
Bioelectrical Impedance Analysis for Preoperative Volemia Assessment in Living Donor Hepatectomy

Abstract
:1. Introduction
2. Patients and Methods
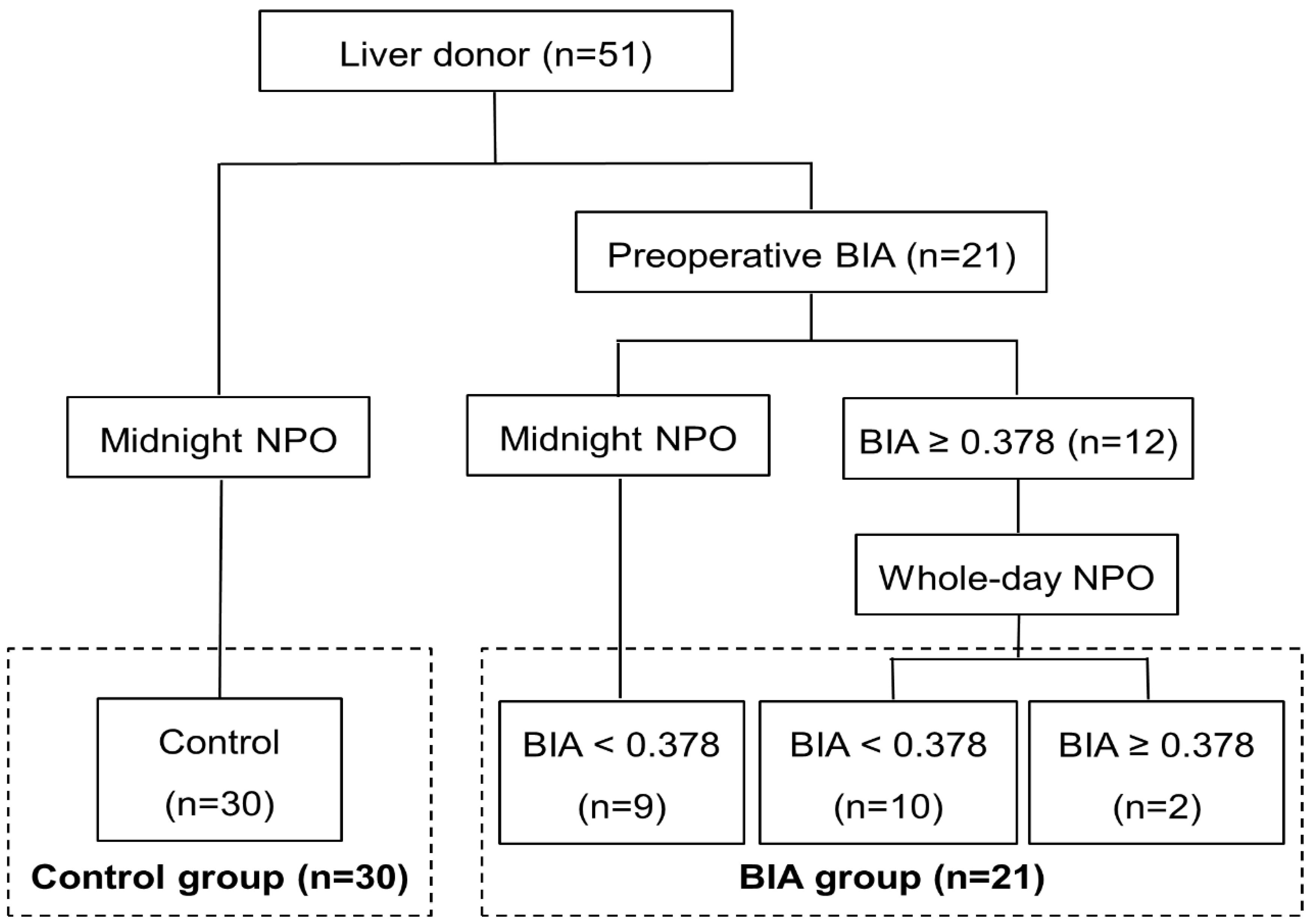
2.1. Patients
2.2. Data Collection
2.3. BIA
2.4. Anesthetic and Surgical Technique
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Humar, A.; Ganesh, S.; Jorgensen, D.; Tevar, A.; Ganoza, A.; Molinari, M.; Hughes, C. Adult living donor versus deceased donor liver transplant (LDLT versus DDLT) at a single center: Time to change our paradigm for liver transplant. Ann. Surg. 2019, 270, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Tran, L.; Humar, A. Current status of adult liver transplantation: Utilization of living donor versus deceased donor graft. Curr. Opin. Organ. Transplant. 2021, 26, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, K.; Shindoh, J.; Margonis, G.A.; Nishioka, Y.; Andreatos, N.; Sekine, A.; Hashimoto, M.; Pawlik, T.M. Effect of background liver cirrhosis on outcomes of hepatectomy for hepatocellular carcinoma. JAMA Surg. 2017, 152, e165059. [Google Scholar] [CrossRef]
- Menahem, B.; Lubrano, J.; Duvoux, C.; Mulliri, A.; Alves, A.; Costentin, C.; Mallat, A.; Launoy, G.; Laurent, A. Liver transplantation versus liver resection for hepatocellular carcinoma in intention to treat: An attempt to perform an ideal meta-analysis. Liver Transpl. 2017, 23, 836–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niemann, C.U.; Feiner, J.; Behrends, M.; Eilers, H.; Ascher, N.L.; Roberts, J.P. Central venous pressure monitoring during living right donor hepatectomy. Liver Transpl. 2007, 13, 266–271. [Google Scholar] [CrossRef]
- Topaloglu, S.; Yesilcicek, C.K.; Calik, A.; Aydin, C.; Kocyigit, S.; Yaman, H.; Kutanis, D.; Karabulut, E.; Dohman, D.; Orem, A.; et al. Efficacy and safety of hepatectomy performed with intermittent portal triad clamping with low central venous pressure. Biomed Res. Int. 2013, 2013, 297971. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.J.; Ventham, N.T.; Harrison, E.M.; Wigmore, S.J. Central venous pressure and liver resection: A systematic review and meta-analysis. HPB 2015, 17, 863–871. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.L.; Wang, W.J.; Wang, W.J.; Cao, N. Effectiveness and safety of controlled venous pressure in liver surgery: A systematic review and network meta-analysis. BioMed Res Int. 2015, 2015, 290234. [Google Scholar] [CrossRef] [Green Version]
- Yu, L.; Sun, H.; Jin, H.; Tan, H. The effect of low central venous pressure on hepatic surgical field bleeding and serum lactate in patients undergoing partial hepatectomy: A prospective randomized controlled trial. BMC Surg. 2020, 20, 25. [Google Scholar] [CrossRef] [Green Version]
- Davies, S.J.; Davenport, A. The role of bioimpedance and biomarkers in helping to aid clinical decision-making of volume assessments in dialysis patients. Kidney Int. 2014, 86, 489–496. [Google Scholar] [CrossRef]
- Zhu, F.; Levin, N.W. Estimation of body composition and normal fluid status using a calf bioimpedance technique. Blood Purif. 2015, 39, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Lopot, F.; Nejedly, B.; Novotna, H.; Mackova, M.; Sulkova, S. Age-related extracellular to total body water volume ratio (Ecv/TBW)--can it be used for “dry weight” determination in dialysis patients? Application of multifrequency bioimpedance measurement. Int. J. Artif. Organs 2002, 25, 762–769. [Google Scholar] [CrossRef] [PubMed]
- Suh, S.W.; Park, H.J.; Choi, Y.S. Preoperative volume assessment using bioelectrical impedance analysis for minimizing blood loss during hepatic resection. HPB 2022, 24, 568–574. [Google Scholar] [CrossRef] [PubMed]
- Suh, K.S.; Suh, S.W.; Lee, J.M.; Choi, Y.; Yi, N.J.; Lee, K.W. Recent advancements in and views on the donor operation in living donor liver transplantation: A single-center study of 886 patients over 13 years. Liver Transpl. 2015, 21, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Ryu, H.G.; Nahm, F.S.; Sohn, H.M.; Jeong, E.J.; Jung, C.W. Low central venous pressure with milrinone during living donor hepatectomy. Am. J. Transplant. 2010, 10, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Mullen, J.T.; Ribero, D.; Reddy, S.K.; Donadon, M.; Zorzi, D.; Gautam, S.; Abdalla, E.K.; Curley, S.A.; Capussotti, L.; Clary, B.M.; et al. Hepatic insufficiency and mortality in 1059 noncirrhotic patients undergoing major hepatectomy. J. Am. Coll. Surg. 2007, 204, 854–864. [Google Scholar] [CrossRef]
- Yi, N.J.; Suh, K.S.; Cho, J.Y.; Lee, H.W.; Cho, E.H.; Yang, S.H.; Cho, Y.B.; Lee, K.U. Three-quarters of right liver donors experienced postoperative complications. Liver Transpl. 2007, 13, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Sun, Y.M.; Wu, F.X.; Yang, L.Q.; Lu, Z.J.; Yu, W.F. Controlled low central venous pressure reduces blood loss and transfusion requirements in hepatectomy. World J. Gastroenterol. 2014, 20, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Chin, J.H.; Kang, S.J.; Jun, I.G.; Song, J.G.; Jeong, S.M.; Park, J.Y.; Hwang, G.S. Association between central venous pressure and blood loss during hepatic resection in 984 living donors. Acta Anaesthesiol. Scand. 2009, 53, 601–606. [Google Scholar] [CrossRef]
- Shin, Y.H.; Ko, J.S.; Kim, G.S.; Gwak, M.S.; Sim, W.S.; Lee, A.R.; Yi, H.W.; Joh, J.W. Impact of hepatic macrovesicular and microvesicular steatosis on the postoperative liver functions after right hepatectomy in living donors. Transplant. Proc. 2012, 44, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Low, S.; Chin, M.C.; Ma, S.; Heng, D.; Deurenberg-Yap, M. Rationale for redefining obesity in Asians. Ann. Acad. Med. Singap. 2009, 38, 66–69. [Google Scholar] [PubMed]
- Saunders, J.K.; Rosman, A.S.; Neihaus, D.; Gouge, T.H.; Melis, M. Safety of hepatic resections in obese veterans. Arch. Surg. 2012, 147, 331–337. [Google Scholar] [PubMed] [Green Version]
- McCormack, L.; Petrowsky, H.; Jochum, W.; Furrer, K.; Clavien, P.A. Hepatic steatosis is a risk factor for postoperative complications after major hepatectomy: A matched case-control study. Ann. Surg. 2007, 245, 923–930. [Google Scholar] [CrossRef]
- Dunki-Jacobs, E.M.; Philips, P.; Scoggins, C.R.; McMasters, K.M.; Martin, R.C.G., II. Stroke volume variation in hepatic resection: A replacement for standard central venous pressure monitoring. Ann. Surg. Oncol. 2014, 21, 473–478. [Google Scholar] [CrossRef]
- Shih, T.H.; Tsou, Y.H.; Huang, C.J.; Chen, C.L.; Cheng, K.W.; Wu, S.C.; Yang, S.S.; Juang, S.E.; Huang, C.E.; Lee, Y.E.; et al. The correlation between CVP and SVV and intraoperative minimal blood loss in living donor hepatectomy. Transplant. Proc. 2018, 50, 2661–2663. [Google Scholar] [CrossRef]
- Correa-Gallego, C.; Berman, A.; Denis, S.C.; Langdon-Embry, L.; O’Connor, D.; Arslan-Carlon, V.; Kingham, T.P.; D’Angelica, M.I.; Allen, P.J.; Fong, Y.; et al. Renal function after low central venous pressure-assisted liver resection: Assessment of 2116 cases. HPB 2015, 17, 258–264. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BIA Group (n = 21) | Control Group (n = 30) | p | |
|---|---|---|---|
| Age, mean (years) | 39.0 (±12.5) | 36.9 (±10.2) | 0.510 |
| Age ≥ 50 (%) | 3 (14.3%) | 3 (10.0%) | 0.640 |
| Male (%) | 11 (52.4%) | 20 (66.7%) | 0.304 |
| Diabetes mellitus | 0 | 2 (6.7%) | 0.227 |
| Hypertension | 0 | 2 (6.7%) | 0.227 |
| BMI, kg/m2 | 23.4 (±2.7) | 24.5 (±2.9) | 0.187 |
| BMI ≥ 25, (%) | 6 (28.6%) | 11 (36.7%) | 0.546 |
| Hepatic steatosis | 1.4 (±2.3) | 1.8 (±2.6) | 0.574 |
| Macrosteatosis ≥ 10% | 0 | 1 (3.3%) | 0.360 |
| Remnant volume, mean (%) | 35.0 (±3.3) | 36.5 (±4.1) | 0.163 |
| Remnant volume < 30% (%) | 1 (4.3%) | 2 (7.1%) | 0.673 |
| Baseline liver function | |||
| TB (mg/dL) | 0.6 (±0.2) | 0.6 (±0.2) | 0.879 |
| Albumin (g/dL) | 4.6 (±0.2) | 4.5 (±0.4) | 0.476 |
| INR | 1.03 (±0.06) | 1.04 (±0.06) | 0.464 |
| Baseline renal function | |||
| Creatinine (mg/dL) | 0.7 (±0.2) | 0.7 (±0.2) | 0.978 |
| BIA Group (n = 21) | Control Group (n = 30) | p | |
|---|---|---|---|
| Operative duration, min | 240.5 (±45.6) | 276.5 (±54.0) | 0.016 |
| Hepatectomy time, min | 167.5 (±32.5) | 203.9 (±42.6) | 0.002 |
| Intraoperative fluids | |||
| Crystalloid, mL | 2623 (±646) | 2452 (±586) | 0.329 |
| Colloid, mL | 183 (±242) | 267 (±254) | 0.245 |
| Urine output, mL | 306 (±170) | 324 (±172) | 0.707 |
| Estimated blood loss, mL | 325 (±212) | 382 (±210) | 0.349 |
| Blood transfusion | 0 | 0 | - |
| Inotropics usage | 9 (39.1%) | 9 (32.1%) | 0.603 |
| Pleural effusion | 2 (9.5%) | 1 (3.3%) | 0.355 |
| AKI | 1 (4.8%) | 2 (7.1%) | 0.731 |
| Postoperative liver insufficiency | 0 | 2 (7.1%) | 0.191 |
| Major postoperative complication | 0 | 0 | - |
| Postoperative hospital stay, days | 10.4 (±2.2) | 10.8 (±3.6) | 0.679 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | p | OR | 95% CI | p |
| Age (yrs) | 0.994 | 0.945–1.045 | 0.809 | |||
| Male | 0.711 | 0.228–2.220 | 0.557 | |||
| Diabetes mellitus | 1.227 | 0.073–20.763 | 0.887 | |||
| Hypertension | - | |||||
| BMI ≥ 25 | 2.308 | 0.703–7.570 | 0.168 | |||
| Macrosteatosis ≥ 10% | - | |||||
| Remnant volume < 30% | 2.571 | 0.218–30.318 | 0.453 | |||
| Baseline liver function | ||||||
| TB (mg/dL) | 0.232 | 0.014–3.910 | 0.311 | |||
| Albumin (g/dL) | 0.671 | 0.118–4.041 | 0.681 | |||
| INR | - | |||||
| Preoperative BIA | 4.318 | 1.296–14.383 | 0.017 | 6.914 | 1.699–28.191 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suh, S.-W. Bioelectrical Impedance Analysis for Preoperative Volemia Assessment in Living Donor Hepatectomy. J. Pers. Med. 2022, 12, 1755. https://doi.org/10.3390/jpm12111755
Suh S-W. Bioelectrical Impedance Analysis for Preoperative Volemia Assessment in Living Donor Hepatectomy. Journal of Personalized Medicine. 2022; 12(11):1755. https://doi.org/10.3390/jpm12111755
Chicago/Turabian StyleSuh, Suk-Won. 2022. "Bioelectrical Impedance Analysis for Preoperative Volemia Assessment in Living Donor Hepatectomy" Journal of Personalized Medicine 12, no. 11: 1755. https://doi.org/10.3390/jpm12111755