
Relationship between Motor Corticospinal System, Endogenous Pain Modulation Mechanisms and Clinical Symptoms in Patients with Knee Osteoarthritis: New Perspectives on an Old Disease
 , and
, and
Abstract
:1. Introduction
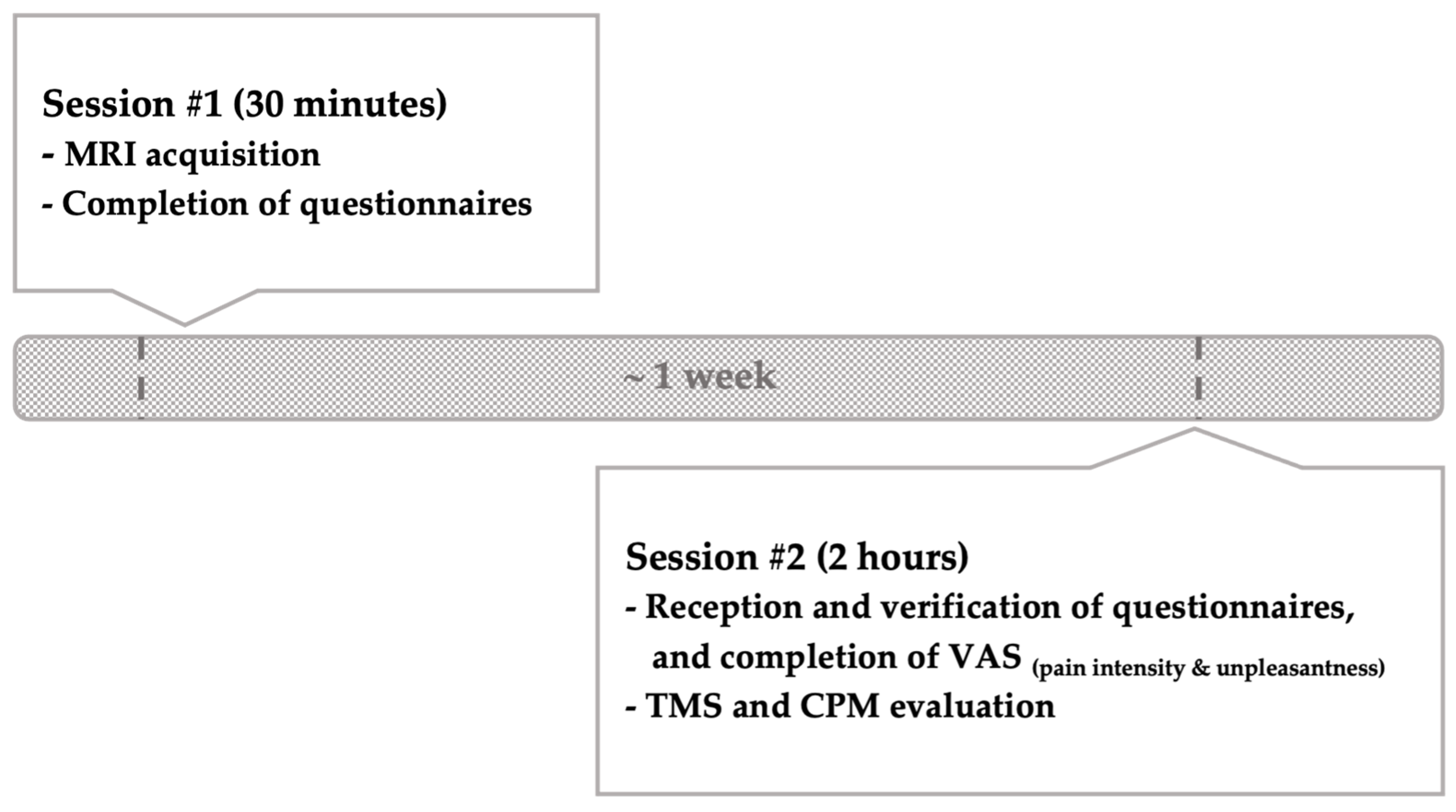
2. Methods
2.1. Participants
2.2. Inhibitory Pain Mechanisms (Bulbospinal Projections)
2.3. Excitatory Pain Mechanisms (Temporal Summation)
2.4. Corticomotor System (Corticospinal Projections and Intracortical Mechanisms)
2.5. OA Signs and Symptoms Assessment
2.6. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
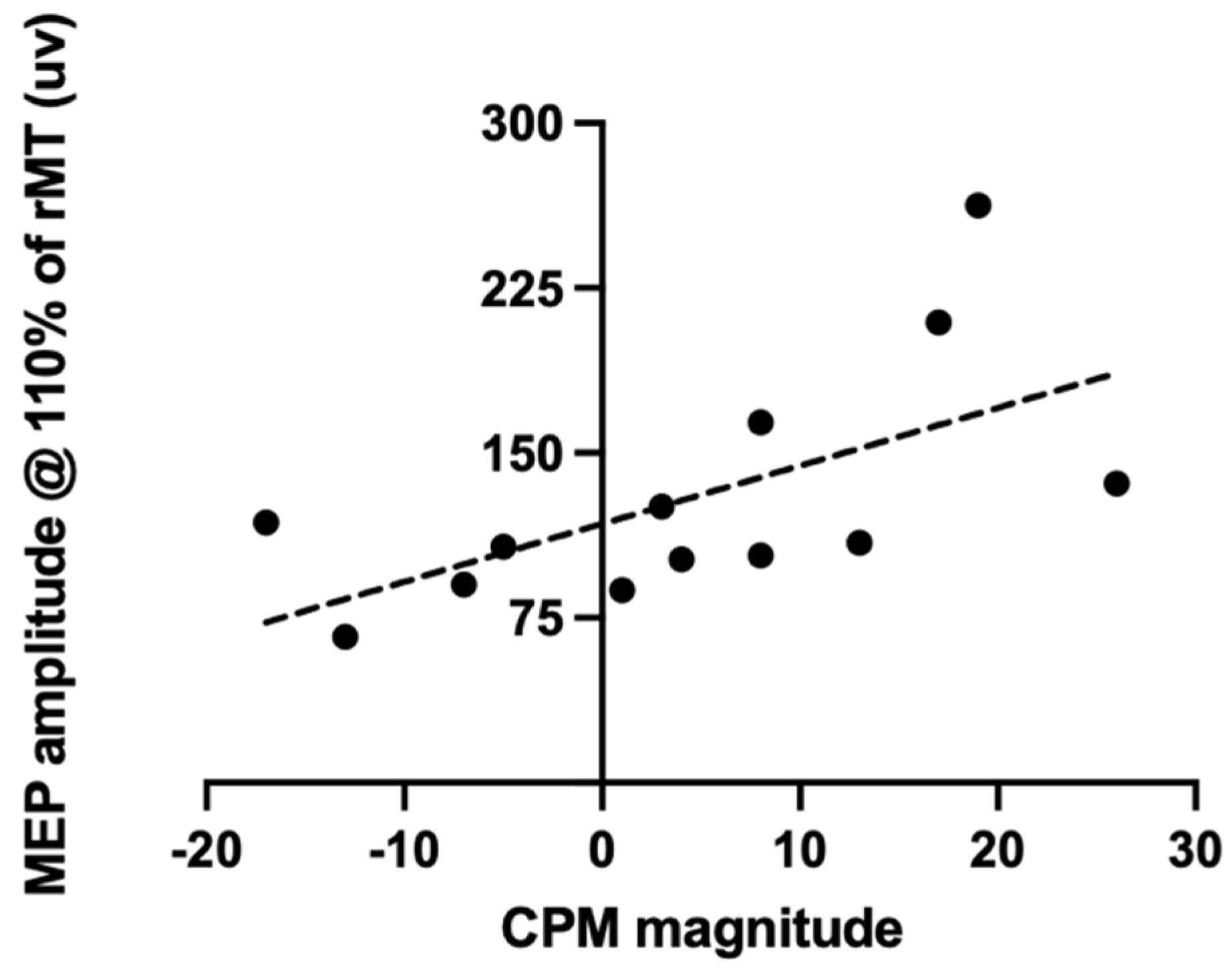
3.2. Correlation between CPM Responses and Corticomotor Excitability
3.3. Relationship between Inhibitory and Excitatory Pain Responses and Clinical Symptoms
3.4. Relationship between TMS Measures and Clinical Symptoms
4. Discussion
4.1. Relationships between Corticospinal and Bulbospinal Projections
4.2. Intracortical Inhibition
4.3. Psychological Symptoms
4.4. Temporal Summation
4.5. Clinical and Rehabilitation Perspectives
4.6. Limits
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hawker, G.A. Osteoarthritis is a serious disease. Clin. Exp. Rheumatol. 2019, 37 (Suppl. S120), 3–6. [Google Scholar]
- Sánchez-Romero, E.A.; González-Zamorano, Y.; Arribas-Romano, A.; Martínez-Pozas, O.; Fernández Espinar, E.; Pedersini, P.; Villafañe, J.H.; Alonso Pérez, J.L.; Fernández-Carnero, J. Efficacy of Manual Therapy on Facilitatory Nociception and Endogenous Pain Modulation in Older Adults with Knee Osteoarthritis: A Case Series. Appl. Sci. 2021, 11, 1895. [Google Scholar] [CrossRef]
- Sánchez Romero, E.A.; Fernández-Carnero, J.; Calvo-Lobo, C.; Ochoa Sáez, V.; Burgos Caballero, V.; Pecos-Martín, D. Is a Combination of Exercise and Dry Needling Effective for Knee OA? Pain Med. 2020, 21, 349–363. [Google Scholar] [CrossRef]
- Glyn-Jones, S.; Palmer, A.J.R.; Agricola, R.; Price, A.J.; Vincent, T.L.; Weinans, H.; Carr, A.J. Osteoarthritis. Lancet 2015, 386, 376–387. [Google Scholar] [CrossRef] [PubMed]
- Felson, D.T. Osteoarthritis as a disease of mechanics. Osteoarthr. Cartil. OARS Osteoarthr. Res. Soc. 2013, 21, 10–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelletier, R.; Higgins, J.; Bourbonnais, D. Is neuroplasticity in the central nervous system the missing link to our understanding of chronic musculoskeletal disorders? BMC Musculoskelet. Disord. 2015, 16, 25. [Google Scholar] [CrossRef] [Green Version]
- Perrot, S. Osteoarthritis pain. Best. Pract. Res. Clin. Rheumatol. 2015, 29, 90–97. [Google Scholar] [CrossRef]
- Salaffi, F.; Ciapetti, A.; Carotti, M. The sources of pain in osteoarthritis: A pathophysiological review. Reumatismo 2014, 66, 57–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petersen, K.K.; Graven-Nielsen, T.; Simonsen, O.; Laursen, M.B.; Arendt-Nielsen, L. Preoperative pain mechanisms assessed by cuff algometry are associated with chronic postoperative pain relief after total knee replacement. Pain 2016, 157, 1400–1406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moana-Filho, E.J.; Herrero Babiloni, A.; Theis-Mahon, N.R. Endogenous pain modulation in chronic orofacial pain: A systematic review and meta-analysis. Pain 2018, 159, 1441–1455. [Google Scholar] [CrossRef]
- Staud, R. Abnormal endogenous pain modulation is a shared characteristic of many chronic pain conditions. Expert. Rev. Neurother. 2012, 12, 577–585. [Google Scholar] [CrossRef]
- Foucher, K.C.; Chmell, S.J.; Courtney, C.A. Duration of symptoms is associated with conditioned pain modulation and somatosensory measures in knee osteoarthritis. J. Orthop. Res. 2019, 37, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Granovsky, Y.; Sprecher, E.; Sinai, A. Motor corticospinal excitability: A novel facet of pain modulation? Pain Rep. 2019, 4, e725. [Google Scholar] [CrossRef] [PubMed]
- Arendt-Nielsen, L.; Nie, H.; Laursen, M.B.; Laursen, B.S.; Madeleine, P.; Simonsen, O.H.; Graven-Nielsen, T. Sensitization in patients with painful knee osteoarthritis. Pain 2010, 149, 573–581. [Google Scholar] [CrossRef]
- Graven-Nielsen, T.; Wodehouse, T.; Langford, R.M.; Arendt-Nielsen, L.; Kidd, B.L. Normalization of widespread hyperesthesia and facilitated spatial summation of deep-tissue pain in knee osteoarthritis patients after knee replacement. Arthritis Rheum. 2012, 64, 2907–2916. [Google Scholar] [CrossRef] [PubMed]
- Baiamonte, B.A.; Stickley, S.C.; Ford, S.J. Nicotine Deprivation Produces Deficits in Pain Perception that are Moderately Attenuated by Caffeine Consumption. J. Psychoact. Drugs. 2016, 48, 159–165. [Google Scholar] [CrossRef]
- Baratloo, A.; Rouhipour, A.; Forouzanfar, M.M.; Safari, S.; Amiri, M.; Negida, A. The Role of Caffeine in Pain Management: A Brief Literature Review. Anesthesiol. Pain Med. 2016, 6, e33193. [Google Scholar] [CrossRef] [Green Version]
- Tousignant-Laflamme, Y.; Pagé, S.; Goffaux, P.; Marchand, S. An experimental model to measure excitatory and inhibitory pain mechanisms in humans. Brain Res. 2008, 1230, 73–79. [Google Scholar] [CrossRef]
- Suzan, E.; Aviram, J.; Treister, R.; Eisenberg, E.; Pud, D. Individually based measurement of temporal summation evoked by a noxious tonic heat paradigm. J. Pain Res. 2015, 8, 409–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbruzzese, G.; Trompetto, C. Clinical and research methods for evaluating cortical excitability. J. Clin. Neurophysiol. 2002, 19, 307–321. [Google Scholar] [CrossRef] [PubMed]
- Rossini, P.M.; Burke, D.; Chen, R.; Cohen, L.G.; Daskalakis, Z.; Di Iorio, R.; Di Lazzaro, V.; Ferreri, F.; Fitzgerald, P.B.; George, M.S.; et al. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clin. Neurophysiol. 2015, 126, 1071–1107. [Google Scholar] [CrossRef]
- Dworkin, R.H.; Turk, D.C.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Katz, N.P.; Kerns, R.D.; Stucki, G.; Allen, R.R.; Bellamy, N.; et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain 2005, 113, 9–19. [Google Scholar] [CrossRef]
- Price, D.D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef]
- Melzack, R. The McGill Pain Questionnaire: Major properties and scoring methods. Pain 1975, 1, 277–299. [Google Scholar] [CrossRef]
- Ferraz, M.B.; Quaresma, M.R.; Aquino, L.R.; Atra, E.; Tugwell, P.; Goldsmith, C.H. Reliability of pain scales in the assessment of literate and illiterate patients with rheumatoid arthritis. J. Rheumatol. 1990, 17, 1022–1024. [Google Scholar] [PubMed]
- Burckhardt, C.S. The use of the McGill Pain Questionnaire in assessing arthritis pain. Pain 1984, 19, 305–314. [Google Scholar] [CrossRef]
- Mendoza, T.; Mayne, T.; Rublee, D.; Cleeland, C. Reliability and validity of a modified Brief Pain Inventory short form in patients with osteoarthritis. Eur. J. Pain 2006, 10, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Cleeland, C.S.; Ryan, K.M. Pain assessment: Global use of the Brief Pain Inventory. Ann. Acad. Med. Singap. 1994, 23, 129–138. [Google Scholar] [PubMed]
- Bellamy, N.; Buchanan, W.W.; Goldsmith, C.H.; Campbell, J.; Stitt, L.W. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J. Rheumatol. 1988, 15, 1833–1840. [Google Scholar]
- Basaran, S.; Guzel, R.; Seydaoglu, G.; Guler-Uysal, F. Validity, reliability, and comparison of the WOMAC osteoarthritis index and Lequesne algofunctional index in Turkish patients with hip or knee osteoarthritis. Clin. Rheumatol. 2010, 29, 749–756. [Google Scholar] [CrossRef]
- Bruce, B.; Fries, J. Longitudinal comparison of the Health Assessment Questionnaire (HAQ) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Arthritis Rheum. 2004, 51, 730–737. [Google Scholar] [CrossRef]
- Neblett, R.M.; Hartzell, M.M.; Cohen, H.; Mayer, T.G.; Williams, M.; Choi, Y.M.; Gatchel, R.J.P. Ability of the central sensitization inventory to identify central sensitivity syndromes in an outpatient chronic pain sample. Clin. J. Pain 2015, 31, 323–332. [Google Scholar] [CrossRef]
- Mayer, T.G.; Neblett, R.; Cohen, H.; Howard, K.J.; Choi, Y.H.; Williams, M.J.; Perez, Y.; Gatchel, R.J. The development and psychometric validation of the central sensitization inventory. Pain Pract. Off. J. World Inst. Pain. 2012, 12, 276–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sullivan, M.; Bishop, S.; Pivik, J. The Pain Catastrophizing Scale: Development and Validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- Ong, W.J.; Kwan, Y.H.; Lim, Z.Y.; Thumboo, J.; Yeo, S.J.; Yeo, W.; Wong, S.B.; Leung, Y.Y. Measurement properties of Pain Catastrophizing Scale in patients with knee osteoarthritis. Clin. Rheumatol. 2021, 40, 295–301. [Google Scholar] [CrossRef] [PubMed]
- French, D.J.; Noël, M.; Vigneau, F.; French, J.; Cyr, C.; Evans, R.T. L’Échelle de dramatisation face à la douleur PCS-CF Adaptation canadienne en langue française de l’échelle «Pain Catastrophizing Scale». Can. J. Behav. Sci. 2005, 37, 181–192. [Google Scholar] [CrossRef]
- Swinkels-Meewisse, E.; Swinkels, R.; Verbeek, A.; Vlaeyen, J.; Oostendorp, R. Psychometric properties of the Tampa Scale for kinesiophobia and the fear-avoidance beliefs questionnaire in acute low back pain. Man. Ther. 2003, 8, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Kori, S.H.; Miller, R.P.; Todd, D.D. Kinesiophobia: A new view of chronic pain behavior. Pain Manag. 1990, 3, 35–43. [Google Scholar]
- Vlaeyen, J.W.; Kole-Snijders, A.M.; Rotteveel, A.M.; Ruesink, R.; Heuts, P.H. The role of fear of movement/(re)injury in pain disability. J. Occup. Rehabil. 1995, 5, 235–252. [Google Scholar] [CrossRef]
- Spielberger, C.; Vagg, P. Psychometric properties of the STAI: A reply to Ramanaiah, Franzen, and Schill. J. Pers. Assess. 1984, 48, 95–97. [Google Scholar] [CrossRef]
- Gauthier, J.; Bouchard, S. Adaptation canadienne-française de la forme révisée du State–Trait Anxiety Inventory de Spielberger. Can. J. Behav. Sci. Rev. Can. Sci. Comport. 1993, 25, 559–578. [Google Scholar] [CrossRef]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry. 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Scogin, F.; Beutler, L.; Corbishley, A.; Hamblin, D. Reliability and validity of the short form beck depression inventory with older adults. J. Clin. Psychol. 1988, 44, 853–857. [Google Scholar] [CrossRef]
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- O’Connell, N.E.; Marston, L.; Spencer, S.; DeSouza, L.H.; Wand, B.M. Non-invasive brain stimulation techniques for chronic pain. Cochrane Database Syst. Rev. 2018, 3, CD008208. [Google Scholar] [CrossRef] [Green Version]
- Korchounov, A.; Ziemann, U. Neuromodulatory neurotransmitters influence LTP-like plasticity in human cortex: A pharmaco-TMS study. Neuropsychopharmacology 2011, 36, 1894–1902. [Google Scholar] [CrossRef] [Green Version]
- Molina-Luna, K.; Pekanovic, A.; Röhrich, S.; Hertler, B.; Schubring-Giese, M.; Rioult-Pedotti, M.-S.; Luft, A.R. Dopamine in motor cortex is necessary for skill learning and synaptic plasticity. PLoS ONE 2009, 4, e7082. [Google Scholar] [CrossRef] [Green Version]
- Kuo, M.F.; Grosch, J.; Fregni, F.; Paulus, W.; Nitsche, M.A. Focusing Effect of Acetylcholine on Neuroplasticity in the Human Motor Cortex. J. Neurosci. 2007, 27, 14442–14447. [Google Scholar] [CrossRef] [Green Version]
- Kuo, M.F.; Paulus, W.; Nitsche, M.A. Boosting focally-induced brain plasticity by dopamine. Cereb. Cortex 2008, 18, 648–651. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lefaucheur, J.P. Motor cortex dysfunction revealed by cortical excitability studies in Parkinson’s disease: Influence of antiparkinsonian treatment and cortical stimulation. Clin. Neurophysiol. 2005, 116, 244–253. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Larrea, L.; Peyron, R. Motor cortex stimulation for neuropathic pain: From phenomenology to mechanisms. NeuroImage 2007, 37, S71–S79. [Google Scholar] [CrossRef] [PubMed]
- Goss, D.A.; Hoffman, R.L.; Clark, B.C. Utilizing Transcranial Magnetic Stimulation to Study the Human Neuromuscular System. J. Vis. Exp. 2012, 59, 3387. [Google Scholar] [CrossRef] [Green Version]
- Tarragó, M.d.G.L.; Deitos, A.; Brietzke, A.P.; Vercelino, R.; Torres, I.L.S.; Fregni, F.; Caumo, W. Descending Control of Nociceptive Processing in Knee Osteoarthritis Is Associated With Intracortical Disinhibition: An Exploratory Study. Medicine 2016, 95, e3353. [Google Scholar] [CrossRef]
- Riddle, D.L.; Wade, J.B.; Jiranek, W.A.; Kong, X. Preoperative pain catastrophizing predicts pain outcome after knee arthroplasty. Clin. Orthop. 2010, 468, 798–806. [Google Scholar] [CrossRef] [Green Version]
- Dekker, J.; van Dijk, G.M.; Veenhof, C. Risk factors for functional decline in osteoarthritis of the hip or knee. Curr. Opin. Rheumatol. 2009, 21, 520–524. [Google Scholar] [CrossRef] [Green Version]
- Martel, M.; Wasan, A.; Edwards, R. Sex differences in the stability of conditioned pain modulation (CPM) among patients with chronic pain. Pain Med. 2013, 14, 1757–1768. [Google Scholar] [CrossRef] [Green Version]
- Edwards, R.R.; Ness, T.J.; Weigent, D.A.; Fillingim, R.B. Individual differences in diffuse noxious inhibitory controls (DNIC): Association with clinical variables. Pain 2003, 106, 427–437. [Google Scholar] [CrossRef]
- Granot, M.; Weissman-Fogel, I.; Crispel, Y.; Pud, D.; Granovsky, Y.; Sprecher, E.; Yarnitsky, D. Determinants of endogenous analgesia magnitude in a diffuse noxious inhibitory control (DNIC) paradigm: Do conditioning stimulus painfulness, gender and personality variables matter? Pain 2008, 136, 142–149. [Google Scholar] [CrossRef]
- Weissman-Fogel, I.; Sprecher, E.; Pud, D. Effects of catastrophizing on pain perception and pain modulation. Exp. Brain Res. 2008, 186, 79–85. [Google Scholar] [CrossRef]
- Nahman-Averbuch, H.; Nir, R.R.; Sprecher, E.; Yarnitsky, D. Psychological Factors and Conditioned Pain Modulation: A Meta-Analysis. Clin. J. Pain 2016, 32, 541–554. [Google Scholar] [CrossRef]
- Sean, M.; Coulombe-Lévêque, A.; Vincenot, M.; Martel, M.; Gendron, L.; Marchand, S.; Léonard, G. Transcutaneous electrical nerve stimulation (TENS): Towards the development of a clinic-friendly method for the evaluation of excitatory and inhibitory pain mechanisms. Can. J. Pain 2020, 5, 56–65. [Google Scholar] [CrossRef]
- Kurien, T.; Arendt-Nielsen, L.; Petersen, K.K.; Graven-Nielsen, T.; Scammell, B.E. Preoperative Neuropathic Pain-like Symptoms and Central Pain Mechanisms in Knee Osteoarthritis Predicts Poor Outcome 6 Months After Total Knee Replacement Surgery. J. Pain. 2018, 19, 1329–1341. [Google Scholar] [CrossRef]
- Neogi, T.; Frey-Law, L.; Scholz, J.; Niu, J.; Arendt-Nielsen, L.; Woolf, C.; Nevitt, M.; Bradley, L.; Felson, D.T. Sensitivity and sensitisation in relation to pain severity in knee osteoarthritis: Trait or state? Ann. Rheum. Dis. 2015, 74, 682–688. [Google Scholar] [CrossRef]
- Petersen, K.K.; Arendt-Nielsen, L.; Simonsen, O.; Wilder-Smith, O.; Laursen, M.B. Presurgical assessment of temporal summation of pain predicts the development of chronic postoperative pain 12 months after total knee replacement. Pain 2015, 156, 55–61. [Google Scholar] [CrossRef]
- Yarnitsky, D.; Granot, M.; Granovsky, Y. Pain modulation profile and pain therapy: Between pro- and antinociception. Pain. 2014, 155, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Kittelson, A.J.; Thomas, A.C.; Kluger, B.M.; Stevens-Lapsley, J.E. Corticospinal and intracortical excitability of the quadriceps in patients with knee osteoarthritis. Exp. Brain Res. 2014, 232, 3991–3999. [Google Scholar] [CrossRef] [PubMed]
- Hunt, M.A.; Zabukovec, J.R.; Peters, S.; Pollock, C.L.; Linsdell, M.A.; Boyd, L.A. Reduced quadriceps motor-evoked potentials in an individual with unilateral knee osteoarthritis: A case report. Case Rep. Rheumatol. 2011, 2011, 537420. [Google Scholar] [CrossRef] [PubMed]
- Burns, L.C.; Ritvo, S.E.; Ferguson, M.K.; Clarke, H.; Seltzer, Z.; Katz, J. Pain catastrophizing as a risk factor for chronic pain after total knee arthroplasty: A systematic review. J. Pain Res. 2015, 8, 21–32. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, G.N.; Rice, D.A.; McNair, P.J.; Kluger, M. Predictors of persistent pain after total knee arthroplasty: A systematic review and meta-analysis. Br. J. Anaesth. 2015, 114, 551–561. [Google Scholar] [CrossRef] [Green Version]
- Parker, R.S.; Lewis, G.N.; Rice, D.A.; McNair, P.J. Is Motor Cortical Excitability Altered in People with Chronic Pain? A Systematic Review and Meta-Analysis. Brain Stimul. 2016, 9, 488–500. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Central sensitization: Implications for the diagnosis and treatment of pain. Pain 2011, 152 (Suppl. S3), S2–S15. [Google Scholar] [CrossRef] [PubMed]
- Jodoin, M.; Rouleau, D.M.; Bellemare, A.; Provost, C.; Larson-Dupuis, C.; Sandman, É.; Laflamme, G.-Y.; Benoit, B.; Leduc, S.; Levesque, M.; et al. Moderate to severe acute pain disturbs motor cortex intracortical inhibition and facilitation in orthopedic trauma patients: A TMS study. PLoS ONE 2020, 15, e0226452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sánchez-Romero, E.A.; Battaglino, A.; Campanella, W.; Turroni, S.; Bishop, M.D.; Villafañe, J.H. Impact on Blood Tests of Lower Limb Joint Replacement for the Treatment of Osteoarthritis: Hip and Knee. Top. Geriatr. Rehabil. 2021, 37, 227–229. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | |
|---|---|
| Number (n) | 28 |
| Gender (F/M) | 14/14 |
| Age (years) | |
| Mean ± SD | 69 ± 7 |
| Range | 57–82 |
| Time since diagnosis (years) | |
| Mean ± SD | 5.5 ± 5.5 |
| Kellgren-Lawrence score (%) | |
| KL 2 | 4 |
| KL 3 | 18 |
| KL 4 | 78 |
| Psychophysical Variables | Mean | Standard Deviation | n |
|---|---|---|---|
| CPM | |||
| Mean pain before CPT ( /100) | 49.9 | 17.9 | 18 |
| Mean pain after CPT ( /100) | 47.0 | 17.5 | |
| Delta score | 2.9 | 12.7 | |
| Temporal summation | |||
| 120–30 s | 14 | 25 | 18 |
| Slopes | 19 | 25 | |
| Neurophysiological variables | |||
| rMT (% of the stimulator’s maximum output) | 51 | 8 | 23 |
| MEP amplitude (µV) @ | |||
| 100% of rMT | 127.60 | 69.47 | 16 |
| 105% of rMT | 129.53 | 62.45 | 17 |
| 110% of rMT | 135.57 | 71.26 | 23 |
| 120% of rMT | 243.18 | 134.87 | 17 |
| 130% of rMT | 243.81 | 150.95 | 22 |
| 140% of rMT | 370.91 | 240.28 | 16 |
| 150% of rMT | 377.00 | 256.92 | 20 |
| Slope of the recruitment curves | 5.38 | 4.91 | 22 |
| CSP (ms) | 183.4 | 48.2 | 16 |
| Clinical symptoms | |||
| MPQ | 28 | ||
| Global score ( /72) | 21 | 13 | |
| Numerical rating scale ( /10) | 4 | 3 | |
| BPI | 28 | ||
| Worst pain last 24 h ( /10) | 6 | 2 | |
| Least pain last 24 h ( /10) | 3 | 2 | |
| Pain on average ( /10) | 5 | 2 | |
| Pain right now ( /10) | 4 | 3 | |
| Incapacity ( /70) | 29 | 14 | |
| WOMAC | 28 | ||
| Pain ( /500) | 254 | 110 | |
| Stiffness ( /200) | 117 | 50 | |
| Functional mobility ( /1 700) | 860 | 369 | |
| CSI ( /100) | 31 | 15 | 22 |
| PCS ( /52) | 14 | 12 | 28 |
| TSK ( /68) | 39 | 9 | 22 |
| STAI | 22 | ||
| State ( /80) | 33 | 11 | |
| Trait ( /80) | 35 | 10 | |
| BDI ( /39) | 3 | 3 | 28 |
| Pain unpleasantness (VAS) | 3 | 3 | 22 |
| TMS Intensity (% of rMT) | 110 | 120 |
|---|---|---|
| MPQ | ||
| Global score | NS | NS |
| Numerical rating scale | rs = 0.50, p = 0.02 | rs = 0.65, p < 0.01 |
| BPI | ||
| Pain at its worst (last 24 h) | rs = 0.54, p < 0.01 | NS |
| Pain at its least (last 24 h) | rs = 0.44, p = 0.04 | rs = 0.50, p = 0.04 |
| Pain interference (last 24 h) | rs = 0.49, p = 0.02 | NS |
| Pain on average | rs = 0.55, p < 0.01 | NS |
| Present pain | rs = 0.51, p = 0.01 | rs = 0.64, p < 0.01 |
| WOMAC | NS | |
| Pain | rs = 0.45, p = 0.03 | |
| Stiffness | NS | |
| Functional mobility | NS | |
| CSI | rs = 0.63, p < 0.01 | NS |
| PCS | rs = 0.43, p = 0.04 | rs = 0.50, p = 0.04 |
| TSK | NS | NS |
| STAI | NS | NS |
| State | ||
| Trai | ||
| BDI (short form) | NS | NS |
| Pain intensity * | NS | rs = 0.53, p = 0.03 |
| Pain unpleasantness * | NS | NS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martel, M.; Gaudreault, N.; Pelletier, R.; Houde, F.; Harvey, M.-P.; Giguère, C.; Balg, F.; Leonard, G. Relationship between Motor Corticospinal System, Endogenous Pain Modulation Mechanisms and Clinical Symptoms in Patients with Knee Osteoarthritis: New Perspectives on an Old Disease. Brain Sci. 2023, 13, 1154. https://doi.org/10.3390/brainsci13081154
Martel M, Gaudreault N, Pelletier R, Houde F, Harvey M-P, Giguère C, Balg F, Leonard G. Relationship between Motor Corticospinal System, Endogenous Pain Modulation Mechanisms and Clinical Symptoms in Patients with Knee Osteoarthritis: New Perspectives on an Old Disease. Brain Sciences. 2023; 13(8):1154. https://doi.org/10.3390/brainsci13081154
Chicago/Turabian StyleMartel, Marylie, Nathaly Gaudreault, René Pelletier, Francis Houde, Marie-Philippe Harvey, Caroline Giguère, Frédéric Balg, and Guillaume Leonard. 2023. "Relationship between Motor Corticospinal System, Endogenous Pain Modulation Mechanisms and Clinical Symptoms in Patients with Knee Osteoarthritis: New Perspectives on an Old Disease" Brain Sciences 13, no. 8: 1154. https://doi.org/10.3390/brainsci13081154