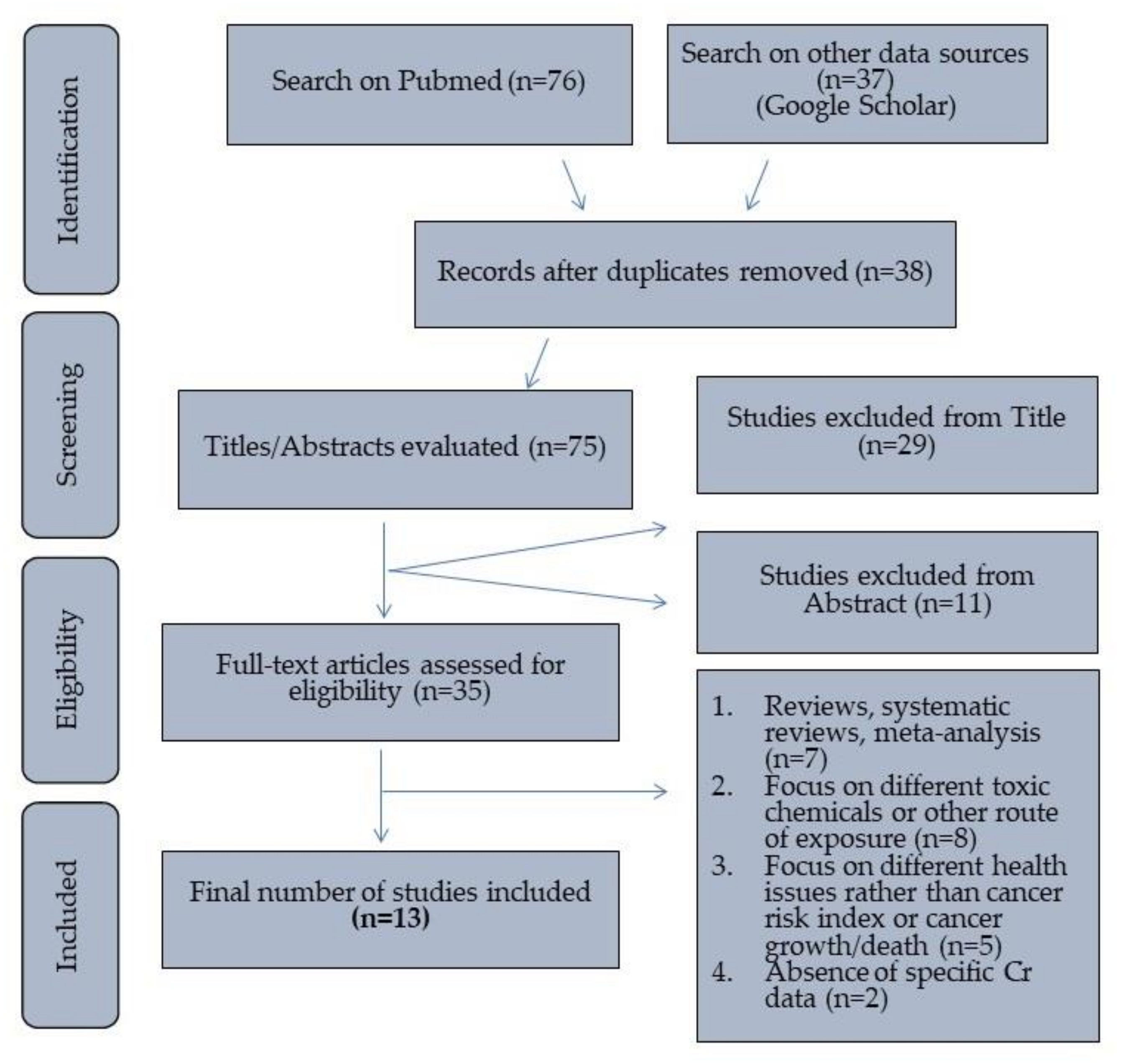
3.1. Characteristics of Main Findings
The total number of articles examined in this systematic review covers the years 2000 (January) to 2022 (November). Of the 13 included studies, 10 are epidemiological case studies (case reports or case series) evaluating cancer and non-cancer indices, while the remaining 3 are epidemiological ecological studies evaluating risk effects at a population level and not at the individual level. For each investigation, information was extracted on the study population and size, study site, total or hexavalent chromium concentration in water (surface and groundwater, drinking and tap water), and human health impacts, with emphasis on cancer.
Surface and underground waters, as well as drinking water, were sampled to determine whether they exceeded quality standards, identify the source of contamination, and quantify the level of pollution. According to Directive 98/83/EC of the Council of the European Union of 3 November 1998 (Joint Ministerial Decision Y2/2600/2001), natural and treated water, which is intended for drinking, cooking, or other domestic uses, regardless of whether it comes from a well, distribution network, bottles, or containers, is characterized as water for human consumption. Most of the studies included in the systematic review did not report the origin of the water samples, both for human consumption and recreational water. The included ecological studies were based on age, sex, and calendar years to estimate effect ratios (RR), including SMR and HI.
Data exports from the ecological studies were performed using the accounting package of Microsoft Excel, and then forest plots were created to assess the overall statistical significance of the data and report potential heterogeneity of the individual results. The studies took place in Asia, specifically in China, Iran, Pakistan, India, and Malaysia, in Africa, specifically in Ghana, and, finally, in Europe, specifically in Greece. All study areas were characterized by significant concentrations of ultramafic rocks, enriched with chromium.
From the case studies, information on cancer health risk indices (LCR, ILCR, CR, HQ, HI, HRA, DALY) was extracted. Health risk assessments are tools used to evaluate the potential health effects of exposure to environmental chemical contaminants. These risk indicators are important because they provide a way to quantify the potential health impacts of various factors, such as exposure to environmental contaminants or the burden of disease in a population. The purpose of them is to help inform public health and social awareness by providing a systematic and scientifically supported assessment of health risks.
There are several indicators used to assess these risks, including Relative Risk (RR), which measures the association between exposure and a health outcome, Standardized Mortality Rate (SMR), which compares mortality rates of a population to a reference population, Lifetime Cancer Risk (LCR), which estimates the probability of developing cancer over a lifetime, Incremental Lifetime Cancer Risk (ILCR), which measures the increase in lifetime cancer risk due to exposure, Cancer Risk (CR), which estimates the probability of developing cancer over a specified time period, Hazard Quotient (HQ), which evaluates the potential risk to human health from exposure to a specific chemical, Hazard Index (HI), which measures overall risk from exposure to multiple chemicals, Health Risk Assessment (HRA), which takes into account multiple routes of exposure and both acute and chronic effects, Disability-Adjusted Life Year (DALY), which measures the overall impact of a disease on a population by considering death and reduced quality of life, and Chronic Daily Intake Index (CDI), which measures chronic exposure to a chemical. These indicators provide a comprehensive approach to assess the potential health impacts of exposure to environmental contaminants.
3.3. Relationship between the Prevalence of Cancer and Chromium Exposure from Drinking Water
The first ecological study [
45] presents mortality rates from all cancers, including stomach and lung cancers, for a remarkable population sample in Liaoning Province, China, which was previously studied by Zhang and Li [
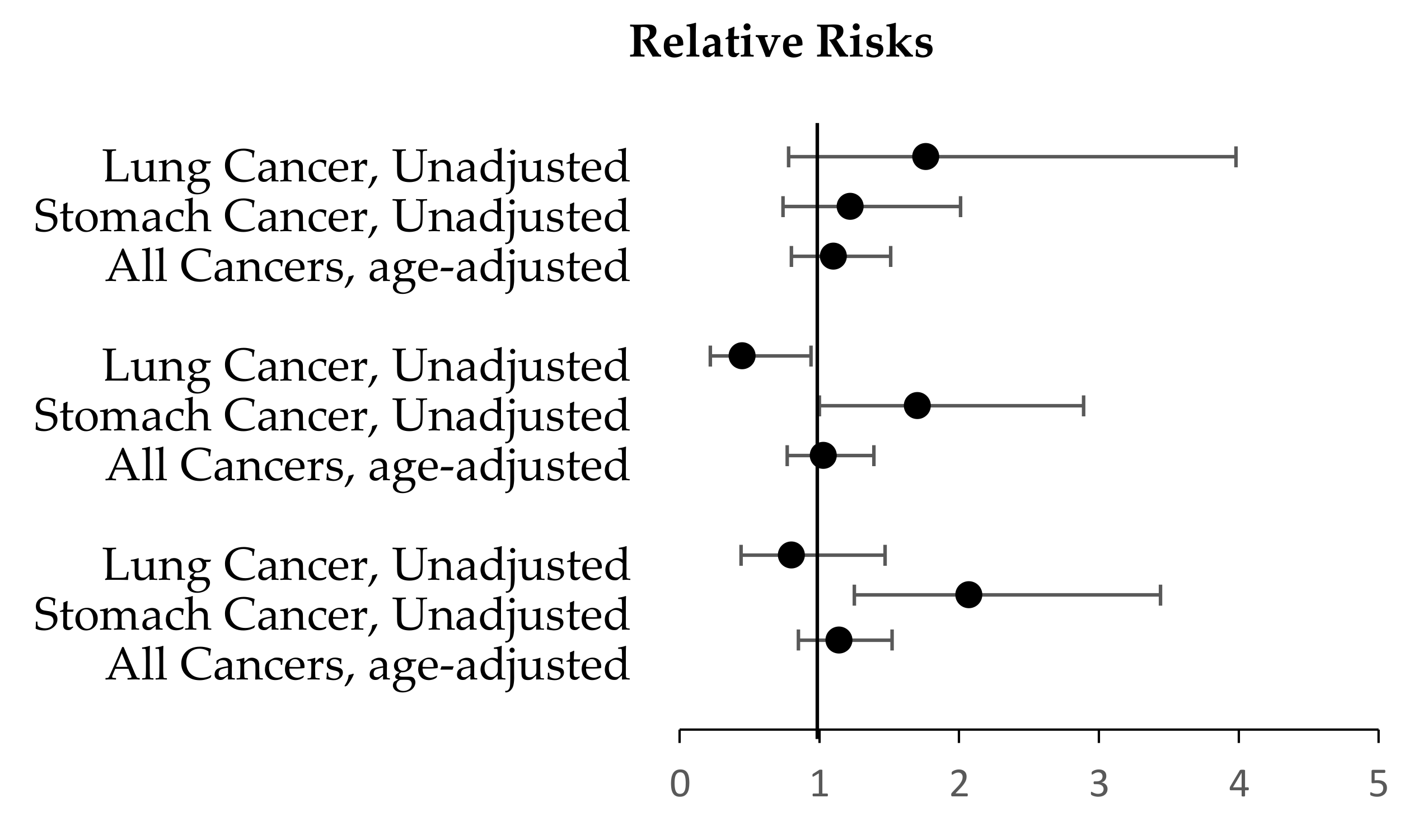
35]. Researchers in Liaoning Province, China, noticed in 1987 that communities with hexavalent chromium-contaminated drinking water had higher all-cancer death rates, stomach cancer, and lung cancer between 1970 and 1978 than the general population [
31]. The effect ratios (RR) and confidence intervals (CI) for death rates from hexavalent chromium-exposed (5) and non-exposed (4) areas were calculated for the period 1970–1978. The age-adjusted rates of stomach and lung cancer were calculated by multiplying the unadjusted rates by the age-adjustment effect ratios for all cancers. The death rate for all cancers was determined to be notably higher in the chromium-exposed area compared to the uncontaminated area (RR 1.13, 95% CI 0.86–1.46) and the entire province (RR 1.23, 95% CI 0.97–1.53). The mortality rate for stomach cancer was higher in exposed areas than in unexposed areas (RR 1.82, 95% CI 1.11–2.91) and across the province (RR 1.69, 95% CI 1.12–2.44). Lung cancer death rates were found to be slightly higher in chromium-contaminated areas than in the rest of the province (RR = 1.15, 95% CI 0.62–2.07) and slightly higher in non-exposed areas. The forest plots (
Figure 2) provide results of Rate Ratios obtained from the ecological study (see details in
Table 5,
Table 6,
Table 7 and
Table 8) [
45].
Table 5.
Main characteristics of the selected case studies included in the systematic review.
Table 5.
Main characteristics of the selected case studies included in the systematic review.
| Reference | Study Location | Population (Sample Size) | Exposure (Water Supply and Other Exposure Measures) | Outcome Measure |
|---|
| [46] | China, Hucan | 70 children | Human behavior pattern survey data collection. A plastic bottle that had been Lacid-washed contained a total of 20 tap water samples. Two more tap water samples were taken from the school’s two different classrooms.
| Calculated cancerous and non-cancerous health disorders (HI, HQ, ILCR). |
| [47] | Iran, Birjand | Total: 235,590 (3–10 years, 11–20 years, and 21–72 years) | Collection of 18 well water samples (72 samples). | Calculated cancerous and non-cancerous health disorders (HI, HQ). Calculated Monte Carlo simulation and sensitivity analysis.
|
| [48] | India, Ropar wetland | Children (under 18) and adults (over 18) | Collected 36 groundwater samples (18 samples during each season). | Calculated cancerous and non-cancerous health disorders (CDI, HI, HQ, CR). |
| [49] | Pakistan, Faisalabad Punjab | 3.2 million | | Calculated cancerous and non-cancerous health disorders (HQ, CR). |
| [50] | Asia, Langat River Basin, Malaysia | The Langat River Basin has 1,494,865 households | Collected water samples from each of the four points in the supply chain for drinking water. | Calculated cancerous and non-cancerous health disorders (CDI, HI, HQ, CR, LCR). A survey of 402 households with a questionnaire.
|
| [51] | Africa, Ghana, Lake Bosomtwe | Children and adults | Collected 30 water samples from Lake Bosomtwe. | Calculated cancerous and non-cancerous health disorders (HI, HQ, CR). |
| [52] | Pakistan, Muslim Bagh | 20,000 Afghan refugees | The study area produced three different types of water samples: mine, karez, and digged well. | Collection of blood samples. Collection of self-reported questionnaire survey. Calculated cancerous and non-cancerous health disorders (CDI, HQ, CR). Calculated indices such as Igeo, EF, and pollution parameters for soil analysis (PLI, PER, Cf, Ei). The indices were calculated using the examined body weight and intake of water from different sources.
|
| [53] | Iran | Total: 83 million (31 provinces divided into 5 regions) | Collected 8000 drinking water samples. | Calculated cancerous and non-cancerous health disorders (CDI, HI, HQ, CR, ILCR) and DALY. |
| [54] | Iran, Saravan | Iran, Saravan | A total of 89 underground water supplies. | Calculated non-cancerous health disorders (CDI, HQ). |
| [55] | China, Hanyuan | | Collected 96 drinking water samples. | Calculated non-cancerous health disorders (HQ, HI, CR). |
Table 6.
Main characteristics of the selected ecological studies included in the systematic review.
Table 6.
Main characteristics of the selected ecological studies included in the systematic review.
| Reference | Study Location | Population (Sample Size) | Exposure (Water Supply and Other Exposure Measures) | Outcome Measure |
|---|
| [45] | China, Liaoning Province, Jinzhou City | A total of 9 areas (divided to 5 exposed and to 4 unexposed areas) | Collected water samples from 5 exposed areas. | Calcualted the mortality rate for estimated person-years at risk using population census data. Calculated SMR and RR for all cancer types, and the CI.
|
| [56] | China, Liaoning Province, Jinzhou City | A total of 4 areas without hexavalent chromium contamination in drinking water. | Information from a previous study for the five areas exposed to hexavalent chromium. | Based on data from an earlier study, cancer deaths per person-years at risk Calculated RR. Trends in dose response in villages exposed to hexavalent chromium via water.
|
| [7] | Greece, Oinofyta Municipality | A total of 5842 permanent and legal residents registered in the Municipality’s records from 1999 to 2009. | Three sets of hexavalent chromium measurements in water: (2007 November–2008 February) and (2007 November–2008 February)/35 samples >10 g/L (maximum concentration of 156 g/L). (2008 September–2008 December) and (2008 September–2008 December)/3 samples: 41–53 g/L. (2007 Jul–2010 Jul) and (2007 Jul–2010 Jul)/13 samples > 10 g/L (maximum 51 g/L). Recent measurements (July 2009–July 2010) indicated lower levels (0.01–1.53 g/L).
| Calculated standardized mortality ratios by sex, age, and calendar year (SMR). Calculated adjusting for age and sex and the CI.
|
Table 7.
Results and conclusions of the selected case studies included in the systematic review.
Table 7.
Results and conclusions of the selected case studies included in the systematic review.
| Reference | Results | Conclusion |
|---|
| [46] | The drinking water was safe. Cr ingestion was mostly responsible for the non-cancer risk. HI at the 75th percentile <1.
| The cancer health risk of the study population is considered negligible through exposure to chromium in drinking water. |
| [47] | Cr(VI): 0.28 to 132.34 g/L, with an average of 21.306 34.68 g/L. A total of 83.33% of the samples for 15 wells had concentrations < WHO standard, while 16.66% of the samples for 3 wells had concentrations > WHO standard. The 95th percentile total HQ value is greater than 1 (both children and adolescent age groups). Children > Teens > Adults is how chromium’s non-carcinogenic risk is distributed among the three age groups in the study area.
| The amount of chromium in groundwater for skin contact and drinking contact is the most important variable impacting the risk of non-carcinogenicity in children and adolescents. |
| [48] | Cr > 0.05 mg/L in 50% of samples taken during the summer and all samples taken during the winter. Cr CDIs were higher in children than in adults. Cr CDIs were higher in both children and adults during the winter season. HQ > 1.00 for Cr in the winter season for children (1.99) and adults (1.54). The HQ values for Cr for children (1.03) are greater than 1.00 in the summer season, but less than 1.00 in the winter season.
| Study population has a high risk of developing cancer. |
| [49] | The drinking water was deemed of poor quality. The HQ values of chromium in drinking water ((2.13, 3.22) were very close to the threshold limit (HQ > 1) in both adults and children.
| Chromium levels in drinking water exceeded the acceptable limit. In adults, chromium posed a high risk of carcinogenicity. |
| [50] | Max concentration of Cr: 12.2 × 10 −4 mg/L. Cr in the basin’s supply water: 0.37 × 10 −3 mg/L. HQ for Cr; Treated water: t: 7.670, p: 8.77 × 10 −8 for 2015.River water: t: 16.83, p: 3.81 × 10−34 for 2015, t: 22.41, p: 5.84 × 10−54 for 2020. Tap water: t: 11.64, p: 5 × 10−15 for 2015.Filtration water: t: 9.35, p: 4.12 × 10−12 for 2015. CR for Cr; Treated water: t: 7.670, p: 8.77 × 10−8 for 2015.River water: t:16.83, p: 3.81 × 10−34 for 2015, t: 22.41, p:5.84 × 10−54 for 2020.Tap water: t: 11.64, p: 5 × 10−15. Filitration water: t: 9.35, p: 4.12 × 10−12.
| The level of Cr in the water was within the acceptable range for consumption. No health risks are associated with consuming Cr through household water filtration. The LCR index of Cr ingestion via household filtration water was within the acceptable range.
|
| [51] | Cr: 0.0032 mg/L. Dissolved Cr was statistically significant at p: 0.05 (F1.59 = 7.905, p = 0.007). Overall chromium: 0.0004 to 0.023 mg/L, with a mean and standard deviation of 0.0032 0.001 mg/L, while all water samples < WHO limit. Cr had a Relative Risk (HI) of 0.27%. The HQ values for oral and dermal Cr exposure in children and adults <1.
| The cancer risk estimates were lower than the USEPA’s chromium cancer risk range. Cr was determined to be of natural origin by PCA and cluster analysis. |
| [52] | Only 2% were aware of heavy metals, and about 5% were aware that Cr plants might also pollute the environment in the area. A total of 3% responded that prevalent diseases in the area are due to contaminated water. The Cr in drinking water: 13,530 ppb. The HQ: Cr 5.7–19 in the main group, while the control group’s HQ values are Cr 0.0035. The HQ values for all of the metals studied indicate that inhalation is the most common route of exposure for both children and adults, followed by ingestion and dermal contact. Cr’s CDI in water: 0.086–0.29. The users of mine water had the highest values and those of open-dug well users had the lowest values. In blood data, the HQ and CDI values of blood samples are within safe limits for various groups.
| Significant metal contamination, especially chromium, was detected in the research area’s drinking water and soil. Inhalation is the most favorable method of transmission for Cr, which poses a serious risk of cancer in both children and adults. |
| [53] | Cr: 12.1 g/L, < WHO limits. Max Cr: 19.8 g/L (Region 5) and low Cr: 1.4 g/L (Region 1). At the national level, Cr had 16.0% of the HQs. The average ILCR for Cr at the national level was 2.05 × 10−5. Incidence, mortality, death rate, DALYs, and DALY rate of cancer associated with chromium exposure through drinking water were determined to be 0.11 at the national level (0.09–0.13). Deaths accounted for approximately 96% of the attributable DALY. Chromium concentrations in water are still mostly related to lung and stomach cancer.
| The average level of chromium in the study population’s drinking water is considerably lower than the national standards established for the purity of that water. |
| [54] | Cr: 0.49 to 20 (g/L), < WHO limits. The mean HQ due to Cr: 0.0143, 0.0186, 0.0143, and 0.0112 for infants, children, teenagers, and adults, respectively. The HQ was lower than allowed.
| Ingestion of Cr (drinking water) exposure does not increase the risk of non-carcinogenic health risks. |
| [55] | The Cr (VI) met the standards of Chinese standards for drinking water quality. Adults have a greater risk of carcinogenesis. The Cr(VI) contributes significantly at 10.97%. The contribution of Cr(VI) is relatively significant, with the maximum estimate of the total carcinogenic risk for adults at 93.84%.
| There is a risk of hexavalent chromium in the water of the study area. Despite this, the values of the element are within the permissible values for the quality of drinking water. |
Table 8.
Results and conclusions of the selected ecological studies included in the systematic review.
Table 8.
Results and conclusions of the selected ecological studies included in the systematic review.
| Reference | Results | Conclusion |
|---|
| [45] | Cr (VI) >20 mg/L. The mortality rate for all cancers (5 study regions with hexavalent chromium in water) was lower than the mortality rate for all cancers (4 combined study regions without hexavalent chromium in water) (RR = 1.13; 95% CI 0.86–1.46). The overall cancer mortality rate was slightly higher in comparison to the province as a whole (1.23; 0.97–1.53). Stomach cancer mortality was significantly higher in regions with contaminated water than in regions without contaminated water (1.82; 1.11–2.91) and across the province (1.82;1.11–2.91) (1.69; 1.12–2.44). Lung cancer mortality was slightly higher in the exposed study regions (1.15; 0.62–2.07), but significantly higher in the province as a whole (1.78; 1.03–2.87). Mortality from other cancers was not increased when compared with either the unexposed study regions (0.86; 0.53–1.36) or the entire province (0.92; 0.58–1.38).
| Higher cancer mortality rates in exposed areas. Other types of cancer mortality (except stomach and lung cancer) did not increase in the exposed areas. A noteworthy link exists between drinking water exposure to hexavalent chromium and mortality from stomach cancer.
|
| [56] | Group B has a higher death rate from stomach cancer and a lower death rate from lung cancer. Lower death rates from stomach cancer in group A, but higher death rates from lung cancer and all other types of cancer. The RR rates between groups B and C were not statistically significant. Death rates for all cancer types were significantly compared between groups A and C. Group B has a higher rate of stomach cancer death and a lower rate of lung cancer death. Trends in dose–response relationships did not show any statistically significant correlations.
| Groups A, B, and C have significantly different age-adjusted and unadjusted cancer mortality rates regardless of chromium hexavalent exposure. |
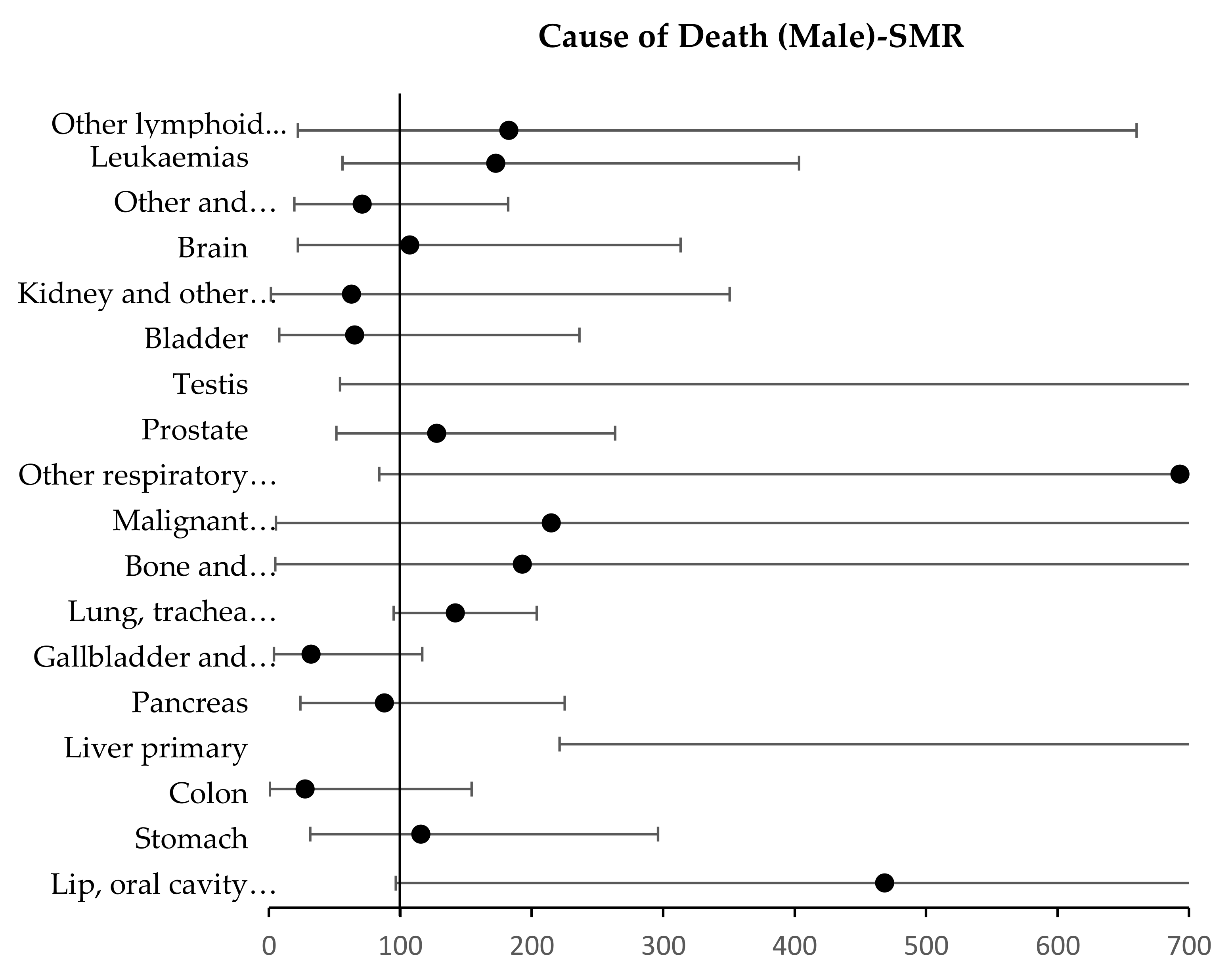
| [7] | The total was 474 deaths (SMR 97.9, 95% CI 89.3–107.1). Cancer-related deaths numbered 118 (SMR 113.6, 95% CI 94.1–136.1). SMR for lung, primary liver, and genital cancer deaths were statistically significant (p: 0.047, SMR 145.1, CI 100.5–202.8, p: 0.001, SMR 1104.2, CI 405.2–2403.3, p: 0.001, SMR 2141.5, CI 54.2–11931.5, p: 0.091). For the year 2009, the SMR for all cancer-related deaths was statistically significant (SMR 193, CI 114–304, p: 0.015).
| High levels of hexavalent chromium in drinking water are considered to be potential human carcinogens. |
Comparing the mortality rates in three different regions produced different results for a similar demographic population in China’s Liaoning Province [
56]. The first group relates to the TangHezi industrial area, where the Jinzhou Alloy Plant factory was located, where hexavalent chromium was not present in the water. Groups B (3 villages) and C (5 villages) are rural areas near the urban-industrial area (group A), with the former not contaminated and the latter contaminated with hexavalent chromium. TangHeZi had a much lower stomach cancer rate and a higher lung cancer rate than agricultural villages, both upgradient and downgradient of the alloy plant. Researchers concluded that the risk of mortality for all cancers is not significantly higher in hexavalent chromium-exposed populations, even though mortality rates in contaminated and non-contaminated areas are similar [
56]. For stomach cancer, the B/A ratio is 1.70, 95% CI 1.00, 2.89,
p = 0.05, while the C/A ratio is 2.07, 95% CI 1.5, 3.44,
p = 0.005. The B/A ratio for lung cancer is significant (RR = 0.45, 95% CI 0.22, 0.94,
p = 0.03). There was no evidence of a dose–response relationship between the Cr (VI) concentration in well water either for stomach cancer or for lung cancer. The Forest plot (
Figure 3) presents the summary statistics for Relative Risks among the three groups.
A similar study in Oinofyta, Greece, from 1999 to 2009, discovered 500 industries that produced industrial waste, and indicated the SMR for various cancers classified by the ICD-9 system in a permanent population (5842) over 11 years [
7]. Cancer is responsible for one out of every four deaths, most of which occur between 20 and 39, with no gender differences. Except for 2009 (SMR = 193, 95% CI 114–304,
p = 0.015), the SMR index for all cancer deaths slightly increased but not statistically (SMR = 114, 95% CI 94–136,
p > 0.05) (
Figure 4,
Figure 5 and
Figure 6). SMR is a key marker for liver, lung, and urogenital cancers. Lung cancer, kidney cancer, and other genitourinary organ cancers among women all had statistically significantly higher SMRs. Total cancer, lung cancer, and stomach cancer all had higher mortality rates. Both males and females demonstrated statistically significant SMR for primary liver cancer (
Figure 4). High SMR values were noted, but without statistical significance, for several cancer types, including cancers of the lip, oral cavity and pharynx, stomach, female colon, female breast, prostate, and leukemia (
Figure 5 and
Figure 6). The mortality rate from liver cancer is considered significant in the population exposed to hexavalent chromium in drinking water.
Another study examined the quantification of the cumulative concentration of 12 metals, including chromium, in water and other exposure media (such as food, PM10, soil/dust) in Okanagan, China, in a sample of children [
46]. Indices were calculated and assessed for cancer and non-cancer lifetime risk (HQ, HI, ILCR), and the contribution of each route of exposure through different routes is given by the indices (average daily dose via inhalation—ADDinhale, average daily dose via ingestion—ADDingest, and average daily dose via dermal contact—ADDdermal). By measuring the ADD for each of these exposure routes, scientists can better understand the potential health effects of a substance and develop appropriate risk management strategies to protect human health and the environment.
Overall, the quality of the drinking water analyzed was considered safe for the population exposed to it, since the total concentrations of metals were within the acceptable limits defined by the National Drinking Water Quality Standard (GB 5749-2006). GB 5749-2006 is China’s National Drinking Water Quality Standard, which is a set of standards that sets permissible limits for various pollutants, including chromium, in drinking water to ensure its safety for human consumption. The drinking water was considered safe for the study population, as the chromium content in the tap water had mean values of 6.67 µg/L, 25%, 6.16 µg/L, 75%, and 7.19 µg/L. The study found that the mean value of chromium content in the tap water was 6.67 µg/L. The values of 25% and 75% indicate the range of chromium content that 25% and 75% of the tap water samples fell within, respectively. Specifically, the statement says that 25% of the tap water samples had a chromium content of 6.16 µg/L or lower, and 75% of the tap water samples had a chromium content of 7.19 µg/L or lower. Although chromium ingestion, via drinking water consumption, was responsible for the overall carcinogenic risk, the contribution to the non-cancer risk index was to a greater extent from chromium inhalation (HI > 1 even at the 25th percentile). However, the overall ILCR was about 100 times above the permissible limit even at the 25th percentile, creating a high concern for potential cancer risks in the study area’s children due to exposure through drinking water consumption.
The total chromium concentrations in drinking water supply wells were examined in Birjand, Iran, in children, adolescents, and adults for more than two years [
47]. The study focused on how chromium concentration changed over time and space, with samples collected from the south side of the study area exhibiting the highest concentration. The estimated daily intake through ingestion absorption (EDling) index and the estimated daily intake through dermal absorption (EDIderm) index were quantified, with the first being significantly higher. The USEPA’s non-carcinogenic risk assessment indicators (HQ, HI) were also evaluated. For the entire study population, the HQ value for the 95th percentile is greater than 1, whereas the children’s population is classified as high risk. In the case of using water for drinking, with a high concentration of chromium, it is necessary to reduce its concentration to the permitted limits.
Similarly, a recent study in the Ropar Wetland, Punjab, India, examined the health risks of toxic metals’ exposure, including total chromium, in adults and children in both summer and winter [
48]. The CDI was established, which was critical for chromium. Non-carcinogenic health risk indicators (HQ, HI > 1) for adults and children, as well as the CR, were identified. In 50% of the samples collected during the summer season and all the samples collected during the winter season, the chromium concentration was above the allowed limit of 0.05 mg/L. The rise in these indices indicates that rising chromium concentrations in groundwater increases cancer risk, especially in children. One factor could be their low body weight. Furthermore, this susceptible population group is more sensitive in winter (HQ: 1.99 and HI: 10.11).
In the city of Punjab, Faisalabad, Pakistan, researchers assessed the quality of surface and drinking water (Water Quality Index—WQI, Surface Water Quality—SAR, and Magnesium Absorption Ratio—MAR) and estimated the potential risk to human health, both in adults and in children, with an emphasis on carcinogenesis due to exposure to potential toxic elements, including chromium (HQ, HI, ADD, CR) [
49]. Chromium values in drinking water ranged between 0.002–0.01 mg/L, while concentrations in surface water ranged between 0.11–0.4 mg/L. Chromium HQ values (2.13, 3.22) were very close to the threshold (HQ > 1) in both adults and corresponding children. In surface water samples, chromium (3.20) had concentrations higher than the threshold established for cancer. Cancer index values were higher for the child population compared to the adult population. The drinking water quality of the study area is considered poor, which is associated with increased human carcinogenesis.
The association between the ingestion of toxic metals, including chromium, through drinking water and potential human carcinogenic risk was extended in the Langat River Basin, Malaysia [
50]. Water samples were collected (river water, water treatment plant (WTP), domestic water, (HH), tap water, and filtered water). Human health risk was assessed by calculating the chronic daily chromium intake, non-carcinogenic risk quotient, and carcinogenic risk index, according to chromium ingestion through drinking water (CDI, HQ, LCR). The average chromium concentration was within the maximum permissible limit for drinking water quality, according to the Ministry of Health Malaysia (MOH), World Health Organization (WHO), and European Commission (EC). The mean dissolved chromium concentration in the water supply basin (0.37 × 10
−3 +/− 0.21 × 10
−3 mg/L) was below the recommended maximum drinking water quality limit (0.5 mg/L). Because the HQ for chromium was significantly below the permissible limit in 2015 and 2020, consuming chromium through residential filtered water does not constitute a health risk. Similarly, the LCR value of chromium ingestion via domestic filtered water was within the safe limit in 2015 and 2020. Although chromium concentrations are within safe limits in the Langat basin, a high concentration of the metal has been found in domestic water (tap water), specifically because the water supply pipeline has been contaminated.
The water quality of Lake Bosomtwe, Ghana, was assessed for the health risk and cancer and non-cancer index for oral and dermal exposure to potential toxic elements, including chromium, in children and adults (ADDingest, ADDdermal, HQ, HI, CR) [
51]. Total chromium concentration ranged from <0.0004 to 0.023 mg/L, with a mean and standard deviation of 0.0032 ± 0.001 mg/L. However, dissolved chromium levels were not detected. All samples of total chromium were under the 0.05 mg/L permissible limit defined by the WHO. The estimated average daily dose via oral consumption (ADDoral) for total chromium for the target groups (ADDoral 3.84 × 10
−7 for children, ADDoral 8.22 × 10
−7 mg/kg/day for adults) was within their respective RfDoral thresholds (oral reference dose of metal—RfDoral 3.00 × 10
−3 mg/L). Similarly, the estimated ADDdermal values for total chromium for the target groups (ADDdermal 1.01 × 10
−8 for children, ADDdermal 1.72 × 10
−8 mg/kg/day for adults) were within their respective RfDoral thresholds (RfDoral 7.50 × 10
−4 mg/L). Research that has already been conducted shows that drinking water enriched with metals has much higher health risks compared with skin contact [
57]. The HQ for chromium was rated less than unity (HQ < 1) (non-carcinogenic risk HQ 7.67 × 10
−4 for children, HQ 1.64 × 10
−3 for adults). The HQ values for all potential exposures, whether oral or dermal, were combined to determine the HI because the population was exposed to a lot of toxic metals. A child’s HI value was 0.82 (HI < 1), which indicates that they are unlikely to encounter non-carcinogenic health impacts. The relative risk contributions of chromium to the risk index are 0.27% for children and 0.35% for adults. The cancer risk estimate was within the limits set by the USEPA for cancer (7.67 × 10
−4 for children and 1.64 × 10
−3 for adults). From the PCA and cluster analysis for the metals, it is not shown that the origin of chromium is due to natural processes.
The degree of carcinogenicity due to exposure to potential hazardous metals including chromium in drinking water was assessed at Iran’s national and regional levels [
55]. They calculated the carcinogenic and non-carcinogenic indices (HRA, CDI, HQ, DALY, ILCR). The concentration of chromium in drinking water was well below the upper limits (12.1 µg/L), with the highest concentration reaching 19.8 µg/L and the lowest at 0.6 µg/L. The total HQ was determined to be 0.45, the total ILCR 2.05 × 10
−5, and the contribution of Cr exposure to the disease-related burden was 19.3%. The contribution of chromium to the total HQ at the national level was 16.0%. Overall, the burden of disease attributable to exposure to potential toxic metals including chromium through drinking water consumption was poor.
In the city of Saravan, Iran, the content of three potential toxic metals, including chromium, was examined in groundwater samples used for drinking water, irrigation, and industrial purposes [
54]. They calculated only the non-cancer index to evaluate human health effects in infants, children, adolescents, and adults (HQ, CDI). Chromium concentration ranged between 0.49 and 20 µg/L, below the WHO guideline of 50 µg/L. The mean serum non-cancer index due to chromium exposure was less than 1 (0.0112–0.0186). Specifically, the mean HQs due to chromium exposure for infants, children, adolescents, and adults were 0.0143, 0.0186, 0.0143, and 0.0112, respectively. All age groups had HQ levels that were below 1. The HQ is insignificant in infants, children, teenagers, and adults, according to the simulation data (CD: 95%). Therefore, chromium exposure through ingested drinking water does not raise the risk of carcinogenic health problems.
Researchers conducted a risk assessment of human health in Hanyuan, China, by collecting drinking water samples and analyzing 10 chemicals, including Cr (VI). Gastrointestinal absorption factors and cancer and non-cancer indices (HQ, HI, CR) were calculated for both adults and children [
55]. The researchers concluded that the carcinogenic risk for adults and the cumulative contribution of Cr (VI) exceeded 95%. In contrast to the non-carcinogenic risk, which was determined to be negligible (0.1%), adults are at a higher risk of developing cancer, with a considerable contribution from Cr (VI) at a rate of 10.97%. The concentration of Cr (VI) in drinking water was 0.002 µg, within the limits set by the WHO and China’s water sanitation. Even when the drinking water quality complies with established requirements, there is still a possibility for health risks.
Potential causes of disease prevalence in the general population in Pakistan’s Baluchistan region were investigated near a chromite mining plant [
52]. For toxic metals analysis, samples of drinking water, soil, and human blood were taken from exposed and unexposed populations. The CDI and HQ indices were calculated. The concentration of the four toxic metals in the water samples increased in the following order: Pb, Co = Ni, Cr. The concentration of chromium in drinking water ranged from 1990 to 13,530 ppb, which is significantly above the WHO’s limit [
18]. It can therefore be concluded that the area’s drinking water is unsuitable for human consumption, primarily because of the high percentage of chromium in the studied sample. The assessment of carcinogenic and non-carcinogenic risks to human health demonstrated that both children and adults are at high risk. The group of industrial workers who had direct contact through mining and drank well water had the maximum concentrations of chromium. The lowest concentrations were found in a group of people who lived near the mine and ingested both filtered and unfiltered drinking water. The calculated CDI and HQ values for chromium in children and adults were higher than the health risk levels (less than 1 or equal to 1). The data showed that the drinking water in the area was becoming unsuitable for consumption due to high chromium concentrations. The important thing that was found was that the local population has no consciousness of the risks of toxic metal contamination. Only 2% of the study population knew that hazardous metals, including chromium, could cause environmental pollution, while only 3% knew that the diseases that exist in the area were due to contaminated water.
3.4. Critical Methodological Quality Assessment and Limitations of Systematic Review
The application of critical appraisal guidelines to evaluate the validity of research findings has become a well-established technique in medical science, encouraging the use of evidence-based practice. The systematic review consisted of non-randomized controlled trials and case reports, also known as case studies, while no clinical studies were found during the systematic search. The Newcastle Ottawa Scale (NOS) and the National Institutes of Health Quality Assessment Tool (NIH) were two extensive approaches used to evaluate the methodological quality of the research taken into consideration and included in the final review. In total, the 3 ecological studies were reviewed and evaluated with the NOS scale (
Table 9), and the other 10 studies were evaluated with the NIH scale (
Table 10) [
58].
The NOS quality scale, suitable for assessing the methodological design of cohort studies and patient-control studies, as well as the modified NOS scale for assessing cross-sectional and ecological studies [
59,
60], uses a system rating with stars to evaluate three parameters in each study, the study population (selection of populations of each group-selection of study groups), the comparison between the selected groups (comparison of research groups), and the presenting of the and the presenting of the results’ health coefficients (exposure or outcome). Studies completing a total score <5 are assessed as low quality, between 5 and 7 are assessed as moderate quality, and >7 as high quality [
61]. In this systematic review, the epidemiological ecological studies are characterized by moderate to high methodological quality.
Similar to the NOS scale, the NIH scale approach consists of 10 risk-of-bias questions or limits (except for 4 questions which are unique for cohort studies) for evaluating validity of the case studies. The questions relate to the study of population and groups, sample size, exposure and outcome, levels of exposure and outcome, and adjustment for potential confounders. Studies with scores 0–3 and 4–6 are determined to have high or probably high risk of bias, respectively, and studies with scores 7–9 are determined to have low or probably low risk of bias [
62]. Epidemiological case studies are characterized by low to high methodological quality.
Our systematic review includes research studies from around the world and assumes the evaluation of epidemiological factors. It covers a wide range of data sources that indicate a positive correlation between total chromium in drinking water and human carcinogenicity risk, creating a huge risk. However, the systematic review has significant limitations.
Despite conducting a thorough search of well-established databases and careful cross-referencing, the possibility of missing a relevant study cannot be eliminated. Furthermore, the systematic review methodology has limitations such as research search, data selection, and publication biases. The researcher’s selection error and personal perception create significant errors, despite the application of thorough methods to analyze the methodological quality of each study included in the review.
Once an epidemiologic study is completed, it is difficult to identify all the variables that may confound the validity of the results. Most epidemiological studies have insufficient data on chromium exposure. Significant data on the hazardous hexavalent form of chromium are lacking, with most studies estimating total chromium. There are significant uncertainties in chromium exposure concentration measurements in water, and valid information on intensity, frequency, duration, and route of exposure is lacking. Individual outcome data, including information on cancer or death from cancer (such as type of primary or metastatic cancer), latency, and risk time, tend to be limited or incomplete. This fact adds significant error to the conclusion since the exposure–outcome relationship may be overestimated or underestimated [
63]. A minority of studies have demonstrated the importance of using reliable statistical models to account for confounders.
The results of epidemiological ecological studies at the population level may not represent the corresponding relationship at the individual level [
64]. An important limitation is the possibility of misclassification of the patient’s cause of death or disease, because the result in both comparison groups may be due to a different cause that is not controlled for separately by the patient. Due to a lack of knowledge, it may be necessary for cancer and non-cancer human health risk indices to make calculated estimations and cautious assumptions. This means that when there are knowledge gaps, human health risk assessments tend to overstate the theoretical risk to protect the public health.
Environmental health risk evaluations also consider the most sensitive (or vulnerable) individuals of the community. This offers a “worst-case scenario” to assist in directing the best choices for reducing the dangers to human health. Human health risk assessment must be considered by the community as considering entire communities or populations. A human health risk assessment emphasizes the type and extent of past, present, and future health risks but does not typically identify specific individuals who have been exposed to a chemical, correlate chemical levels estimated in individuals or groups of people to health outcomes, or diagnose disease, and thus should not be used in place of a discussion with a medical or health practitioner.


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





