

Treatment of Palatally Displaced Canines Using Miniscrews for Direct or Indirect Anchorage: A Three-Dimensional Prospective Cohort Study on Tooth Movement Speed

Abstract
:1. Introduction
2. Materials and Methods
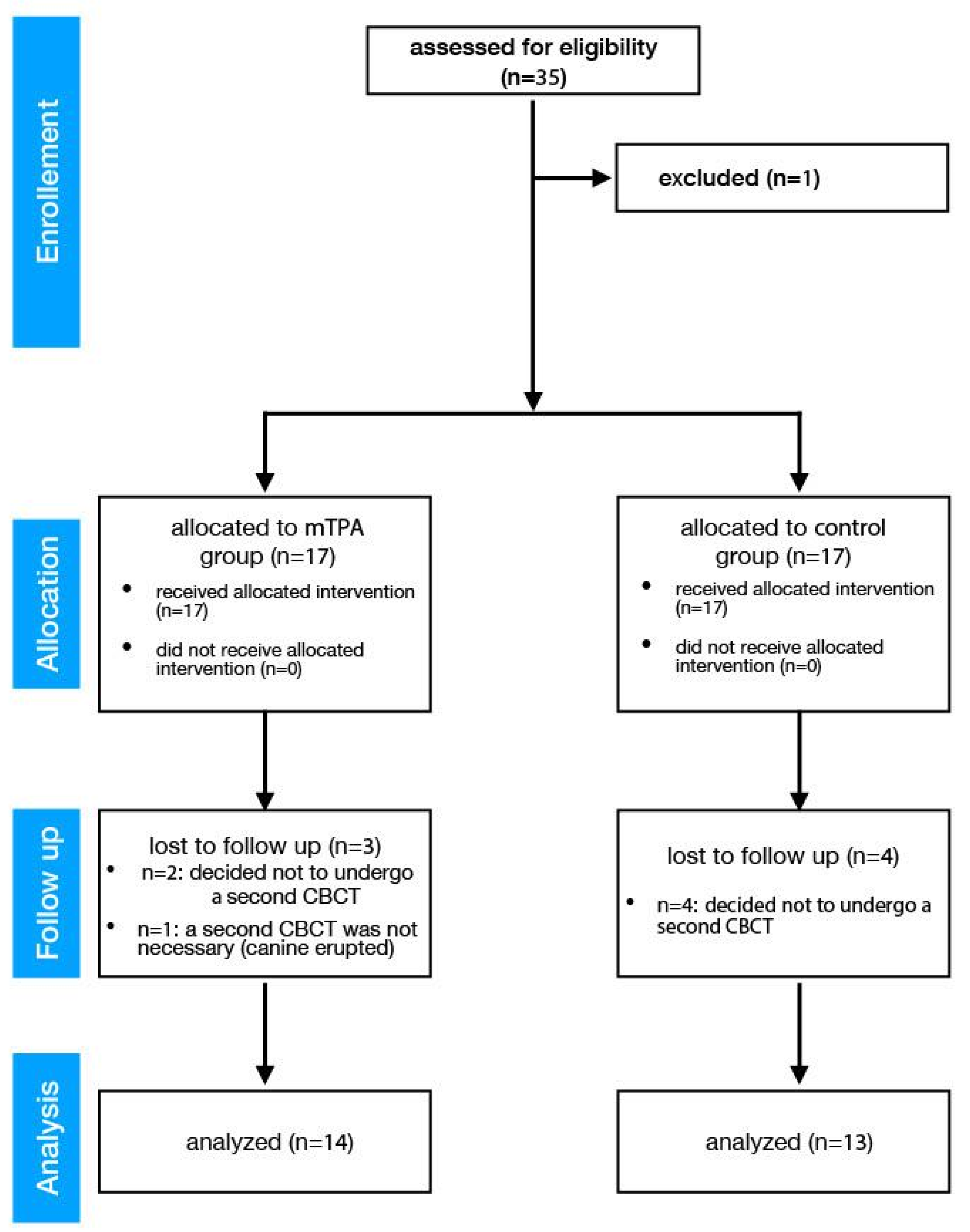
2.1. Prospective Controlled Study
2.2. Population
- Patients of both sexes aged between 12 and 30 years;
- Presence of one or two palatal maxillary impacted canines, with the need for surgical exposure and orthodontic treatment.
- Presence of periodontal disease;
- Patients with systemic diseases such as arthritis, diabetes, etc.;
- Pregnant patients;
- Previous orthodontic treatment;
- Smokers.
2.3. Intervention
2.4. Comparison
2.4.1. Test Group (Indirect Anchorage)
2.4.2. Control Group (Direct Anchorage)
2.4.3. Evaluation of the Results
2.5. Sample Size
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. Limits of the Study
4.2. Interpretation and Generalizability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oberoi, S.; Knueppel, S. Three-dimensional assessment of impacted canines and root resorption using cone beam computed tomography. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Fleming, P.S.; Sharma, P.K.; DiBiase, A.T. How to … mechanically erupt a palatal canine. J. Orthod. 2010, 37, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Sinha, P.K.; Nanda, R.S. Management of impacted maxillary canines using mandibular anchorage. Am. J. Orthod. Dentofac. Orthop. 1999, 115, 254–257. [Google Scholar] [CrossRef]
- Schmidt, A.D.; Kokich, V.G. Periodontal response to early uncovering, autonomous eruption, and orthodontic alignment of palatally impacted maxillary canines. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 449–455. [Google Scholar] [CrossRef] [PubMed]
- Dekel, E.; Nucci, L.; Weill, T.; Flores-Mir, C.; Becker, A.; Perillo, L.; Chaushu, S. Impaction of maxillary canines and its effect on the position of adjacent teeth and canine development: A cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e135–e147. [Google Scholar] [CrossRef] [PubMed]
- Al-Khanati, N.M.; Albassal, A.; Kara Beit, Z. Unusual Indications of Teeth Transplantation: A Literature Review. Cureus 2022, 14, e29030. [Google Scholar] [CrossRef]
- Bishara, S.E.; Kommer, D.D.; McNeil, M.H.; Montagano, L.N.; Oesterle, L.J.; Youngquist, H.W. Management of impacted canines. Am. J. Orthod. 1976, 69, 371–387. [Google Scholar] [CrossRef]
- Kokich, V.G.; Mathews, D.A. Impacted teeth: Surgical and orthodontic considerations. In Orthodontics and Dentofacial Orthopedics; McNamara, J.A., Jr., Ed.; Needham Press: Ann Arbor, MI, USA, 2001. [Google Scholar]
- Heravi, F.; Shafaee, H.; Forouzanfar, A.; Zarch, S.H.; Merati, M. The effect of canine disimpaction performed with temporary anchorage devices (TADs) before comprehensive orthodontic treatment to avoid root resorption of adjacent teeth. Dent. Press. J. Orthod. 2016, 21, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Annarumma, F.; D’Emidio, M.; Rodi, G.; Battista, G.; Papi, G.; Migliorati, M. The effectiveness of miniscrews in the three-dimensional control of a palatal impacted canine: “Canine Only” approach. Case Rep. Int. Orthod. 2021, 19, 716–725. [Google Scholar] [CrossRef]
- Paduano, S.; Cioffi, I.; Iodice, G.; d’Antò, V.; Riccitiello, F.; Pellegrino, G.; Valletta, R. Correction of multiple canine impactions by mixed straightwire and cantilever mechanics: A case report. Case Rep. Dent. 2014, 2014, 925019. [Google Scholar] [CrossRef]
- Grisar, K.; Fransen, J.; Smeets, M.; Hoppenreijs, T.; Ghaeminia, H.; Politis, C.; Jacobs, R. Surgically assisted orthodontic alignment of impacted maxillary canines: A retrospective analysis of functional and esthetic outcomes and risk factors for failure. Am. J. Orthod. Dentofac. Orthop. 2021, 159, e461–e471. [Google Scholar] [CrossRef] [PubMed]
- Hourfar, J.; Ruff, C.J.; Wilmes, B.; Ludwig, B.; Kanavakis, G. Rapid Maxillary Expansion and Upper-Molar Distalization with a Miniscrew-Supported Hybrid Appliance. J. Clin. Orthod. 2016, 50, 476–484. [Google Scholar] [PubMed]
- Migliorati, M.; Cevidanes, L.; Sinfonico, G.; Drago, S.; Dalessandri, D.; Isola, G.; Biavati, A.S. Three dimensional movement analysis of maxillary impacted canine using TADs: A pilot study. Head Face Med. 2021, 17, 1. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria; Available online: http://www.R-project.org/ (accessed on 1 December 2019).
- Becker, A.; Chaushu, G.; Chaushu, S. Analysis of failure in the treatment of impacted maxillary canines. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 743–754. [Google Scholar] [CrossRef] [PubMed]
- Grisar, K.; Luyten, J.; Preda, F.; Martin, C.; Hoppenreijs, T.; Politis, C.; Jacobs, R. Interventions for impacted maxillary canines: A systematic review of the relationship between initial canine position and treatment outcome. Orthod. Craniofac. Res. 2021, 24, 180–193. [Google Scholar] [CrossRef]
- Parkin, N.A.; Milner, R.S.; Deery, C.; Tinsley, D.; Smith, A.M.; Germain, P.; Freeman, J.V.; Bell, S.J.; Benson, P.E. Periodontal health of palatally displaced canines treated with open or closed surgical technique: A multicenter, randomized controlled trial. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 176–184. [Google Scholar] [CrossRef] [Green Version]
- Mavreas, D.; Athanasiou, A.E. Factors affecting the duration of orthodontic treatment: A systematic review. Eur. J. Orthod. 2008, 30, 386–395. [Google Scholar] [CrossRef] [Green Version]
- Weltman, B.; Vig, K.W.; Fields, H.W.; Shanker, S.; Kaizar, E.E. Root resorption associated with orthodontic tooth movement: A systematic review. Am. J. Orthod. Dentofac. Orthop. 2010, 137, 462–476. [Google Scholar] [CrossRef] [Green Version]
- Heravi, F.; Shafaee, H.; Forouzanfar, A.; Zarch, S.H.; Merati, M. Forced eruption of palatally impacted canines using bracket-head miniscrews. J. Clin. Orthod. 2014, 48, 576–580. [Google Scholar]
- Kocsis, A.; Seres, L. Orthodontic screws to extrude impacted maxillary canines. J. Orofac. Orthop. 2012, 73, 19–27. [Google Scholar] [CrossRef]
- Chaushu, S.; Becker, A.; Chaushu, G. Lingual orthodontic treatment and absolute anchorage to correct an impacted maxillary canine in an adult. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 811–819. [Google Scholar] [CrossRef]
- Lo Giudice, A.; Ronsivalle, V.; Lagravere, M.; Leonardi, R.; Martina, S.; Isola, G. Transverse dentoalveolar response of mandibular arch after rapid maxillary expansion (RME) with tooth-borne and bone-borne appliances: A CBCT retrospective study. Angle Orthod. 2020, 90, 680–687. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, A.; Leonardi, R.; Ronsivalle, V.; Allegrini, S.; Lagravère, M.; Marzo, G.; Isola, G. Evaluation of pulp cavity/chamber changes after tooth-borne and bone-borne rapid maxillary expansion. A CBCT study using surface-based superimposition and deviation analysis. Clin. Oral Investig. 2020, 25, 2237–2247. [Google Scholar] [CrossRef] [PubMed]
- Lo Giudice, A.; Ronsivalle, V.; Spampinato, C.; Leonardi, R. Fully Automatic Segmentation of The Mandible Based On Convolutional Neural Networks (CNNs). Orthod. Craniofac. Res. 2021, 24, 100–107. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Group (13 Patients, 20 Teeth) | Test Group (mTPA) (14 Patients, 15 Teeth) | p-Value | |
|---|---|---|---|
| Timespan (days) | 85.50 [73.00, 99.00] | 130.00 [108.00, 189.00] | <0.001 |
| Apex | |||
| Displacement (mm) | 3.09 [2.07, 4.70] | 3.32 [1.75, 4.54] | 0.868 |
| Speed (mm/day) | 0.03 [0.01, 0.04] | 0.03 [0.02, 0.05] | 0.507 |
| Monthly Speed (mm/month) | 1.05 [0.74, 1.64] | 0.72 [0.27, 1.30] | 0.205 |
| Cusp | |||
| Displacement (mm) | 5.71 (3.10) | 5.31 (3.50) | 0.722 |
| Speed (mm/day) | 0.06 [0.03, 0.09] | 0.04 [0.03, 0.06] | 0.210 |
| Monthly Speed (mm/month) | 1.89 [1.04, 2.84] | 1.08 [0.81, 1.91] | 0.210 |
| Minimum | 25% | Median | 75% | Maximum | p-Value | |
|---|---|---|---|---|---|---|
| Test Teeth N = 16 | −0.10 | −0.05 | 0.01 | 0.16 | 0.87 | 0.207 |
| Control Teeth N = 42 | −1.27 | −0.54 | −0.01 | 0.12 | 0.46 | |
| Second Incisor N = 29 | −0.78 | −0.32 | 0.04 | 0.13 | 0.87 | 0.608 |
| First Bicuspid N = 29 | −1.27 | −0.52 | −0.03 | 0.16 | 0.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Migliorati, M.; Drago, S.; Bocchino, T.; Michelotti, A.; D’Antò, V. Treatment of Palatally Displaced Canines Using Miniscrews for Direct or Indirect Anchorage: A Three-Dimensional Prospective Cohort Study on Tooth Movement Speed. Appl. Sci. 2022, 12, 10935. https://doi.org/10.3390/app122110935
Migliorati M, Drago S, Bocchino T, Michelotti A, D’Antò V. Treatment of Palatally Displaced Canines Using Miniscrews for Direct or Indirect Anchorage: A Three-Dimensional Prospective Cohort Study on Tooth Movement Speed. Applied Sciences. 2022; 12(21):10935. https://doi.org/10.3390/app122110935
Chicago/Turabian StyleMigliorati, Marco, Sara Drago, Tecla Bocchino, Ambra Michelotti, and Vincenzo D’Antò. 2022. "Treatment of Palatally Displaced Canines Using Miniscrews for Direct or Indirect Anchorage: A Three-Dimensional Prospective Cohort Study on Tooth Movement Speed" Applied Sciences 12, no. 21: 10935. https://doi.org/10.3390/app122110935