

Adapting Neural-Based Models for Position Error Compensation in Robotic Catheter Systems
 , , , ,
, , , ,
Abstract
:Featured Application
Abstract
1. Introduction
- (1)
- The design and development of a custom 2-DOF RCS for endovascular navigation with specification analysis of its main components.
- (2)
- The experimental characterization of the slave robot’s responses to uniform and varying motion commands.
- (3)
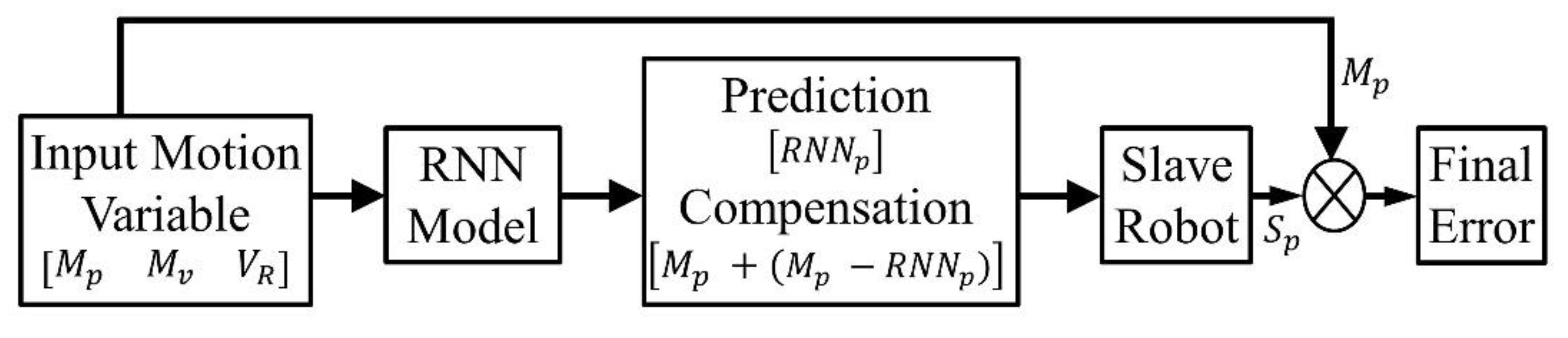
- An open-loop control model with validation of the neural-based controllers for position prediction and error compensation in the slave robot using in-silico and in-RCS experiments.
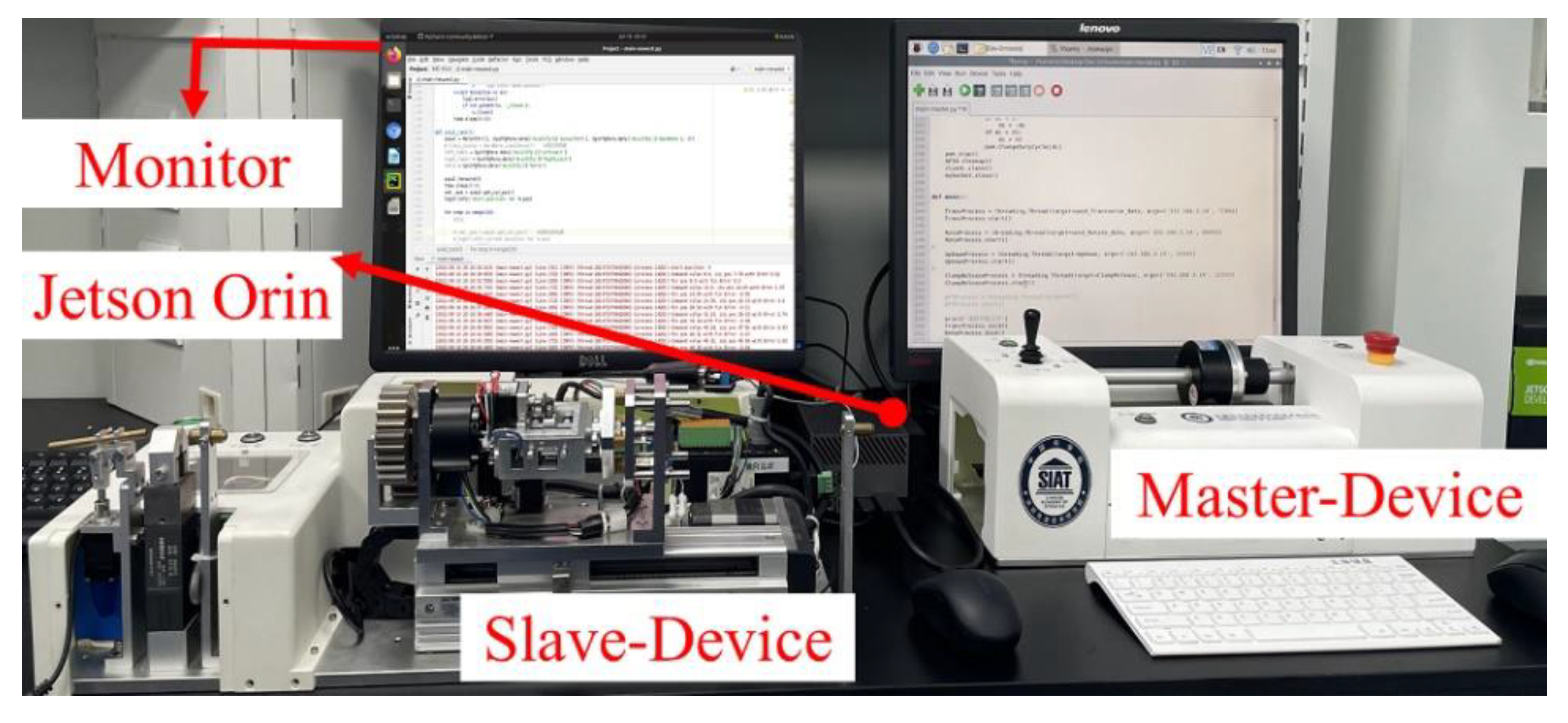
2. Design of the Robotic Catheter System
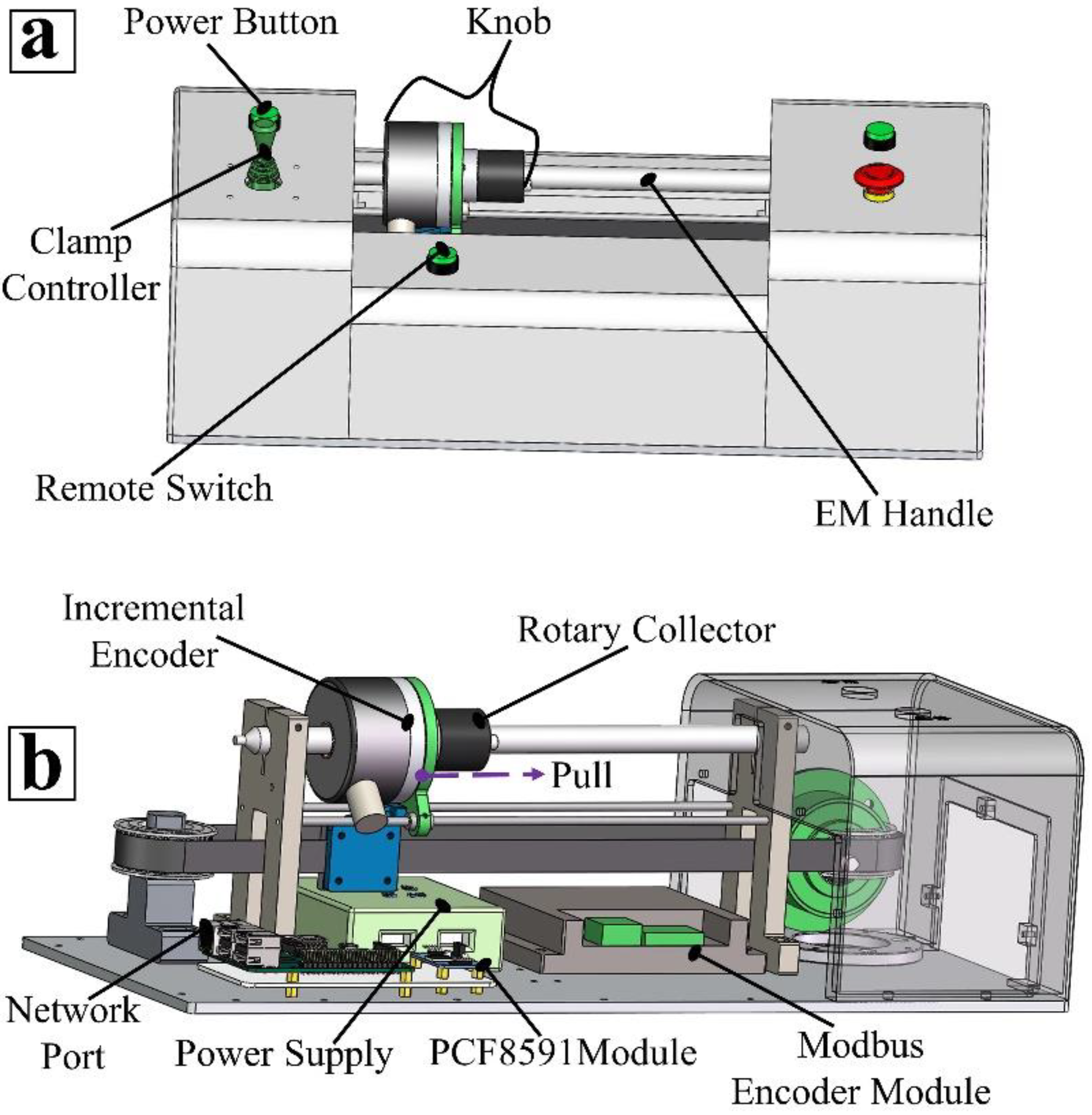
2.1. Design of the Master Robotic Device
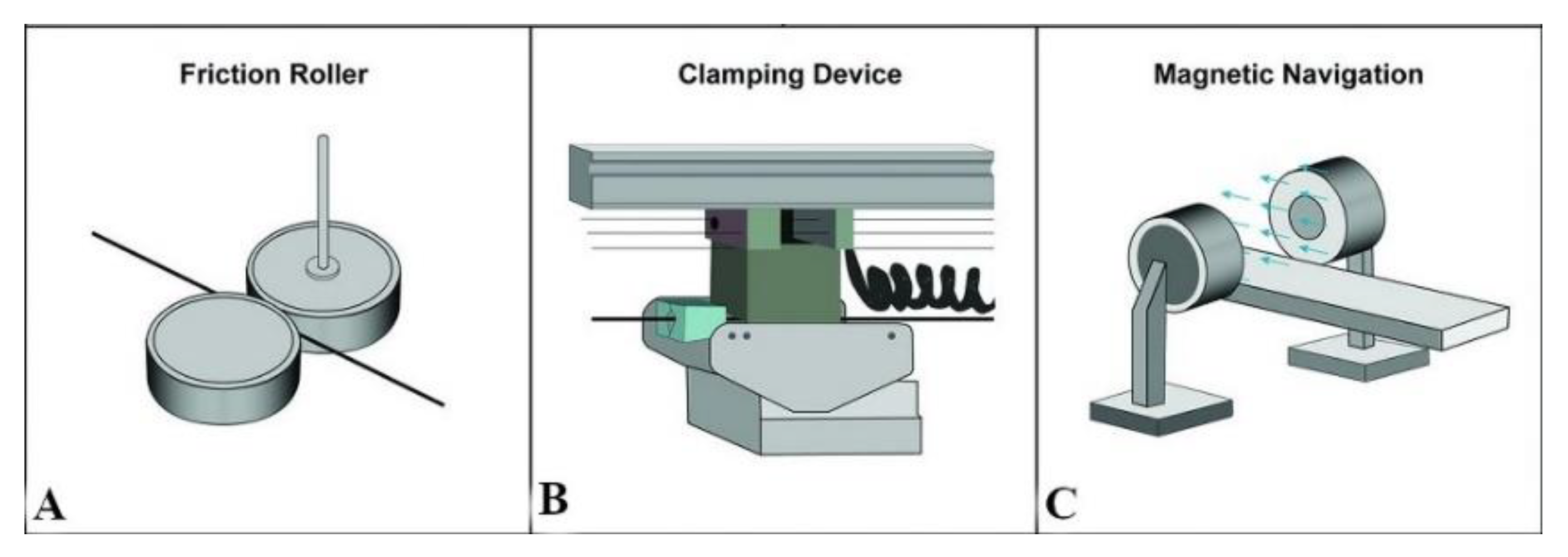
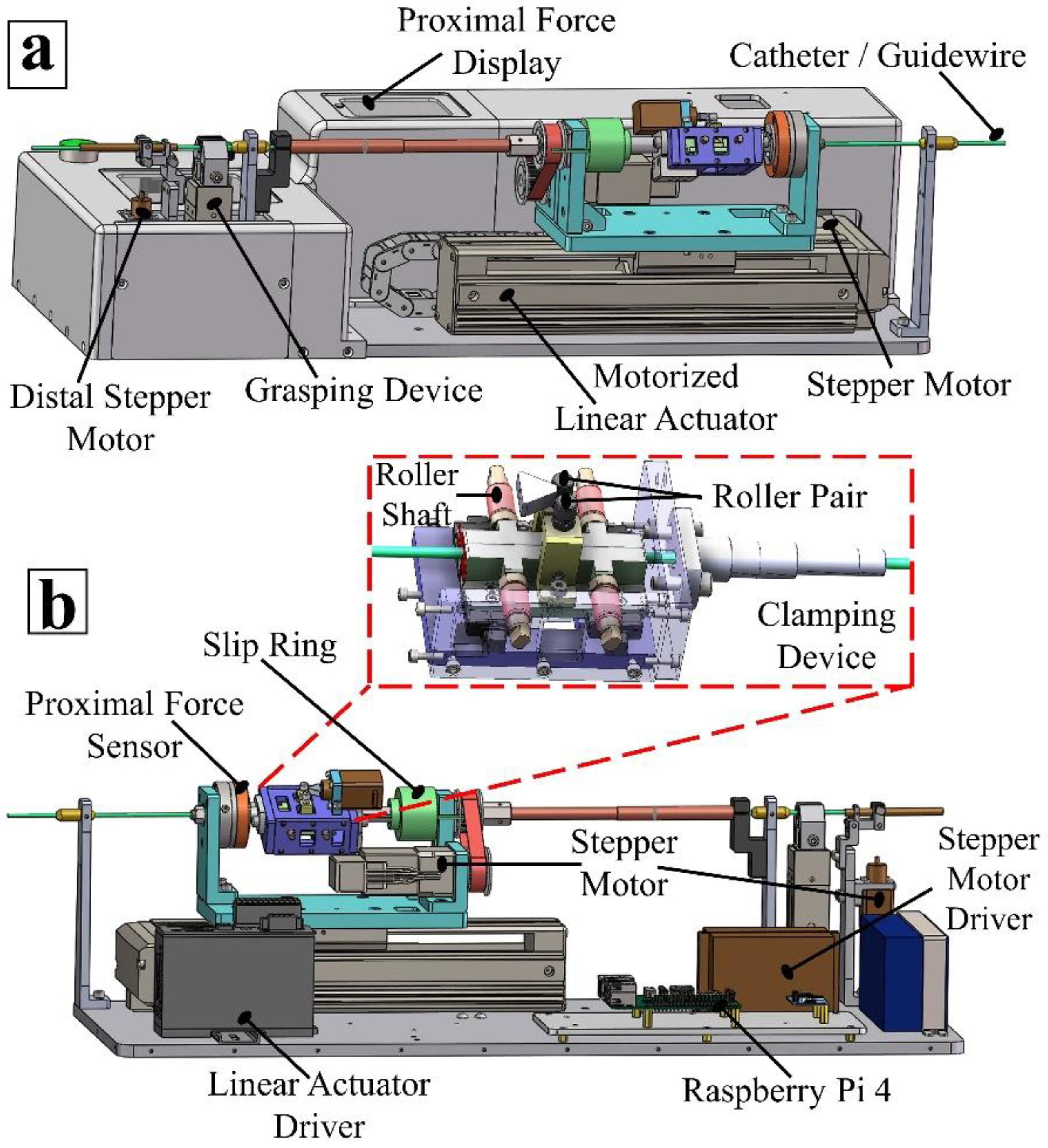
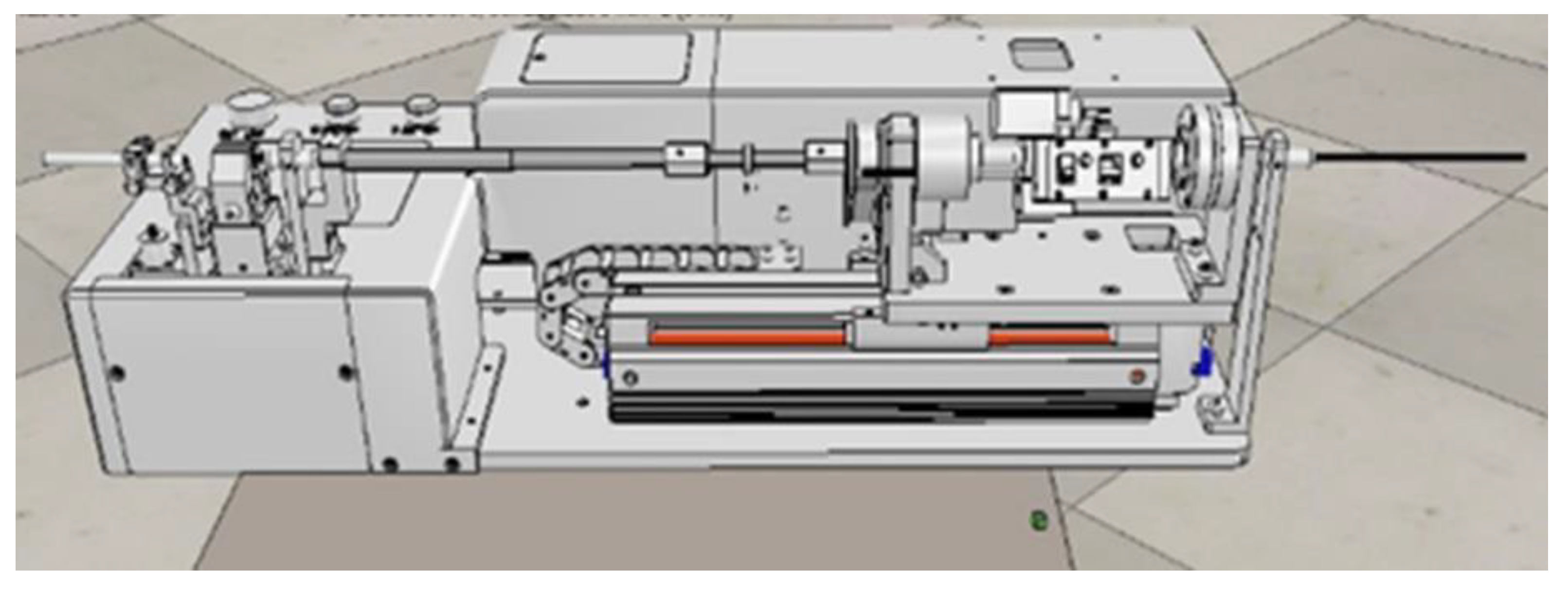
2.2. Design of the Slave Robotic Device
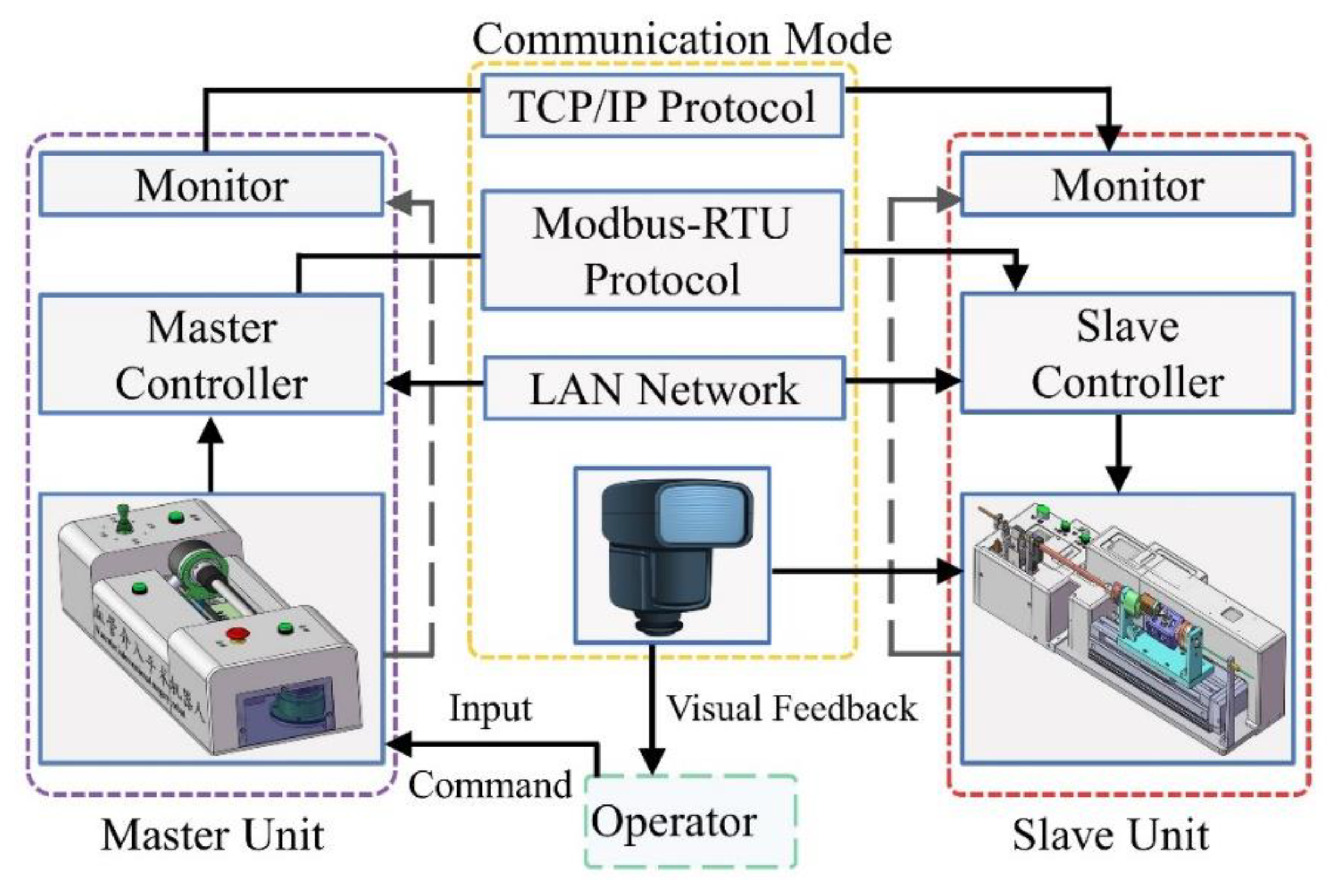
2.3. Communication Modality
3. Characterization of Position-Tracking Error in Robotic Catheter Systems
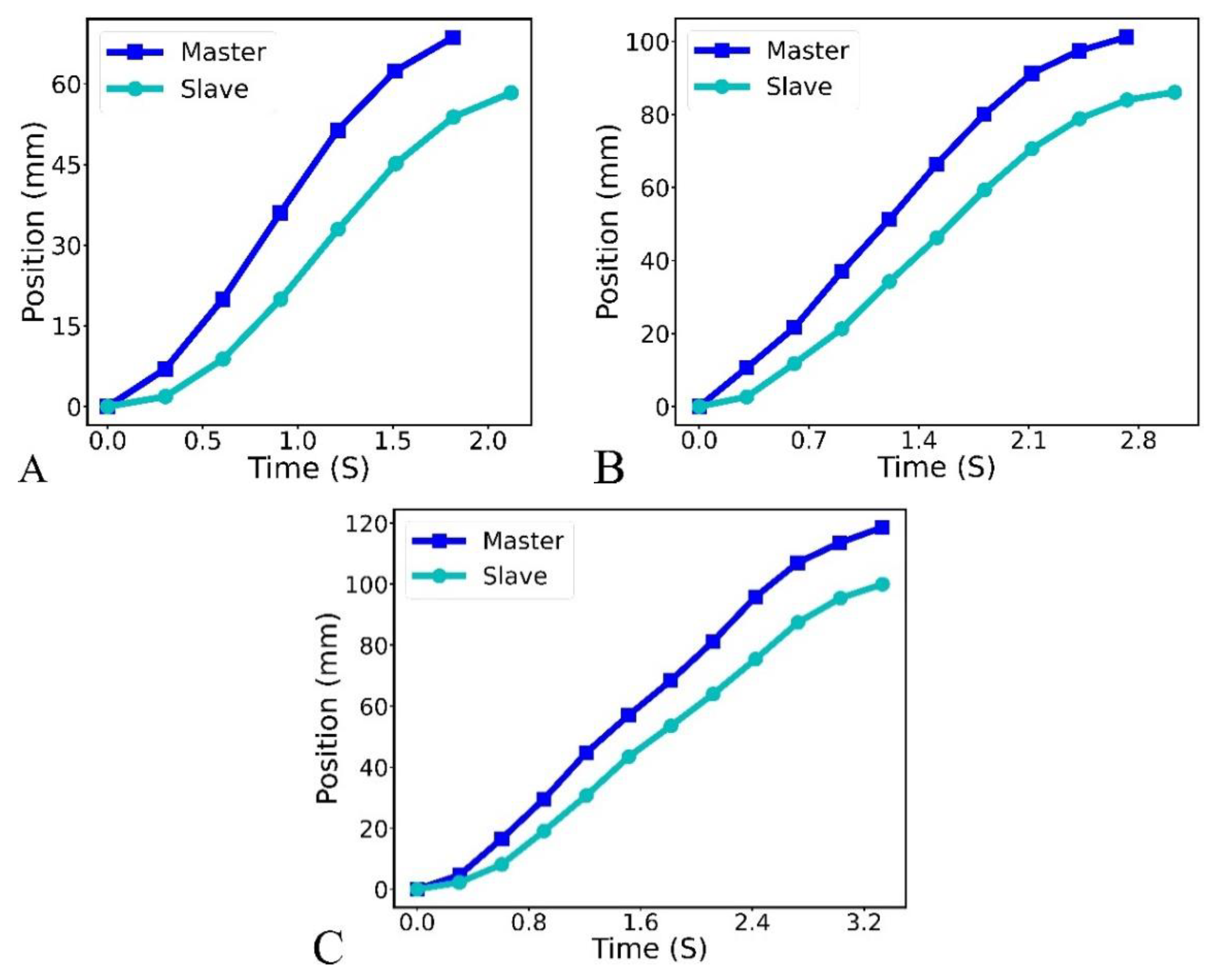
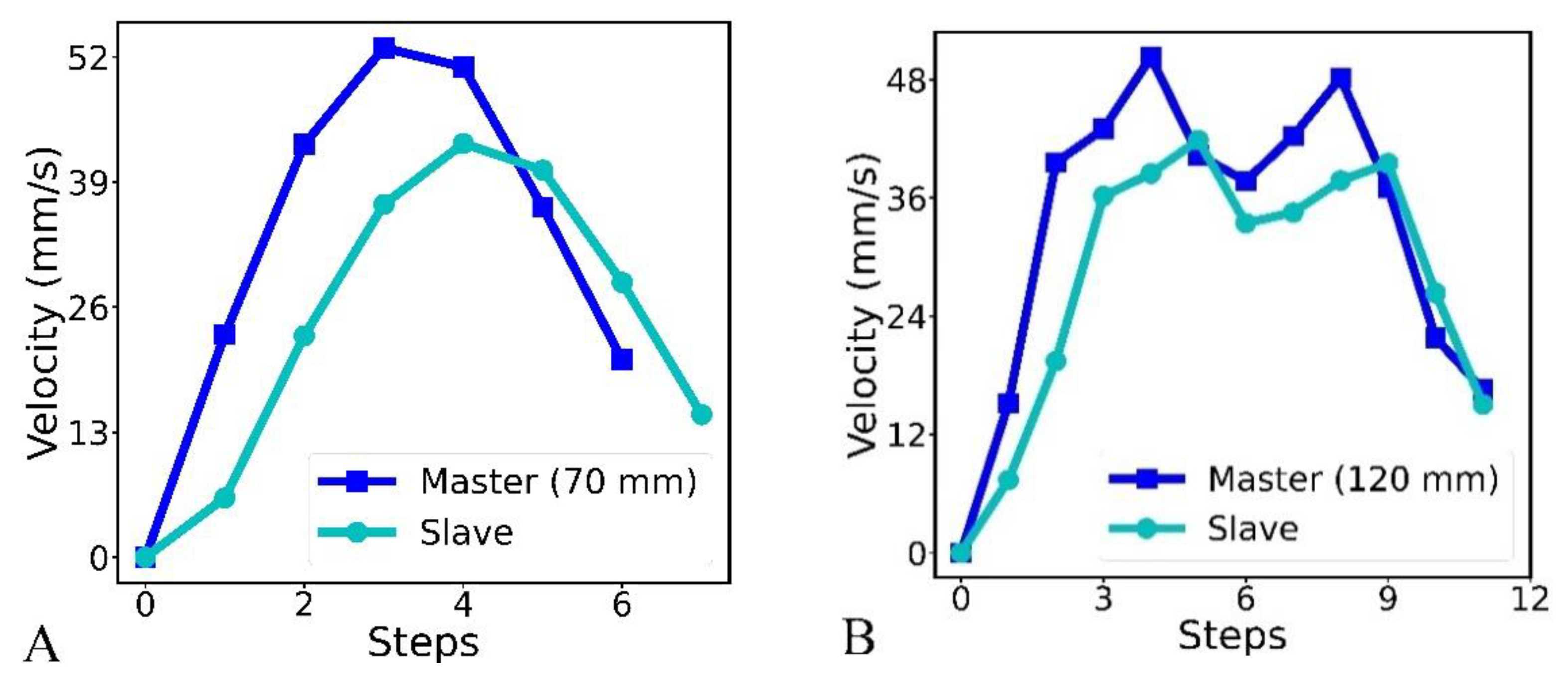
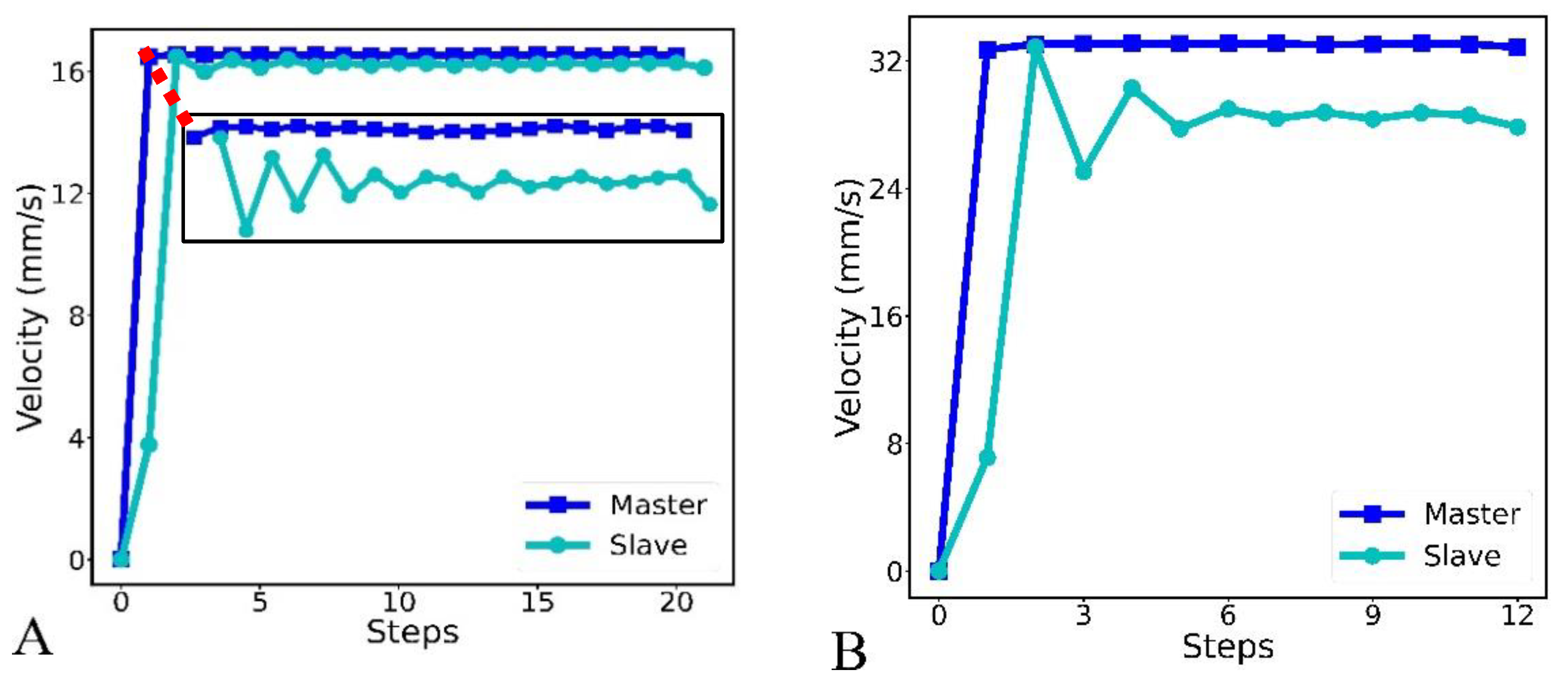
3.1. Experimental Observation of the Master–Slave Position and Velocity Based on an Operator Hand Motion
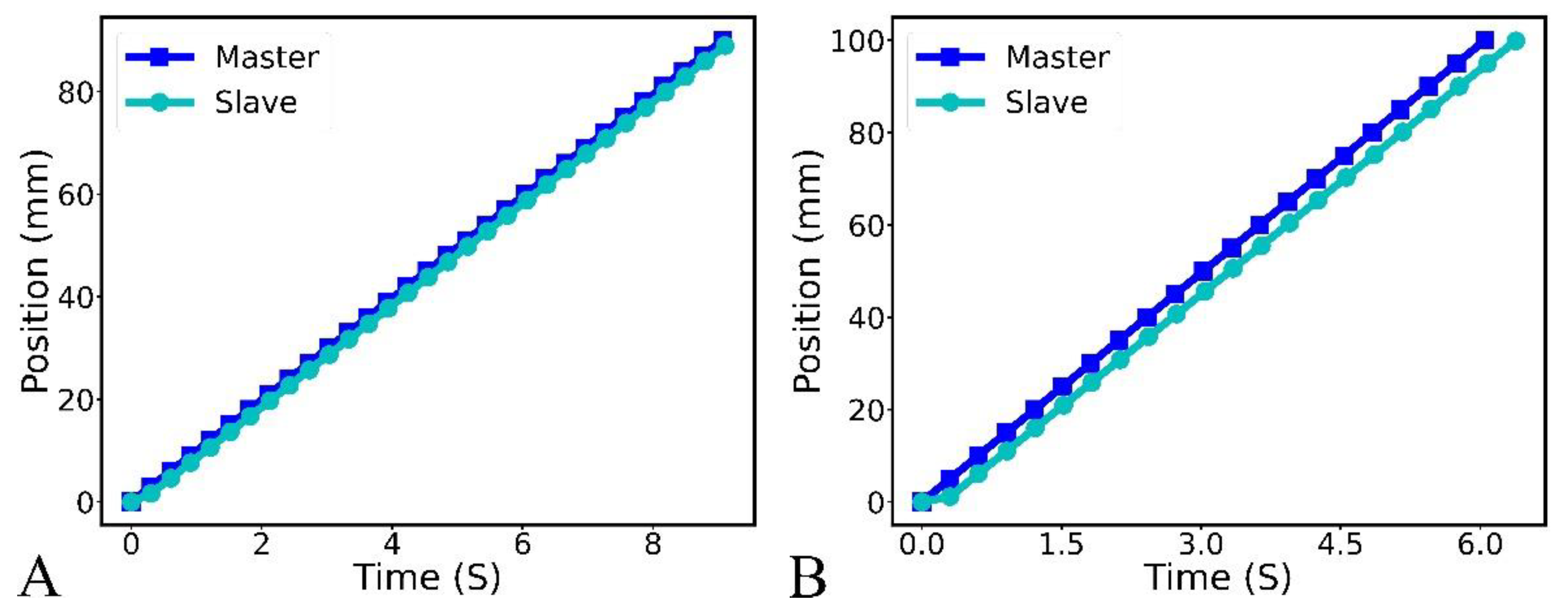
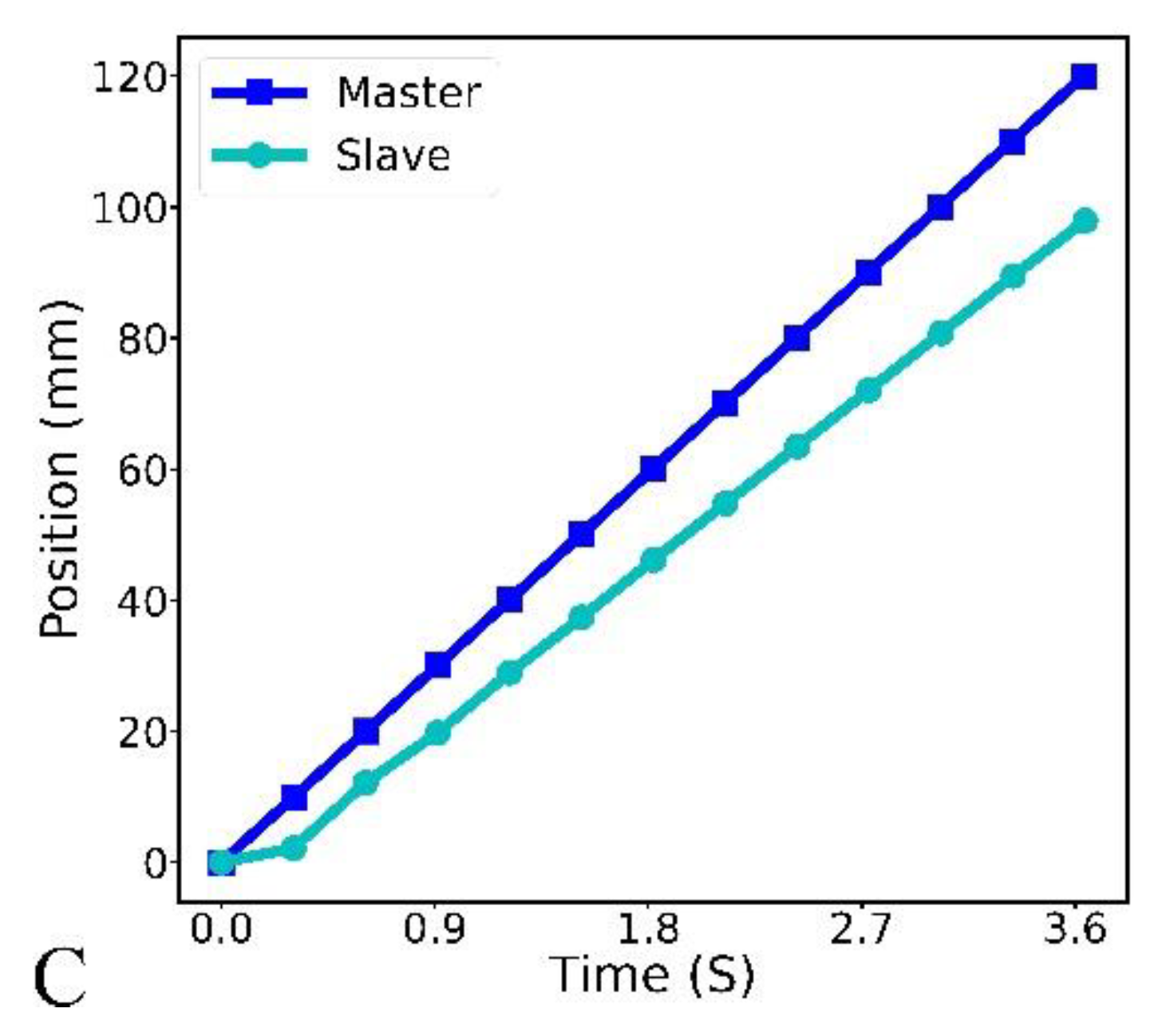
3.2. Experimental Observation of Master–Slave Position and Velocity under Uniform Translational Motion
4. Recurrent Neural Network Modeling
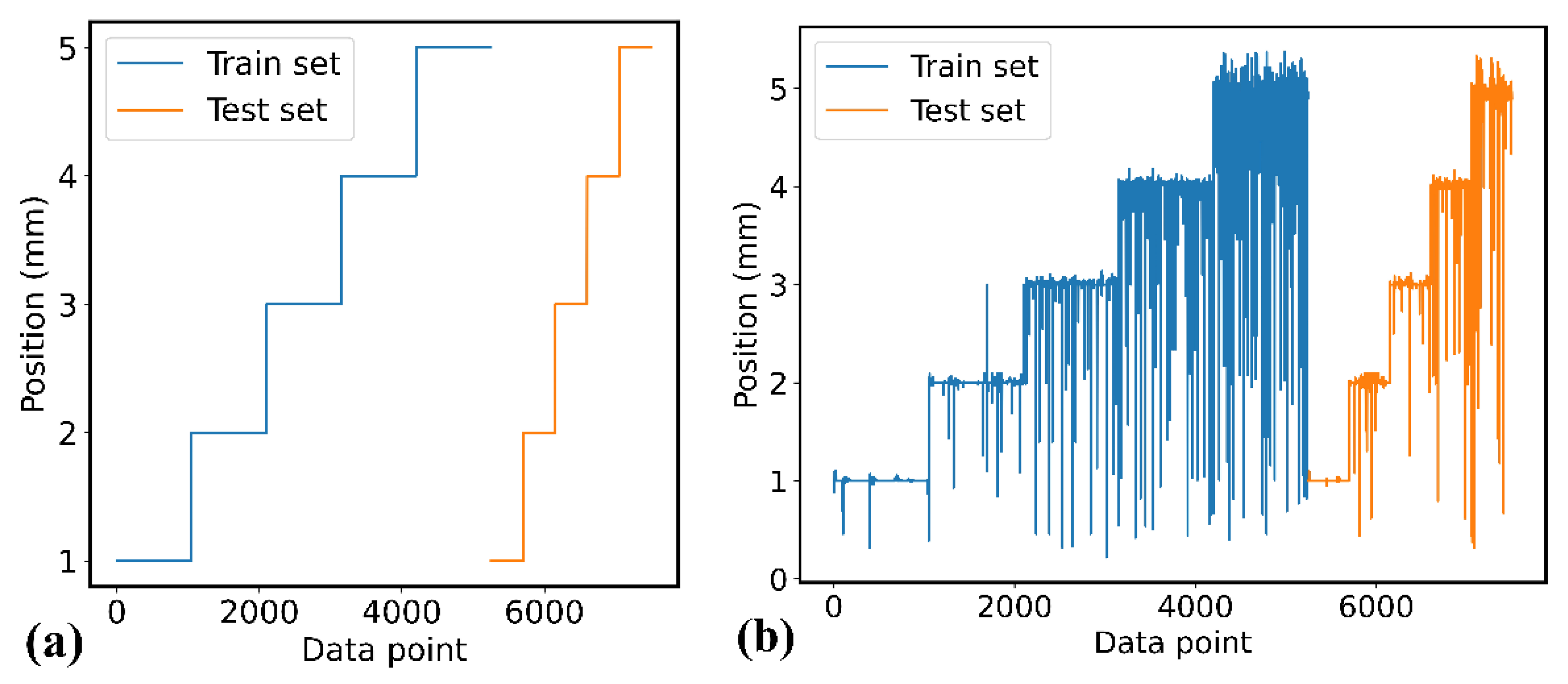
4.1. Data Pre-Processing
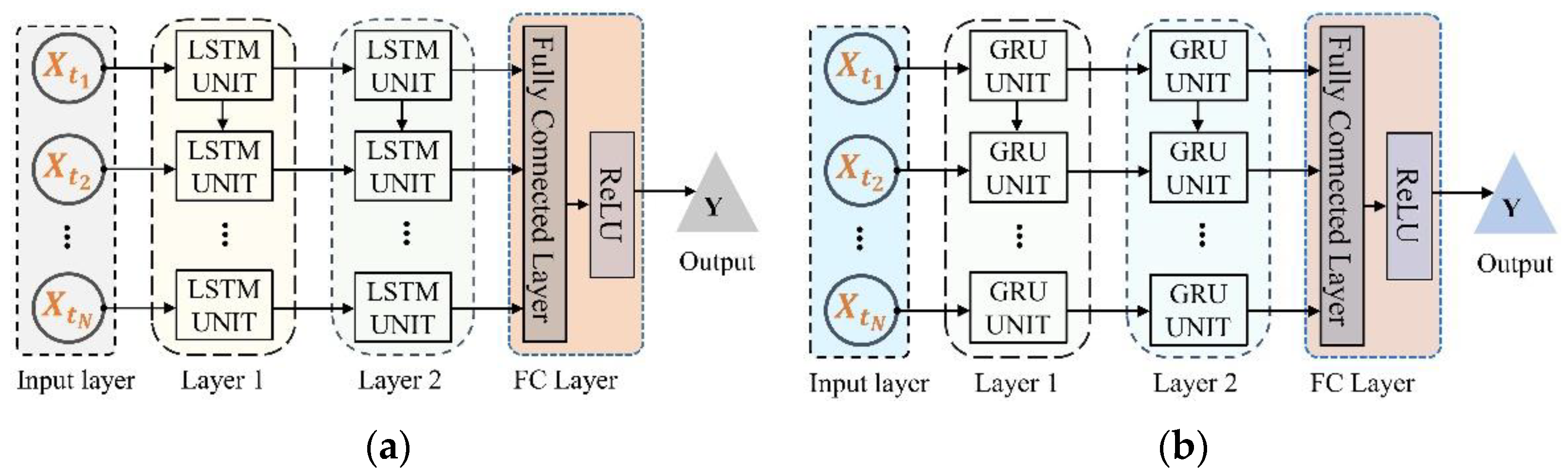
4.2. Recurrent Neural Network
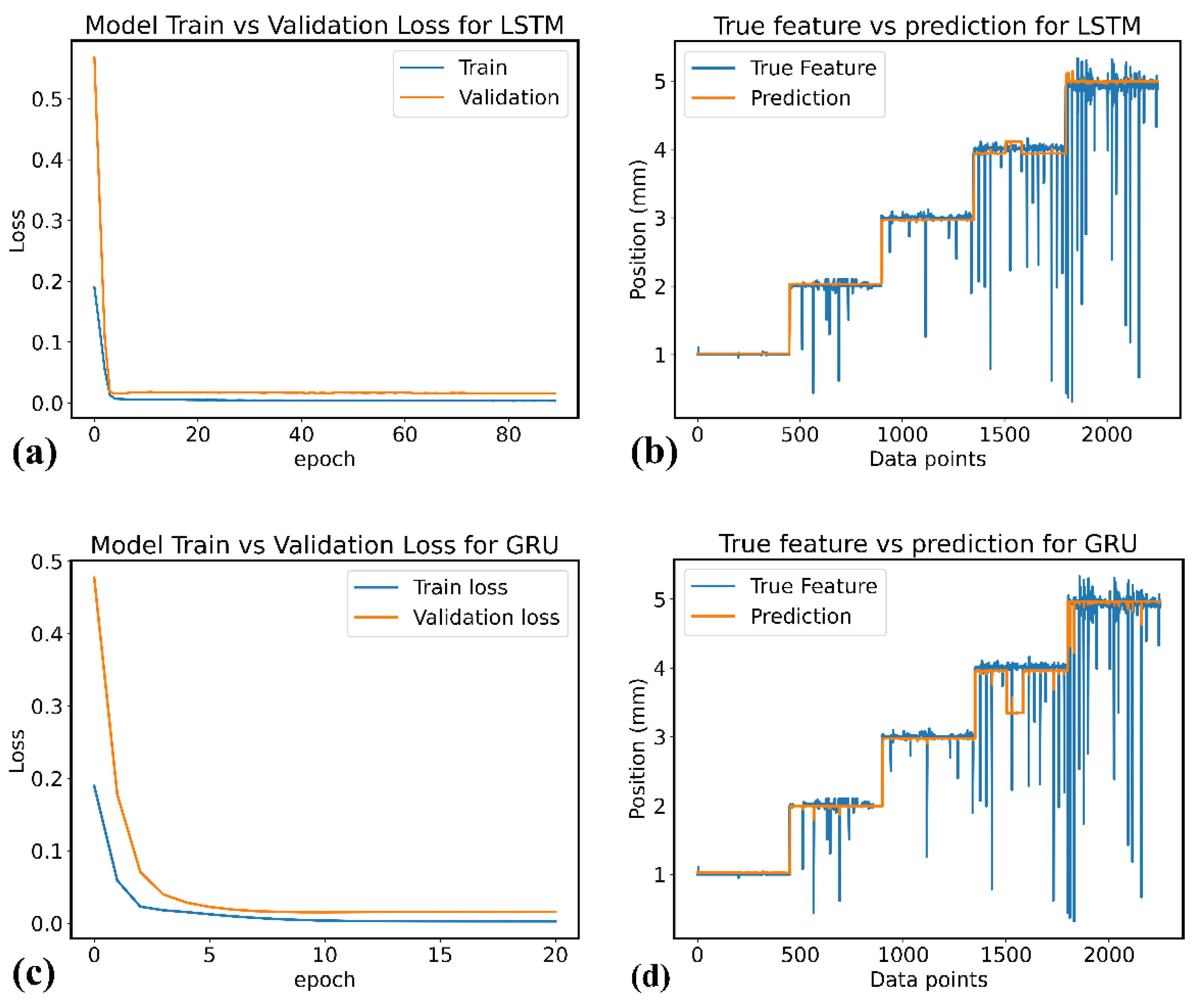
4.3. Model Training and Evaluation
- Mean Absolute Error: The mean absolute error indicates the average sum of the absolute difference between the actual slave robot position () and the predicted position (), as given in Equation (3).
- Mean Square Error: The mean square error is the average of the squared error values between the model’s prediction and the slave robot response, represented by Equation (4).
5. Experimental Study and Results
5.1. In-Silico Modeling and Evaluation
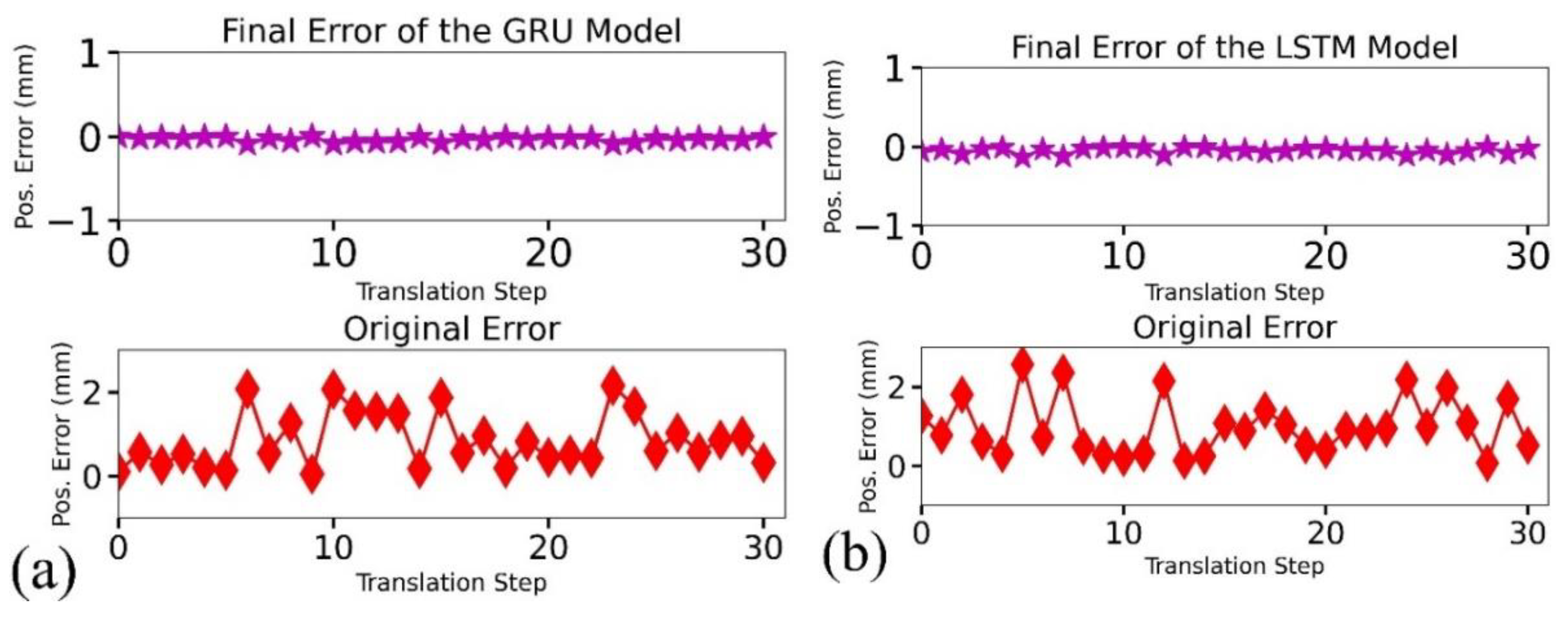
5.2. In-Silico Results and Evaluation
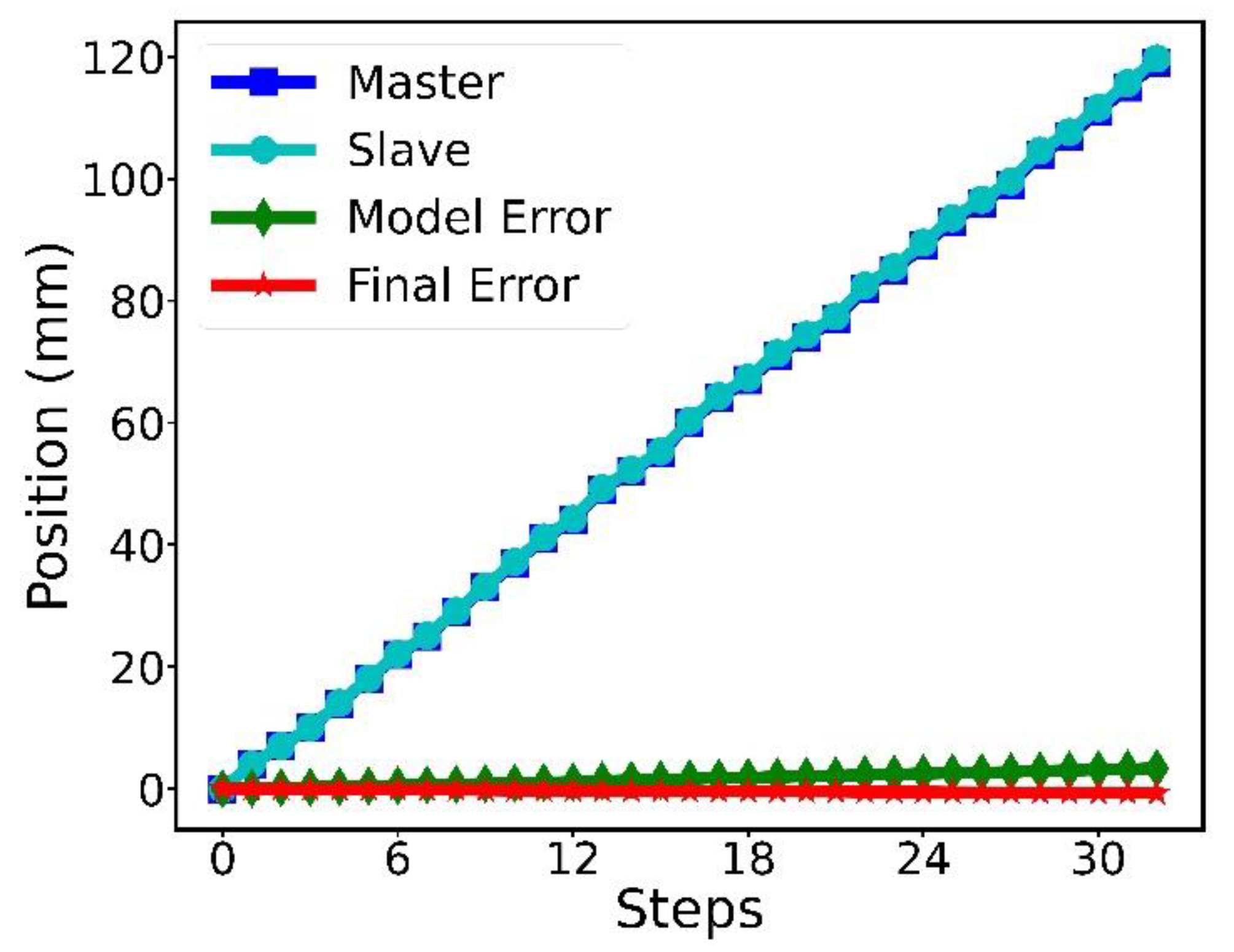
5.3. In-RCS Results and Evaluation
6. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update A Report from the American Heart Association. Circulation 2021, 143, E254–E743. [Google Scholar] [CrossRef]
- Gatto, L.; Prati, F. Subclinical atherosclerosis: How and when to treat it? Eur. Hear. J. Suppl. 2020, 22, E87–E90. [Google Scholar] [CrossRef]
- Cohn, W.E.; Frazier, O.H.; Mallidi, H.R.; Cooley, D.A. Coronary Artery Disease, Cardiovascular Medicine; Willerson, J.T., Holmes, D.R., Jr., Eds.; Springer: London, UK, 2015; p. 657. [Google Scholar] [CrossRef]
- Akinyemi, T.O.; Omisore, O.M.; Duan, W.; Lu, G.; Al-Handerish, Y.; Han, S.; Wang, L. Fiber Bragg Grating-Based Force Sensing in Robot-Assisted Cardiac Interventions: A Review. IEEE Sens. J. 2021, 21, 10317–10331. [Google Scholar] [CrossRef]
- Watson, T.J.; Ong, P.J.L.; Tcheng, J.E. Primary Angioplasty: A Practical Guide; Springer: Singapore, 2018. [Google Scholar]
- Bergman, P.; Blacker, S.J.; Kottenstette, N.; Saber, O.; Sokhanvar, S. Robotic-Assisted Percutaneous Coronary Intervention. In Handbook of Robotic and Image-Guided Surgery; Elsevier: Amsterdam, The Netherlands, 2020; pp. 341–362. [Google Scholar]
- Akinyemi, T.O.; Omisore, O.M.; Duan, W.; Lu, G.; Du, W.; Alhanderish, Y.; Li, Y.; Wang, L. Development of a Millinewton FBG-Based Distal Force Sensor for Intravascular Interventions. In Proceedings of the 16th International Conference on Control, Automation, Robotics and Vision (ICARCV), Shenzhen, China, 13–15 December 2020; IEEE: New York, NY, USA, 2021; pp. 511–515. [Google Scholar] [CrossRef]
- Kalra, A.; Bhatt, D.L.; Kleiman, N.S. A 24-Month Interventional Cardiology Fellowship: Learning Motor Skills Through Blocked Repetition. JACC Cardiovasc. Interv. 2017, 10, 210–211. [Google Scholar] [CrossRef]
- Lee, C.W.J.; Rao, A. Current training in Cardiac devices–a Cardiology trainee perspective: A questionnaire survey. MedEdPublish 2017, 6, 130. [Google Scholar]
- Omisore, O.M.; Akinyemi, T.; Duan, W.; Wang, L. A Novel Sample-efficient Deep Reinforcement Learning with Episodic Policy Transfer for PID-Based Control in Cardiac Catheterization Robots. October 2021. Available online: http://arxiv.org/abs/2110.14941 (accessed on 1 June 2022).
- Kinnaird, T.; Kwok, C.S.; Kontopantelis, E.; Ossei-Gerning, N.; Ludman, P.; de Belder, M.; Andreson, R.; Mamas, M.A. Incidence, determinants, and outcomes of coronary perforation during percutaneous coronary intervention in the United Kingdom Between 2006 and 2013. Circ. Cardiovasc. Interv. 2016, 9, e003449. [Google Scholar] [CrossRef]
- Omisore, O.M.; Duan, W.; Akinyemi, T.; Han, S.; Du, W.; Alhanderish, Y.; Wang, L. Design of a Master-Slave Robotic System for Intravascular Catheterization during Cardiac Interventions. In Proceedings of the International Conference on Control, Automation, Robotics and Vision (ICARCV), Shenzhen, China, 13–15 December 2020; IEEE: New York, NY, USA, 2021; pp. 996–1000. [Google Scholar]
- Weisz, G.; Metzger, D.C.; Caputo, R.P.; Delgado, J.A.; Marshall, J.J.; Vetrovec, G.W.; Reisman, M.; Waksman, R.; Granada, J.F.; Novack, V.; et al. Safety and feasibility of robotic percutaneous coronary intervention: PRECISE (percutaneous robotically-enhanced coronary intervention) study. J. Am. Coll. Cardiol. 2013, 61, 1596–1600. [Google Scholar] [CrossRef] [Green Version]
- Smitson, C.C.; Ang, L.; Pourdjabbar, A.; Reeves, R.; Patel, M.; Mahmud, E. Safety and feasibility of a novel, second-generation robotic-assisted system for percutaneous coronary intervention: First in-human report. J. Invasive Cardiol. 2018, 30, 152–156. [Google Scholar] [CrossRef]
- CorPath GRX System Operator’s Manual. Available online: https://www.roboticpci.com/assets/Documents/150-07702_Rev_C_CorPath_GRX_Operator’s_Manual.pdf (accessed on 31 August 2022).
- Dupont, P.E.; Nelson, B.J.; Goldfarb, M.; Hannaford, B.; Menciassi, A.; O’Malley, M.K.; Simaan, N.; Valdastri, P.; Yang, G.Z. A decade retrospective of medical robotics research from 2010 to 2020. Sci. Robot. 2021, 6, 8017. [Google Scholar] [CrossRef]
- Akinyemi, T.O.; Omisore, O.M.; Duan, W.; Lu, G.; Al-Handerish, Y.; Han, S.; Wang, L. Towards a Fiber Bragg Grating-Based Force Sensing in Robot-Assisted Cardiac Interventions. IEEE Sens. Lett. 2022, 21, 5000104. [Google Scholar] [CrossRef]
- Al-Ahmad, O.; Ourak, M.; Smits, J.; Jeanquart, S.; Deserranno, N.; Bernhard, F.; Kassahun, Y.; Yu, B.; Vander Poorten, E. Development of an Innovative Sleeve-Based Robotic Catheter Driver. In Proceedings of the 8th Joint Workshop on New Technologies for Computer/Robot Assisted Surgery, London, UK, 10–11 September 2018; pp. 2–3. [Google Scholar]
- Payne, C.J.; Rafii-Tari, H.; Yang, G.-Z. A force feedback system for Endovascular catheterization. In Proceedings of the International Conference on Intelligent Robots and Systems, Vilamoura-Algarve, Portugal, 7–12 October 2012; IEEE: New York, NY, USA, 2012; pp. 1298–1304. [Google Scholar]
- Cha, H.J.; Yi, B.J.; Won, J.Y. An assembly-type master-slave catheter and guidewire driving system for vascular intervention. Proc. Inst. Mech. Eng. H 2017, 231, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Thakur, Y.; Bax, J.S.; Holdsworth, D.W.; Drangova, M. Design and performance evaluation of a remote catheter navigation system. IEEE Trans. Biomed. Eng. 2009, 56, 1901–1908. [Google Scholar] [CrossRef] [PubMed]
- Richter, F.; Orosco, R.K.; Yip, M.C. Motion scaling solutions for improved performance in high delay surgical teleoperation. In Proceedings of the International Conference on Robotics and Automation Montreal, Montreal, QC, Canada, 20–24 May 2019; IEEE: New York, NY, USA, 2019; pp. 1590–1595. [Google Scholar]
- Sankaran, N.K.; Chembrammel, P.; Siddiqui, A.; Snyder, K.; Kesavadas, T. Design and Development of Surgeon Augmented Endovascular Robotic System. IEEE Trans. Biomed. Eng. 2018, 65, 2483–2493. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Zhou, J.; Zhang, X.; Zhou, Q. Development of a Robotic Catheter Manipulation System Based on BP Neural Network PID Controller. Appl. Bionics Biomech. 2020, 2020, 8870106. [Google Scholar] [CrossRef] [PubMed]
- Guo, J.; Jin, X.; Guo, S.; Du, W. Study on the tracking performance of the vascular interventional surgical robotic system based on the fuzzy-PID controller. In Proceedings of the International Conference on Mechatronics and Automation (ICMA), Takamatsu, Japan, 6–9 August 2017; IEEE: New York, NY, USA, 2017; pp. 29–34. [Google Scholar]
- Omisore, O.M.; Han, S.; Ren, L.; Wang, L. A fuzzy-PD model for master-slave tracking in teleoperated robotic surgery. In Proceedings of the Biomedical Circuits and Systems Conference, Shanghai, China, 17–19 October 2016; IEEE: New York, NY, USA, 2017. [Google Scholar]
- Omisore, O.M.; Han, S.P.; Ren, L.X.; Wang, G.S.; Ou, F.L.; Li, H.; Wang, L. Towards Characterization and Adaptive Compensation of Backlash in a Novel Robotic Catheter System for Cardiovascular Interventions. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 824–838. [Google Scholar] [CrossRef]
- Wang, H.; Chang, J.; Yu, H.; Liu, H.; Hou, C.; Lu, H. Research on a Novel Vascular Interventional Surgery Robot and Control Method Based on Precise Delivery. IEEE Access 2021, 9, 26568–26582. [Google Scholar] [CrossRef]
- Yu, H.; Wang, H.; Chang, J.; Niu, J.; Wang, F.; Yan, Y.; Tian, H.; Fang, J.; Lu, H. A Novel Vascular Intervention Surgical Robot Based on Force Feedback and Flexible Clamping. App. Sci. 2021, 11, 611. [Google Scholar] [CrossRef]
- Guo, S.; Song, Y.; Yin, X.; Zhang, L.; Tamiya, T.; Hirata, H.; Ishihara, H. A novel robot-assisted endovascular catheterization system with haptic force feedback. IEEE Trans. Robot. 2019, 35, 685–696. [Google Scholar] [CrossRef]
- Hasanzadeh, S.; Janabi-Sharifi, F.; Keenan, P. Backlash characterization and position control of a robotic catheter manipulator using experimentally-based kinematic model. Mechatronics 2017, 44, 94–106. [Google Scholar] [CrossRef]
- Omisore, O.M.; Han, S.; Zhou, T.; Al-Handarish, Y.; Du, W.; Ivanov, K.; Wang, L. Learning-based Parameter Estimation for Hysteresis Modeling in Robotic Catheterization. In Proceedings of the 41st IEEE Conference of Engineering in Medicine and Biology Society, Berlin, Germany, 23–27 July 2019; IEEE: New York, NY, USA, 2019; pp. 5399–5402. [Google Scholar]
- Beaman, C.B.; Kaneko, N.; Meyers, P.M.; Tateshima, S. A review of robotic interventional neuroradiology. Am. J. Neuroradiol. 2021, 42, 808–814. [Google Scholar] [CrossRef]
- Bai, W.; Cursi, F.; Guo, X.; Huang, B.; Lo, B.; Yang, G.Z.; Yeatman, E.M. Task-Based LSTM Kinematic Modeling for a Tendon-Driven Flexible Surgical Robot. IEEE Trans. Med. Robot. Bionics 2022, 4, 339–342. [Google Scholar] [CrossRef]
- Wu, D.; Zhang, Y.; Ourak, M.; Niu, K.; Dankelman, J.; Vander Poorten, E. Hysteresis Modeling of Robotic Catheters Based on Long Short-Term Memory Network for Improved Environment Reconstruction. IEEE Rob. Autom Lett. 2021, 6, 2106–2113. [Google Scholar] [CrossRef]
- Cursi, F.; Bai, W.; Yeatman, E.M.; Kormushev, P. Model Learning With Backlash Compensation for a Tendon-Driven Surgical Robot. IEEE Rob. Autom. Lett. 2022, 7, 7958–7965. [Google Scholar] [CrossRef]
- Choi, J.; Park, S.; Kim, Y.H.; Moon, Y.; Choi, J. A vascular intervention assist device using bi-motional roller cartridge structure and clinical evaluation. Biosensors 2021, 11, 329. [Google Scholar] [CrossRef] [PubMed]
- Józefowicz, R.; Zaremba, W.; Sutskever, I. An Empirical Exploration of Recurrent Network Architectures. In Proceedings of the 32nd International Conference on Machine Learning, ICML, Lille, France, 6–11 July 2015; JMLR: Massuchesetts, MA, USA; pp. 2342–2350. [Google Scholar]
- Cho, K.; Van Merriënboer, B.; Bahdanau, D.; Bengio, Y. On the properties of neural machine translation: Encoder-decoder approaches. arXiv 2014, arXiv:1409.1259. [Google Scholar]
- Zhou, W.; Guo, S.; Guo, J.; Meng, F.; Chen, Z. ADRC-Based Control Method for the Vascular Intervention Master–Slave Surgical Robotic System. Micromachines 2021, 12, 1439. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Distance (mm) | Error (mm) | Resultant Error (%) |
|---|---|---|
| 30 | 3.84 2.03 | 19.90 |
| 45 | 6.38 2.30 | 14.83 |
| 70 | 7.43 3.72 | 14.66 |
| 100 | 10.67 4.30 | 15.11 |
| 120 | 13.14 6.11 | 15.51 |
| Model | MAE (mm) | MSE (mm2) |
|---|---|---|
| LSTM | 0.0825 | 0.0958 |
| GRU | 0.0906 | 0.0964 |
| Authors | Control Method | Experiment Type | Max. Error (mm) |
|---|---|---|---|
| Ma et al. [24] | MLP-PID | Simulation/in-RCS | 1.50 |
| Omisore et al. [10] | RL-PID | Simulation | 0.003 |
| Zhou et al. [40] | ADRC | RCS | 0.87 |
| Wang et al. [28] | FSMC | Simulation | 0.65 |
| This study | LSTM/GRU | Simulation/in-RCS | 0.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akinyemi, T.O.; Omisore, O.M.; Chen, X.; Duan, W.; Du, W.; Yi, G.; Wang, L. Adapting Neural-Based Models for Position Error Compensation in Robotic Catheter Systems. Appl. Sci. 2022, 12, 10936. https://doi.org/10.3390/app122110936
Akinyemi TO, Omisore OM, Chen X, Duan W, Du W, Yi G, Wang L. Adapting Neural-Based Models for Position Error Compensation in Robotic Catheter Systems. Applied Sciences. 2022; 12(21):10936. https://doi.org/10.3390/app122110936
Chicago/Turabian StyleAkinyemi, Toluwanimi O., Olatunji M. Omisore, Xingyu Chen, Wenke Duan, Wenjing Du, Guanlin Yi, and Lei Wang. 2022. "Adapting Neural-Based Models for Position Error Compensation in Robotic Catheter Systems" Applied Sciences 12, no. 21: 10936. https://doi.org/10.3390/app122110936