61 * | 1 | ||||||||
| −0.10 | 0.07 | 1 | |||||||
| 0.29 * | 0.35 * | 0.19 | 1 | ||||||
| 0.42 * | 0.60 * | 0.14 | 0.06 | 1 | |||||
| 0.28 * | 0.39 * | −0.15 | 0.64 * | −0.05 | 1 | ||||
| 0.39 * | 0.50 * | 0.03 | 0.38 * | 0.19 * | 0.47 * | 1 | |||
| 0.27 * | 0.42 * | 0.03 | 0.40 * | 0.18 * | 0.32 * | 0.46 * | 1 | ||
| 0.53 * | 0.58 * | −0.08 | 0.24 * | 0.44 * | 0.34 * | 0.47 * | 0.43 * | 1 | |
| 0.49 * | 0.46 * | 0.13 | 0.27 * | 0.38 * | 0.12 | 0.54 * | 0.33 * | 0.40 * | 1 |
| Physical Functioning | Role of Physical Health | General Health | Bodily Pain | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B (SE) | t | p-Value | B (SE) | t | p-Value | B (SE) | t | p-Value | B (SE) | t | p-Value | |
| Sex (Female vs. Male) | −1.03 (0.44) | −2.08 | 0.040 | −0.07 (0.15) | 0.45 | 0.656 | 0.44 (0.63) | 0.69 | 0.492 | −0.87 (0.41) | −2.12 | 0.036 |
| Age | −0.01 (0.05) | −0.19 | 0.851 | −0.01 (0.01) | 0.65 | 0.518 | 0.02 (0.05) | 0.52 | 0.601 | 0.00 (0.04) | −0.03 | 0.978 |
| Time since infection | 0.05 (0.02) | 2.09 | 0.039 | −0.02 (0.02) | 1.06 | 0.291 | 0.04 (0.02) | 2.11 | 0.037 | −0.06 (0.06) | −1.05 | 0.296 |
| OBQ | 0.22 (0.03) | 8.08 | <0.001 | −0.01 (0.01) | 1.20 | 0.231 | 0.16 (0.02) | 6.69 | <0.001 | 0.05 (0.02) | 3.00 | 0.003 |
| R2 (%) | 36.5 | −0.8 | 26 | 7.2 | ||||||||
| Model | F (4; 117) = 18.39; p < 0.001 | F (4; 117) = 0.76; p = 0.551 | F (4; 117) = 11.60; p < 0.001 | F (4; 117) = 3.36; p = 0.012 | ||||||||
| Vitality | Role of Emotional Limitations | Mental Health | Social Functioning | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B (SE) | t | p-Value | B (SE) | t | p-Value | B (SE) | t | p-Value | B (SE) | t | p-Value | |
| Sex (Female vs. Male) | −1.02 (0.86) | −1.18 | 0.239 | −0.08 (0.31) | −0.27 | 0.789 | 0.42 (0.81) | 0.52 | 0.604 | −0.23 (0.29) | −0.79 | 0.432 |
| Age | −0.03 (0.06) | −0.51 | 0.611 | 0.02 (0.02) | 0.91 | 0.365 | −0.06 (0.06) | −0.98 | 0.33 | 0.03 (0.02) | 1.38 | 0.169 |
| Time since infection | −0.03 (0.01) | −2.14 | 0.034 | 0.02 (0.04) | 0.50 | 0.616 | 0.16 (0.10) | 1.56 | 0.121 | −0.02 (0.04) | −0.60 | 0.552 |
| OBQ | 0.15 (0.03) | 4.75 | <0.001 | 0.04 (0.01) | 3.39 | 0.001 | 0.09 (0.03) | 2.89 | 0.005 | 0.05 (0.01) | 4.81 | <0.001 |
| R2 (%) | 16 | 8.4 | 9.2 | 14.11 | ||||||||
| Model | F (4; 117) = 6.78; p < 0.001 | F (4; 116) = 3.07; p = 0.019 | F (4; 117) = 3.35; p = 0.012 | F (4;1 17) = 5.98; p < 0.001 | ||||||||
| Health Transition | |||
|---|---|---|---|
| B (SE) | t | p-Value | |
| Sex (Female vs. Male) | −5.17 (2.16) | −2.40 | 0.018 |
| Age | 0.20 (0.16) | 1.26 | 0.211 |
| Time since infection | −0.86 (0.27) | −3.13 | 0.002 |
| OBQ | 0.52 (0.08) | 6.56 | <0.001 |
| R2 (%) | 29.5 | ||
| Model | F (4; 117) = 13.66; p < 0.001 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodríguez-Pérez, M.P.; Sánchez-Herrera-Baeza, P.; Rodríguez-Ledo, P.; Huertas-Hoyas, E.; Fernández-Gómez, G.; Montes-Montes, R.; Pérez-de-Heredia-Torres, M. Influence of Clinical and Sociodemographic Variables on Health-Related Quality of Life in the Adult Population with Long COVID. J. Clin. Med. 2023, 12, 4222. https://doi.org/10.3390/jcm12134222
Rodríguez-Pérez MP, Sánchez-Herrera-Baeza P, Rodríguez-Ledo P, Huertas-Hoyas E, Fernández-Gómez G, Montes-Montes R, Pérez-de-Heredia-Torres M. Influence of Clinical and Sociodemographic Variables on Health-Related Quality of Life in the Adult Population with Long COVID. Journal of Clinical Medicine. 2023; 12(13):4222. https://doi.org/10.3390/jcm12134222
Chicago/Turabian StyleRodríguez-Pérez, Mª Pilar, Patricia Sánchez-Herrera-Baeza, Pilar Rodríguez-Ledo, Elisabet Huertas-Hoyas, Gemma Fernández-Gómez, Rebeca Montes-Montes, and Marta Pérez-de-Heredia-Torres. 2023. "Influence of Clinical and Sociodemographic Variables on Health-Related Quality of Life in the Adult Population with Long COVID" Journal of Clinical Medicine 12, no. 13: 4222. https://doi.org/10.3390/jcm12134222