
Donor, Recipient and Surgeon Sex and Sex-Concordance and their Impact on Liver Transplant Outcome

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wallis, C.J.D.; Jerath, A.; Coburn, N.; Klaassen, Z.; Luckenbaugh, A.N.; Magee, D.E.; Hird, A.E.; Armstrong, K.; Ravi, B.; Esnaola, N.F.; et al. Association of Surgeon-Patient Sex Concordance With Postoperative Outcomes. JAMA Surg. 2022, 157, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Wallis, C.J.; Ravi, B.; Coburn, N.; Nam, R.K.; Detsky, A.S.; Satkunasivam, R. Comparison of postoperative outcomes among patients treated by male and female surgeons: A population based matched cohort study. BMJ 2017, 359, j4366. [Google Scholar] [CrossRef]
- Tsugawa, Y.; Jena, A.B.; Figueroa, J.F.; Orav, E.J.; Blumenthal, D.M.; Jha, A.K. Comparison of Hospital Mortality and Readmission Rates for Medicare Patients Treated by Male vs Female Physicians. JAMA Intern. Med. 2017, 177, 206–213. [Google Scholar] [CrossRef]
- Gross, R.; McNeill, R.; Davis, P.; Lay-Yee, R.; Jatrana, S.; Crampton, P. The association of gender concordance and primary care physicians' perceptions of their patients. Women Health 2008, 48, 123–144. [Google Scholar] [CrossRef]
- Malhotra, J.; Rotter, D.; Tsui, J.; Llanos, A.A.M.; Balasubramanian, B.A.; Demissie, K. Impact of Patient–Provider Race, Ethnicity, and Gender Concordance on Cancer Screening: Findings from Medical Expenditure Panel Survey. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1804–1811. [Google Scholar] [CrossRef]
- Greenwood, B.N.; Carnahan, S.; Huang, L. Patient-physician gender concordance and increased mortality among female heart attack patients. Proc. Natl. Acad. Sci. USA 2018, 115, 8569–8574. [Google Scholar] [CrossRef]
- Schieber, A.-C.; Delpierre, C.; Lepage, B.; Afrite, A.; Pascal, J.; Cases, C.; Lombrail, P.; Lang, T.; Kelly-Irving, M.; INTERMEDE Group. Do gender differences affect the doctor–patient interaction during consultations in general practice? Results from the INTERMEDE study. Fam. Pract. 2014, 31, 706–713. [Google Scholar] [CrossRef]
- Bertakis, K.D.; Helms, L.J.; Callahan, E.J.; Azari, R.; Robbins, J.A. The influence of gender on physician practice style. Med. Care 1995, 33, 407–416. [Google Scholar] [CrossRef]
- Lurie, N.; Slater, J.; McGovern, P.; Ekstrum, J.; Quam, L.; Margolis, K. Preventive care for women. Does the sex of the physician matter? N. Engl. J. Med. 1993, 329, 478–482. [Google Scholar] [CrossRef]
- Carpenter, A.-M.; Tan, S.A.; Costopoulos, K.; Cooper, L.A.; Sarosi, G.A.; Shaw, C.M. Gender Diversity in General Surgery Residency Leadership. J. Surg. Educ. 2018, 75, e68–e71. [Google Scholar] [CrossRef]
- Schizas, D.; Papapanou, M.; Routsi, E.; Mastoraki, A.; Lidoriki, I.; Zavras, N.; Avgerinos, D.V.; Lazaris, A.M.; Tsaroucha, A. Career barriers for women in surgery. Surgeon 2022, 20, 275–283. [Google Scholar] [CrossRef] [PubMed]
- AAMC. The State of Women in Academic Medicine: The Pipeline and Pathways to Leadership. Available online: https://www.aamc.org/members/gwims/statistics/ (accessed on 22 December 2022).
- Cullaro, G.; Sarkar, M.; Lai, J.C. Sex-based disparities in delisting for being "too sick" for liver transplantation. Am. J. Transplant. 2018, 18, 1214–1219. [Google Scholar] [CrossRef] [PubMed]
- Melk, A.; Babitsch, B.; Borchert-Mörlins, B.; Claas, F.; Dipchand, A.I.; Eifert, S.; Eiz-Vesper, B.; Epping, J.; Falk, C.S.; Foster, B.; et al. Equally Interchangeable? How Sex and Gender Affect Transplantation. Transplantation 2019, 103, 1094–1110. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.M.; Heimbach, J.K.; Larson, J.J.; Mara, K.C.; Kim, W.R.; Kamath, P.S.; Therneau, T.M. Reduced Access to Liver Transplantation in Women: Role of Height, MELD Exception Scores, and Renal Function Underestimation. Transplantation 2018, 102, 1710–1716. [Google Scholar] [CrossRef]
- Cholongitas, E.; Marelli, L.; Kerry, A.; Goodier, D.W.; Nair, D.; Thomas, M.; Patch, D.; Burroughs, A.K. Female liver transplant recipients with the same GFR as male recipients have lower MELD scores—A systematic bias. Am. J. Transplant. 2007, 7, 685–692. [Google Scholar] [CrossRef]
- Mindikoglu, A.L.; Regev, A.; Seliger, S.L.; Magder, L.S. Gender disparity in liver transplant waiting-list mortality: The importance of kidney function. Liver Transpl. 2010, 16, 1147–1157. [Google Scholar] [CrossRef]
- Myers, R.P.; Shaheen, A.A.; Aspinall, A.I.; Quinn, R.R.; Burak, K.W. Gender, renal function, and outcomes on the liver transplant waiting list: Assessment of revised MELD including estimated glomerular filtration rate. J. Hepatol. 2011, 54, 462–470. [Google Scholar] [CrossRef]
- Lai, J.C.; Terrault, N.A.; Vittinghoff, E.; Biggins, S.W. Height contributes to the gender difference in wait-list mortality under the MELD-based liver allocation system. Am. J. Transplant. 2010, 10, 2658–2664. [Google Scholar] [CrossRef]
- Nephew, L.D.; Goldberg, D.S.; Lewis, J.D.; Abt, P.; Bryan, M.; Forde, K.A. Exception Points and Body Size Contribute to Gender Disparity in Liver Transplantation. Clin. Gastroenterol. Hepatol. 2017, 15, 1286–1293.e2. [Google Scholar] [CrossRef]
- Yeow, M.; Soh, S.; Wong, J.; Tan, E.; Ganpathi Iyer, S. Gender Diversity in Transplantation Leadership Positions in Transplantation. J. Organizations. Transplant. 2022, 106, e352–e353. [Google Scholar] [CrossRef]
- Choubey, A.P.; Bullock, B.; Choubey, A.S.; Pai, K.; Ortiz, A.C.; Khan, S.A.; Mishra, A.; James, R.; Koizumi, N.; Pearson, T.; et al. Transplant surgery departmental leaders do not represent workforce demographics especially among women and underrepresented minorities—A retrospective analysis. Am. J. Surg. 2022, 224, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Coburn, N.; Wallis, C.J.D.; Baxter, N. Links between age and sex of surgeons and patients’ outcomes. BMJ 2018, 361, k1691. [Google Scholar] [CrossRef]
- AAMC. ACGME Residents and Fellows by Sex and Specialty. Available online: https://www.aamc.org/data-reports/workforce/interactive-data/acgme-residents-and-fellows-sex-and-specialty-2017 (accessed on 22 December 2022).
- Riner, A.N.; Herremans, K.M.; Neal, D.W.; Johnson-Mann, C.; Hughes, S.J.; McGuire, K.P.; Upchurch, G.R., Jr.; Trevino, J.G. Diversification of Academic Surgery, Its Leadership, and the Importance of Intersectionality. JAMA Surg. 2021, 156, 748–756. [Google Scholar] [CrossRef] [PubMed]
- Kaldas, F.M.; Rocca, J.P.; Bhati, C.S.; Duan, N.; Evenson, A.R.; Tan, H.P.; Redfield, R.R.; di Sabato, D.M.; Yoshida, A.; Abt, P.L.; et al. The Abdominal Transplant Surgery Workforce: Current state and future trends. Clin. Transplant. 2019, 33, e13659. [Google Scholar] [CrossRef] [PubMed]
- de Rosner-van Rosmalen, M.; Adelmann, D.; Berlakovich, G.A.; Francoz, C.; Selzner, N.; Berenguer, M.; Watt, K.D.; Man, N.K.; Burra, P.; Pai, S.-L. Women Leadership in Liver Transplantation—Results of an International Survey. Transplantation 2022, 106, 1699–1702. [Google Scholar] [CrossRef]
- Legaz, I.; Navarro Noguera, E.; Bolarín, J.M.; Campillo, J.A.; Moya, R.; Luna, A.; Miras, M.; Minguela, A.; Álvarez-López, M.R.; Muro, M. Patient Sex in the Setting of Liver Transplant in Alcoholic Liver Disease. Exp. Clin. Transplant. 2019, 17, 355–362. [Google Scholar] [CrossRef]
- Bolarín, J.M.; Pérez-Cárceles, M.D.; Hernández Del Rincón, J.P.; Luna, A.; Minguela, A.; Muro, M.; Legaz, I. Causes of Death and Survival in Alcoholic Cirrhosis Patients Undergoing Liver Transplantation: Influence of the Patient’s Clinical Variables and Transplant Outcome Complications. Diagnostics 2021, 11, 968. [Google Scholar] [CrossRef]
- Moylan, C.A.; Brady, C.W.; Johnson, J.L.; Smith, A.D.; Tuttle-Newhall, J.E.; Muir, A.J. Disparities in liver transplantation before and after introduction of the MELD score. Jama 2008, 300, 2371–2378. [Google Scholar] [CrossRef]
- Mathur, A.K.; Schaubel, D.E.; Gong, Q.; Guidinger, M.K.; Merion, R.M. Sex-based disparities in liver transplant rates in the United States. Am. J. Transplant. 2011, 11, 1435–1443. [Google Scholar] [CrossRef] [Green Version]
- Croome, K.P.; Segal, D.; Hernandez-Alejandro, R.; Adams, P.C.; Thomson, A.; Chandok, N. Female donor to male recipient gender discordance results in inferior graft survival: A prospective study of 1,042 liver transplants. J. Hepato-Biliary-Pancreat. Sci. 2014, 21, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.W.; Han, S.; Lee, S.; Cha, H.H.; Ahn, S.; Ahn, H.S.; Ko, J.S.; Gwak, M.S.; Kim, G.S.; Joh, J.W.; et al. Higher Risk of Posttransplant Liver Graft Failure in Male Recipients of Female Donor Grafts Might Not Be Due to Anastomotic Size Disparity. Transplantation 2018, 102, 1115–1123. [Google Scholar] [CrossRef] [PubMed]
- Wallis, C.J.D.; Jerath, A.; Kaneshwaran, K.; Hallet, J.; Coburn, N.; Wright, F.C.; Conn, L.G.; Bischof, D.; Covelli, A.; Klaassen, Z.; et al. Association Between Surgeon and Anesthesiologist Sex Discordance and Postoperative Outcomes: A Population-based Cohort Study. Ann. Surg. 2022, 276, 81–87. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
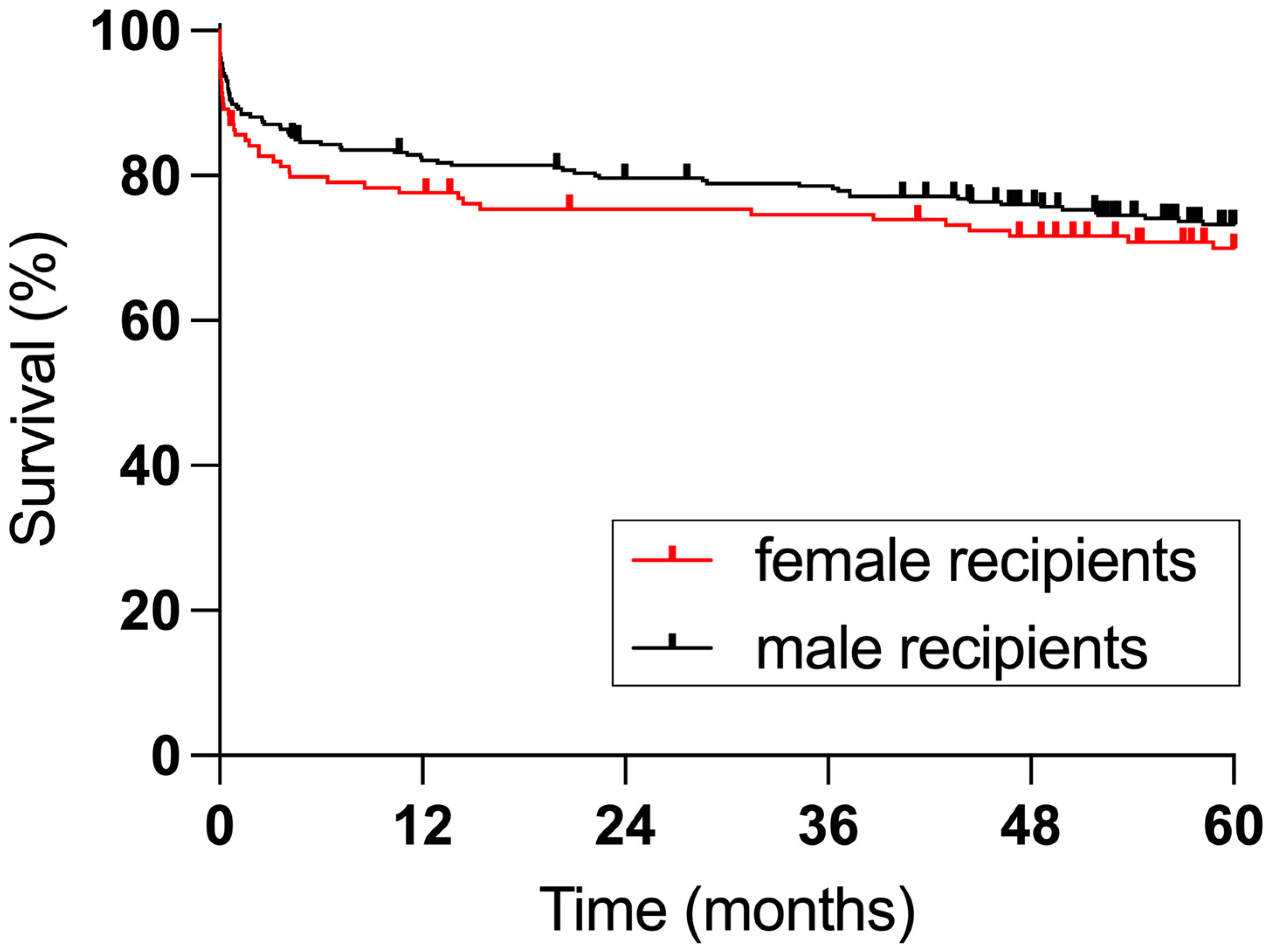
| Female Recipients (n = 139) | Male Recipients (n = 286) | p | |
|---|---|---|---|
| Age (yrs) | 51 (18–69) | 55 (18–71) | 0.0594 |
| BMI (kg/m2) | 24.4 (15.1–41.5) | 26.2 (16.1–44.3) | 0.0009 |
| MELD score | 16 (6–40) | 15 (6–40) | 0.0716 |
| Diagnosis (%) | <0.0001 | ||
| acute liver failure | 15.1 | 3.8 | |
| alcoholic cirrhosis | 17.3 | 21.0 | |
| hepatitis B/C | 5.8 | 14.0 | |
| HCC | 5.0 | 9.1 | |
| NASH | 15.1 | 25.5 | |
| PBC/PSC/AIH | 20.1 | 15.0 | |
| other | 21.6 | 11.5 | |
| Donor Risk Index | 1.837 (1.040–2.855) | 1.746 (0.9730–2.678) | 0.0272 |
| CIT (min) | 477 (226–1020) | 470 (175–949) | 0.5411 |
| WIT (min) | 28 (16–65) | 30 (16–80) | 0.0009 |
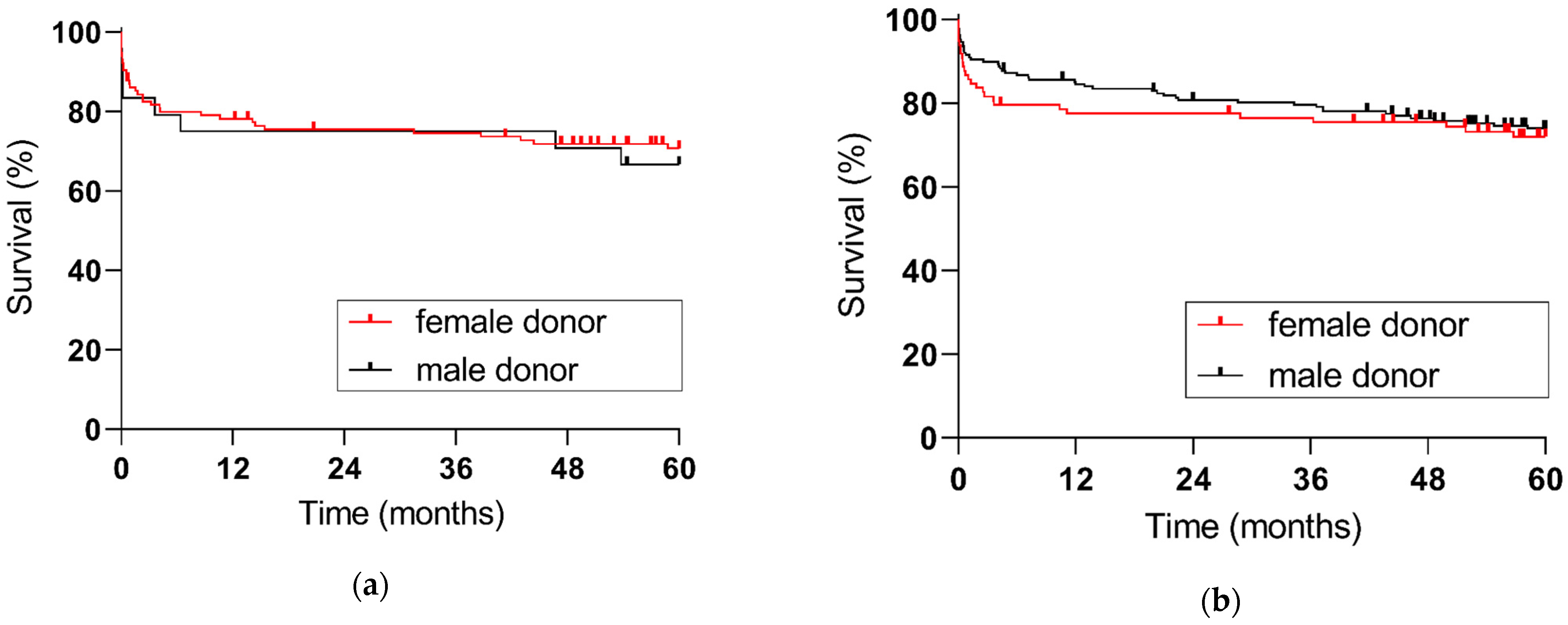
| Female Donor (n = 213) | Male Donor (n = 212) | p | |
|---|---|---|---|
| Age (yrs) | 60 (1–89) | 56 (1–87) | 0.0182 |
| BMI (kg/m2) | 25.6 (12.5–51.4) | 26.3 (13.3–58.8) | 0.0012 |
| DRI | 1.908 (0.9730–2.678) | 1.672 (0.9730–2.855) | <0.0001 |
| Brain death (%) | 0.0185 | ||
| Trauma | 7.98 | 13.21 | |
| Anoxia | 17.37 | 25.00 | |
| CVA | 69.01 | 54.25 | |
| other | 5.63 | 7.55 |
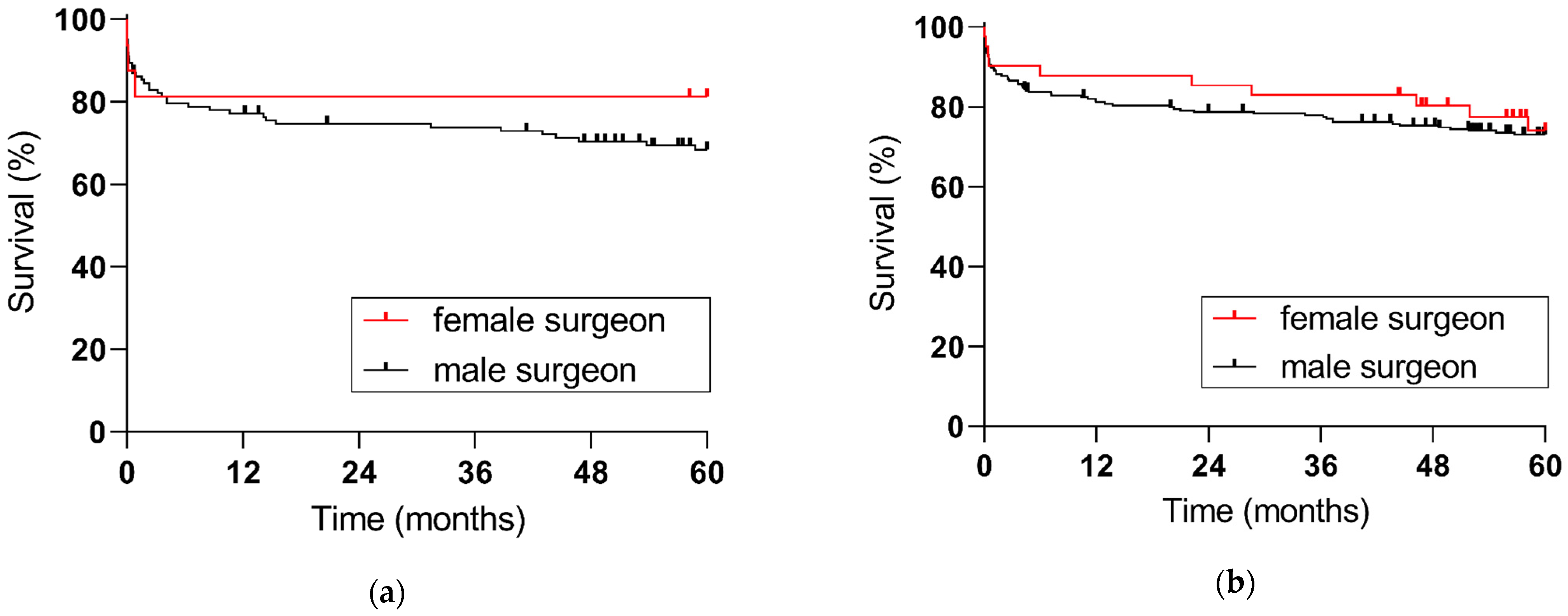
| Female Surgeon (n = 57) | Male Surgeon (n = 368) | p | |
|---|---|---|---|
| Recipient age | 54 (20–69) | 54 (18–71) | 0.5664 |
| Recipient BMI (kg/m2) | 26.5 (15.1–44.3) | 25.4 (16.1–43.6) | 0.4979 |
| Recipient MELD | 14 (7–40) | 16 (6–40) | 0.1452 |
| DRI | 1.837 (1.053–2.255) | 1.768 (0.9730–2.855) | 0.8372 |
| CIT (min) | 440 (323–787) | 472 (175–1020) | 0.3699 |
| WIT (min) | 34 (16–65) | 29 (16–80) | 0.0002 |
| Hazard Ratio (HR) | 95% Confidence Interval (CI) | p | |
|---|---|---|---|
| Recipient female sex | 0.991 | 0.579, 1.697 | 0.975 |
| Recipient age (per 10 yrs.) | 1.204 | 1.017, 1.425 | 0.031 |
| MELD Score | 1.042 | 1.022, 1.063 | <0.001 |
| Donor Risk Index | 1.311 | 0.797, 2.155 | 0.286 |
| Surgeon-recipient sex concordance | 1.074 | 0.638, 1.809 | 0.788 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazilescu, L.I.; Bernheim, I.; Treckmann, J.; Radunz, S. Donor, Recipient and Surgeon Sex and Sex-Concordance and their Impact on Liver Transplant Outcome. J. Pers. Med. 2023, 13, 281. https://doi.org/10.3390/jpm13020281
Mazilescu LI, Bernheim I, Treckmann J, Radunz S. Donor, Recipient and Surgeon Sex and Sex-Concordance and their Impact on Liver Transplant Outcome. Journal of Personalized Medicine. 2023; 13(2):281. https://doi.org/10.3390/jpm13020281
Chicago/Turabian StyleMazilescu, Laura Ioana, Isabel Bernheim, Jürgen Treckmann, and Sonia Radunz. 2023. "Donor, Recipient and Surgeon Sex and Sex-Concordance and their Impact on Liver Transplant Outcome" Journal of Personalized Medicine 13, no. 2: 281. https://doi.org/10.3390/jpm13020281