
Mycobacterium Tuberculosis Infection after Kidney Transplantation: A Comprehensive Review

 , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Epidemiology and Risk Factors for Tuberculosis in Kidney Transplantation
3.1. Epidemiology of Tuberculosis in Solid Organ Transplantation
3.2. Epidemiology of Tuberculosis in Kidney Transplantation
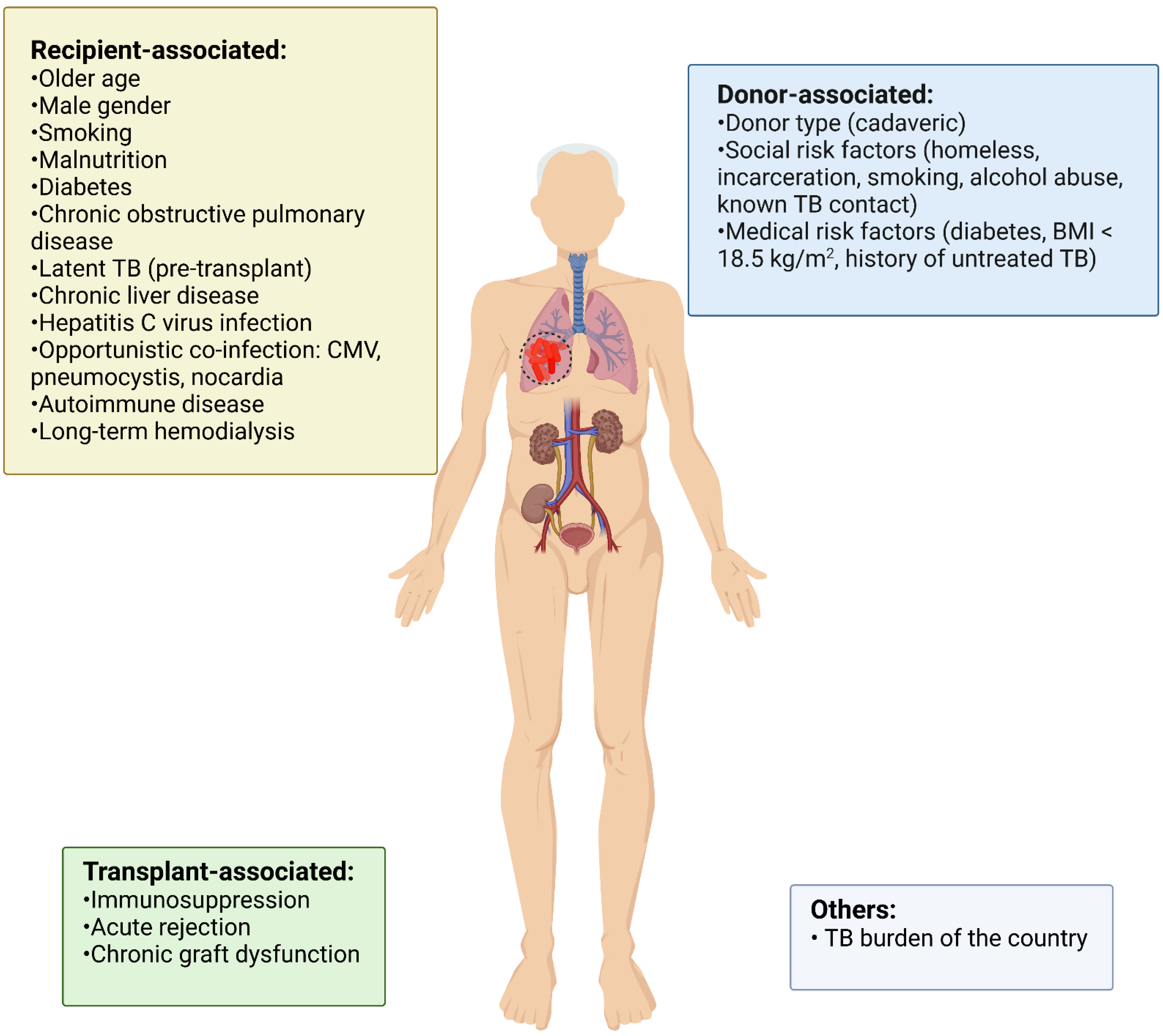
3.3. Risk Factors for Tuberculosis in Kidney Transplantation


{kind=link}
{kind=link}
| First Author Name (Year) | Population | Recruiting Period | TB Patients/Total Patients | TB Frequency | Time of TB Diagnosis after KT (Months) | TB Type | Graft Loss | Rejection | Mortality |
|---|---|---|---|---|---|---|---|---|---|
| Apaydin et al. (2000) [57] | Turkey | 1986–1998 | 16/274 | 5.8% | 6 (3–119) | Pulmonary (50%) Other (50%) | 6.3% | 6.3% | 31% |
| Biz et al. (2000) [61] | Brazil | 1976–1996 | 30/1264 | 2.5% | 54 (1.5–216) | Pulmonary (60%) Other (40%) | 10% | 16.6% | 23.3% |
| Koselj et al. (2000) [62] | Slovenia | 1980–1997 | 8/273 | 2.9% | 34 (1–96) | Pulmonary (62.5%) Other (37.5%) | 12.5% | 25% | 25% |
| Sharma et al. (2000) [63] | India | NA | 21/163 | 12.9% | 42 ± 10 | Pulmonary (47.6%) Other (52.4%) | 14.3% | NA | 23.8% |
| Vachharajani et al. (2000) [60] | India | 1989–1991 | 16/109 | 14.7% | 6.5 (1-18) | Pulmonary (43.7%) Other (56.3%) | NA | 12.5% | 18.7% |
| John et al. (2001) [24] | India | 1986–1999 | 166/1414 | 13.3% | NA | Pulmonary (48.2%) Other (51.8%) | 6% | NA | 31.9% |
| Lezaic et al. (2001) [42] | Yugoslavia | 1980–1998 | 16/456 | 3.1% | 40.5 (1.5–120) | Pulmonary (62.5%) Other (37.5%) | 18.7% | 0% | 37.5% |
| Naqvi et al. (2001) [18] | Pakistan | 1985–2000 | 130/850 | 15.2% | 12 (10–60) | Pulmonary (52%) Other (48%) | 18.5% | 22.7% | 29% |
| Melchor et al. (2002) [52] | Mexico | 1992–2000 | 10/545 | 1.8% | 22.5 (2–88) | Pulmonary (60%) Other (40%) | NA | NA | 50% |
| Niewczas et al. (2002) [51] | Poland | 1991–2000 | 15/1289 | 1.2% | 2 (1–44) | Pulmonary (66.6%) Other (33.4%) | 26.6% | 6.6% | 6.6% |
| Dridi et al. (2003) [53] | Tunisia | 1980–2002 | 5/368 | 1.3% | 27 (3–63) | Pulmonary (60%) Other (40%) | NA | 0% | 40% |
| El-Agroudy et al. (2003) [71] | Egypt | 1976–1999 | 45/1200 | 3.8% | 49.8 ± 41.5 | Pulmonary (37.7%) Other (62.3%) | 35% | 55.6% | 24.4% |
| Queipo et al. (2003) [44] | Spain | 1980–2000 | 20/1261 | 1.6% | 20.5 (2–114) | Pulmonary (60%) Other (40%) | 5% | NA | 15% |
| Vandermarliere et al. (2003) [47] | Belgium | 1963–2001 | 9/2502 | 0.4% | 64 (5–188) | Pulmonary (67%) Other (33%) | 66.6% | 33.3% | 0% |
| Klote et al. (2004) [36] | USA | 1998–2000 | 66/15870 | 0.4% | 19.6 ± 12 | Pulmonary (62%) Other (38%) | NA | NA | 23% |
| Matuck et al. (2004) [56] | Brazil | 1981–2002 | 44/982 | 4.5% | 36 ± 10.8 | Pulmonary (51%) Other (49%) | NA | 0% | 34.9% |
| Atasever et al. (2005) [43] | Turkey | 1994–2002 | 20/443 | 4.5% | 53.1 (2–255) | Pulmonary (35%) Other (65%) | NA | NA | 28.3% |
| Chen et al. (2006) [32] | Taiwan | 1983–2003 | 29/756 | 3.8% | 57.9 (1.2–145.2) | Pulmonary (71%) Other (29%) | 65.5% | 13.6% | 41.4% |
| Ergun et al. (2006) [38] | Turkey | 1990–2004 | 10/283 | 3.5% | 38 (3–81) | Pulmonary (50%) Other (50%) | NA | 0% | NA |
| Ghafari et al. (2007) [55] | Iran | 1989–2005 | 52/1350 | 3.9% | 54.6 (4–140) | Pulmonary (68%) Other (32%) | 37% | 25% | 23% |
| Kaaroud et al. (2007) [58] | Tunisia | 1986–2006 | 9/359 | 2.5% | 49.6 (3–156) | Pulmonary (55.5%) Other (44.5%) | NA | NA | 22.2% |
| Ram et al. (2007) [23] | India | 1989–2005 | 27/202 | 13.3% | NA | Pulmonary (33.3%) Other (66.7%) | 38.6% | NA | 0% |
| Basiri et al. (2008) [59] | Iran | 1964–2003 | 44/12820 | 0.3% | 25.1 (0.5–78) | Pulmonary (59%) Other (41%) | NA | 0% | NA |
| Chen et al. (2008) [33] | China | 1991–2007 | 43/2333 | 1.7% | 8 (1–156) | Pulmonary (71%) Other (29%) | 12.2% | 29.3% | 21.7% |
| Ruangkanchanasetr et al. (2008) [49] | Thailand | 1987–2007 | 5/151 | 3.3% | 23 (1–47) | Pulmonary (100%) | NA | 20% | 0% |
| Rungruanghiranya et al. (2008) [48] | Thailand | 1992–2007 | 9/270 | 3.3% | 36 (4–115) | Pulmonary (56%) Other (44%) | 22.2% | 0% | 22.2% |
| Torres et al. (2008) [37] | Spain | 1976–2004 | 16/2012 | 0.8% | 41.9 ± 18.2 | Pulmonary (68.7%) Other (22.3%) | NA | 37.5% | NA |
| Guida et al. (2009) [54] | Brazil | 1984–2007 | 23/1342 | 1.7% | 53 ± 49 | Pulmonary (43.5%) Other (56.5%) | 13% | 13% | 13% |
| Canet et al. (2011) [35] | France | 1986–2006 | 74/16,146 | 0.5% | 10 (4–27) | Pulmonary (32.6%) Other (67.4%) | 33% | 26.5% | 6.1% |
| Ersan et al. (2011) [41] | Turkey | 1992–2010 | 9/320 | 2.8% | 21 (1–150) | Pulmonary (44.4%) Other (55.6%) | 22.2% | 0% | 22.2% |
| Jung et al. (2012) [27] | South Korea | 2000–2010 | 23/1097 | 2.1% | 26 (3.1–113.2) | NA | NA | 0% | 14.3% |
| Ou et al. (2012) [31] | Taiwan | 1997–2006 | 109/4554 | 2.4% | 25.2 (0.1–118.5) | Pulmonary (68.8%) Other (31.2%) | 13.8% | NA | 22.9% |
| Boubaker et al. (2013) [40] | Tunisia | 1986–2009 | 16/491 | 3.2% | 23.6 (12.3–190.8) | Pulmonary (50%) Other (50%) | 25% | 18.7% | 12.5% |
| Marques et al. (2013) [30] | Brazil | 2000–2010 | 43/1549 | 2.8% | 6.5 (0.6–120.8) | Pulmonary (74%) Other (26%) | 44% | 16% | 12% |
| Rocha et al. (2013) [45] * | Brazil | 1998–2010 | 90/7833 | 1.1% | 80.4 ± 40.8 * | Pulmonary (61.1%) Other (38.9%) | 62.5%* | 25%* | 12.5%* |
| Higuita et al. (2014) [39] | Colombia | 2005–2013 | 12/641 | 1.9% | 9 (2.3–32.8) | Pulmonary (50%) Other (50%) | 8.3% | 8.3% | 16.6% |
| Akhtar et al. (2016) [25] | Pakistan | 2009–2011 | 46/910 | 5% | NA | Pulmonary (48%) Other (52%) | 2.2% | NA | 13% |
| Meinerz et al. (2016) [28] | Brazil | 2000–2012 | 60/1737 | 3.5% | 13.4 (1–121.3) | Pulmonary (78.3%) Other (21.7%) | 21.6% | 1.7% | 25% |
| Costa et al. (2017) [29] | Brazil | 1994–2014 | 34/1604 | 2.1% | 25.5 (1–168) | Pulmonary (47%) Other (53%) | 18.5% | 44.1% | NA |
| Gras et al. (2018) [34] | France | 2005–2015 | 32/3974 | 0.8% | 22.3 (8.9–66) | Pulmonary (68%) Other (22%) | 15.6% | 15.6% | 15.6% |
| Eswarappa et al. (2019) [22] | India | 2004–2015 | 21/244 | 8.6% | 30 (18–54) | Pulmonary (57%) Other (43%) | NA | 33.3% | 19% |
| Viana et al. (2019) [64] | Brazil | 1998–2014 | 152/11,453 | 1.3% | 18.8 (7.2–60) | Pulmonary (47.3%) Other (52.7%) | 25.6% | 17.9% | 19% |
| Park et al. (2021) [26] | South Korea | 2011–2015 | 125/7462 | 1.7% | NA | NA | 8% | NA | 16% |
| Thitisuriyarax et al. (2021) [50] | Thailand | 1992–2018 | 26/787 | 3.4% | 17 (4–59) | Pulmonary (48.1%) Other (51.9%) | 37% | 11.5% | 25.9% |
| Zou et al. (2021) [21] | China | 2005–2020 | 12/1300 | 0.9% | 22.1(3–120) | Pulmonary (92%) Other (8%) | NA | NA | NA |
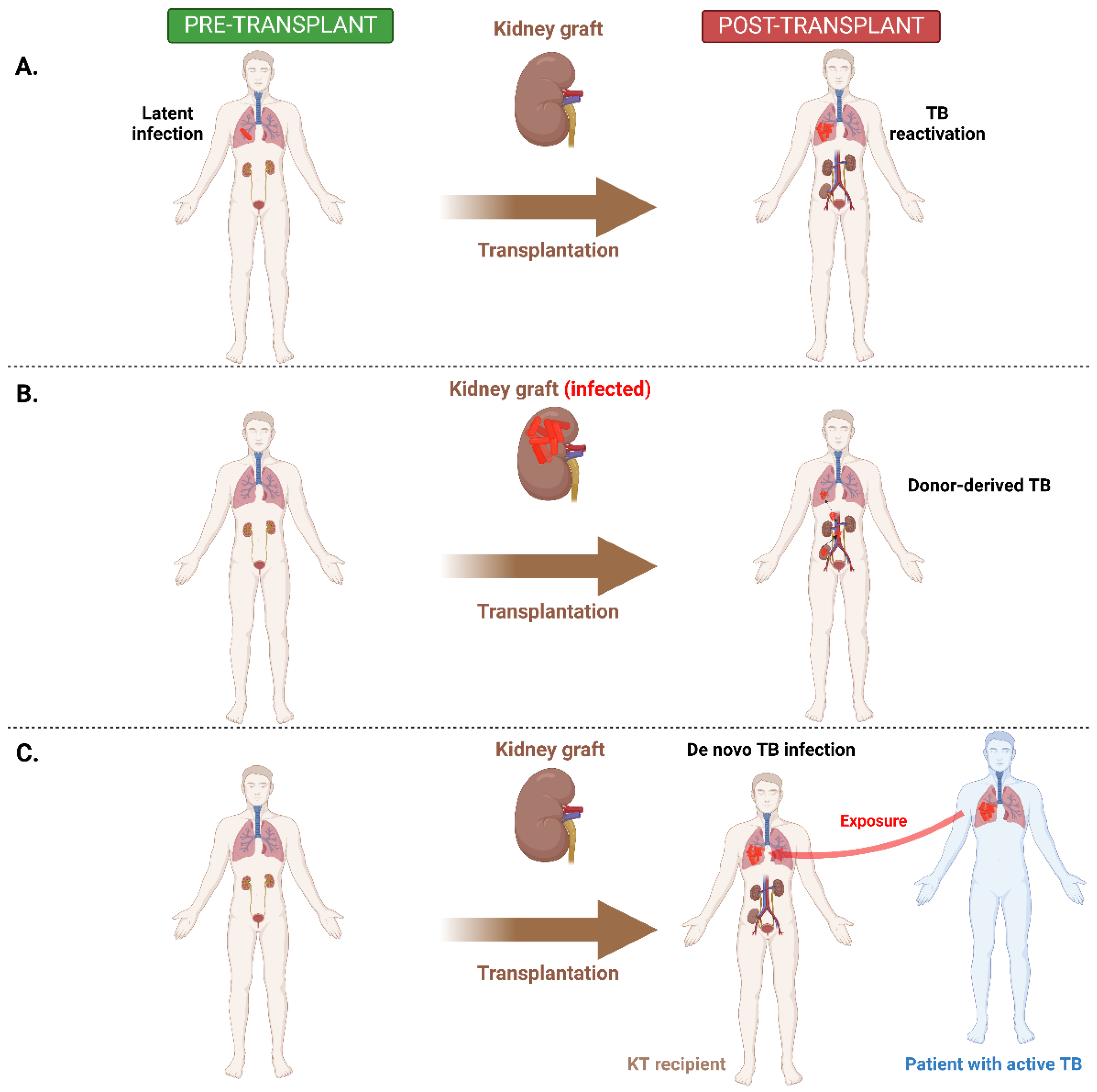
4. Transmission and Pathogenesis of Tuberculosis in Kidney Transplant Recipients
5. Diagnostic and Treatment Challenges
5.1. Diagnostic Challenges
5.1.1. Active Tuberculosis
5.1.2. Latent Tuberculosis
| First Author (Year) | Recipient Age (Years) | Recipient Gender | Recipient History of TB | Donor Type | Donor Age | Donor Gender | Donor History of TB | Diagnosis Modality | Diagnosis Time after KT | Symptoms | Localization | Graft Failure | Rejection | Death |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Graham et al.(2001) [88] | 44 | M | NR | DD | 69 | F | NR | Culture, histopathology | 14 months | Anuria | Kidney graft | Yes | No | No |
| Malone et al. (2007) [89] | 53 | M | NR | DD | NR | NR | NR | Culture, histopathology | 29 months | Nausea | Kidney graft | NR | NR | No |
| Edathoud et al. (2010) [90] | 48 | M | NR | DD | 26 | F | NR | Sputum, BAL, culture, PCR, histopathology | 2 months | Fever | Pulmonary, kidney graft, bone marrow | No | No | No |
| Edathoud et al. (2010) [90] | 29 | F | NR | DD | 26 | F | NR | Culture, histopathology | 1 month | Fever | Liver | No | No | No |
| Edathoud et al. (2010) [90] | 30 | M | NR | DD | NR | NR | NR | Culture, histopathology | 21 days | Fever | Bone marrow | No | No | Yes |
| Al-Nesf et al. (2014) [91] | 53 | F | NR | LD | NR | NR | NR | Smear, culture, histopathology | 2 months | Fever, abdominal pain | Kidney graft | Yes | No | No |
| Bucher et al. (2016) [92] | 69 | M | No | DD | 67 | F | Yes | Culture, PCR | 42 days | Skin lesions, cough, anuria | Skin, pulmonary, kidney graft, genitourinary | Yes | No | No |
| Abad et al. (2018) [81] | 30 | M | NR | LD | NR | NR | NR | PCR | 45 days | NR | Miliary | NR | NR | Yes |
| Abad et al. (2018) [81] | 50 | F | NR | DD | 46 | F | NR | PCR, culture | 45 days | Fever | Pulmonary, liver, kidney graft, spleen | NR | NR | Yes |
| Abad et al. (2018) [81] | 23 | F | NR | DD | 46 | F | NR | PCR | 47 days | Fever | Miliary, kidney graft | No | No | No |
| Clemente et al. (2021) [93] | 45 | M | No | DD | 23 | F | Yes | Culture | 2 months | Fever, nights sweats, chills | Pulmonary, central nervous system, thyroid, kidney graft | Yes | Yes | Yes |
| Ulisses et al. (2022) [94] | 18 | F | No | DD | 17 | M | Unknown | CT, PCR urine, wound | 37 days | Fever | Pulmonary, renal, miliary | No | No | No |
5.2. Treatment Challenges
5.2.1. Active Tuberculosis
5.2.2. Latent Tuberculosis
6. Outcomes
6.1. Rejection
6.2. Graft Loss
6.3. Mortality
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tonelli, M.; Wiebe, N.; Knoll, G.; Bello, A.; Browne, S.; Jadhav, D.; Klarenbach, S.; Gill, J. Systematic Review: Kidney Transplantation Compared with Dialysis in Clinically Relevant Outcomes. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2011, 11, 2093–2109. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.S.; Abichandani, R.; Kausz, A.T.; Pereira, B.J.G. Mortality after Kidney Transplant Failure: The Impact of Non-Immunologic Factors. Kidney Int. 2002, 62, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Watkins, A.; Aull, M.; Serur, D.; Hartono, C.; Kapur, S. Causes of Graft Loss After Kidney Transplantation Following Rabbit-Antithymocyte Gobulin Induction and Steroid-Sparing Maintenance. Abstract# 2922. Transplantation 2014, 98, 146. [Google Scholar]
- Chan, S.; Pascoe, E.M.; Clayton, P.A.; McDonald, S.P.; Lim, W.H.; Sypek, M.P.; Palmer, S.C.; Isbel, N.M.; Francis, R.S.; Campbell, S.B.; et al. Infection-Related Mortality in Recipients of a Kidney Transplant in Australia and New Zealand. Clin. J. Am. Soc. Nephrol. 2019, 14, 1484–1492. [Google Scholar] [CrossRef] [PubMed]
- Karuthu, S.; Blumberg, E.A. Common Infections in Kidney Transplant Recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 2058–2070. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.who.int/teams/global-tuberculosis-programme/tb-reports/global-tuberculosis-report-2021 (accessed on 1 August 2022).
- Https://Data.Worldbank.Org/Indicator/SH.TBS.INCD. Available online: https://data.worldbank.org/indicator/SH.TBS.INCD (accessed on 1 August 2022).
- Torre-Cisneros, J.; Doblas, A.; Aguado, J.M.; San Juan, R.; Blanes, M.; Montejo, M.; Cervera, C.; Len, O.; Carratala, J.; Cisneros, J.M.; et al. Tuberculosis after Solid-Organ Transplant: Incidence, Risk Factors, and Clinical Characteristics in the RESITRA (Spanish Network of Infection in Transplantation) Cohort. Clin. Infect. Dis. 2009, 48, 1657–1665. [Google Scholar] [CrossRef] [PubMed]
- Kwon, D.E.; Han, S.H.; Han, K.D.; La, Y.; Lee, K.H. Incidence Rate of Active Tuberculosis in Solid Organ Transplant Recipients: Data from a Nationwide Population Cohort in a High-Endemic Country. Transpl. Infect. Dis. 2021, 23, e13729. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.I.; Daly, J.S.; Blumberg, E.; Kumar, D.; Sester, M.; Schluger, N.; Kim, S.-H.; Schwartz, B.S.; Ison, M.G.; Humar, A.; et al. Diagnosis and Management of Tuberculosis in Transplant Donors: A Donor-Derived Infections Consensus Conference Report. Am. J. Transplant. 2012, 12, 2288–2300. [Google Scholar] [CrossRef]
- Bumbacea, D.; Arend, S.M.; Eyuboglu, F.; Fishman, J.A.; Goletti, D.; Ison, M.G.; Jones, C.E.; Kampmann, B.; Kotton, C.N.; Lange, C.; et al. The Risk of Tuberculosis in Transplant Candidates and Recipients: A TBNET Consensus Statement. Eur. Respir. J. 2012, 40, 990–1013. [Google Scholar] [CrossRef]
- Subramanian, A.K.; Theodoropoulos, N.M. Mycobacterium Tuberculosis Infections in Solid Organ Transplantation: Guidelines from the Infectious Diseases Community of Practice of the American Society of Transplantation. Clin. Transplant. 2019, 33, e13513. [Google Scholar] [CrossRef]
- Meije, Y.; Piersimoni, C.; Torre-Cisneros, J.; Dilektasli, A.G.; Aguado, J.M. Mycobacterial Infections in Solid Organ Transplant Recipients. Clin. Microbiol. Infect. 2014, 20 (Suppl. 7), 89–101. [Google Scholar] [CrossRef] [Green Version]
- Muñoz, P.; Rodríguez, C.; Bouza, E. Mycobacterium Tuberculosis Infection in Recipients of Solid Organ Transplants. Clin. Infect. Dis. 2005, 40, 581–587. [Google Scholar] [CrossRef]
- Abad, C.L.R.; Razonable, R.R. Mycobacterium Tuberculosis after Solid Organ Transplantation: A Review of More than 2000 Cases. Clin. Transplant. 2018, 32, e13259. [Google Scholar] [CrossRef]
- Anand, M.; Nayyar, E.; Concepcion, B.; Salani, M.; Schaefer, H. Tuberculosis in Kidney Transplant Recipients: A Case Series. World J. Transplant. 2017, 7, 213–221. [Google Scholar] [CrossRef]
- Aguado, J.M.; Torre-Cisneros, J.; Fortún, J.; Benito, N.; Meije, Y.; Doblas, A.; Muñoz, P. Tuberculosis in Solid-Organ Transplant Recipients: Consensus Statement of the Group for the Study of Infection in Transplant Recipients (GESITRA) of the Spanish Society of Infectious Diseases and Clinical Microbiology. Clin. Infect. Dis. 2009, 48, 1276–1284. [Google Scholar] [CrossRef]
- Naqvi, A.; Rizvi, A.; Hussain, Z.; Hafeez, S.; Hashmi, A.; Akhtar, F.; Hussain, M.; Ahmed, E.; Akhtar, S.; Muzaffar, R.; et al. Developing World Perspective of Posttransplant Tuberculosis: Morbidity, Mortality, and Cost Implications. Transplant. Proc. 2001, 33, 1787–1788. [Google Scholar] [CrossRef]
- Mamishi, S.; Pourakbari, B.; Moradzadeh, M.; van Leeuwen, W.B.; Mahmoudi, S. Prevalence of Active Tuberculosis Infection in Transplant Recipients: A Systematic Review and Meta-Analysis. Microb. Pathog. 2020, 139, 103894. [Google Scholar] [CrossRef]
- Helleberg, M.; Cho, D.; Ekenberg, C.; Sørensen, S.; Rix, M.; Gustafsson, F.; Rasmussen, A.; Perch, M.; Andersen, P.H.S.; Lundgren, J.D.; et al. Tuberculosis among Patients Undergoing Solid Organ Transplantation or Dialysis in a Low-Endemic Country, 2004–2017. Tuberc. Res. Treat. 2020, 2020, 7636975. [Google Scholar] [CrossRef]
- Zou, J.; Wang, T.; Qiu, T.; Chen, Z.; Zhou, J.; Ma, X.; Jin, Z.; Xu, Y.; Zhang, L. Clinical Characteristics of Tuberculous Infection Following Renal Transplantation. Transpl. Immunol. 2022, 70, 101523. [Google Scholar] [CrossRef]
- Marques, I.D.B.; Azevedo, L.S.; Pierrotti, L.C.; Caires, R.A.; Sato, V.A.H.; Carmo, L.P.F.; Ferreira, G.F.; Gamba, C.; de Paula, F.J.; Nahas, W.C.; et al. Clinical Features and Outcomes of Tuberculosis in Kidney Transplant Recipients in Brazil: A Report of the Last Decade. Clin. Transplant. 2013, 27, E169–E176. [Google Scholar] [CrossRef]
- Ou, S.-M.; Liu, C.-J.; Teng, C.-J.; Lin, Y.-T.; Chang, Y.-S.; Chiang, S.-C.; Tzeng, C.-H.; Chen, T.-J. Impact of Pulmonary and Extrapulmonary Tuberculosis Infection in Kidney Transplantation: A Nationwide Population-Based Study in Taiwan. Transpl. Infect. Dis. 2012, 14, 502–509. [Google Scholar] [CrossRef]
- Chen, C.-H.; Lian, J.-D.; Cheng, C.-H.; Wu, M.-J.; Lee, W.-C.; Shu, K.-H. Mycobacterium Tuberculosis Infection Following Renal Transplantation in Taiwan. Transpl. Infect. Dis. Off. J. Transplant. Soc. 2006, 8, 148–156. [Google Scholar] [CrossRef]
- Chen, S.-Y.; Wang, C.-X.; Chen, L.-Z.; Fei, J.-G.; Deng, S.-X.; Qiu, J.; Li, J.; Chen, G.-O.; Fu, H.-M.; Xie, C.-M. Tuberculosis in Southern Chinese Renal-Transplant Recipients. Clin. Transplant. 2008, 22, 780–784. [Google Scholar] [CrossRef]
- Gras, J.; De Castro, N.; Montlahuc, C.; Champion, L.; Scemla, A.; Matignon, M.; Lachâtre, M.; Raskine, L.; Grall, N.; Peraldi, M.N.; et al. Clinical Characteristics, Risk Factors, and Outcome of Tuberculosis in Kidney Transplant Recipients: A Multicentric Case-Control Study in a Low-Endemic Area. Transpl. Infect. Dis. 2018, 20, e12943. [Google Scholar] [CrossRef]
- Canet, E.; Dantal, J.; Blancho, G.; Hourmant, M.; Coupel, S. Tuberculosis Following Kidney Transplantation: Clinical Features and Outcome. A French Multicentre Experience in the Last 20 Years. Nephrol. Dial. Transplant. 2011, 26, 3773–3778. [Google Scholar] [CrossRef]
- Klote, M.M.; Agodoa, L.Y.; Abbott, K. Mycobacterium Tuberculosis Infection Incidence in Hospitalized Renal Transplant Patients in the United States, 1998-2000. Am. J. Transplant. 2004, 4, 1523–1528. [Google Scholar] [CrossRef]
- Torres, J.; Aguado, J.M.; San Juan, R.; Andrés, A.; Sierra, P.; López-Medrano, F.; Morales, J.M. Hepatitis C Virus, an Important Risk Factor for Tuberculosis in Immunocompromised: Experience with Kidney Transplantation. Transpl. Int. 2008, 21, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Ergun, I.; Ekmekci, Y.; Sengul, S.; Kutlay, S.; Dede, F.; Canbakan, B.; Erbay, B. Mycobacterium Tuberculosis Infection in Renal Transplant Recipients. Transplant. Proc. 2006, 38, 1344–1345. [Google Scholar] [CrossRef] [PubMed]
- Higuita, L.M.S.; Nieto-Ríos, J.F.; Daguer-Gonzalez, S.; Ocampo-Kohn, C.; Aristizabal-Alzate, A.; Velez-Echeverri, C.; Vanegas-Ruiz, J.J.; Ramirez-Sanchez, I.; Tobon, J.J.Z.; Zuluaga-Valencia, G.A. Tuberculosis in Renal Transplant Patients: The Experience of a Single Center in Medellín-Colombia, 2005–2013. Braz. J. Nephrol. 2014, 36, 512–518. [Google Scholar] [CrossRef] [PubMed]
- Eswarappa, M.; Devi, G.H.; John, M.M.; Chennabasappa, G.K.; Siddaiah, G.M. Tuberculosis in Renal Transplant Recipients: Our Decade Long Experience with an Opportunistic Invader. Indian J. Tuberc. 2020, 67, 73–78. [Google Scholar] [CrossRef]
- Boubaker, K.; Gargah, T.; Abderrahim, E.; Ben Abdallah, T.; Kheder, A. Mycobacterium Tuberculosis Infection Following Kidney Transplantation. Biomed Res. Int. 2013, 2013, 347103. [Google Scholar] [CrossRef] [Green Version]
- Ersan, S.; Celik, A.; Atila, K.; Aykut Sifil, A.; Cavdar, C.; Soylu, A.; Bora, S.; Gulay, H.; Camsari, T. Tuberculosis in Renal Transplant Recipients. Ren. Fail. 2011, 33, 753–757. [Google Scholar] [CrossRef]
- Lezaic, V.; Radivojevic, R.; Radosavljevic, G.; Blagojevic, R.; Djukanovic, L.; Simic, S.; Cvok, T. Does Tuberculosis after Kidney Transplantation Follow the Trend of Tuberculosis in General Population? Ren. Fail. 2001, 23, 97–106. [Google Scholar] [CrossRef]
- Atasever, A.; Bacakoglu, F.; Toz, H.; Basoglu, O.K.; Duman, S.; Basak, K.; Guzelant, A.; Sayiner, A. Tuberculosis in Renal Transplant Recipients on Various Immunosuppressive Regimens. Nephrol. Dial. Transplant. 2005, 20, 797–802. [Google Scholar] [CrossRef]
- Queipo, J.A.; Broseta, E.; Santos, M.; Sánchez-Plumed, J.; Budía, A.; Jiménez-Cruz, F. Mycobacterial Infection in a Series of 1261 Renal Transplant Recipients. Clin. Microbiol. Infect. 2003, 9, 518–525. [Google Scholar] [CrossRef]
- Rocha, A.; Lourenço, L.; Viana, L.; Taver, M.; Gaspar, M.; Medina-Pestana, J.O. Abdominal Tuberculosis Following Kidney Transplantation: Clinicopathologic Features and Follow-up in a Unique Case Series. Clin. Transplant. 2013, 27, E591–E596. [Google Scholar] [CrossRef]
- El-Agroudy, A.E.; El-Baz, M.A.; Ismail, A.M.; Ali-El-Dein, B.; Shehab El-Dein, A.B.; Ghoneim, M.A. Clinical Features and Course of Kaposi’s Sarcoma in Egyptian Kidney Transplant Recipients. Am. J. Transplant. 2003, 3, 1595–1599. [Google Scholar] [CrossRef]
- Vandermarliere, A.; Van Audenhove, A.; Peetermans, W.E.; Vanrenterghem, Y.; Maes, B. Mycobacterial Infection after Renal Transplantation in a Western Population. Transpl. Infect. Dis. 2003, 5, 9–15. [Google Scholar] [CrossRef]
- Rungruanghiranya, S.; Ekpanyaskul, C.; Jirasiritum, S.; Nilthong, C.; Pipatpanawong, K.; Mavichak, V. Tuberculosis in Thai Renal Transplant Recipients: A 15-Year Experience. Transplant. Proc. 2008, 40, 2376–2379. [Google Scholar] [CrossRef]
- Ruangkanchanasetr, P.; Natejumnong, C.; Kitpanich, S.; Chaiprasert, A.; Luesutthiviboon, L.; Supaporn, T. Prevalence and Manifestations of Tuberculosis in Renal Transplant Recipients: A Single-Center Experience in Thailand. Transplant. Proc. 2008, 40, 2380–2381. [Google Scholar] [CrossRef]
- Ram, R.; Swarnalatha, G.; Prasad, N.; Dakshinamurty, K. V Tuberculosis in Renal Transplant Recipients. Transpl. Infect. Dis. 2007, 9, 97–101. [Google Scholar] [CrossRef]
- Thitisuriyarax, S.; Vanichanan, J.; Udomkarnjananun, S.; Townamchai, N.; Jutivorakool, K. Risk Factors and Clinical Outcomes of Tuberculosis among Kidney Transplant Recipients in High Endemic Country. Transpl. Infect. Dis. 2021, 23, e13566. [Google Scholar] [CrossRef]
- Niewczas, M.; Ziółkowski, J.; Rancewicz, Z.; Szymanska, K.; Kwiatkowski, A.; Gałazka, T.; Senatorski, G.; Paczek, L. Tuberculosis in Patients after Renal Transplantation Remains Still a Clinical Problem. Transplant. Proc. 2002, 34, 677–679. [Google Scholar] [CrossRef]
- Melchor, J.L.; Gracida, C.; Ibarra, A. Increased Frequency of Tuberculosis in Mexican Renal Transplant Recipients: A Single-Center Experience. Transplant. Proc. 2002, 34, 78–79. [Google Scholar] [CrossRef]
- Dridi, A.; Kaaroud, H.; Boubaker, K.; Abdallah, T.B.; El-Younsi, F.; Moussa, F.B.; Hidri, H.; Abderrahim, E.; Khedher, A.; Ben Maïz, H. Tuberculosis in Renal Transplant Recipients. Transplant. Proc. 2003, 35, 2682–2683. [Google Scholar] [CrossRef]
- Guida, J.P.S.; Bignotto Rosane, D.; Urbini-Santos, C.; Alves-Filho, G.; Ribeiro Resende, M.; Mazzali, M. Tuberculosis in Renal Transplant Recipients: A Brazilian Center Registry. Transplant. Proc. 2009, 41, 883–884. [Google Scholar] [CrossRef]
- Ghafari, A.; Makhdoomi, K.; Ahmadpoor, P.; Afshari, A.T.; Fallah, M.M.; Rezaee, K. Tuberculosis in Iranian Kidney Transplant Recipients: A Single-Center Experience. Transplant. Proc. 2007, 39, 1008–1011. [Google Scholar] [CrossRef]
- Matuck, T.A.; Brasil, P.; Alvarenga, M.d.F.A.C.; Morgado, L.; Rels, M.D.; da Costa, A.C.P.; Araújo, M.; Rodrigues, M.E.; de Carvalho, D.d.B.M. Tuberculosis in Renal Transplants in Rio de Janeiro. Transplant. Proc. 2004, 36, 905–906. [Google Scholar] [CrossRef]
- Apaydin, S.; Altiparmak, M.R.; Serdengeçti, K.; Ataman, R.; Oztürk, R.; Erek, E. Mycobacterium Tuberculosis Infections after Renal Transplantation. Scand. J. Infect. Dis. 2000, 32, 501–505. [Google Scholar] [CrossRef]
- Kaaroud, H.; Beji, S.; Boubaker, K.; Abderrahim, E.; Ben Hamida, F.; Ben Abdallah, T.; El Younsi, F.; Ben Moussa, F.; Kheder, A. Tuberculosis after Renal Transplantation. Transplant. Proc. 2007, 39, 1012–1013. [Google Scholar] [CrossRef]
- Basiri, A.; Hosseini-Moghaddam, S.M.; Simforoosh, N.; Einollahi, B.; Hosseini, M.; Foirouzan, A.; Pourrezagholi, F.; Nafar, M.; Zargar, M.A.; Pourmand, G.; et al. The Risk Factors and Laboratory Diagnostics for Post Renal Transplant Tuberculosis: A Case-Control, Country-Wide Study on Definitive Cases. Transpl. Infect. Dis. 2008, 10, 231–235. [Google Scholar] [CrossRef] [PubMed]
- John, G.T.; Shankar, V.; Abraham, A.M.; Mukundan, U.; Thomas, P.P.; Jacob, C.K. Risk Factors for Post-Transplant Tuberculosis. Kidney Int. 2001, 60, 1148–1153. [Google Scholar] [CrossRef] [PubMed]
- Vachharajani, T.; Abreo, K.; Phadke, A.; Oza, U.; Kirpalani, A. Diagnosis and Treatment of Tuberculosis in Hemodialysis and Renal Transplant Patients. Am. J. Nephrol. 2000, 20, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Biz, E.; Pereira, C.A.; Moura, L.A.; Sesso, R.; Vaz, M.L.; Silva Filho, A.P.; Pestana, J.O. The Use of Cyclosporine Modifies the Clinical and Histopathological Presentation of Tuberculosis after Renal Transplantation. Rev. Inst. Med. Trop. Sao Paulo 2000, 42, 225–230. [Google Scholar] [CrossRef]
- Koselj, M.; Kandus, A.; Ales, A.; Bren, A.F. Mycobacterial Infection in Renal Transplant Recipients. Transplant. Proc. 2000, 32, 152–154. [Google Scholar] [CrossRef]
- Sharma, A.K.; Tolani, S.L.; Rathi, G.L.; Gupta, H.P.; Gupta, R. Tuberculosis after Renal Transplantation. Transplant. Proc. 2000, 32, 1959. [Google Scholar] [CrossRef]
- Viana, L.A.; Cristelli, M.P.; Santos, D.W.; Tavares, M.G.; Dantas, M.T.C.; Felipe, C.R.; Silva, H.T.; Pestana, J.M. Influence of Epidemiology, Immunosuppressive Regimens, Clinical Presentation, and Treatment on Kidney Transplant Outcomes of Patients Diagnosed with Tuberculosis: A Retrospective Cohort Analysis. Am. J. Transplant. 2019, 19, 1421–1431. [Google Scholar] [CrossRef]
- Akhtar, S.; Naseem, A.; Dodani, S.; Naqvi, R.; Ahmad, E.; Naqvi, A.; Rizvi, A. Tuberculosis in Renal Transplant Recipients on Isoniazid Prophylaxis. Eur. Respir. J. 2016, 48, PA2104. [Google Scholar] [CrossRef]
- Park, S.; Park, S.; Kim, J.E.; Yu, M.-Y.; Kim, Y.C.; Kim, D.K.; Joo, K.W.; Kim, Y.S.; Han, K.; Lee, H. Risk of Active Tuberculosis Infection in Kidney Transplantation Recipients: A Matched Comparative Nationwide Cohort Study. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2021, 21, 3629–3639. [Google Scholar] [CrossRef]
- Jung, J.Y.; Joo, D.J.; Lee, C.-H.; Park, M.S.; Kim, Y.S.; Kim, M.S.; Kim, S.I.; Kim, Y.S.; Kim, S.K.; Chang, J.; et al. Pre-Transplant Risk Factors for Tuberculosis after Kidney Transplant in an Intermediate Burden Area. Int. J. Tuberc. Lung Dis. 2012, 16, 248–254. [Google Scholar] [CrossRef]
- Meinerz, G.; da Silva, C.K.; Goldani, J.C.; Garcia, V.D.; Keitel, E. Epidemiology of Tuberculosis after Kidney Transplantation in a Developing Country. Transpl. Infect. Dis. 2016, 18, 176–182. [Google Scholar] [CrossRef]
- Costa, S.D.; de Sandes-Freitas, T.V.; Jacinto, C.N.; Martiniano, L.V.M.; Amaral, Y.S.; Paes, F.J.V.N.; Sales, M.L.d.M.B.O.; Esmeraldo, R.d.M.; Daher, E.d.F. Tuberculosis after Kidney Transplantation Is Associated with Significantly Impaired Allograft Function. Transpl. Infect. Dis. 2017, 19, e12750. [Google Scholar] [CrossRef]
- Reis-Santos, B.; Gomes, T.; Horta, B.L.; Maciel, E.L.N. Tuberculosis Prevalence in Renal Transplant Recipients: Systematic Review and Meta-Analysis. J. Bras. Nefrol. 2013, 35, 206–213. [Google Scholar] [CrossRef]
- Al-Efraij, K.; Mota, L.; Lunny, C.; Schachter, M.; Cook, V.; Johnston, J. Risk of Active Tuberculosis in Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Int. J. Tuberc. Lung Dis. 2015, 19, 1493–1499. [Google Scholar] [CrossRef]
- Alemu, A.; Bitew, Z.W.; Diriba, G.; Seid, G.; Eshetu, K.; Chekol, M.T.; Berhe, N.; Gumi, B. Tuberculosis Incidence in Patients with Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2022, 122, 188–201. [Google Scholar] [CrossRef]
- Subramanian, A.K. Tuberculosis in Solid Organ Transplant Candidates and Recipients: Current and Future Challenges. Curr. Opin. Infect. Dis. 2014, 27, 316–321. [Google Scholar] [CrossRef]
- Nasir, N.; Sarfaraz, S.; Khanum, I.; Ansari, T.; Nasim, A.; Dodani, S.K.; Luxmi, S. Tuberculosis in Solid Organ Transplantation: Insights from TB Endemic Areas. Curr. Infect. Dis. Rep. 2021, 23, 14. [Google Scholar] [CrossRef]
- Basiri, A.; Moghaddam, S.M.M.H.; Simforoosh, N.; Einollahi, B.; Hosseini, M.; Foirouzan, A.; Pourrezagholi, F.; Nafar, M.; Zargar, M.A.; Pourmand, G.; et al. Preliminary Report of a Nationwide Case-Control Study for Identifying Risk Factors of Tuberculosis Following Renal Transplantation. Transplant. Proc. 2005, 37, 3041–3044. [Google Scholar] [CrossRef]
- El-Agroudy, A.E.; Refaie, A.F.; Moussa, O.M.; Ghoneim, M.A. Tuberculosis in Egyptian Kidney Transplant Recipients: Study of Clinical Course and Outcome. J. Nephrol. 2003, 16, 404–411. [Google Scholar]
- Pai, M.; Behr, M.A.; Dowdy, D.; Dheda, K.; Divangahi, M.; Boehme, C.C.; Ginsberg, A.; Swaminathan, S.; Spigelman, M.; Getahun, H.; et al. Tuberculosis. Nat. Rev. Dis. Prim. 2016, 2, 16076. [Google Scholar] [CrossRef]
- Singh, N.; Paterson, D.L. Mycobacterium Tuberculosis Infection in Solid-Organ Transplant Recipients: Impact and Implications for Management. Clin. Infect. Dis. 1998, 27, 1266–1277. [Google Scholar] [CrossRef]
- Shu, C.-C.; Tsai, M.-K.; Lin, S.-W.; Wang, J.-Y.; Yu, C.-J.; Lee, C.-Y. Latent Tuberculosis Infection Increases in Kidney Transplantation Recipients Compared With Transplantation Candidates: A Neglected Perspective in Tuberculosis Control. Clin. Infect. Dis. 2020, 71, 914–923. [Google Scholar] [CrossRef]
- Shingde, R.; Habachou, L.I.; Calisa, V.; Craig, J.C.; Tong, A.; Chen, S.C.-A.; Wong, G. Unexpected Donor-Derived Infectious Transmissions by Kidney Transplantation: A Systematic Review. Transpl. Infect. Dis. 2018, 20, e12851. [Google Scholar] [CrossRef]
- Cooper, A.M. Cell-Mediated Immune Responses in Tuberculosis. Annu. Rev. Immunol. 2009, 27, 393–422. [Google Scholar] [CrossRef]
- O’Garra, A.; Redford, P.S.; McNab, F.W.; Bloom, C.I.; Wilkinson, R.J.; Berry, M.P.R. The Immune Response in Tuberculosis. Annu. Rev. Immunol. 2013, 31, 475–527. [Google Scholar] [CrossRef]
- Day, C.L.; Abrahams, D.A.; Lerumo, L.; Janse van Rensburg, E.; Stone, L.; O’rie, T.; Pienaar, B.; de Kock, M.; Kaplan, G.; Mahomed, H.; et al. Functional Capacity of Mycobacterium Tuberculosis-Specific T Cell Responses in Humans Is Associated with Mycobacterial Load. J. Immunol. 2011, 187, 2222–2232. [Google Scholar] [CrossRef]
- Caccamo, N.; Guggino, G.; Joosten, S.A.; Gelsomino, G.; Di Carlo, P.; Titone, L.; Galati, D.; Bocchino, M.; Matarese, A.; Salerno, A.; et al. Multifunctional CD4(+) T Cells Correlate with Active Mycobacterium Tuberculosis Infection. Eur. J. Immunol. 2010, 40, 2211–2220. [Google Scholar] [CrossRef]
- Agarwal, S.K.; Bhowmik, D.; Mahajan, S.; Bagchi, S. Impact of Type of Calcineurin Inhibitor on Post-Transplant Tuberculosis: Single-Center Study from India. Transpl. Infect. Dis. 2017, 19, e12626. [Google Scholar] [CrossRef]
- Abad, C.L.R.; Razonable, R.R. Donor Derived Mycobacterium Tuberculosis Infection after Solid-Organ Transplantation: A Comprehensive Review. Transpl. Infect. Dis. 2018, 20, e12971. [Google Scholar] [CrossRef]
- WHO. Available online: https://www.who.int/publications/i/item/9789241548908 (accessed on 19 August 2022).
- Hadaya, K.; Bridevaux, P.-O.; Roux-Lombard, P.; Delort, A.; Saudan, P.; Martin, P.-Y.; Janssens, J.-P. Contribution of Interferon-γ Release Assays (IGRAs) to the Diagnosis of Latent Tuberculosis Infection After Renal Transplantation. Transplantation 2013, 95, 1485–1490. [Google Scholar] [CrossRef]
- Maciel, M.M.M.D.; Ceccato, M.d.G.; Carvalho, W.d.S.; de Navarro, P.D.; Farah, K.d.P.; de Miranda, S.S. Prevalence of Latent Mycobacterium Tuberculosis Infection in Renal Transplant Recipients. J. Bras. Pneumol. 2018, 44, 461–468. [Google Scholar] [CrossRef] [PubMed]
- Rahimifard, N.; Mahmoudi, S.; Mamishi, S.; Pourakbari, B. Prevalence of Latent Tuberculosis Infection in Transplant Candidates: A Systematic Review and Meta-Analysis. Microb. Pathog. 2018, 125, 401–410. [Google Scholar] [CrossRef] [PubMed]
- Krishnamoorthy, S.; Kumaresan, N.; Zumla, A. Latent Tuberculosis Infection and Renal Transplantation—Diagnosis and Management. Int. J. Infect. Dis. 2019, 80S, S73–S76. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-H.; Lee, S.-O.; Park, J.B.; Park, I.-A.; Park, S.J.; Yun, S.-C.; Jung, J.H.; Kim, Y.H.; Kim, S.C.; Choi, S.-H.; et al. A Prospective Longitudinal Study Evaluating the Usefulness of a T-Cell-Based Assay for Latent Tuberculosis Infection in Kidney Transplant Recipients. Am. J. Transplant. 2011, 11, 1927–1935. [Google Scholar] [CrossRef]
- Graham, J.C.; Kearns, A.M.; Magee, J.G.; El-Sheikh, M.F.; Hudson, M.; Manas, D.; Gould, F.K.; Orr, K.E.; Freeman, R. Tuberculosis Transmitted through Transplantation. J. Infect. 2001, 43, 251–254. [Google Scholar] [CrossRef]
- Malone, A.; McConkey, S.; Dorman, A.; Lavin, P.; Gopthanian, D.; Conlon, P. Mycobacterium Tuberculosis in a Renal Transplant Transmitted from the Donor. Ir. J. Med. Sci. 2007, 176, 233–235. [Google Scholar] [CrossRef]
- Edathodu, J.; Alrajhi, A.; Halim, M.; Althawadi, S. Multi-Recipient Donor-Transmitted Tuberculosis. Int. J. Tuberc. Lung Dis. 2010, 14, 1493–1495. [Google Scholar]
- Al-Nesf, M.A.; Al-Ani, O.I.; Al-Ani, A.A.; Rashed, A.H. Renal allograft tuberculosis with infected lymphocele transmitted from the donor. Saudi J. Kidney Dis. Transpl. 2014, 25, 370–375. [Google Scholar] [CrossRef]
- Bucher, J.N.; Schoenberg, M.B.; Freytag, I.; Lange, U.; Hofmann-Thiel, S.; Guba, M.O.; Werner, J.; Eder, A.; Schelling, G.; Stangl, M. Donor-Derived Tuberculosis after Solid Organ Transplantation in Two Patients and a Staff Member. Infection 2016, 44, 365–370. [Google Scholar] [CrossRef]
- Clemente, W.T.; Faria, L.C.; Cota, G.F.; Amado, L.R.d.N.; Oliveira, J.G.F.; de Miranda, S.S.; Cançado, O.L.; Romanelli, R.M.C.; Lima, A.S.; Frade, L.B.; et al. Donor-Derived Tuberculosis: A Case Report and the Role of Communication Gaps in Transplantation Safety. Case Rep. Transplant. 2021, 2021, 8816426. [Google Scholar] [CrossRef]
- Ulisses, L.R.d.S.; Cardoso, H.S.S.; Alves, I.C.C.; Medeiros, I.N.; de Oliveira, C.G.; de Almeida, T.M.; Castro, F.F.D.S.; da Silva, C.N.G.N.; de Lima, L.V.; Fontoura, R.P.; et al. Donor-Derived TB after Kidney Transplantation: A Case Report. J. Bras. Nefrol. 2022, 44, 126–129. [Google Scholar] [CrossRef]
- Bolt, H.M. Rifampicin, a Keystone Inducer of Drug Metabolism: From Herbert Remmer’s Pioneering Ideas to Modern Concepts. Drug Metab. Rev. 2004, 36, 497–509. [Google Scholar] [CrossRef]
- Nakada, Y.; Yamamoto, I.; Kobayashi, A.; Mafune, A.; Yamakawa, T.; Matsuo, N.; Tanno, Y.; Ohkido, I.; Yamamoto, H.; Yokoyama, K.; et al. Acute Vascular Rejection during Antituberculosis Therapy in a Kidney Transplant Patient. Nephrology 2014, 19 (Suppl. 3), 27–30. [Google Scholar] [CrossRef]
- Chuang, H.-W.; Chung, T.-L.; Lee, P.-T.; Wang, J.-S. Acute Antibody-Mediated Rejection with Graft Loss during Anti-Tuberculosis Therapy in Kidney Transplantation. Kaohsiung J. Med. Sci. 2015, 31, 437–439. [Google Scholar] [CrossRef]
- Chenhsu, R.Y.; Loong, C.C.; Chou, M.H.; Lin, M.F.; Yang, W.C. Renal Allograft Dysfunction Associated with Rifampin-Tacrolimus Interaction. Ann. Pharmacother. 2000, 34, 27–31. [Google Scholar] [CrossRef]
- Sasi, S.; Varghese, M.K.; Nair, A.P.; Hashim, S.; Al Maslamani, M. Tuberculosis in an Allogeneic Transplant Kidney: A Rare Case Report and Review of Literature. Cureus 2020, 12, e11661. [Google Scholar] [CrossRef]
- López-Montes, A.; Gallego, E.; López, E.; Pérez, J.; Lorenzo, I.; Llamas, F.; Serrano, A.; Andrés, E.; Illescas, L.; Gómez, C. Treatment of Tuberculosis with Rifabutin in a Renal Transplant Recipient. Am. J. Kidney Dis. 2004, 44, e59–e63. [Google Scholar] [CrossRef]
- Yoon, H.E.; Jeon, Y.J.; Chung, H.W.; Shin, S.J.; Hwang, H.S.; Lee, S.J.; Chang, Y.K.; Choi, B.S.; Park, C.W.; Kim, Y.S.; et al. Safety and Efficacy of a Quinolone-Based Regimen for Treatment of Tuberculosis in Renal Transplant Recipients. Transplant. Proc. 2012, 44, 730–733. [Google Scholar] [CrossRef]
- De Castilla, D.L.; Rakita, R.M.; Spitters, C.E.; Narita, M.; Jain, R.; Limaye, A.P. Short-Course Isoniazid Plus Rifapentine Directly Observed Therapy for Latent Tuberculosis in Solid-Organ Transplant Candidates. Transplantation 2014, 97, 206–211. [Google Scholar] [CrossRef]
- Milburn, H.; Ashman, N.; Davies, P.; Doffman, S.; Drobniewski, F.; Khoo, S.; Ormerod, P.; Ostermann, M.; Snelson, C. Guidelines for the Prevention and Management of Mycobacterium Tuberculosis Infection and Disease in Adult Patients with Chronic Kidney Disease. Thorax 2010, 65, 559–570. [Google Scholar] [CrossRef]
- Sun, H.-Y.; Singh, N. Opportunistic Infection-Associated Immune Reconstitution Syndrome in Transplant Recipients. Clin. Infect. Dis. 2011, 53, 168–176. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.-Y.; Munoz, P.; Torre-Cisneros, J.; Aguado, J.M.; Lattes, R.; Montejo, M.; Garcia-Reyne, A.; Bouza, E.; Valerio, M.; Lara, R.; et al. Mycobacterium Tuberculosis—Associated Immune Reconstitution Syndrome in Solid-Organ Transplant Recipients. Transplantation 2013, 95, 1173–1181. [Google Scholar] [CrossRef] [PubMed]
- Antony, S.J.; Ynares, C.; Dummer, J.S. Isoniazid Hepatotoxicity in Renal Transplant Recipients. Clin. Transplant. 1997, 11, 34–37. [Google Scholar] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorohan, B.M.; Ismail, G.; Tacu, D.; Obrișcă, B.; Ciolan, G.; Gîngu, C.; Sinescu, I.; Baston, C. Mycobacterium Tuberculosis Infection after Kidney Transplantation: A Comprehensive Review. Pathogens 2022, 11, 1041. https://doi.org/10.3390/pathogens11091041
Sorohan BM, Ismail G, Tacu D, Obrișcă B, Ciolan G, Gîngu C, Sinescu I, Baston C. Mycobacterium Tuberculosis Infection after Kidney Transplantation: A Comprehensive Review. Pathogens. 2022; 11(9):1041. https://doi.org/10.3390/pathogens11091041
Chicago/Turabian StyleSorohan, Bogdan Marian, Gener Ismail, Dorina Tacu, Bogdan Obrișcă, Gina Ciolan, Costin Gîngu, Ioanel Sinescu, and Cătălin Baston. 2022. "Mycobacterium Tuberculosis Infection after Kidney Transplantation: A Comprehensive Review" Pathogens 11, no. 9: 1041. https://doi.org/10.3390/pathogens11091041