
Quality of Life after Surgical Treatment for Chronic Otitis Media: A Systematic Review of the Literature
 , ,
, ,
Abstract
:1. Introduction
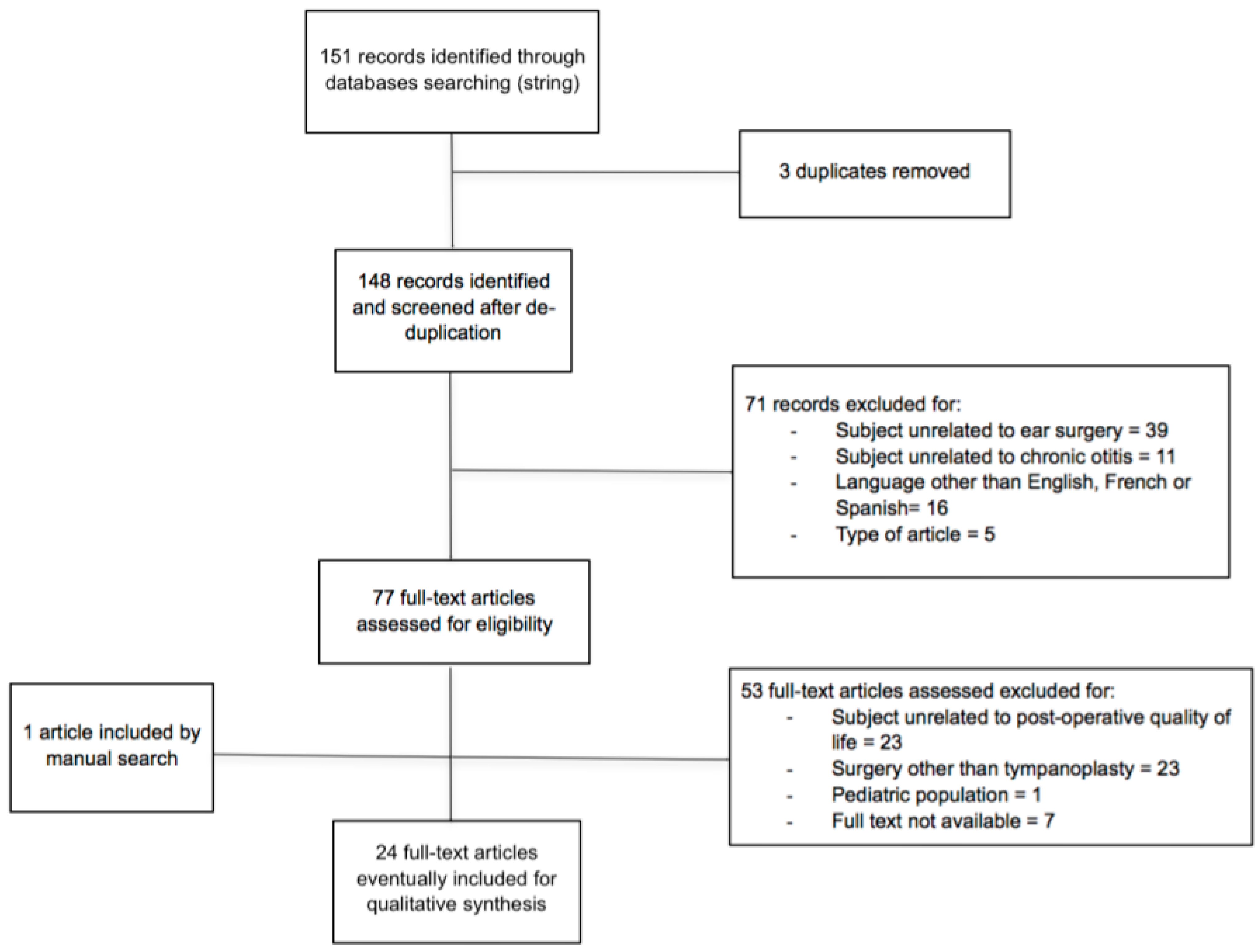
2. Methods
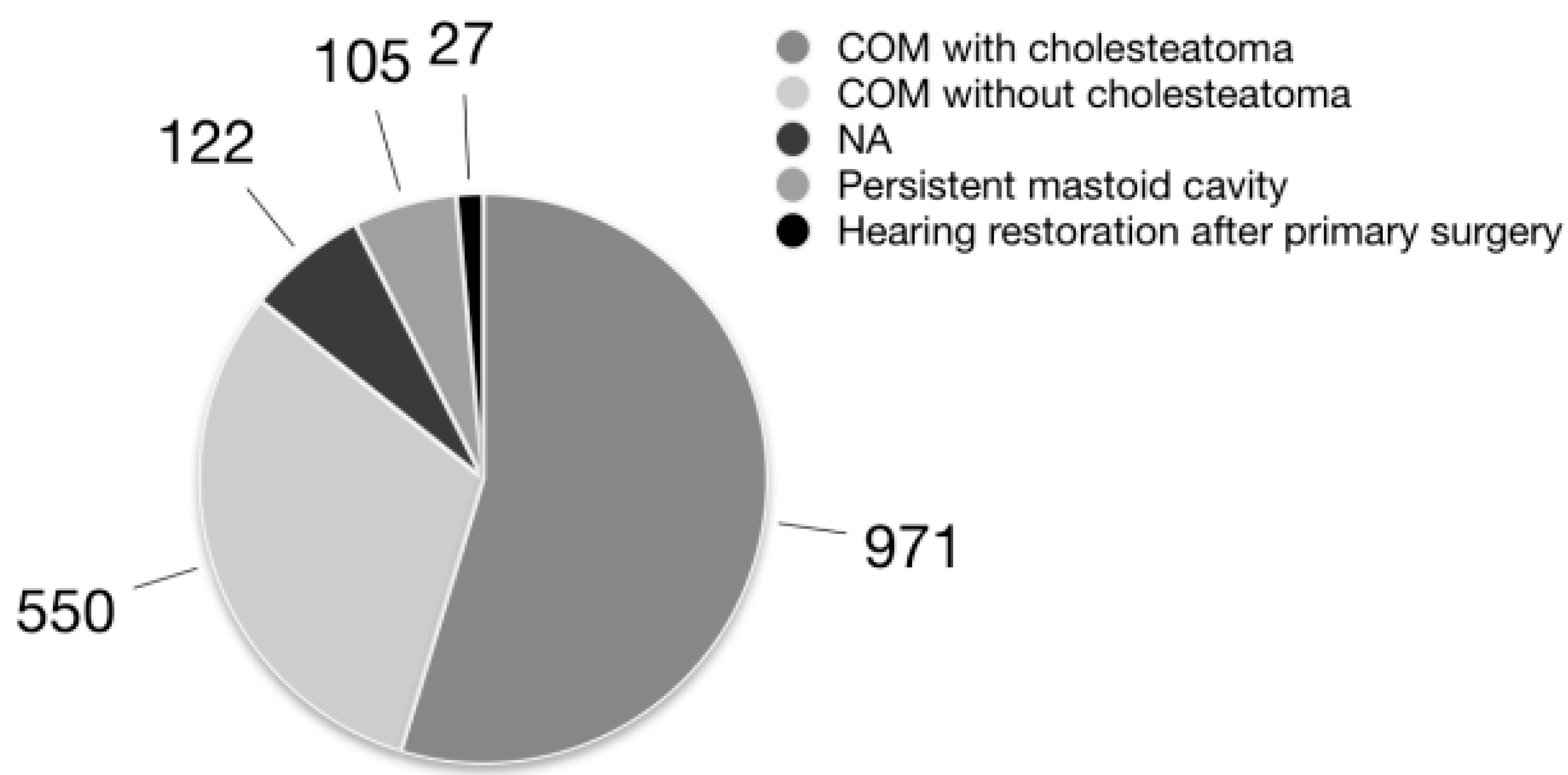
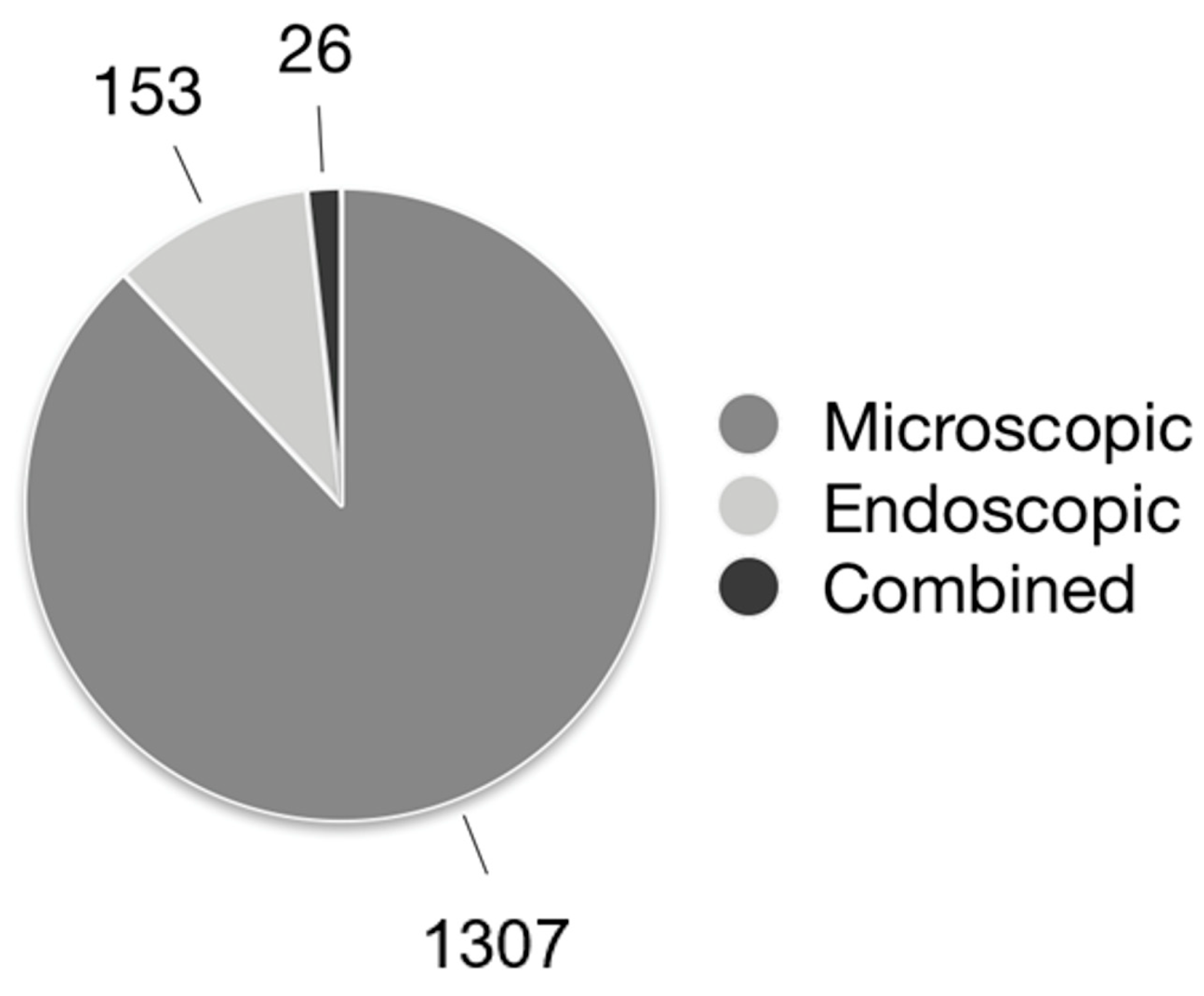
3. Results
4. Discussion
4.1. Questionnaires
4.2. Surgical Technique
4.3. Primary vs. Revision Surgery
4.4. Post-Operative Hearing and QoL
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dornhoffer, J.L.; Smith, J.; Richter, G.; Boeckmann, J. Impact on Quality of Life after Mastoid Obliteration. Laryngoscope 2008, 118, 1427–1432. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.S.; Yung, M.W. A systematic review of patient-reported outcome measures for chronic suppurative otitis media. Laryngoscope 2016, 126, 1458–1463. [Google Scholar] [CrossRef] [PubMed]
- Tarabichi, M.; Ayache, S.; Nogueira, J.F.; Al Qahtani, M.; Pothier, D.D. Endoscopic management of chronic otitis media and tympanoplasty. Otolaryngol. Clin. N. Am. 2013, 46, 155–163. [Google Scholar] [CrossRef]
- Baumann, I.; Gerendas, B.; Plinkert, P.K.; Praetorius, M. General and disease-specific quality of life in patients with chronic suppurative otitis media—A prospective study. Health Qual. Life Outcomes 2011, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Si, Y.; Chen, Y.; Xu, G.; Chen, X.; He, W.; Zhang, Z. Cartilage tympanoplasty combined with eustachian tube balloon dilatation in the treatment of adhesive otitis media. Laryngoscope 2019, 129, 1462–1467. [Google Scholar] [CrossRef]
- Lucidi, D.; De Corso, E.; Paludetti, G.; Sergi, B. Quality of life and functional results in canal wall down vs canal wall up mastoidectomy. Acta Otorhinolaryngol. Ital. 2019, 39, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Quaranta, N.; Iannuzzi, L.; Petrone, P.; D’Elia, A.; Quaranta, A. Quality of Life after Cholesteatoma Surgery: Intact–Canal Wall Tympanoplasty versus Canal Wall–Down Tympanoplasty with Mastoid Obliteration. Ann. Otol. Rhinol. Laryngol. 2014, 123, 89–93. [Google Scholar] [CrossRef]
- Berling Holm, K.; Bornefalk-Hermansson, A.; Knutsson, J.; von Unge, M. Surgery for Chronic Otitis Media Causes Greater Taste Disturbance Than Surgery for Otosclerosis. Otol. Neurotol. 2019, 40, e32–e39. [Google Scholar] [CrossRef] [Green Version]
- Baetens, W.; Dinther, J.V.; Vanspauwen, R.; Maryn, Y.; Zarowski, A.; Offeciers, E. Health Related Quality of Life after the Bony Obliteration Tympanoplasty for COM with Cholesteatoma using the COMQ12—A Disease Specific PROM. J. Int. Adv. Otol. 2019, 15, 396–399. [Google Scholar] [CrossRef]
- Jung, K.H.; Cho, Y.S.; Hong, S.H.; Chung, W.H.; Lee, G.J.; Hong, S.D. Quality-of-life assessment after primary and revision ear surgery using the chronic ear survey. Arch. Otolaryngol. Head Neck Surg. 2010, 136, 358–365. [Google Scholar] [CrossRef]
- Maile, E.J.; Tharu, P.B.; Blanchford, H.L.; Edmiston, R.; Youngs, R. Quality of life of Nepali patients with ear disease before and after corrective surgery. Trop. Med. Int. Health 2015, 20, 1041–1047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uluyol, S.; Ugur, O.; Arslan, I.B.; Yagiz, O.; Gumussoy, M.; Cukurova, I. Effects of cavity reconstruction on morbidity and quality of life after canal wall down tympanomastoidectomy. Braz. J. Otorhinolaryngol. 2018, 84, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.Y.; Cho, Y.S.; Lee, N.J.; Lee, J.; Chung, W.H.; Hong, S.H. Factors associated with quality of life after ear surgery in patients with chronic otitis media. Arch. Otolaryngol. Head Neck Surg. 2012, 138, 840–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Westerberg, J.; Mäki-Torkko, E.; Harder, H. The evaluation of canal wall up cholesteatoma surgery with the Glasgow Benefit Inventory. Eur. Arch. Otorhinolaryngol. 2020, 277, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, K.; Vaid, L.; Taneja, H.C. Effect of Type 1 Tympanoplasty on the Quality of Life of CSOM Patients. Indian J. Otolaryngol. Head Neck Surg. 2016, 68, 468–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lailach, S.; Kemper, M.; Lasurashvili, N.; Beleites, T.; Zahnert, T.; Neudert, M. Health-related quality of life measurement after cholesteatoma surgery: Comparison of three different surgical techniques. Eur. Arch. Otorhinolaryngol. 2015, 272, 3177–3185. [Google Scholar] [CrossRef]
- Bernardeschi, D.; Pyatigorskaya, N.; Russo, F.Y.; De Seta, D.; Corallo, G.; Ferrary, E.; Nguyen, Y.; Sterkers, O. Anatomical, functional and quality-of-life results for mastoid and epitympanic obliteration with bioactive glass s53p4: A prospective clinical study. Clin. Otolaryngol. 2017, 42, 387–396. [Google Scholar] [CrossRef] [Green Version]
- Kurien, G.; Greeff, K.; Gomaa, N.; Ho, A. Mastoidectomy and mastoid obliteration with autologous bone graft: A quality of life study. J. Otolaryngol. Head Neck Surg. 2013, 42, 49. [Google Scholar] [CrossRef] [Green Version]
- Weiss, N.M.; Bächinger, D.; Rrahmani, A.; Bernd, H.E.; Huber, A.; Mlynski, R.; Röösli, C. Mapping the ChOLE classification to hearing outcomes and disease-specific health-related quality of life. Eur. Arch. Otorhinolaryngol. 2020, 277, 2729–2738. [Google Scholar] [CrossRef]
- Weiss, N.M.; Bächinger, D.; Botzen, J.; Großmann, W.; Mlynski, R. Mastoid cavity obliteration leads to a clinically significant improvement in health-related quality of life. Eur. Arch. Otorhinolaryngol. 2020, 277, 1637–1643. [Google Scholar] [CrossRef]
- Lailach, S.; Langanke, T.; Zahnert, T.; Garthus-Niegel, S.; Neudert, M. Impact of depressive disorders on quality of life after middle ear surgery in patients with chronic otitis media. Eur. Arch. Otorhinolaryngol. 2021, 278, 3217–3225. [Google Scholar] [CrossRef] [PubMed]
- Bächinger, D.; Großmann, W.; Mlynski, R.; Weiss, N.M. Characteristics of health-related quality of life in different types of chronic middle ear disease. Eur. Arch. Otorhinolaryngol. 2021, 278, 3795–3800. [Google Scholar] [CrossRef]
- Bächinger, D.; Mlynski, R.; Weiss, N.M. Establishing the minimal clinically important difference (MCID) of the Zurich Chronic Middle Ear Inventory (ZCMEI-21) in patients treated for chronic middle ear disease. Eur. Arch. Otorhinolaryngol. 2020, 277, 1039–1044. [Google Scholar] [CrossRef] [Green Version]
- Taneja, V.; Milner, T.D.; Iyer, A. Endoscopic ear surgery: Does it have an impact on quality of life? Our experience of 152 cases. Clin. Otolaryngol. 2020, 45, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Mishra, A.K.; Mallick, A.; Galagali, J.R.; Gupta, A.; Sethi, A.; Ghotra, A. Mastoid cavity obliteration using bone pâté versus bioactive glass granules in the management of chronic otitis media (squamous disease): A prospective comparative study. J. Laryngol. Otol. 2021, 135, 492–500. [Google Scholar] [CrossRef] [PubMed]
- Lucidi, D.; Reale, M.; Fermi, M.; Bassano, E.; Bonali, M.; Fernandez, I.J.; Presutti, L.; Alicandri-Ciufelli, M. Disease-specific quality of life and psychological distress after endoscopic tympanoplasty. Eur. Arch. Otorhinolaryngol. 2022, 279, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Nadol, J.B.; Staecker, H.; Gliklich, R.E. Outcomes assessment for chronic otitis media: The Chronic Ear Survey. Laryngoscope 2000, 110, 32–35. [Google Scholar] [CrossRef]
- Baumann, I.; Kurpiers, B.; Plinkert, P.K.; Praetorius, M. Development and validation of the Chronic Otitis Media Outcome Test 15 (COMOT-15). Measurement of health-related quality of life in patients with chronic otitis media. HNO 2009, 57, 889–895. [Google Scholar] [CrossRef]
- Bächinger, D.; Röösli, C.; Ditzen, B.; Huber, A.M. Development and validation of the Zurich chronic middle ear inventory (ZCMEI-21): An electronic questionnaire for assessing quality of life in patients with chronic otitis media. Eur. Arch. Oto-Rhino-Laryngol. 2016, 273, 3073–3081. [Google Scholar] [CrossRef]
- Robinson, K.; Gatehouse, S.; Browning, G.G. Measuring patient benefit from otorhinolaryngological surgery and therapy. Ann. Otol. Rhinol. Laryngol. 1996, 105, 415–422. [Google Scholar] [CrossRef]
- Tulachan, B.; Swar, R.; Borgohain, B.N. Comparison of Healing Time Following Modified Radical Mastoidectomy with or without Mastoid Cavity Obliteration. Glob. J. Otolaryngol. 2018, 15, 555921. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Terminology to Identify Chronic Otitis Media and Its Variants as the Treated Pathology | Number of Articles Using It |
|---|---|
| Chronic otitis media (COM) with or without cholesteatoma | 7 |
| Cholesteatoma | 6 |
| Chronic suppurative otitis media (CSOM) with or without cholesteatoma | 4 |
| Cholesteatoma vs. inflammatory mucosa/process | 2 |
| Chronic otitis media (COM) vs. cholesteatoma | 2 |
| Chronic otitis media squamous disease with cholesteatoma | 1 |
| Mucosal vs. squamous chronic otitis media | 1 |
| Adhesive otitis media | 1 |
| Authors | Year | N Of Patients Eventually Included | Surgery | Comparison of Qol between Groups | Questionnaires | Quality of Evidence | Risk of Bias | |
|---|---|---|---|---|---|---|---|---|
| 1 | Baumann I. et al. [4] | 2011 | 90 | TPL | Preop vs. postop | COMOT-15; SF-36 | Low | Low |
| 2 | Si Y. et al. [5] | 2018 | 120 | TPL with or without ETBD | No surgery vs. ETBD vs. CT vs. CT + ETBD | THI; COMOT-15; ETS | High | Low |
| 3 | Lucidi D. et al. [6] | 2019 | 81 | CWU TPL and CWD TPL without obliteration | CWU TPL vs. CWD TPL without obliteration | CES; COMOT-15 | Moderate | Low |
| 4 | Quaranta N. et al. [7] | 2014 | 100 | CWU TPL and CWD TPL with obliteration | CWU TPL vs. CWD TPL with obliteration | CES | Moderate | Low |
| 5 | Berling Holm K. et al. [8] | 2018 | 37 | Middle ear surgery (not better specified) | Preop vs. postop in cholesteatoma group; cholesteatoma vs. otosclerosis | SF-36 | Low | Low |
| 6 | Baetens W. et al. [9] | 2019 | 26 | CWD TPL with obliteration | Preop vs. postop | COMQ-12 | Low | High |
| 7 | Jung K.H. et al. [10] | 2010 | 41 | CWU TPL and CWD TPL | Primary vs. revision surgery | CES | Low | Low |
| 8 | Maile E.J. et al. [11] | 2015 | 161 | Middle ear surgery (not better specified) | Preop vs. postop | GBI | Low | Low |
| 9 | Uluyol S. et al. [12] | 2018 | 22 | CWD TPL and CWD TPL with reconstruction | CWD TPL vs. CWD TPL with reconstruction | GBI | Low | Low |
| 10 | Choi S.Y. et al. [13] | 2012 | 156 | TPL with or without mastoidectomy | Preop vs. postop | CES | Moderate | High |
| 11 | Westerberg J. et al. [14] | 2020 | 34 | CWU TPL with obliteration | Preop vs. postop | GBI | Low | High |
| 12 | Bhatia K. et al. [15] | 2016 | 37 | Type 1 TPL | Preop vs. postop | COM-5 | Low | High |
| 13 | Lailach S. et al. [16] | 2015 | 97 | ETC; TCM; CWD TPL with obliteration | ETC vs. TCM vs. CWD with obliteration | COMOT-15 | Moderate | Low |
| 14 | Bernardeschi D. et al. [17] | 2016 | 39 | CWU TPL and CWD TPL with epitympanic and mastoid obliteration with bioactive glass s53p4 | CWD TPL VS. CWU TPL; primary versus revision surgery; cholesteatoma vs. non-cholesteatomatous otitis media | GBI and a surgery-specific questionnaire | Low | High |
| 15 | Kurien G. et al. [18] | 2013 | 58 | CWD TPL with primary or secondary obliteration | Primary vs. secondary obliteration | GBI | Low | High |
| 16 | Dornhoffer J.L. et al. [1] | 2008 | 23 | Revision of open cavity with secondary obliteration | Preop vs. postop | GBI with three additional, surgery-specific questions | Low | High |
| 17 | Weiss N.M., Bächinger D., Rrahmani A., et al. [19] | 2020 | 54 | NA | Comparison between patients with different cholesteatoma stage according to the ChOLE classification | ZCMEI-21 | Moderate | High |
| 18 | Weiss N.M., Bächinger D., Botzen J., et al. [20] | 2020 | 25 | Revision of open cavity with secondary obliteration | Preop vs. postop | ZCMEI-21 | Low | High |
| 19 | Lailach S. et al. [21] | 2021 | 102 | CWU TPL and CWD TPL | Preop vs. postop | COMOT-15, ZCMEI-21, SF-36, PHQ-9 | Moderate | High |
| 20 | Bächinger D., Großmann W. et al. [22] | 2021 | 108 | CWU TPL, CWD TPL, secondary obliteration, hearing restoration surgery | Cholesteatoma vs. COM vs. PMC | ZCMEI-21 | Low | High |
| 21 | Bächinger D., Mlynski R. et al. [23] | 2020 | 103 | CWU TPL, CWD TPL, secondary obliteration, hearing restoration surgery | Cholesteatoma vs. COM vs. PMC | ZCMEI-21 | Moderate | High |
| 22 | Taneja V. et al. [24] | 2020 | 108 | TEES, microscopic TPL, micro-endoscopic TPL | Endoscopic vs. microscopic and combined approaches; cholesteatoma vs. non-cholesteatomatous otitis media | GBI | Moderate | Low |
| 23 | Mishra A.K. et al. [25] | 2021 | 68 | CWD TPL with obliteration | Bone patè vs. bioactive glass obliteration | GBI | High | Low |
| 24 | Lucidi D. et al. [26] | 2022 | 85 | TEES and open centrifugal endoscopic tympanoplasty | Cholesteatoma vs. COM; primary vs. revision surgery; endoscopic transcanal vs. open centrifugal TPL | CES; DASS-21 | Moderate | High |
| Questionnaire for Quality of Life Assessment | Number of Articles Using It |
|---|---|
| GBI | 8 |
| CES | 5 |
| COMOT-15 | 5 |
| ZCMEI-21 | 5 |
| SF-36 | 3 |
| COM-5 | 1 |
| SURGERY-SPECIFIC QUESTIONNAIRES | 2 |
| COMQ-12 | 1 |
| PHQ-9 | 1 |
| THI | 1 |
| ETS | 1 |
| DASS-21 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucidi, D.; Cantaffa, C.; Nocini, R.; Martone, A.; Alicandri-Ciufelli, M.; Marchioni, D.; Presutti, L.; Molinari, G. Quality of Life after Surgical Treatment for Chronic Otitis Media: A Systematic Review of the Literature. J. Pers. Med. 2022, 12, 1959. https://doi.org/10.3390/jpm12121959
Lucidi D, Cantaffa C, Nocini R, Martone A, Alicandri-Ciufelli M, Marchioni D, Presutti L, Molinari G. Quality of Life after Surgical Treatment for Chronic Otitis Media: A Systematic Review of the Literature. Journal of Personalized Medicine. 2022; 12(12):1959. https://doi.org/10.3390/jpm12121959
Chicago/Turabian StyleLucidi, Daniela, Carla Cantaffa, Riccardo Nocini, Andrea Martone, Matteo Alicandri-Ciufelli, Daniele Marchioni, Livio Presutti, and Giulia Molinari. 2022. "Quality of Life after Surgical Treatment for Chronic Otitis Media: A Systematic Review of the Literature" Journal of Personalized Medicine 12, no. 12: 1959. https://doi.org/10.3390/jpm12121959