

Explanatory Capacity of Postural Control and Physical Fitness in Cognitive Impairment and Support Needs among Individuals with Intellectual Disabilities—A Cross-Sectional Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
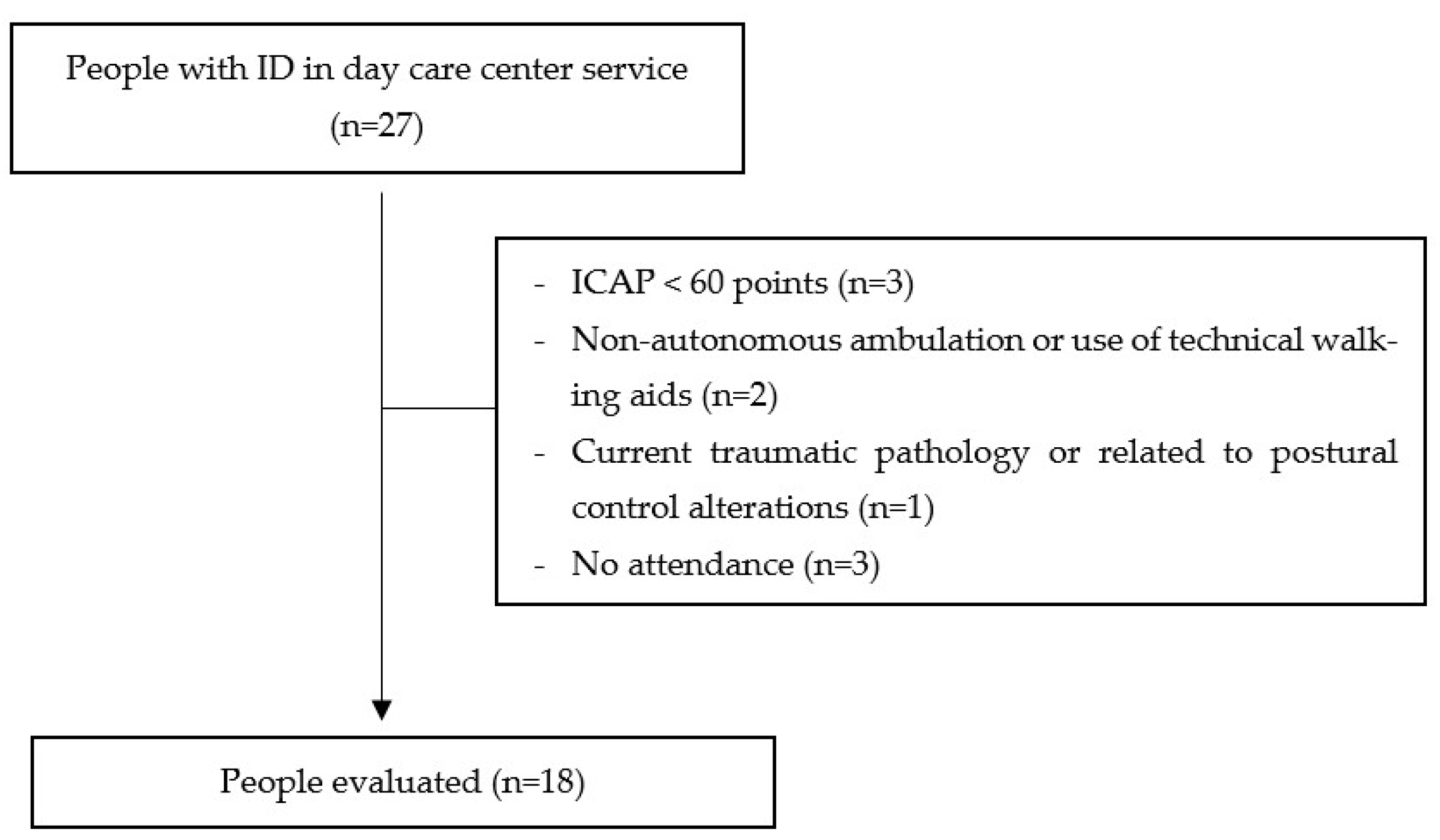
2.2. Description of the Sample
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Participants Characteristics
3.2. Cognitive Impairment
3.3. Support Service Needs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schalock, R.L.; Luckasson, R.; Tassé, M. Defining, Diagnosing, Classifying, and Planning Supports for People with Intellectual Disability: An Emerging Consensus. Siglo Cero 2021, 52, 29–36. [Google Scholar] [CrossRef]
- Patel, D.R.; Cabral, M.D.; Ho, A.; Merrick, J. A Clinical Primer on Intellectual Disability. Transl. Pediatr. 2020, 9, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Tassé, M.J.; Balboni, G.; Navas, P.; Luckasson, R.; Nygren, M.A.; Belacchi, C.; Bonichini, S.; Reed, G.M.; Kogan, C.S. Developing Behavioural Indicators for Intellectual Functioning and Adaptive Behaviour for ICD-11 Disorders of Intellectual Development. J. Intellect. Disabil. Res. 2019, 63, 386–407. [Google Scholar] [CrossRef] [PubMed]
- Salvador-Carulla, L.; Rodríguez-Blázquez, C.; Martorell, A. Intellectual Disability: An Approach from the Health Sciences Perspective. Salud Publica Mex 2008, 50, s142–s150. [Google Scholar] [CrossRef] [PubMed]
- Maïano, C.; Hue, O.; April, J. Fundamental Movement Skills in Children and Adolescents with Intellectual Disabilities: A Systematic Review. J. Appl. Res. Intellect. Disabil. 2019, 32, 1018–1033. [Google Scholar] [CrossRef]
- Enkelaar, L.; Smulders, E.; van Schrojenstein Lantman-de Valk, H.; Geurts, A.C.H.; Weerdesteyn, V. A Review of Balance and Gait Capacities in Relation to Falls in Persons with Intellectual Disability. Res. Dev. Disabil. 2012, 33, 291–306. [Google Scholar] [CrossRef]
- Bahiraei, S.; Daneshmandi, H. The Effect and Durability of Functional Exercises on Balance Evaluation Systems Test (BESTest) Scores in People with Intellectual Disabilities: A Preliminary Report. J. Intellect. Disabil. Res. 2022, 66, 880–892. [Google Scholar] [CrossRef]
- Bahiraei, S.; Daneshmandi, H.; Norasteh, A.A.; Sokhangoei, Y. The Study of Biomechanical Gait Cycle and Balance Characteristics in Intellectual Disabilities: A Systematic Review. Phys. Treat. Specif. Phys. Ther. J. 2018, 8, 63–76. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; ISBN 9781608310180. [Google Scholar]
- Oppewal, A.; Hilgenkamp, T.I.M.; van Wijck, R.; Evenhuis, H.M. Feasibility and Outcomes of the Berg Balance Scale in Older Adults with Intellectual Disabilities. Res. Dev. Disabil. 2013, 34, 2743–2752. [Google Scholar] [CrossRef]
- Sibley, K.M.; Beauchamp, M.K.; Van Ooteghem, K.; Straus, S.E.; Jaglal, S.B. Using the Systems Framework for Postural Control to Analyze the Components of Balance Evaluated in Standardized Balance Measures: A Scoping Review. Arch. Phys. Med. Rehabil. 2015, 96, 122–132.e29. [Google Scholar] [CrossRef]
- Fourcade, P.; Hansen, C.; LeBozec, S.; Bouisset, S. Simultaneous Postural Adjustments (SPA) Scrutinized Using the Lissajous Method. J. Biomech. 2014, 47, 3645–3649. [Google Scholar] [CrossRef] [PubMed]
- Memari, S.; Yiou, E.; Fourcade, P. The Role(s) of “Simultaneous Postural Adjustments” (SPA) during Single Step Revealed with the Lissajous Method. J. Biomech. 2020, 108, 109910. [Google Scholar] [CrossRef] [PubMed]
- Horak, F.B.; Wrisley, D.M.; Frank, J. The Balance Evaluation Systems Test (BESTest) to Differentiate Balance Deficits. Phys. Ther. 2009, 89, 484–498. [Google Scholar] [CrossRef] [PubMed]
- Hallemans, A.; Van de Walle, P.; Wyers, L.; Verheyen, K.; Schoonjans, A.S.; Desloovere, K.; Ceulemans, B. Clinical Usefulness and Challenges of Instrumented Motion Analysis in Patients with Intellectual Disabilities. Gait. Posture 2019, 71, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Bojanek, E.K.; Wang, Z.; White, S.P.; Mosconi, M.W. Postural Control Processes during Standing and Step Initiation in Autism Spectrum Disorder. J. Neurodev. Disord. 2020, 12, 1. [Google Scholar] [CrossRef]
- Maïano, C.; Hue, O.; Morin, A.J.S.; Lepage, G.; Tracey, D.; Moullec, G. Exercise Interventions to Improve Balance for Young People with Intellectual Disabilities: A Systematic Review and Meta-analysis. Dev. Med. Child Neurol. 2019, 61, 406–418. [Google Scholar] [CrossRef]
- Duclos, N.; Duclos, C.; Mesure, S. Control Postural: Fisiología, Conceptos Principales e Implicaciones Para La Readaptación. EMC Kinesiterapia Med. Física 2017, 38, 1–9. [Google Scholar] [CrossRef]
- Tangen, G.G.; Engedal, K.; Bergland, A.; Moger, T.A.; Mengshoel, A.M. Relationships Between Balance and Cognition in Patients With Subjective Cognitive Impairment, Mild Cognitive Impairment, and Alzheimer Disease. Phys. Ther. 2014, 94, 1123–1134. [Google Scholar] [CrossRef]
- Oppewal, A.; Hilgenkamp, T.I.M. Adding Meaning to Physical Fitness Test Results in Individuals with Intellectual Disabilities. Disabil. Rehabil. 2020, 42, 1406–1413. [Google Scholar] [CrossRef]
- Hsu, P.J.; Chou, H.S.; Pan, Y.H.; Ju, Y.Y.; Tsai, C.L.; Pan, C.Y. Sedentary Time, Physical Activity Levels and Physical Fitness in Adults with Intellectual Disabilities. Int. J. Environ. Res. Public Health 2021, 18, 5033. [Google Scholar] [CrossRef]
- Simón-Siles, S.; Font-Farré, M.; Guerra-Balic, M.; Nishishinya-Aquino, M.; Oviedo, G.R. Effects of Exercise on Fitness in Adults with Intellectual Disability: A Protocol of an Overview of Systematic Reviews. BMJ Open 2022, 12, e058053. [Google Scholar] [CrossRef] [PubMed]
- Hilgenkamp, T.I.M.; van Wijck, R.; Evenhuis, H.M. Physical Fitness in Older People with ID—Concept and Measuring Instruments: A Review. Res. Dev. Disabil. 2010, 31, 1027–1038. [Google Scholar] [CrossRef]
- Sampaio, A.; Marques-Aleixo, I.; Seabra, A.; Mota, J.; Marques, E.; Carvalho, J. Physical Fitness in Institutionalized Older Adults with Dementia: Association with Cognition, Functional Capacity and Quality of Life. Aging Clin. Exp. Res. 2020, 32, 2329–2338. [Google Scholar] [CrossRef]
- Zhao, X.; Huang, H.; Du, C. Association of Physical Fitness with Cognitive Function in the Community-Dwelling Older Adults. BMC Geriatr. 2022, 22, 868. [Google Scholar] [CrossRef]
- Van Ingen, D.J.; Moore, L.L.; Zaja, R.H.; Rojahn, J. The Behavior Problems Inventory (BPI-01) in Community-Based Adults with Intellectual Disabilities: Reliability and Concurrent Validity Vis-à-Vis the Inventory for Client and Agency Planning (ICAP). Res. Dev. Disabil. 2010, 31, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Ayaso-Maneiro, J.; Domínguez-Prado, D.M.; García-Soidán, J.L. Application of a Therapeutic Exercise Program in Adults with Intellectual Disability. Apunts. Med. L’esport 2014, 49, 45–52. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. Mini-Mental State. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef] [PubMed]
- Montero, D. Assessment of Adaptive Behavior in People with Disabilities. Adaptation and Validation of the ICAP; Psychopedagogical Resources and Instruments: Bilbao, Spain, 1993; ISBN 8427118414. [Google Scholar]
- Reguera-García, M.M.; Leirós-Rodríguez, R.; Fernández-Baro, E.; Álvarez-Barrio, L. Reliability and Validity of the Six Spot Step Test in People with Intellectual Disability. Brain. Sci. 2021, 11, 201. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Senior Fitness Test Manual; Human Kinetics: New York, NY, USA, 2013; ISBN 1450411185. [Google Scholar]
- Tombaugh, T.N.; McIntyre, N.J. The Mini-Mental State Examination: A Comprehensive Review. J. Am. Geriatr. Soc. 1992, 40, 922–935. [Google Scholar] [CrossRef]
- Vera-Bachmann, D.; Gálvez-Nieto, J.; Trizano-Hermosilla, I.; Álvarez-Espinoza, A. Psychometric Examination of the Inventory for Client and Agency Planning (ICAP), in Chilean Students. Iberoam. J. Diagn. Eval. 2020, 1, 119–129. [Google Scholar] [CrossRef]
- Potter, K.; Brandfass, K. The Mini-Balance Evaluation Systems Test (Mini-BESTest). J. Physiother. 2015, 61, 225. [Google Scholar] [CrossRef] [PubMed]
- Godi, M.; Franchignoni, F.; Caligari, M.; Giordano, A.; Turcato, A.M.; Nardone, A. Comparison of Reliability, Validity, and Responsiveness of the Mini-BESTest and Berg Balance Scale in Patients With Balance Disorders. Phys. Ther. 2013, 93, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Berg, K.; Wood-Dauphinee, S.; Williams, J.I. The Balance Scale: Reliability Assessment with Elderly Residents and Patients with an Acute Stroke. Scand. J. Rehabil. Med. 1995, 27, 27. [Google Scholar] [PubMed]
- Downs, S.; Marquez, J.; Chiarelli, P. The Berg Balance Scale Has High Intra- and Inter-Rater Reliability but Absolute Reliability Varies across the Scale: A Systematic Review. J. Physiother. 2013, 59, 93–99. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Cicioglu, I. Assessment of Physical Fitness Levels of Elderly Turkish Males over 60 Years. Coll. Antropol. 2010, 34, 1323–1327. [Google Scholar]
- Milanovic, Z.; Jorgić, B.; Trajković, N.; Sporis; Pantelić, S. James Age-Related Decrease in Physical Activity and Functional Fitness among Elderly Men and Women. Clin. Interv. Aging 2013, 8, 549–556. [Google Scholar] [CrossRef]
- McGilton, K.S.; Vellani, S.; Zheng, N.; Wang, D.; Yeung, L.; Escrig-Pinol, A. Healthcare Professionals’ Perspectives on Rehabilitating Persons with Cognitive Impairment. Dementia 2021, 20, 1772–1790. [Google Scholar] [CrossRef]
- Kiosses, D.N. IADL Functions, Cognitive Deficits, and Severity of Depression: A Preliminary Study. Am. J. Geriatr. Psychiatry 2005, 13, 244–249. [Google Scholar] [CrossRef]
- McKenzie, K.; Metcalfe, D.; Murray, G. A Review of Measures Used in the Screening, Assessment and Diagnosis of Dementia in People with an Intellectual Disability. J. Appl. Res. Intellect. Disabil. 2018, 31, 725–742. [Google Scholar] [CrossRef]
- Saito, H.; Yamanaka, M.; Kasahara, S.; Fukushima, J. Relationship between Improvements in Motor Performance and Changes in Anticipatory Postural Adjustments during Whole-Body Reaching Training. Hum. Mov. Sci. 2014, 37, 69–86. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.-H.; Tang, P.-F.; Wang, Y.-H.; Lin, K.-H.; Chiu, M.-J.; Chen, S.-H.A. Role of the Premotor Cortex in Leg Selection and Anticipatory Postural Adjustments Associated with a Rapid Stepping Task in Patients with Stroke. Gait Posture 2010, 32, 487–493. [Google Scholar] [CrossRef] [PubMed]
- Varghese, J.P.; Merino, D.M.; Beyer, K.B.; McIlroy, W.E. Cortical Control of Anticipatory Postural Adjustments Prior to Stepping. Neuroscience 2016, 313, 99–109. [Google Scholar] [CrossRef]
- Cavaggioni, L.; Trecroci, A.; Tosin, M.; Iaia, F.M.; Alberti, G. Individualized Dry-Land Intervention Program for an Elite Paralympic Swimmer. J. Sports Med. Phys. Fit. 2018, 59, 82–86. [Google Scholar] [CrossRef] [PubMed]
- De Leeuw, M.J.; Oppewal, A.; Elbers, R.G.; Knulst, M.W.E.J.; van Maurik, M.C.; van Bruggen, M.C.; Hilgenkamp, T.I.M.; Bindels, P.J.E.; Maes-Festen, D.A.M. Healthy Ageing and Intellectual Disability Study: Summary of Findings and the Protocol for the 10-Year Follow-up Study. BMJ Open 2022, 12, e053499. [Google Scholar] [CrossRef]
- Carson, R.G. Get a Grip: Individual Variations in Grip Strength Are a Marker of Brain Health. Neurobiol. Aging 2018, 71, 189–222. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Muscle Strength. Curr. Opin. Clin. Nutr. Metab. Care 2015, 18, 465–470. [Google Scholar] [CrossRef] [PubMed]
- Tajali, S.; Rouhani, M.; Mehravar, M.; Negahban, H.; Sadati, E.; Oskouei, A.E. Effects of External Perturbations on Anticipatory and Compensatory Postural Adjustments in Patients with Multiple Sclerosis and a Fall History. Int. J. MS Care 2018, 20, 164–172. [Google Scholar] [CrossRef]
- Cheung, K.K.W.; Au, K.Y.; Lam, W.W.S.; Jones, A.Y.M. Effects of a Structured Exercise Programme on Functional Balance in Visually Impaired Elderly Living in a Residential Setting. Hong Kong Physiother. J. 2008, 26, 45–50. [Google Scholar] [CrossRef]


{kind=link}
| Mean ± Sd | Range Min–Max | |
|---|---|---|
| Age (years) | 37.50 ± 10.75 | 22.00–58.00 |
| Weight (kg) | 76.83 ± 21.46 | 46.90–124.20 |
| Height (cm) | 163.67 ± 13.72 | 143.00–201.00 |
| BMI (kg/m2) | 28.63 ± 7.18 | 18.83–42.98 |
| TUG (s) | 7.29 ± 1.97 | 5.07–11.70 |
| FRT (cm) | 27.33 ± 10.92 | 17.00–64.00 |
| SSST (s) | 10.66 ± 2.89 | 7.29–18.42 |
| MMSE (0–30 points) | 22.28 ± 5.27 | 12.00–30.00 |
| ICAP (score) | 7.33 ± 0.91 | 6.00–9.00 |
| MBT-T (0–28 points) | 19.61 ± 4.65 | 11.00–27.00 |
| MBT-APA (0–6 points) | 3.78 ± 1.44 | 2.00–6.00 |
| MBT-CPA (0–6 points) | 3.06 ± 1.98 | 0.00–6.00 |
| MBT-SO (0–6 points) | 5.28 ± 1.07 | 3.00–6.00 |
| MBT-G (0–10 points) | 7.50 ± 1.58 | 4.00–10.00 |
| BBS (0–56 points) | 51.17 ± 3.96 | 43.00–56.00 |
| SFT-1 (n rep) | 11.83 ± 3.52 | 7.00–18.00 |
| SFT-2 (n rep) | 14.11 ± 4.03 | 7.00–21.00 |
| SFT-3 (cm) | −24.24 ± 13.07 | −42.00–0.00 |
| SFT-4 (cm) | −23.22 ± 14.96 | −47.00–0.00 |
| SFT-5 (m) | 265.43 ± 101.12 | 150.40–555.00 |
| SFT-6 (s) | 7.30 ± 1.98 | 5.07–11.70 |
| Model 1 | Model 2 | Model 3 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | (95% CI) | β | p | r2 | B | (95% CI) | β | p | r2 | B | (95% CI) | β | p | r2 | |
| MBT-T | 0.41 | (−0.15; 0.97) | 0.37 | 0.14 | 0.13 | 0.43 | 0.15 | ||||||||
| MBT-APA | 1.63 | (−0.11; 3.37) | 0.44 | 0.07 | 0.20 | 2.68 | (−0.19; 5.54) | 0.73 | 0.23 | 0.13 | 5.17 | (−1.57; 11.91) | 1.42 | ||
| MBT-CPA | 0.92 | (−0.40; 2.24) | 0.35 | 0.16 | 0.12 | 0.75 | (−0.84; 2.34) | 0.28 | 1.85 | (−1.51; 5.22) | 0.70 | ||||
| MBT-SO | 0.44 | (−2.15; 3.03) | 0.09 | 0.72 | 0.01 | −1.98 | (−5.22; 1.27) | −0.40 | −4.31 | (−12.37; 3.75) | −0.87 | ||||
| MBT-G | 0.58 | (−1.16; 2.32) | 0.17 | 0.49 | 0.03 | −1.07 | (−3.22; 1.14) | −0.32 | 0.21 | (−3.59; 4.02) | 0.06 | ||||
| BBS | −0.02 | (−0.72; 0.68) | −0.02 | 0.95 | 0.00 | −1.40 | (−3.05; 0.26) | −1.05 | |||||||
| SFT-1 | 0.48 | (−0.27; 1.23) | 0.32 | 0.20 | 0.10 | 0.62 | (−0.93; 2.17) | 0.42 | 0.83 | −0.26 | −0.92 | (−3.98; 2.13) | −0.62 | ||
| SFT-2 | 0.47 | (−0.17; 1.12) | 0.36 | 0.14 | 0.13 | 0.20 | (−0.84; 1.24) | 0.15 | 0.61 | (−0.67; 1.88) | 0.46 | ||||
| SFT-3 | −0.01 | (−0.24; 0.21) | −0.04 | 0.89 | 0.00 | −0.04 | (−0.41; 0.34) | −0.09 | 0.07 | (−0.52; 0.67) | 0.18 | ||||
| SFT-4 | 0.05 | (−0.14; 0.23) | 0.13 | 0.61 | 0.02 | 0.07 | (−0.20; 0.34) | 0.19 | 0.05 | (−0.31; 0.41) | 0.13 | ||||
| SFT-5 | −0.01 | (−0.03; 0.02) | −0.13 | 0.62 | 0.02 | −0.01 | (−0.05; 0.03) | −0.19 | 0.03 | (−0.03; 0.09) | 0.60 | ||||
| SFT-6 | −0.33 | (−1.73; 1.07) | −0.13 | 0.62 | 0.02 | 0.40 | (−2.45; 3.25) | 0.15 | −0.57 | (−6.51; 5.36) | −0.22 | ||||
| Model 1 | Model 2 | Model 3 | Model 4 | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B | (95% CI) | β | p | r2 | B | (95% CI) | β | p | r2 | B | (95% CI) | β | p | r2 | B | (95% CI) | β | p | r2 | |
| MBT-T | 0.13 | (0.05; 0.21) | 0.65 | 0.004 | 0.42 | 0.36 | ||||||||||||||
| MBT-APA | 0.44 | (0.20; 0.68) | 0.69 | 0.001 | 0.48 | 0.45 | (0.38; 0.86) | 0.71 | 0.031 | 0.39 | 1.14 | (−0.31; 2.59) | 1.81 | 0.44 | (0.19; 0.69) | 0.70 | 0.002 | 0.45 | ||
| MBT-CPA | 0.23 | (0.03; 0.44) | 0.51 | 0.030 | 0.26 | 0.13 | (−0.10; 0.36) | 0.28 | 0.18 | (−0.47; 0.82) | 0.29 | |||||||||
| MBT-SO | 0.32 | (−0.09; 0.74) | 0.38 | 0.118 | 0.15 | −0.10 | (−0.57; 0.36) | −0.12 | −0.87 | (−2.39; 0.66) | −1.02 | |||||||||
| MBT-G | 0.21 | (−0.07; 0.49) | 0.37 | 0.132 | 0.14 | −0.09 | (−0.40; 0.23) | −0.15 | 0.12 | (−0.50; 0.73) | 0.20 | |||||||||
| BBS | 0.09 | (−0.02; 0.21) | 0.41 | 0.092 | 0.17 | −0.18 | (−0.55; 0.19) | −0.78 | ||||||||||||
| SFT-1 | 0.09 | (−0.04; 0.22) | 0.35 | 0.155 | 0.12 | 0.04 | (−0.18; 0.26) | 0.16 | 0.250 | 0.18 | −0.29 | (−0.81; 0.24) | −1.11 | 0.311 | ||||||
| SFT-2 | 0.12 | (0.02; 0.22) | 0.52 | 0.027 | 0.27 | 0.08 | (−0.06; 0.23) | 0.36 | 0.17 | (−0.06; 0.41) | 0.75 | |||||||||
| SFT-3 | 0.00 | (−0.04; 0.04) | −0.05 | 0.851 | 0.00 | 0.00 | (−0.05; 0.06) | 0.04 | 0.03 | (−0.06; 0.13) | 0.46 | |||||||||
| SFT-4 | 0.02 | (−0.01; 0.05) | 0.30 | 0.233 | 0.09 | 0.03 | (−0.01; 0.06) | 0.39 | 0.03 | (−0.03; 0.09) | 0.42 | |||||||||
| SFT-5 | 0.00 | (−0.01; 0.00) | −0.22 | 0.373 | 0.05 | 0.00 | (−0.00; 0.00) | −0.26 | 0.00 | (−0.01; 0.02) | 0.50 | |||||||||
| SFT-6 | −0.13 | (−0.37; 0.10) | −0.29 | 0.246 | 0.08 | −0.12 | (−0.52; 0.28) | −0.27 | −0.37 | (−1.33; 0.60) | −0.80 | |||||||||
| MMSE | 0.08 | (−0.00; 0.16) | 0.46 | 0.055 | 0.21 | −0.07 | (−0.26; 0.12) | −0.40 | ||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reguera-García, M.M.; Fernández-Baró, E.; Diez-Vega, I.; Varona-Echave, I.; Seco-Calvo, J. Explanatory Capacity of Postural Control and Physical Fitness in Cognitive Impairment and Support Needs among Individuals with Intellectual Disabilities—A Cross-Sectional Pilot Study. Brain Sci. 2023, 13, 1213. https://doi.org/10.3390/brainsci13081213
Reguera-García MM, Fernández-Baró E, Diez-Vega I, Varona-Echave I, Seco-Calvo J. Explanatory Capacity of Postural Control and Physical Fitness in Cognitive Impairment and Support Needs among Individuals with Intellectual Disabilities—A Cross-Sectional Pilot Study. Brain Sciences. 2023; 13(8):1213. https://doi.org/10.3390/brainsci13081213
Chicago/Turabian StyleReguera-García, María Mercedes, Eva Fernández-Baró, Ignacio Diez-Vega, Irene Varona-Echave, and Jesús Seco-Calvo. 2023. "Explanatory Capacity of Postural Control and Physical Fitness in Cognitive Impairment and Support Needs among Individuals with Intellectual Disabilities—A Cross-Sectional Pilot Study" Brain Sciences 13, no. 8: 1213. https://doi.org/10.3390/brainsci13081213