
Subjective Perception and Psychoacoustic Aspects of the Laryngectomee Voice: The Impact on Quality of Life
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Clinical Series
2.2. Quality of Life Measurements
2.2.1. The V-RQoL Questionnaire (Appendix A)
2.2.2. The SECEL Questionnaire (Appendix B)
2.3. The INFVo Scale
Speech Samples
- Emission of the isolated and prolonged vowel /a/ at a comfortable pitch and intensity;
- Automatic seriations, as progressive numbering from 1 to 10;
- reading aloud a short, standardized text, consisting of 5 sentences for a total of 100 syllables;
- A repetition test (the examiner says a word and the patient must repeat it) of phonetically balanced words, which includes all the phonemes of the Italian language;
- An oral diadochokinesis test, in which the patient was asked to pronounce the 3 syllables of the sequence [PA/TA/KA] in five seconds as quickly as possible.
- Maximum phonation time (MPT), in seconds, by measuring the length of the prolonged emission;
- Proportion of the vocal structure (PV), which depends on the number of speech pauses during the production of automatic series;
- Percentage of speech (in syllables per second), which is calculated on the basis of the time needed to read the chosen text;
- Number of phonetic distortions or substitutions occurred during the word repetition test;
- Oral diadochokinesis (DDK), in syllables/second, through the rapid reproduction of a syllabic sequence;
- Presence/absence of noise during speech.
2.4. Statistical Analysis
3. Results
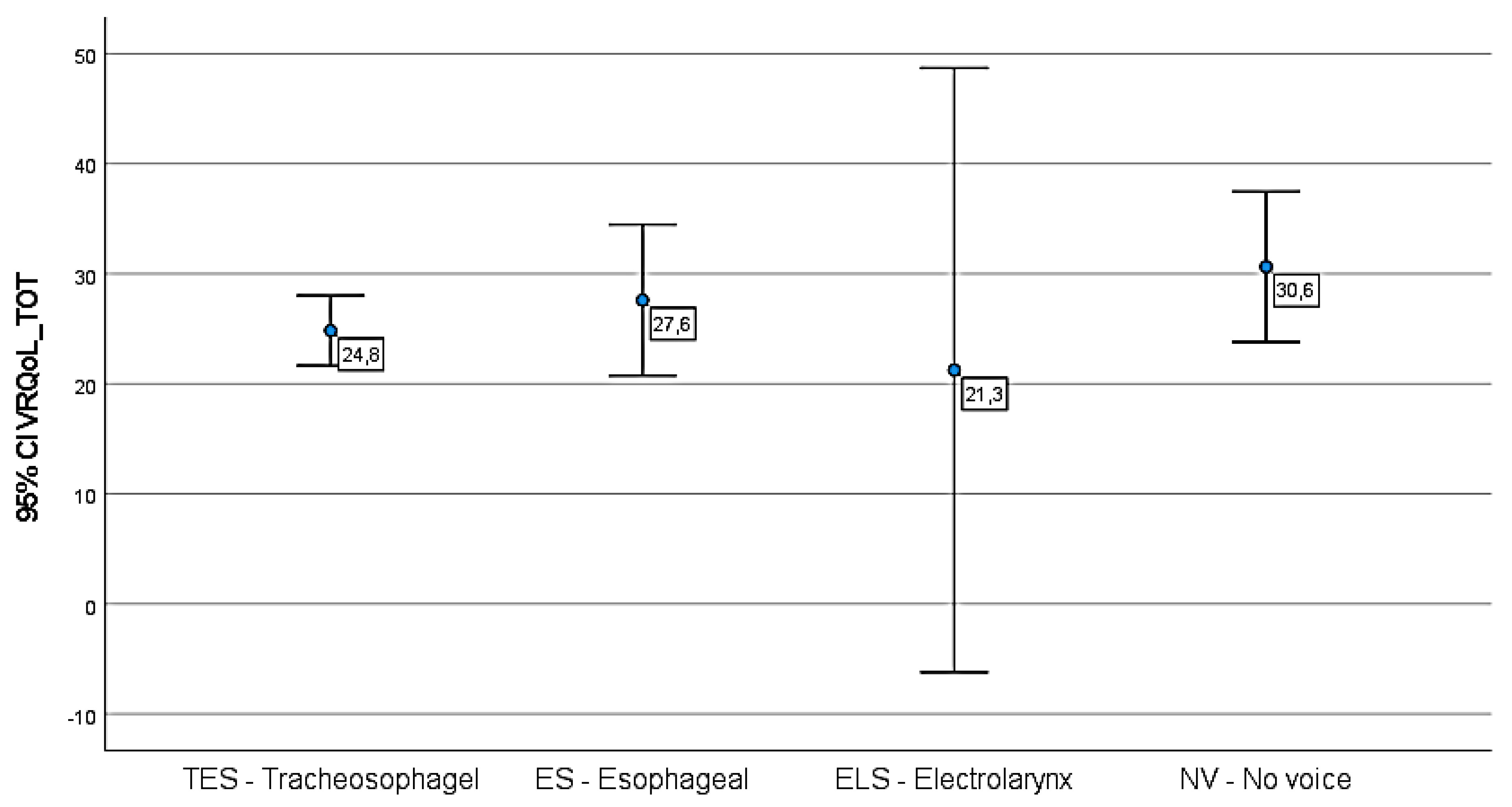
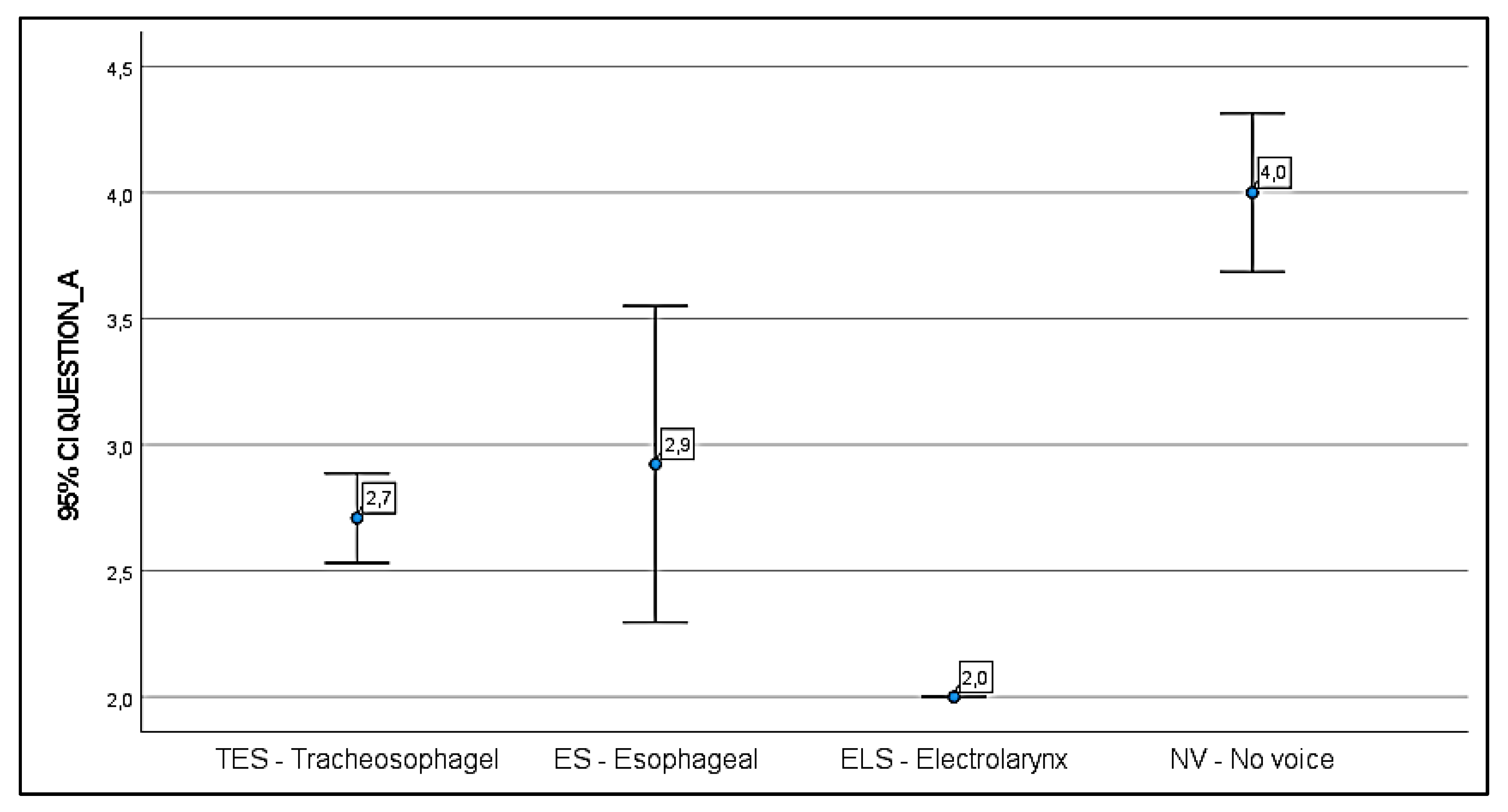
3.1. V-RQoL Questionnaire
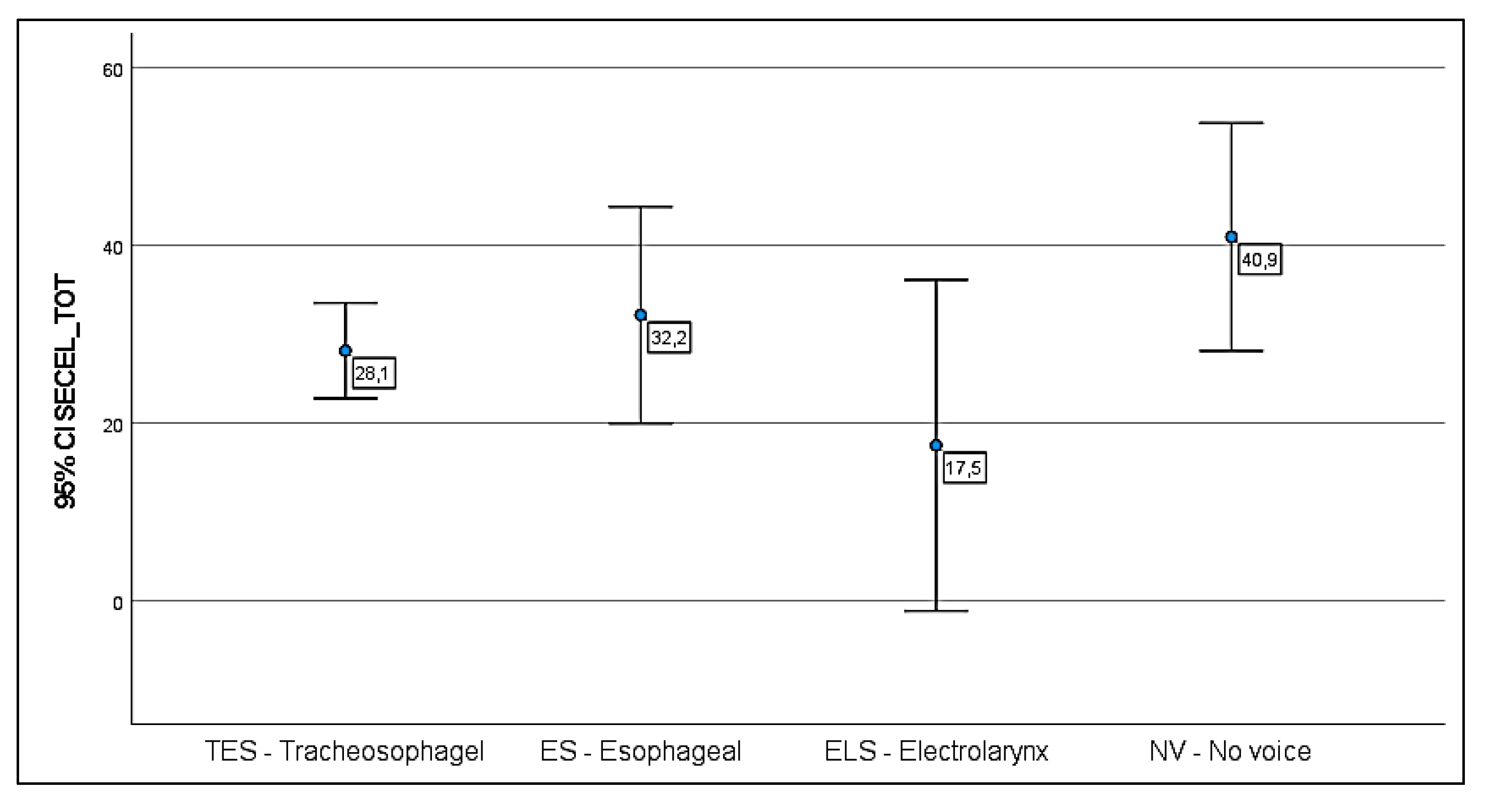
3.2. SECEL Questionnaire
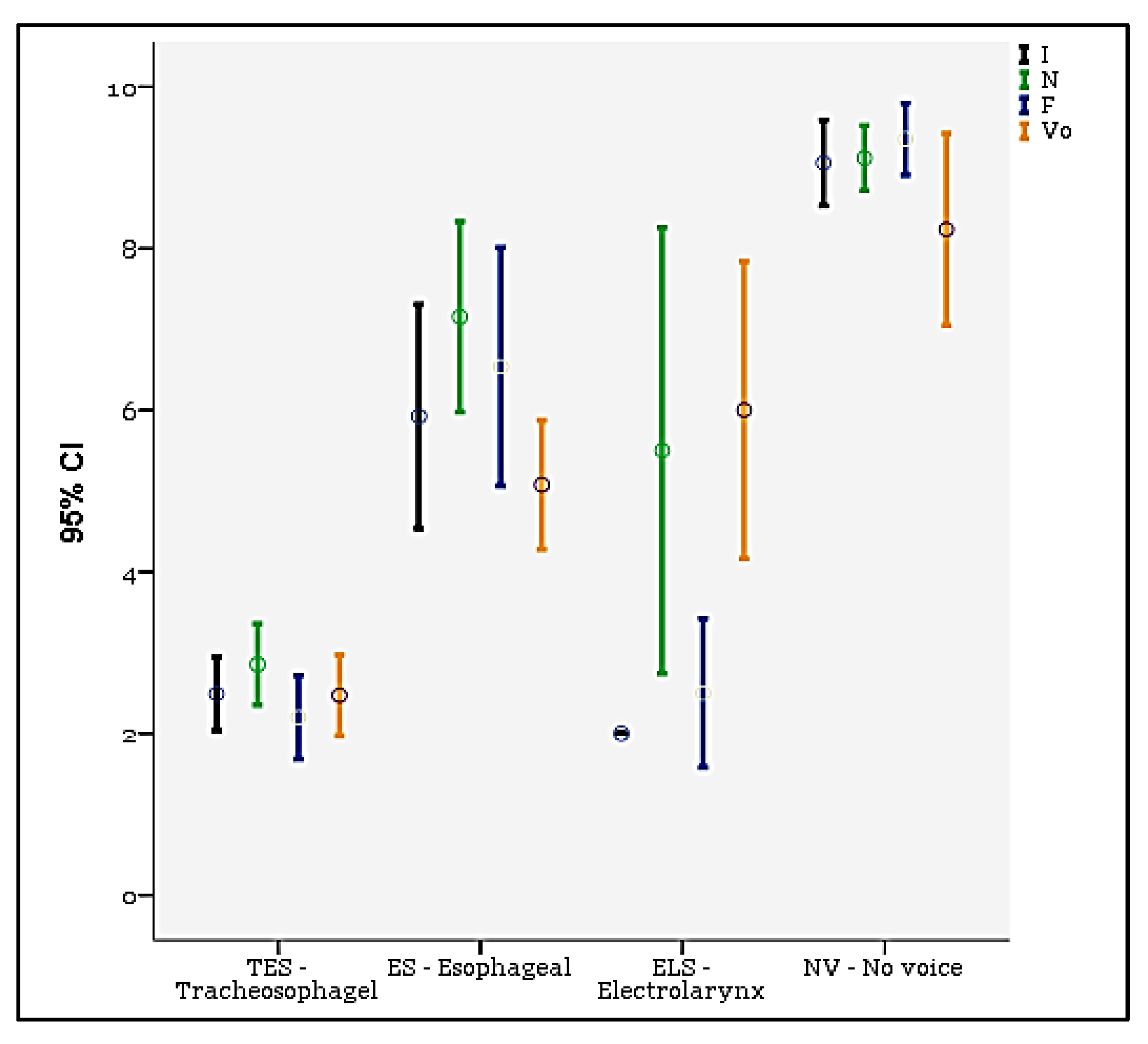
3.3. INFVo Scale
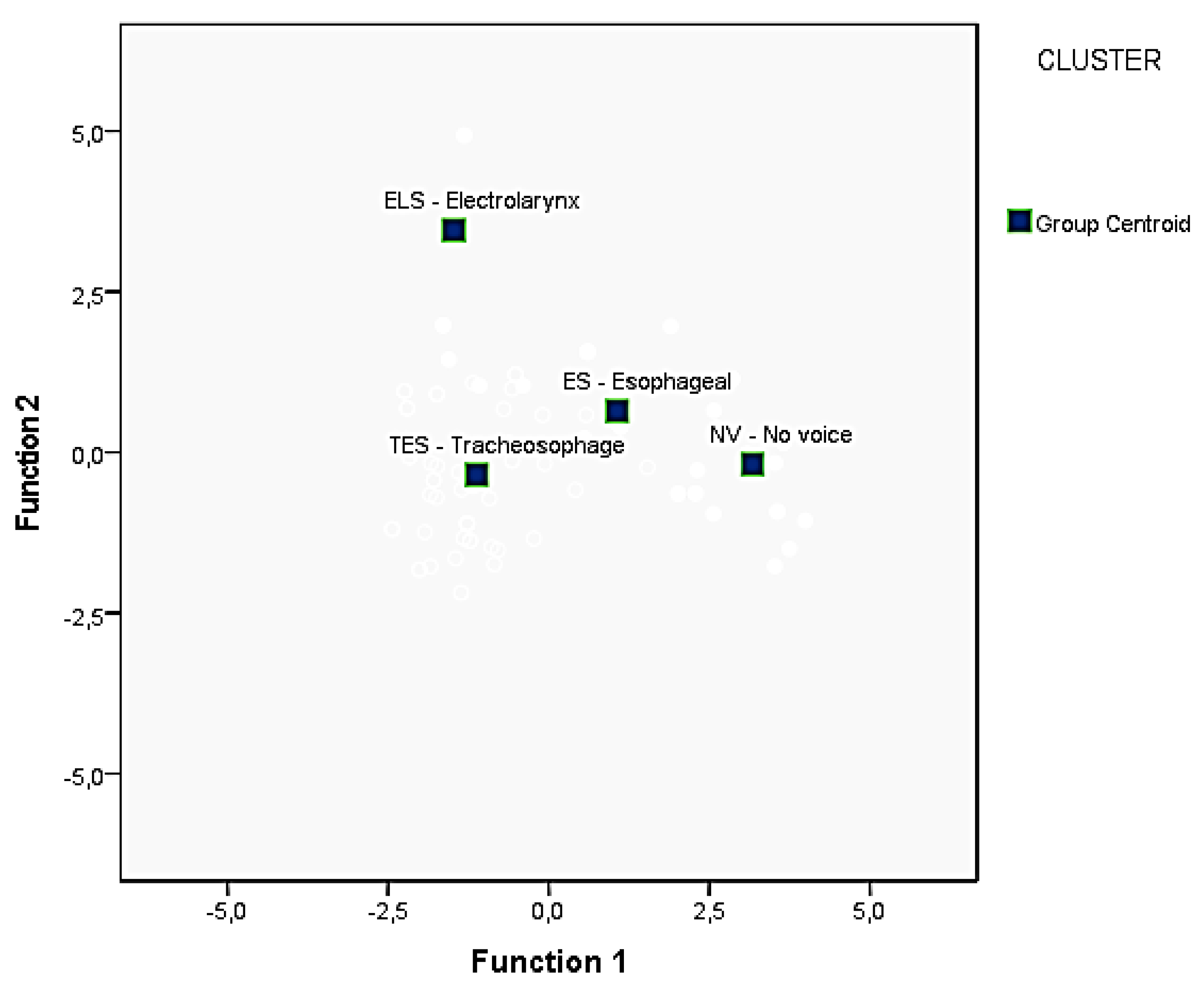
3.4. Discriminant Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. V-RQoL Questionnaire (Voice Related Quality of Life Survey)

Appendix B. SECEL (Self Evaluation of Communication Experiences after Laryngectomy)



References
- Perry, A.; Casey, E.; Cotton, S. Quality of life after total laryngectomy: Functioning, psychological well-being and self-efficacy. Int. J. Lang. Commun. Disord. 2015, 50, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Scott, A.J.; McGuire, J.K.; Manning, K.; Leach, L.; Fagan, J.J. Quality of life after total laryngectomy: Evaluating the effect of socioeconomic status. J. Laryngol. Otol. 2019, 133, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Rickford, J.; Coveney, J.; Baker, J.; Hersh, D. Living with the altered self: A qualitative study of life after total laryngectomy. Int. J. Speech Lang. Pathol. 2013, 15, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Costa, J.M.; López, M.; García, J.; León, X.; Quer, M. Impact of total laryngectomy on return to work. Acta Otorrinolaringol. Esp. 2018, 69, 74–79. [Google Scholar] [CrossRef]
- Tang, C.G.; Sinclair, C.F. Voice Restoration After Total Laryngectomy. Otolaryngol. Clin. N. Am. 2015, 48, 687–702. [Google Scholar] [CrossRef]
- Ward, E.C.; van As-Brooks, C.J. Head and Neck Cancer: Treatment, Rehabilitation, and Outcomes; Plural Publishing: San Diego, CA, USA, 2014. [Google Scholar]
- Lorenz, K.Z. Rehabilitation after Total Laryngectomy—A Tribute to the Pioneers of Voice Restoration in the Last Two Centuries. Front. Med. 2017, 4, 81. [Google Scholar] [CrossRef] [Green Version]
- Kaye, R.; Tang, C.G.; Sinclair, C.F. The electrolarynx: Voice restoration after total laryngectomy. Med. Devices 2017, 10, 133–140. [Google Scholar] [CrossRef] [Green Version]
- Kotake, K.; Suzukamo, Y.; Kai, I.; Iwanaga, K.; Takahashi, A. Social support and substitute voice acquisition on psychological adjustment among patients after laryngectomy. Eur. Arch. Otorhinolaryngol. 2017, 274, 1557–1565. [Google Scholar] [CrossRef] [Green Version]
- Moerman, M.B.; Martens, J.P.; Van der Borgt, M.J.; Peleman, M.; Gillis, M.; Dejonckere, P.H. Perceptual evaluation of substitution voices: Development and evaluation of the (I)INFVo rating scale. Eur. Arch. Otorhinolaryngol. 2005, 263, 183–187. [Google Scholar] [CrossRef]
- Moerman, M.; Martens, J.P.; Crevier-Buchman, L.; de Haan, E.; Grand, S.; Tessier, C.; Woisard, V.; Dejonckere, P. The INFVo perceptual rating scale for substitution voicing: Development and reliability. Eur. Arch. Otorhinolaryngol. 2006, 263, 435–439. [Google Scholar] [CrossRef]
- Schindler, A.; Mozzanica, F.; Brignoli, F.; Maruzzi, P.; Evitts, P.; Ottaviani, F. Reliability and validity of the Italian self-evaluation of communication experiences after laryngeal cancer questionnaire. Head Neck 2013, 35, 1606–1615. [Google Scholar] [CrossRef]
- Schindler, A.; Ginocchio, D.; Atac, M.; Maruzzi, P.; Madaschi, S.; Ottaviani, F.; Mozzanica, F. Reliability of the Italian INFVo scale and correlations with objective measures and VHI scores. Acta Otorhinolaryngol. Ital. 2013, 33, 121–127. [Google Scholar]
- Longobardi, Y.; Savoia, V.; Bussu, F.; Morra, L.; Mari, G.; Nesci, D.A.; Parrilla, C.; D’Alatri, L. Integrated rehabilitation after total laryngectomy: A pilot trial study. Support. Care Cancer 2019, 27, 3537–3544. [Google Scholar] [CrossRef]
- D’Alatri, L.; Longobardi, Y.; Parrilla, C.; Crudo, F.; Oliveto, G.; Mari, G.; Marchese, M.R.; Passali, G.C.; Cefaro, C.A.; Paludetti, G.; et al. Long-term voice outcomes and quality of life after open partial horizontal laryngectomy type II vs. total laryngectomy: A cross-sectional study. Clin. Otolaryngol. 2022, 47, 464–470. [Google Scholar] [CrossRef]
- Fantini, M.; Crosetti, E.; Pizzorni, N.; Sprio, A.E.; Bertolin, A.; Rizzotto, G.; Schindler, A.; Succo, G. Voice and communication after open partial horizontal laryngectomies: A cross-sectional outcome study. Head Neck 2022, 44, 2248–2256. [Google Scholar] [CrossRef]
- Hirano, M. Psycho-acoustic evaluation of voice: GRBAS scale. In Clinical Examination of Voice; Hirano, M., Ed.; Springer: Berlin/Heidelberg, Germany, 1981. [Google Scholar]
- Schindler, A.; Cuccarini, V.; Bottero, A.; Dobrea, C.; Capaccio, P.; Ottaviani, F. Long-term vocal functional result after glottectomy: A multidimensional analysis. Eur. Arch. Otorhinolaryngol. 2007, 264, 1039–1044. [Google Scholar] [CrossRef]
- Kazi, R.; Kiverniti, E.; Prasad, V.; Venkitaraman, R.; Nutting, C.; Clarke, P.; Rhys-Evans, P.; Harrington, K. Multidimensional assessment of female tracheoesophageal prosthetic speech. Clin. Otolaryngol. 2006, 31, 511–517. [Google Scholar] [CrossRef]
- Makeieff, M.; de la Breteque, A.; Guerrier, B.; Giovanni, A. Voice handicap evaluation after supracricoid partial laryngectomy. Laryngoscope 2009, 119, 746–750. [Google Scholar] [CrossRef]
- Bron, L.; Pasche, P.; Brossard, E.; Monnier, P.; Schweizer, V. Functional analysis after supracricoid partial laryngectomy with cricohyoidoepiglottopexy. Laryngoscope 2002, 112, 1289–1293. [Google Scholar] [CrossRef]
- Laudadio, P.; Presutti, L.; Dall’Olio, D.; Cunsolo, E.; Consalici, R.; Amorosa, L.; Cancellieri, A.; Bocciolini, C. Supracricoid laryngectomies: Long-term oncological and functional results. Acta Otolaryngol. 2006, 126, 640–649. [Google Scholar] [CrossRef]
- Hogikyan, N.D.; Sethuraman, G. Validation of an instrument to measure voice-related quality of life (V-RQOL). J. Voice 1999, 13, 557–569. [Google Scholar] [CrossRef] [PubMed]
- Blood, G.W. Development and assessment of a scale addressing communication needs of patients with laryngectomies. Am. J. Speech-Lang. Pathol. 1993, 2, 82–90. [Google Scholar] [CrossRef]
- Morawska, J.; Niebudek-Bogusz, E.; Zaborowski, K.; Wiktorowicz, J.; Śliwińska-Kowalska, M. V-RQOL as a tool for assessing the impact of voice disorders on the quality of life in occupational voice users. Otorynolaryngologia 2015, 14, 96–103. [Google Scholar]
- Rangarajan, A.; Selvaraj, J.L.; Santhanam, D.P. The Voice-Related Quality Of Life: A Study on the Reliability and Validity of the Tamil Version. Clin. Med. Insights Ear Nose Throat 2019, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moukarbel, R.V.; Doyle, P.C.; Yoo, J.H.; Franklin, J.H.; Day, A.M.; Fung, K. Voice-related quality of life (V-RQOL) outcomes in laryngectomees. Head Neck 2011, 33, 31–36. [Google Scholar] [CrossRef]
- Grässel, E.; Hoppe, U.; Rosanowski, F. Graduierung des Voice-Related-Quality-of-Life-Index [Grading of the voice-related quality of life index]. HNO 2009, 57, 896–901. [Google Scholar] [CrossRef]
- Finizia, C.; Bergman, B.; Lindström, J. A cross-sectional validation study of Self-Evaluation of Communication Experiences after Laryngeal Cancer—A questionnaire for use in the voice rehabilitation of laryngeal cancer patients. Acta Oncol. 1999, 38, 573–580. [Google Scholar]
- Eadie, T.L.; Bowker, B.C. Coping and Quality of Life After Total Laryngectomy. Otolaryngol. Head Neck Surg. 2012, 146, 959–965. [Google Scholar] [CrossRef] [Green Version]
- Johansson, M.; Rydén, A.; Finizia, C. Self-evaluation of communication experiences after laryngeal cancer—A longitudinal questionnaire study in patients with laryngeal cancer. BMC Cancer 2008, 8, 80. [Google Scholar] [CrossRef] [Green Version]
- Boersma, P.; Weenink, D. PRAAT: Doing Phonetics by Computer, Version 5.2.34. 2007. Available online: http://www.fon.hum.uva.nl/praat/ (accessed on 20 October 2022).
- Moerman, M.; Pieters, G.; Martens, J.; Van der Borgt, M.-J.; Dejonckere, P. Objective evaluation of the quality of substitution voices. Eur. Arch. Otorhinolaryngol. 2004, 261, 541–547. [Google Scholar] [CrossRef]
- Van Immerseel, L.M.; Martens, J.P. Pitch and voiced/unvoiced determination with an auditory model. J. Acoust. Soc. Am. 1992, 91, 3511–3526. [Google Scholar] [CrossRef]
- Bray, J.H.; Maxwell, S.E. Analyzing and Interpreting Significant MANOVAs. Rev. Educ. Res. 1982, 52, 340–367. [Google Scholar] [CrossRef]
- Motta, G.; Salerno, G. Tracheoesophageal prostheses. Acta Otorhinolaryngol. Ital. 1992, 12, 245–255. [Google Scholar]
- Pereira da Silva, A.; Feliciano, T.; Vaz Freitas, S.; Esteves, S.; Almeida ESousa, C. Quality of life in patients submitted to total laryngectomy. J. Voice 2015, 29, 382–388. [Google Scholar] [CrossRef]
- van Sluis, K.E.; Kornman, A.F.; van der Molen, L.; van den Brekel, M.W.M.; Yaron, G. Women’s perspective on life after total laryngectomy: A qualitative study. Int. J. Lang. Commun. Disord. 2020, 55, 188–199. [Google Scholar] [CrossRef] [Green Version]
- Souza, F.G.R.; Santos, I.C.; Bergmann, A.; Thuler, L.C.S.; Freitas, A.S.; Freitas, E.Q.; Dias, F.L. Quality of life after total laryngectomy: Impact of different vocal rehabilitation methods in a middle income country. Health Qual. Life Outcomes 2020, 18, 92. [Google Scholar] [CrossRef]
- Polat, B.; Orhan, K.S.; Kesimli, M.C.; Gorgulu, Y.; Ulusan, M.; Deger, K. The effects of indwelling voice prosthesis on the quality of life, depressive symptoms, and self-esteem in patients with total laryngectomy. Eur. Arch. Otorhinolaryngol. 2015, 272, 3431–3437. [Google Scholar] [CrossRef]
- Ţiple, C.; Drugan, T.; Dinescu, F.V.; Mureşan, R.; Chirilă, M.; Cosgarea, M. The impact of vocal rehabilitation on quality of life and voice handicap in patients with total laryngectomy. J. Res. Med. Sci. 2016, 21, 127. [Google Scholar]
- Allegra, E.; La Mantia, I.; Bianco, M.R.; Drago, G.D.; Le Fosse, M.C.; Azzolina, A.; Grillo, C.; Saita, V. Verbal performance of total laryngectomized patients rehabilitated with esophageal speech and tracheoesophageal speech: Impacts on patient quality of life. Psychol. Res. Behav. Manag. 2019, 12, 675–681. [Google Scholar] [CrossRef] [Green Version]
- Galli, A.; Giordano, L.; Biafora, M.; Tulli, M.; di Santo, D.; Bussi, M. Voice prosthesis rehabilitation after total laryngectomy: Are satisfaction and quality of life maintained over time? Acta Otorhinolaryngol. Ital. 2019, 39, 162–168. [Google Scholar] [CrossRef] [Green Version]
- Hansen, K.; Chenoweth, M.; Thompson, H.; Strouss, A. Role of the Speech-Language Pathologist (SLP) in the Head and Neck Cancer Team. Cancer Treat Res. 2018, 174, 31–42. [Google Scholar] [PubMed]
- Sivero, L.; Siciliano, S.; Chini, A.; Volpe, S.; Gennarelli, N.; Salerno, G.; Sivero, S. Oncological and psychological evaluation of laryngectomized patients, pre and post implantation of voice prostheses. A single center experience. Ann. Ital. Chir. 2022, 93, 633–636. [Google Scholar] [PubMed]
- Ricciardiello, F.; Caraglia, M.; Iorio, B.; Abate, T.; Boccellino, M.; Colella, G.; Oliva, F.; Ferrise, P.; Zappavigna, S.; Faenza, M.; et al. Aggressiveness pattern and second primary tumor risk associated with basaloid squamous cell carcinoma of the larynx. Oncotarget 2017, 8, 95791–95798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mesolella, M.; Iorio, B.; Misso, G.; Luce, A.; Cimmino, M.; Iengo, M.; Landi, M.; Sperlongano, P.; Caraglia, M.; Ricciardiello, F. Role of perineural invasion as a prognostic factor in laryngeal cancer. Oncol. Lett. 2016, 11, 2595–2598. [Google Scholar] [CrossRef] [Green Version]
- van Sluis, K.E.; van der Molen, L.; van Son, R.J.J.H.; Hilgers, F.J.M.; Bhairosing, P.A.; van den Brekel, M.W.M. Objective and subjective voice outcomes after total laryngectomy: A systematic review. Eur. Arch. Otorhinolaryngol. 2018, 275, 11–26. [Google Scholar] [CrossRef] [Green Version]
- Mesolella, M.; Iorio, B.; Buono, S.; Cimmino, M.; Motta, G. Supracricoid Partial Laryngectomy: Oncological and Functional Outcomes. Int. Arch. Otorhinolaryngol. 2021, 26, e075–e084. [Google Scholar] [CrossRef]
- Mesolella, M.; Evangelista, A.; Allosso, S.; Matano, E.; Motta, G.; Motta, G. New Therapeutic Strategies in the Treatment of Stomal Recurrence after Total Laryngectomy: Role of Immunotherapy. Ear Nose Throat J. 2022, 21, 145–155. [Google Scholar] [CrossRef]
- Eadie, T.L.; Dai, A.M.B.; Sawin, D.E.; Lamvik, K.; Doyle, P.C. Auditory-perceptual speech outcomes and quality of life after total laryngectomy. Otolaryngol. Head Neck Surg. 2013, 148, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Cox, S.R.; Doyle, P.C. The Influence of Electrolarynx Use on Postlaryngectomy Voice-Related Quality of Life. Otolaryngol. Head Neck Surg. 2014, 150, 1005–1009. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | TES | ES | ELS | NV | |
|---|---|---|---|---|---|
| Sample size | 55 (62%) | 13 (15%) | 4 (4%) | 17 (19%) | |
| Age mean (range) | 64 (45–78) | 65 (44–81) | 63 (57–69) | 62 (49–76) | n.s. |
| Male | 45 (82%) | 12 (92%) | 4 (100%) | 16 (94%) | 0.750 |
| Female | 10 (18%) | 1 (8%) | 0 (0%) | 1 (6%) | |
| Non-smoker | 10 (18%) | 0 (0%) | 0 (0%) | 1 (6%) | 0.460 |
| Former smoker | 40 (73%) | 13 (100%) | 4 (100%) | 16 (94%) | |
| Smoker | 5 (9%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Time since LT (mean, ys) | 2.80 | 2.38 | 3.00 | 2.12 | |
| Radiotherapy | 32 (58%) | 6 (46%) | 2 (50%) | 10 (59%) | 0.062 |
| Chemotherapy | 14 (25.5%) | 4 (30.8%) | 0 (0%) | 4 (23.5%) | 0.760 |
| Speech therapy | 42 (76.4%) | 10 (77%) | 2 (50%) | 4 (23.5%) | 0.002 |
| STEP | TOLERANCE | F TO REMOVE | WILKS’ LAMBDA | |
|---|---|---|---|---|
| 1 | I | 1.000 | 76,494 | |
| 2 | I | 0.307 | 20,822 | 0.296 |
| N | 0.307 | 16,654 | 0.270 | |
| 3 | I | 0.286 | 22,510 | 0.248 |
| N | 0.259 | 10,620 | 0.189 | |
| V0 | 0.404 | 6587 | 0.169 | |
| Function | Eigenvalue | % of Variance | Cumulative % | Canonical Correlation |
|---|---|---|---|---|
| 1 | 3.104 a | 77.1 | 77.1 | 0.870 |
| 2 | 0.711 a | 17.7 | 94.8 | 0.645 |
| 3 | 0.211 a | 5.2 | 100.0 | 0.417 |
| Group | Predicted Group Membership | ||||||
|---|---|---|---|---|---|---|---|
| TES-Tracheoesophagel | ES–Esophagel | ELS–Electrolarynx | NV–No Voice | Total | |||
| Original | Count | TES-Tracheoesophagel | 49 | 5 | 0 | 1 | 55 |
| ES–Esophagel | 2 | 9 | 0 | 2 | 13 | ||
| ELS–Electrolarynx | 0 | 0 | 4 | 0 | 4 | ||
| NV–No Voice | 0 | 4 | 0 | 13 | 17 | ||
| % | TES-Tracheoesophagel | 89.1 | 9.1 | 0.0 | 1.8 | 100.0 | |
| ES–Esophagel | 15.4 | 69.2 | 0.0 | 15.4 | 100.0 | ||
| ELS–Electrolarynx | 0.0 | 0.0 | 100.0 | 0.0 | 100.0 | ||
| NV–No Voice | 0.0 | 23.5 | 0.0 | 76.5 | 100.0 | ||
| Dependent Variable | Group Comparison | Mean Difference | Sig. |
|---|---|---|---|
| Question A | TES vs. NV | −1.291 | <0.0001 |
| ES vs. NV | −1.077 | <0.0001 | |
| ELS vs. NV | −2.000 | <0.0001 | |
| I | TES vs. ES | −3.432 | <0.0001 |
| TES vs. NV | −6.568 | <0.0001 | |
| ES vs. ELS | 3.923 | <0.0001 | |
| ES vs. NV | −3.136 | <0.0001 | |
| ELS vs. NV | −7.079 | <0.0001 | |
| N | TES vs. ES | −4.299 | <0.0001 |
| TES vs. ELS | −2.645 | 0.023 | |
| TES vs. NV | −6.263 | <0.0001 | |
| ES vs. NV | −1.964 | 0.016 | |
| ELS vs. NV | −3.618 | 0.002 | |
| Vo | TES vs. ES | −2.604 | <0.0001 |
| TES vs. ELS | −3.527 | 0.003 | |
| TES vs. NV | −5.763 | <00001 | |
| ES vs. NV | −3.158 | <00001 |
| QUESTION A | I | N | F | Vo | SECEL_TOT | VRQoL_TOT | ||
|---|---|---|---|---|---|---|---|---|
| QUESTION A | Pearson Correlation | 1 | 0.520 ** | 0.446 ** | 0.505 ** | 0.403 ** | 0.462 ** | 0.334 ** |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | ||
| N | 89 | 89 | 89 | 89 | 89 | 89 | 89 | |
| I | Pearson Correlation | 0.520 ** | 1 | 0.925 ** | 0.968 ** | 0.857 ** | 0.281 ** | 0.234 * |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | <0.001 | 0.008 | 0.27 | ||
| N | 89 | 89 | 89 | 89 | 89 | 89 | 89 | |
| N | Pearson Correlation | 0.446 ** | 0.925 ** | 1 | 0.953 ** | 0.894 ** | 0.288 ** | 0.201 * |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | <0.001 | 0.006 | 0.59 | ||
| N | 89 | 89 | 89 | 89 | 89 | 89 | 89 | |
| F | Pearson Correlation | 0.505 ** | 0.968 ** | 0.953 ** | 1 | 0.878 ** | 0.307 ** | 0.246 * |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | <0.001 | 0.003 | 0.020 | ||
| N | 89 | 89 | 89 | 89 | 89 | 89 | 89 | |
| Vo | Pearson Correlation | 0.403 ** | 0.857 ** | 0.894 ** | 0.878 ** | 1 | 0.290 ** | 0.207 |
| Sig. (2-tailed) | <0.001 | <0.001 | <0.001 | <0.001 | 0.006 | 0.052 | ||
| N | 89 | 89 | 89 | 89 | 89 | 89 | 89 | |
| SECEL_TOT | Pearson Correlation | 0.462 ** | 0.281 ** | 0.288 ** | 0.307 ** | 0.290 ** | 1 | 0.577 ** |
| Sig. (2-tailed) | <0.001 | 0.008 | 0.006 | 0.003 | 0.006 | <0.001 | ||
| N | 89 | 89 | 89 | 89 | 89 | 89 | 89 | |
| VRQoL_TOT | Pearson Correlation | 0.334 ** | 0.234 ** | 0.201 | 0.246 * | 0.207 | 0.577 ** | 1 |
| Sig. (2-tailed) | 0.001 | 0.027 | 0.059 | 0.020 | 0.052 | <0.001 | ||
| N | 89 | 89 | 89 | 89 | 89 | 89 | 89 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mesolella, M.; Allosso, S.; D’aniello, R.; Pappalardo, E.; Catalano, V.; Quaremba, G.; Motta, G.; Salerno, G. Subjective Perception and Psychoacoustic Aspects of the Laryngectomee Voice: The Impact on Quality of Life. J. Pers. Med. 2023, 13, 570. https://doi.org/10.3390/jpm13030570
Mesolella M, Allosso S, D’aniello R, Pappalardo E, Catalano V, Quaremba G, Motta G, Salerno G. Subjective Perception and Psychoacoustic Aspects of the Laryngectomee Voice: The Impact on Quality of Life. Journal of Personalized Medicine. 2023; 13(3):570. https://doi.org/10.3390/jpm13030570
Chicago/Turabian StyleMesolella, Massimo, Salvatore Allosso, Roberto D’aniello, Emanuela Pappalardo, Vincenzo Catalano, Giuseppe Quaremba, Gaetano Motta, and Grazia Salerno. 2023. "Subjective Perception and Psychoacoustic Aspects of the Laryngectomee Voice: The Impact on Quality of Life" Journal of Personalized Medicine 13, no. 3: 570. https://doi.org/10.3390/jpm13030570