
Could Vulnerability to Motion Sickness and Chronic Pain Coexist within a Sensorimotor Phenotype? Insights from over 500 Pre-Pain Motion Sickness Reports

Abstract
:1. Introduction
1.1. Overlapping Processes of Motion Sickness and Pain
1.2. Neural Basis of Motion Sickness and Pain
1.3. The Sensorimotor Conflict Phenotype Hypothesis
2. Methods
2.1. Design
2.2. Subjects
2.3. Outcomes
2.4. Analysis
3. Results
3.1. Descriptive Data
3.2. Group Differences in Characteristic
3.3. Primary Analysis
3.4. Secondary Analysis
4. Discussion
Strengths, Limitations and Future Directions
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef] [PubMed]
- Moseley, G.L.; Vlaeyen, J.W. Beyond nociception: The imprecision hypothesis of chronic pain. Pain 2015, 156, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Vlaeyen, J.W.; Crombez, G.; Linton, S.J. The fear-avoidance model of pain. Pain 2016, 157, 1588–1589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, A.J. Cortical origin of pathological pain. Lancet 1999, 354, 1464–1466. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J. Pain amplification—A perspective on the how, why, when, and where of central sensitization. J. Appl. Biobehav. Res. 2018, 23, e12124. [Google Scholar] [CrossRef]
- Vittersø, A.D.; Halicka, M.; Buckingham, G.; Proulx, M.J.; Bultitude, J.H. The sensorimotor theory of pathological pain revisited. Neurosci. Biobehav. Rev. 2022, 139, 104735. [Google Scholar] [CrossRef]
- Irmak, T.; Pool, D.M.; de Winkel, K.N.; Happee, R. Validating models of sensory conflict and perception for motion sickness prediction. Biol. Cybern. 2023, 117, 185–209. [Google Scholar] [CrossRef]
- Treisman, M. Motion sickness: An evolutionary hypothesis. Science 1977, 197, 493–495. [Google Scholar] [CrossRef]
- Wolpert, D.M.; Diedrichsen, J.; Flanagan, J.R. Principles of sensorimotor learning. Nat. Rev. Neurosci. 2011, 12, 739–751. [Google Scholar] [CrossRef]
- Rothgangel, A.; Braun, S.; Winkens, B.; Beurskens, A.; Smeets, R. Traditional and augmented reality mirror therapy for patients with chronic phantom limb pain (PACT study): Results of a three-group, multicentre single-blind randomized controlled trial. Clin. Rehabil. 2018, 32, 1591–1608. [Google Scholar] [CrossRef]
- Thieme, H.; Morkisch, N.; Rietz, C.; Dohle, C.; Borgetto, B. The efficacy of movement representation techniques for treatment of limb pain—A systematic review and meta-analysis. J. Pain 2016, 17, 167–180. [Google Scholar] [CrossRef]
- Don, S.; Voogt, L.; Meeus, M.; De Kooning, M.; Nijs, J. Sensorimotor incongruence in people with musculoskeletal pain: A systematic review. Pain Pract. 2017, 17, 115–128. [Google Scholar] [CrossRef] [Green Version]
- Knudsen, L.F.; Drummond, P.D. Optokinetic stimulation increases limb pain and forehead hyperalgesia in complex regional pain syndrome. Eur. J. Pain 2015, 19, 781–788. [Google Scholar] [CrossRef] [Green Version]
- McCabe, C.S.; Cohen, H.; Blake, D.R. Somaesthetic disturbances in fibromyalgia are exaggerated by sensory–motor conflict: Implications for chronicity of the disease? Rheumatology 2007, 46, 1587–1592. [Google Scholar] [CrossRef] [Green Version]
- Legrain, V.; Iannetti, G.D.; Plaghki, L.; Mouraux, A. The pain matrix reloaded: A salience detection system for the body. Prog. Neurobiol. 2011, 93, 111–124. [Google Scholar] [CrossRef] [Green Version]
- Cohen, B.; Dai, M.; Yakushin, S.B.; Cho, C. The neural basis of motion sickness. J. Neurophysiol. 2019, 121, 973–982. [Google Scholar] [CrossRef]
- Ruscheweyh, R.; Kühnel, M.; Filippopulos, F.; Blum, B.; Eggert, T.; Straube, A. Altered experimental pain perception after cerebellar infarction. Pain 2014, 155, 1303–1312. [Google Scholar] [CrossRef]
- Mauk, M.D.; Medina, J.F.; Nores, W.L.; Ohyama, T. Cerebellar function: Coordination, learning or timing? Curr. Biol. 2000, 10, R522–R525. [Google Scholar] [CrossRef] [Green Version]
- Reeber, S.L.; Otis, T.S.; Sillitoe, R.V. New roles for the cerebellum in health and disease. Front. Syst. Neurosci. 2013, 7, 83. [Google Scholar] [CrossRef] [Green Version]
- Habas, C. Functional connectivity of the cognitive cerebellum. Front. Syst. Neurosci. 2021, 15, 27. [Google Scholar] [CrossRef]
- Mariën, P.; Paquier, P.F. A synthesis of the role of the cerebellum in cognition. Aphasiology 2005, 19, 3–19. [Google Scholar] [CrossRef]
- Mehnert, J.; May, A. Functional and structural alterations in the migraine cerebellum. J. Cereb. Blood Flow Metab. 2019, 39, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Cuomo-Granston, A.; Drummond, P.D. Migraine and motion sickness: What is the link? Prog. Neurobiol. 2010, 91, 300–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engard, N.C. LimeSurvey. Available online: http://limesurvey.org (accessed on 15 May 2015).
- Golding, J.F. Predicting individual differences in motion sickness susceptibility by questionnaire. Personal. Individ. Differ. 2006, 41, 237–248. [Google Scholar] [CrossRef]
- Soer, R.; Köke, A.J.A.; Vroomen, P.C.A.J.; Stegeman, P.; Smeets, R.J.E.M.; Coppes, M.H.; Reneman, M.F. Extensive validation of the pain disability index in 3 groups of patients with musculoskeletal pain. Spine 2013, 38, E562–E568. [Google Scholar] [CrossRef]
- Naeinian, M.R.; Shairi, M.; Sharifi, M.; Hadian, M. To study reliability and validity for a brief measure for assessing Generalized Anxiety Disorder (GAD-7). Clin. Psychol. Personal. 2011, 9, 41–50. [Google Scholar]
- Abdi, H. Holm’s sequential Bonferroni procedure. Encycl. Res. Des. 2010, 1, 1–8. [Google Scholar]
- Johnson, R.A.; Wichern, D.W. Applied Multivariate Statistical Analysis; Qatar University: Doha, Qatar, 2002. [Google Scholar]
- Paillard, A.C.; Quarck, G.; Paolino, F.; Denise, P.; Paolino, M.; Golding, J.F.; Ghulyan-Bedikian, V. Motion sickness susceptibility in healthy subjects and vestibular patients: Effects of gender, age and trait-anxiety. J. Vestib. Res. 2013, 23, 203–209. [Google Scholar] [CrossRef]
- Elbeltagy, R.; Galhom, D.; Hammad, M.; Dawa, G. Audio-vestibular dysfunction in rheumatoid arthritis: An undervalued extra-articular feature. Indian J. Otol. 2018, 24, 47–52. [Google Scholar] [CrossRef]
- Heydari, N.; Hajiabolhassan, F.; Fatahi, J.; Movaseghi, S.; Jalaie, S. Vestibular Function can be Affected by Autoimmune Processes in Rheumatoid Arthritis. Aud. Vest. Res. 2015, 24, 193–200. [Google Scholar]
- Mezhov, V.; Guymer, E.; Littlejohn, G. Central sensitivity and fibromyalgia. Intern. Med. J. 2021, 51, 1990–1998. [Google Scholar] [CrossRef]
- Chien, A.; Sterling, M. Sensory hypoaesthesia is a feature of chronic whiplash but not chronic idiopathic neck pain. Man. Ther. 2010, 15, 48–53. [Google Scholar] [CrossRef]
- Aster, H.-C.; Evdokimov, D.; Braun, A.; Üçeyler, N.; Kampf, T.; Pham, M.; Homola, G.A.; Sommer, C. CNS imaging characteristics in fibromyalgia patients with and without peripheral nerve involvement. Sci. Rep. 2022, 12, 6707. [Google Scholar] [CrossRef]
- Kim, H.; Kim, J.; Loggia, M.L.; Cahalan, C.; Garcia, R.G.; Vangel, M.G.; Wasan, A.D.; Edwards, R.R.; Napadow, V. Fibromyalgia is characterized by altered frontal and cerebellar structural covariance brain networks. NeuroImage Clin. 2015, 7, 667–677. [Google Scholar] [CrossRef] [Green Version]
- Drummond, P. Motion sickness and migraine: Optokinetic stimulation increases scalp tenderness, pain sensitivity in the fingers and photophobia. Cephalalgia 2002, 22, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Campbell, C.M.; Edwards, R.R. Mind–body interactions in pain: The neurophysiology of anxious and catastrophic pain-related thoughts. Transl. Res. 2009, 153, 97–101. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Controls | LBP | NP | WAD | RA | FMS | Migraine | Total | |
|---|---|---|---|---|---|---|---|---|
| n | 165 | 198 | 59 | 72 | 46 | 114 | 41 | 695 |
| Males | 62 | 49 | 16 | 10 | 5 | 5 | 3 | 150 |
| Females | 103 | 149 | 43 | 62 | 41 | 109 | 38 | 545 |
| Age Mean (SD) | 38 (12) | 48 (12) | 51 (12) | 45 (13) | 49 (14) | 47 (13) | 45 (12) | 46 (13) |
| Controls | LBP | NP | WAD | RA | FMS | Migraine | Total | |
|---|---|---|---|---|---|---|---|---|
| Duration (years) Mean (SD) | N/A | 13.1 (10.8) | 13.7 (11.1) | 12.0 (9.6) | 9.8 (11.4) | 12.9 (9.9) | 20.7 (12.7) | 13.3 (10.9) |
| Av. Pain Intensity 0–10 | N/A | 5.8 (2.1) | 5.7 (2.0) | 5.4 (2.1) | 5.9 (1.7) | 6.7 (1.8) | 4.5 (2.8) | 5.8 (2.1) |
| Worst Pain Intensity 0–10 | N/A | 7.8 (2.2) | 7.4 (2.4) | 7.4 (2.4) | 8.4 (1.6) | 8.7 (1.7) | 6.7 (3.4) | 7.9 (2.3) |
| GAD7 score Mean (SD) | 3.0 (3.5) | 7.0 (5.7) | 6.0 (5.2) | 6.1 (4.5) | 7.0 (5.6) | 8.3 (5.4) | 6.3 (5.1) | 6.0 (5.3) |
| PDI score Mean (SD) | N/A | 39.6 (19.3) | 39.3 (18.2) | 34.0 (20.0) | 45.7 (14.7) | 49.0 (15.4) | 37.4 (18.7) | 41.2 (18.7) |
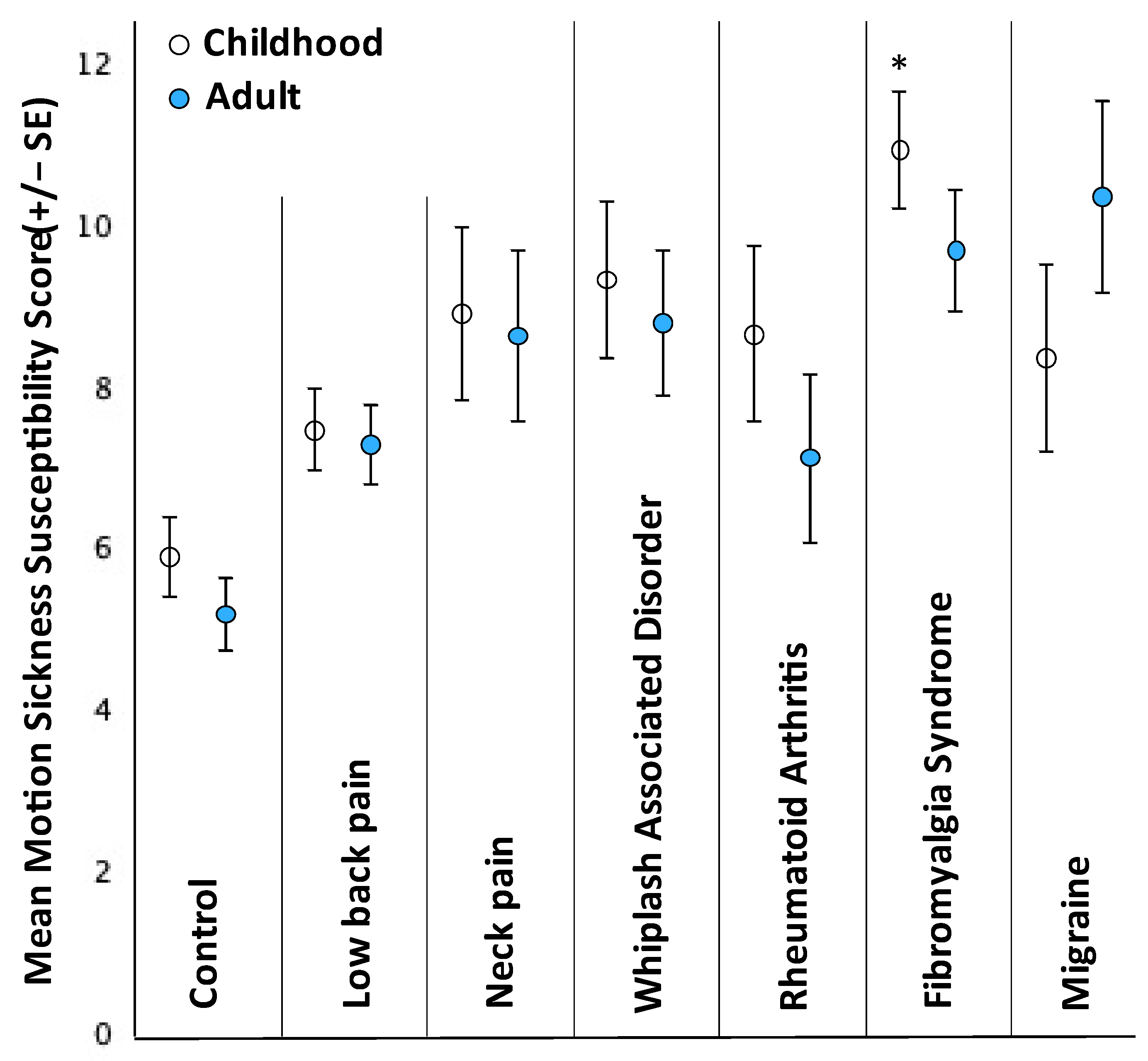
| MSSQ Child Mean (SD) | 6.0 (6.2) | 7.6 (7.3) | 8.9 (8.2) | 9.5 (8.2) | 8.8 (7.5) | 11.0 (7.8) | 8.5 (7.3) | 8.2 (7.5) |
| MSSQ Adult Mean (SD) | 5.4 (5.7) | 7.4 (6.9) | 8.8 (8.2) | 8.9 (7.6) | 7.2 (7.1) | 9.8 (8.0) | 10.5 (7.4) | 7.8 (7.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harvie, D.S. Could Vulnerability to Motion Sickness and Chronic Pain Coexist within a Sensorimotor Phenotype? Insights from over 500 Pre-Pain Motion Sickness Reports. Brain Sci. 2023, 13, 1063. https://doi.org/10.3390/brainsci13071063
Harvie DS. Could Vulnerability to Motion Sickness and Chronic Pain Coexist within a Sensorimotor Phenotype? Insights from over 500 Pre-Pain Motion Sickness Reports. Brain Sciences. 2023; 13(7):1063. https://doi.org/10.3390/brainsci13071063
Chicago/Turabian StyleHarvie, Daniel Simon. 2023. "Could Vulnerability to Motion Sickness and Chronic Pain Coexist within a Sensorimotor Phenotype? Insights from over 500 Pre-Pain Motion Sickness Reports" Brain Sciences 13, no. 7: 1063. https://doi.org/10.3390/brainsci13071063