
Parapharyngeal Space Tumors: Our Experience
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preoperative Evaluations
2.2. Embolization Treatments
2.3. Statistical Data
3. Results
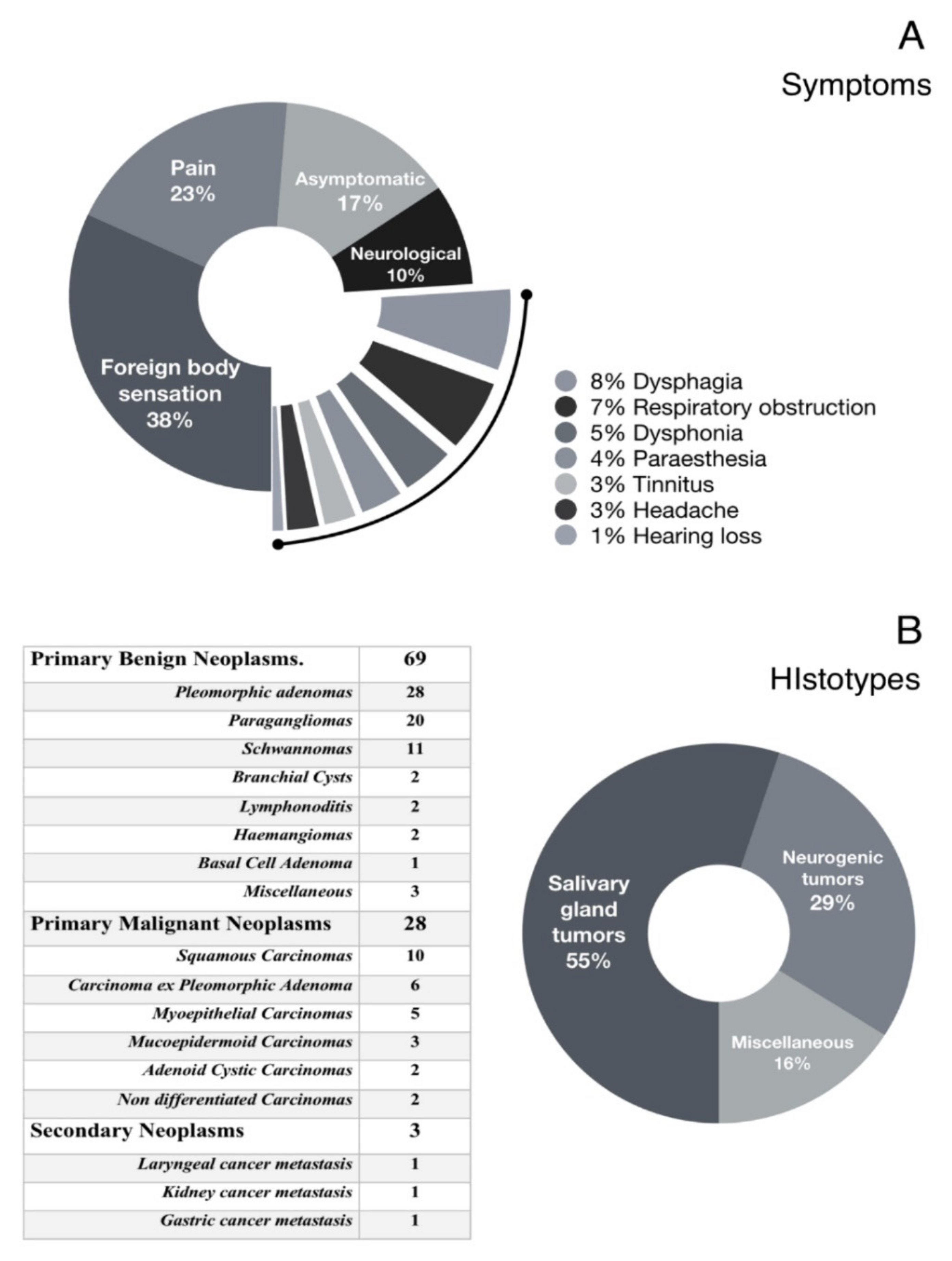
3.1. Clinical Features
3.2. Hystopathologic Diagnoses
3.3. Surgery
3.4. Post-Operative Complications
3.5. Embolization Procedures Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Riffat, F.; Dwivedi, R.C.; Palme, C.; Fish, B.; Jani, P. A systematic review of 1143 parapharyngeal space tumors reported over 20 years. Oral Oncol. 2014, 50, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Kuet, M.-L.; Kasbekar, A.V.; Masterson, L.; Jani, P. Management of tumors arising from the parapharyngeal space: A systematic review of 1,293 cases reported over 25 years. Laryngoscope 2015, 125, 1372–1381. [Google Scholar] [CrossRef] [PubMed]
- van Hees, T.; van Weert, S.; Witte, B.; Leemans, C.R. Tumors of the parapharyngeal space: The VU University Medical Center experience over a 20-year period. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 967–972. [Google Scholar] [CrossRef]
- López, F.; Suárez, C.; Poorten, V.V.; Mäkitie, A.; Nixon, I.J.; Strojan, P.; Hanna, E.Y.; Rodrigo, J.P.; de Bree, R.; Quer, M.; et al. Contemporary management of primary parapharyngeal space tumors. Head Neck 2019, 41, 522–535. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, M.; Schreiber, A.; Mattavelli, D.; Lombardi, D.; Rampinelli, V.; Doglietto, F.; Rodella, L.F.; Nicolai, P. Surgical anatomy of the parapharyngeal space: Multiperspective, quantification-based study. Head Neck 2019, 41, 642–656. [Google Scholar] [CrossRef]
- Fernandes, T.; Lobo, J.C.; Castro, R.; Oliveira, M.I.; Som, P.M. Anatomy and pathology of the masticator space. Insights Imaging 2013, 4, 605–616. [Google Scholar] [CrossRef]
- Li, Q.-Y.; Zhang, S.-X.; Liu, Z.-J.; Tan, L.-W.; Qiu, M.-G.; Li, K.; Cui, G.-Y.; Guo, Y.-L.; Yang, X.-P.; Zhang, W.-G.; et al. The pre-styloid compartment of the parapharyngeal space: A three-dimensional digitized model based on the Chinese Visible Human. Surg. Radiol. Anat. 2004, 26, 411–416. [Google Scholar] [CrossRef]
- Bootz, F.; Greschus, S.; van Bremen, T. Diagnosis and treatment of parapharyngeal space tumors. HNO 2016, 64, 815–821. [Google Scholar] [CrossRef]
- Dallan, I.; Fiacchini, G.; Turri-Zanoni, M.; Seccia, V.; Battaglia, P.; Casani, A.P.; Cristofani-Mencacci, L.; Sellari-Franceschini, S. Endoscopic-assisted transoral-transpharyngeal approach to parapharyngeal space and infratemporal fossa: Focus on feasibility and lessons learned. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3965–3972. [Google Scholar] [CrossRef]
- Chen, W.-L.; Fan, S.; Huang, Z.-Q.; Zhang, D.-M. Endoscopy-assisted transoral versus endoscopy-assisted transcervical minimal incision plus mandibular osteotomy approach in resection of large parapharyngeal space tumors. J. Craniofacial Surg. 2017, 28, 976–979. [Google Scholar] [CrossRef]
- Chu, F.; Tagliabue, M.; Giugliano, G.; Calabrese, L.; Preda, L.; Ansarin, M. From transmandibular to transoral robotic approach for parapharyngeal space tumors. Am. J. Otolaryngol. 2017, 38, 375–379. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, W.J., Jr.; Chandler, J.R. Transoral excision of lateral parapharyngeal space tumors presenting intraorally. Laryngoscope 1988, 98, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Pilolli, F.; Giordano, L.; Galli, A.; Bussi, M. Parapharyngeal space tumours: Video-assisted minimally invasive 12-transcervical approach. Acta Otorhinolaryngol Ital. 2016, 36, 259–264. [Google Scholar] [CrossRef]
- Seethala, R.R. Salivary Gland Tumors: Current Concepts and Controversies. Surg. Pathol. Clin. 2017, 10, 155–176. [Google Scholar] [CrossRef] [PubMed]
- Seifert, G.; Brocheriou, C.; Cardesa, A.; Eveson, J. WHO International Histological Classification of Tumours Tentative Histological Classification of Salivary Gland Tumours. Pathol. Res. Pract. 1990, 186, 555–581. [Google Scholar] [CrossRef]
- Strohl, M.P.; El-Sayed, I.H. Contemporary Management of Parapharyngeal Tumors. Curr. Oncol. Rep. 2019, 21, 103. [Google Scholar] [CrossRef]
- Grilli, G.; Suarez, V.; Muñoz, M.G.; Costales, M.; Llorente, J.L. Parapharyngeal Space Primary Tumours. Acta Otorrinolaringol. 2017, 68, 138–144. [Google Scholar] [CrossRef]
- Weber, A.L. Computed tomography and magnetic resonance imaging of the nasopharynx. Isr. J. Med. Sci. 1992, 28, 161–168. [Google Scholar] [PubMed]
- Stambuk, H.E.; Patel, S.G. Imaging of the Parapharyngeal Space. Otolaryngol. Clin. N. Am. 2008, 41, 77–101. [Google Scholar] [CrossRef]
- Nagornaya, N.; Bhatia, R.G. Imaging for Parapharyngeal Space Tumors, Poststyloid Parapharyngeal Space Paraganglioma. In Encyclopedia of Otolaryngology, Head and Neck Surgery; Kountakis, S.E., Ed.; Springer: Berlin/Heidelberg, Germany, 2013; pp. 1256–1259. [Google Scholar]
- Farrag, T.Y.; Lin, F.R.; Koch, W.M.; Califano, J.A.; Cummings, C.W.; Farinola, M.A.; Tufano, R.P. The role of pre-operative CT-guided FNAB for parapharyngeal space tumors. Otolaryngol. Head Neck Surg. 2007, 136, 411–414. [Google Scholar] [CrossRef]
- Kim, J.W.; Ryu, C.H.; Doo, H.; Choi, Y.J.; Lee, J.H.; Cho, K.-J.; Roh, J.-L.; Choi, S.-H.; Kim, S.Y.; Nam, S.Y. PP094: Diagnostic accuracy of CT/MRI and FNAB for parapharyngeal space tumors. Oral Oncol. 2013, 49 (Suppl. 1), S126. [Google Scholar] [CrossRef]
- Bradley, P.J.; Bradley, P.T.; Olsen, K.D. Update on the management of parapharyngeal tumours. Curr. Opin. Otolaryngol. Head Neck Surg. 2011, 19, 92–98. [Google Scholar] [CrossRef]
- Abbas, J.R.; Hamlett, K.E.L.; de Carpentier, J. Image-guided transnasal endoscopic fine needle aspiration or biopsy of parapharyngeal space tumours. J. Laryngol. Otol. 2018, 132, 1026–1028. [Google Scholar] [CrossRef] [PubMed]
- Khafif, A.; Segev, Y.; Kaplan, D.M.; Gil, Z.; Fliss, D.M. Surgical management of parapharyngeal space tumors: A 10-year review. Otolaryngol. Head Neck Surg. 2005, 132, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Mydlarz, W.K.; Agrawal, N. Transparotid and transcervical approaches for removal of deep lobe parotid gland and parapharyngeal space tumors. Oper. Tech. Otolaryngol. Head Neck Surg. 2014, 25, 234–239. [Google Scholar] [CrossRef]
- Carrau, R.L.; Myers, E.N.; Johnson, J.T. Management of Tumors Arising in the Parapharyngeal Space. Laryngoscope 1990, 100, 583–589. [Google Scholar] [CrossRef] [PubMed]
- Basaran, B.; Polat, B.; Unsaler, S.; Ulusan, M.; Aslan, I.; Hafiz, G. Parapharyngeal space tumours: The efficiency of a transcervical approach without mandibulotomy through review of 44 cases. Acta Otorhinolaryngol. Ital. 2014, 34, 310–316. [Google Scholar] [PubMed]
- Sheahan, P. Transcervical approach for removal of benign parapharyngeal space tumors. Oper. Tech. Otolaryngol. Head Neck Surg. 2014, 25, 227–233. [Google Scholar] [CrossRef]
- Abdel-Haleem, A.; El Sayed, A.; Hakeem, H.A. Transmandibular approach in parapharyngeal tumors: When to do it? Egypt. J. Ear Nose Throat Allied Sci. 2011, 12, 25–31. [Google Scholar] [CrossRef]
- Betka, J.; Chovanec, M.; Klozar, J.; Taudy, M.; Plzák, J.; Kodetová, D.; Lisý, J. Transoral and combined transoral-transcervical approach in the surgery of parapharyngeal tumors. Eur. Arch. Oto-Rhino-Laryngol. 2010, 267, 765–772. [Google Scholar] [CrossRef]
- Ducic, Y.; Oxford, L.; Pontius, A.T. Transoral Approach to the Superomedial Parapharyngeal Space. Otolaryngol. Head Neck Surg. 2006, 134, 466–470. [Google Scholar] [CrossRef]
- Panda, S.; Sikka, K.; Thakar, A.; Sharma, S.C.; Krishnamurthy, P. Transoral robotic surgery for the parapharyngeal space: Expanding the transoral corridor. J. Robot. Surg. 2020, 14, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Floros, P.; Sorrentino, M.; Magnuson, J.S. Transoral robotic parapharyngeal approach to the submandibular space. Head Neck 2020, 42, 3776–3778. [Google Scholar] [CrossRef] [PubMed]
- Rizzo-Riera, E.; Rubi-Oña, C.; García-Wagner, M.; Costa, A.A.-D.; Miralles, J.; Enchev, E.; Rama-López, J. Advanced Robotic Surgery of the Parapharyngeal Space: Transoral Robotic Styloidectomy in Eagle Syndrome. J. Craniofacial Surg. 2020, 31, 2339–2341. [Google Scholar] [CrossRef] [PubMed]
- Duek, I.; Amit, M.; Sviri, G.E.; Gil, Z. Combined endoscopic transcervical-transoral robotic approach for resection of parapharyngeal space tumors. Head Neck 2017, 39, 786–790. [Google Scholar] [CrossRef]
- Maglione, M.; Guida, A.; Pavone, E.; Longo, F.; Aversa, C.; Villano, S.; Ionna, F. Transoral robotic surgery of parapharyngeal space tumours: A series of four cases. Int. J. Oral Maxillofac. Surg. 2018, 47, 971–975. [Google Scholar] [CrossRef]
- Arshad, H.; Durmus, K.; Ozer, E. Transoral robotic resection of selected parapharyngeal space tumors. Eur. Arch. Oto-Rhino-Laryngol. 2012, 270, 1737–1740. [Google Scholar] [CrossRef]
- Chan, J.Y.K.; Tsang, R.K.; Eisele, D.W.; Richmon, J.D. Transoral robotic surgery of the parapharyngeal space: A case series and systematic review. Head Neck 2015, 37, 293–298. [Google Scholar] [CrossRef]
- Chu, F.; De Berardinis, R.; Tagliabue, M.; Zorzi, S.; Bandi, F.; Ansarin, M. The Role of Transoral Robotic Surgery for Parapharyngeal Space: Experience of a Tertiary Center. J. Craniofacial Surg. 2020, 31, 117–120. [Google Scholar] [CrossRef]
- Weinstein, G.S.; O’Malley, B.W., Jr.; Desai, S.C.; Quon, H. Transoral robotic surgery: Does the ends justify the means? Curr. Opin. Otolaryngol. Head Neck Surg. 2009, 17, 126–131. [Google Scholar] [CrossRef] [Green Version]
- Pedicelli, A.; Lozupone, E.; Valente, I.; Snider, F.; Rigante, M.; D’Argento, F.; Alexandre, A.; Garignano, G.; Chiumarulo, L.; Paludetti, G.; et al. Pre-operative direct puncture embolization of head and neck hypervascular tumors using SQUID 12. Interv. Neuroradiol. 2020, 26, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Hashizume, T.; Shimohira, M.; Ohta, K.; Suzuki, K.; Sawada, Y.; Nakamura, Y.; Suzuki, M.; Murakami, S.; Shibamoto, Y. Preoperative transcatheter arterial embolization using a gelatin sponge for head and neck tumors. Minim. Invasive Ther. Allied Technol. 2018, 28, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Valavanis, A. Preoperative embolization of the head and neck: Indications, patient selection, goals, and precautions. Am. J. Neuroradiol. 1986, 7, 943–952. [Google Scholar] [PubMed]
- Pérez-García, C.; Rosati, S.; Serrano-Hernando, F.J.; Aliño, L.L.-I.; Moreu, M. Preoperative Squid embolization of carotid paragangliomas with direct puncture. Neuroradiol. J. 2020, 33, 224–229. [Google Scholar] [CrossRef]
- Moreno-Paredes, S.; Rodríguez-Alcalá, L.; Martínez, J.M.-L.; Locatelli, N.M.; López, C.V.; Fernández, J.L.V.; Peña, Á.C. Facial palsy after embolization with Squid® 12. BMC Neurol. 2021, 21, 45. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Surgical Approach | N | % | MTS (cm) | TM (min) |
|---|---|---|---|---|
| Transmandibular | 15 | 16 | 8.3 | 239.5 |
| Transcervical | 55 | 57 | 3.9 | 74.6 |
| Transoral | 26 | 27 | 2.9 | 54.5 |
| Transmandibular (N = 15) | Transcervical (N = 55) | Transoral (N = 26) | |
|---|---|---|---|
| Non-neurologic | 4/15 (26.6%) | 1/55 (1.8%) | 3/26 (11.6%) |
| Ab-ingestis Pneumonia | 2 | - | - |
| Persistent local pain | 1 | - | - |
| Dyspnea | |||
| Vomit | - | - | 1 |
| Disorientation | 1 | - | - |
| Trismus | - | - | - |
| Hemorrhage | - | - | 2 |
| Neurologic | 6/15 (40%) | 10/55 (18.2%) | - |
| Vagus nerve injury | 5 | - | - |
| Glossopharyngeal injury | 1 | - | - |
| Facial nerve injury | - | 6 | - |
| Spinal nerve injury | - | 2 | - |
| Recurrent nerve injury | - | 2 | - |
| Aesthetic Outcome | 5/15 (30%) | 3/55 (5.5%) | - |
| Lip numbness | 3 | - | - |
| Unsightly scar | 2 | 3 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galli, J.; Rolesi, R.; Gallus, R.; Seccia, A.; Pedicelli, A.; Bussu, F.; Scarano, E. Parapharyngeal Space Tumors: Our Experience. J. Pers. Med. 2023, 13, 283. https://doi.org/10.3390/jpm13020283
Galli J, Rolesi R, Gallus R, Seccia A, Pedicelli A, Bussu F, Scarano E. Parapharyngeal Space Tumors: Our Experience. Journal of Personalized Medicine. 2023; 13(2):283. https://doi.org/10.3390/jpm13020283
Chicago/Turabian StyleGalli, Jacopo, Rolando Rolesi, Roberto Gallus, Annalisa Seccia, Alessandro Pedicelli, Francesco Bussu, and Emanuele Scarano. 2023. "Parapharyngeal Space Tumors: Our Experience" Journal of Personalized Medicine 13, no. 2: 283. https://doi.org/10.3390/jpm13020283