

Preliminary Stages for COVID-19 Detection Using Image Processing
Abstract
:1. Introduction
- We analyze how various preprocessing techniques can be used to enhance feature extraction in each of the investigated works.
- We present a detailed discussion of the different segmentation approaches employed in each reviewed paper, with the goal of delivering significant features that are reliable for COVID-19 detection.
- We provide a comprehensive analysis of the various augmentation methods employed to address the issue of a lack of images available for COVID-19 detection.
- We present a complete investigation of the various feature extraction techniques used to distinguish COVID-19 images from normal images.
2. Concept and Background
3. Source of Information
3.1. X-ray
3.2. Computed Tomography (CT)
3.3. Ultrasound
- Image acquisition is user dependent.
- The field of view is limited.
- Ultrasound images are typically acquired off-plane compared to the true axial, sagittal, or coronal planes, resulting in difficulty in correlating them with other cross-sectional imaging methods.
- Lesional identification can be difficult due to its echogenicity relative to the organ that is scrutinized.
- The quality of imaging can be affected by the physical characteristics of the patient [24].
4. Related Surveys
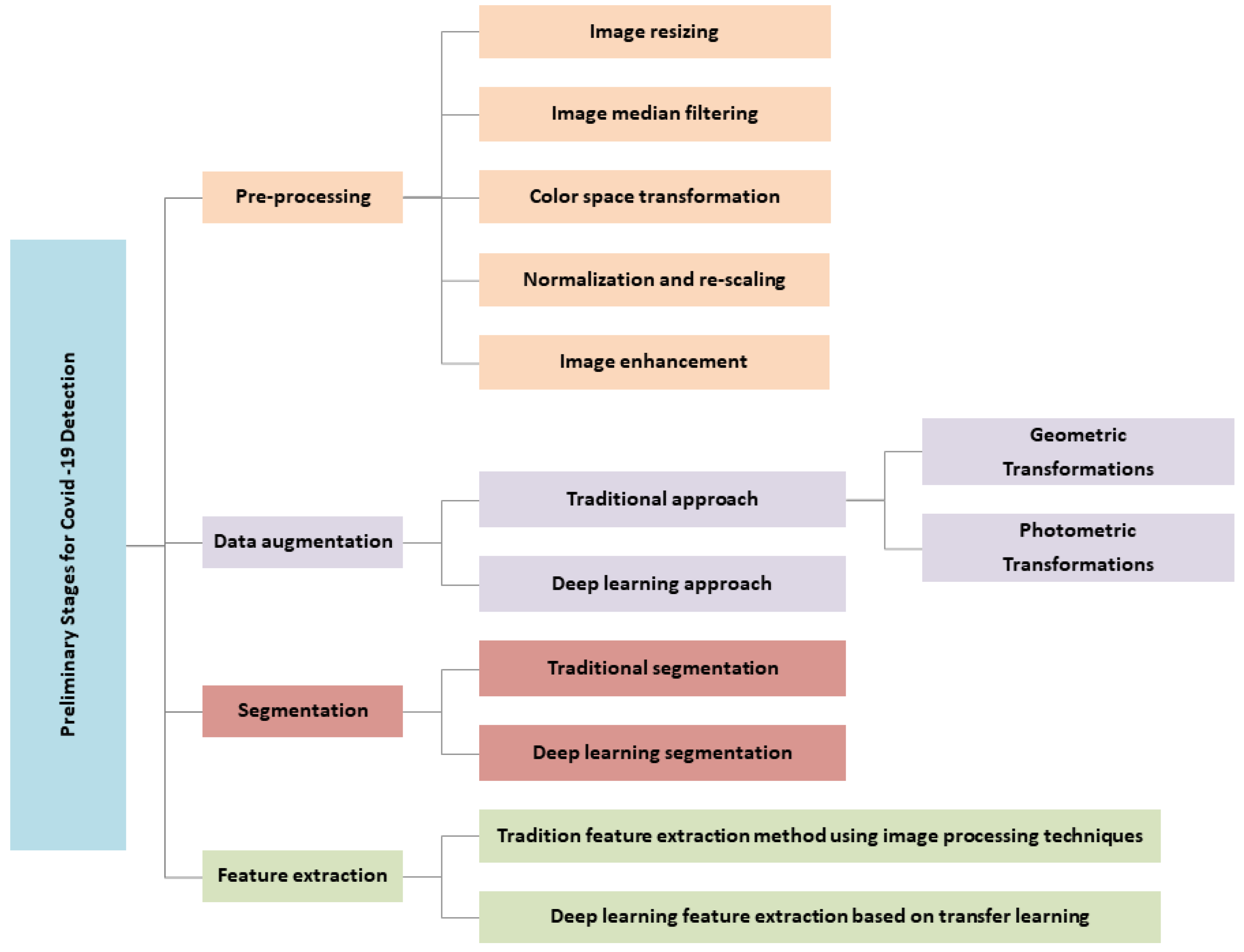
5. Taxonomy of the Preliminary Stages for COVID-19 Detection
6. Preprocessing
- Reducing or eliminating the impact of data variability on model performance, as images are obtained from a variety of datasets with varied image sizes and acquisition conditions [35].
- Improving the contrast of an image [12].
- Producing accurate and consistent findings when classifying COVID-19 from chest images.
- Making the illness zone in the image more evident in comparison to the original image [12].
6.1. Image Resizing
6.2. Image Filtering
6.3. Color Space Transformation
6.4. Normalization and Rescaling
6.5. Image Enhancement
7. Data Augmentation
7.1. Traditional Data Augmentation Approach
7.1.1. Geometric Transformations
7.1.2. Photometric Transformations
7.2. Deep Learning Data Augmentation Approach
8. Segmentation
8.1. Traditional Segmentation
8.2. Deep Learning Segmentation
- The FCN architecture has been employed for lung segmentation in COVID-19 patients. In this architecture, FC layers are replaced with convolutional layers to record the output as a local map. These maps are up-sampled using the previously mentioned method, which employs backward convolution learning with certain stride size. A 1 × 1 convolution layer at the network’s end produces the corresponding pixel label as the output. The output detail quantity of this layer is constrained by the current stride size in the deconvolution stage. Several skip connections have been introduced to the network from the lower levels to the end layer to address this issue and improve the quality of the results [83].
- The SegNet decoder is designed in such a way that an up-sampling layer is positioned in the decoder for each down-sampling layer in the encoding section, unlike the deconvolution layers in FCN networks. These layers are incapable of learning; when the extraction values of the maximum pooling layer are located, and the remaining output cells are set to zero [84].
- While the U-Net network has the same amount of pooling and up-sampling layers as SegNet, it uses trainable deconvolution layers instead. In addition, the up-sampling and down-sampling layers in this network have a matching skip connection [85]. For COVID-19 diagnosis applications, U-Net is a widely utilized technique for segmenting both lung regions generally and affected lung regions [82,86,87].
- The Res2Net module separates feature maps into numerous subsets and processes them through a set of 3 × 3 filters after 1 × 1 convolution. The outputs are combined, then 1 × 1 convolution is applied. The set of this process is residually structured, and it is consequently called the Res2Net module. The scale dimension (the number of feature groups in the Res2Net block) is a parameter included in this module; as the scale increases, the model learns features with larger receptive field sizes. Res2Net can be used in conjunction with current modules such as cardinality dimension, squeeze, and excitation. In addition, it can be easily combined with several other models, such as ResNeXt, ResNet, DLA, and Big Little Net [88].
- UNet++ is made up of an encoder and a decoder that are linked together by a sequence of layered dense convolutional blocks. Prior to fusion, the semantic gap between the encoder and decoder feature maps are bridged. The encoder extracts feature by down-sampling, while the decoder maps feature to the original image by up-sampling and performs pixel classification to achieve the goal of segmentation. Zhou et al. [89] developed UNet++, which is significantly more sophisticated than U-Net, as it inserts a nested convolutional structure between the encoding and decoding paths. Clearly, such a network can increase segmentation performance. Consequently, the training process is more difficult.
- VB-Net is a modified three-dimensional convolutional neural network that integrates V-Net 14 and the bottleneck structure of V-Net 15. VB-Net is divided into two pathways. The first is a contracting path that uses down-sampling and convolution to extract global image features. The second is a broad approach that includes up-sampling and operations to combine fine-grained image data. A bottleneck structure is implemented into VB-Net 15, which makes it much faster than V-Net 14 in terms of speed. A three-layer stack is used in the bottleneck design. The first layer, with a 1 × 1 × 1 kernel, reduces the number of channels and feeds the data for a conventional 3 × 3 × 3 kernel layer processing, then the channels of the feature maps are restored by another 1 × 1 × 1 kernel layer. The three layers utilize 1 × 1 × 1, 3 × 3 × 3, and 1 × 1 × 1 convolution kernels. The model size and inference time are significantly decreased by combining and minimizing the feature map channels and cross-channel features, which are efficiently fused by convolution. As a result, VB-Net is more suitable for handling huge amounts of 3D volumetric data than the classic V-Net.
9. Feature Extraction
9.1. Traditional Feature Extraction Method
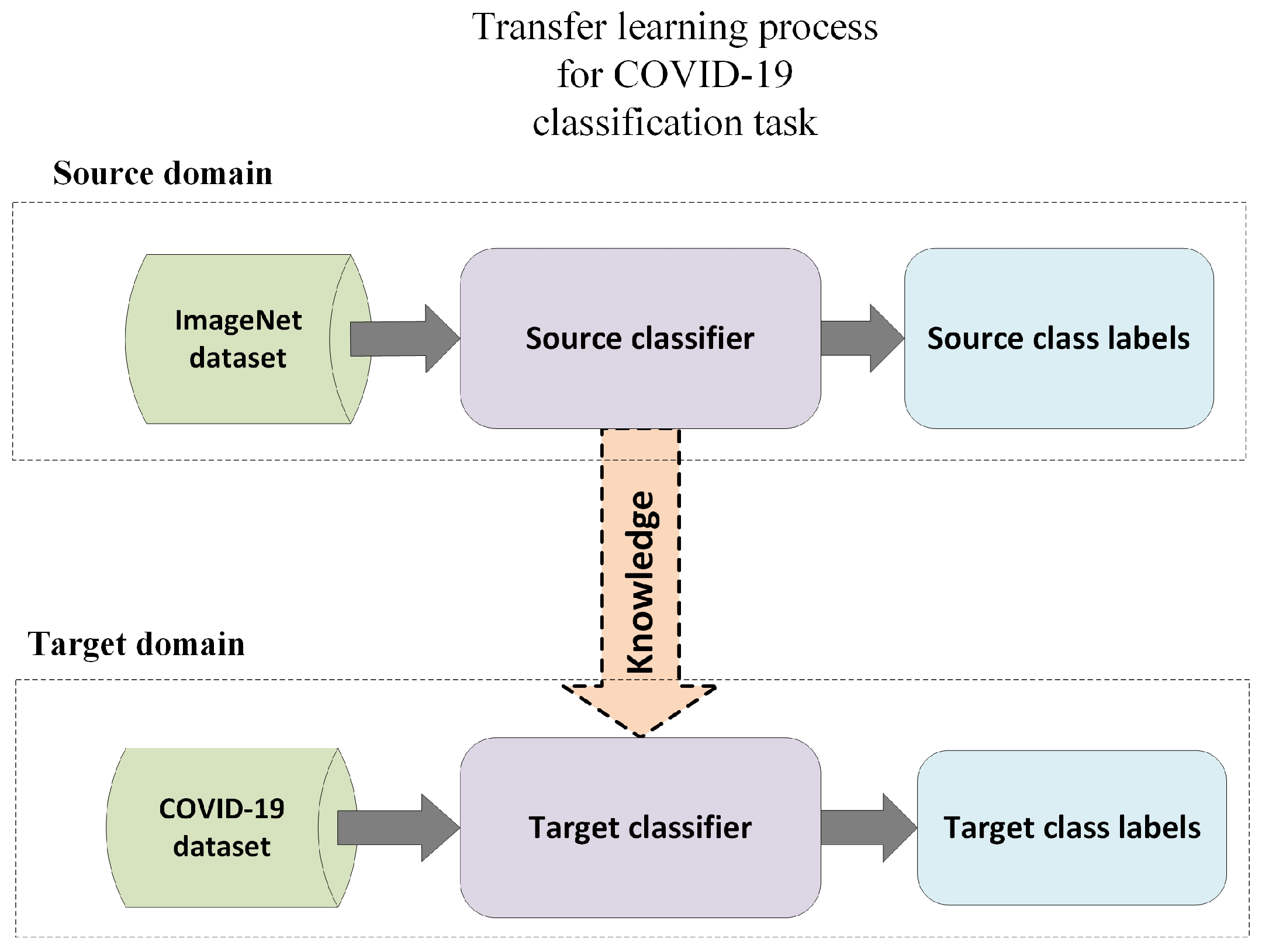
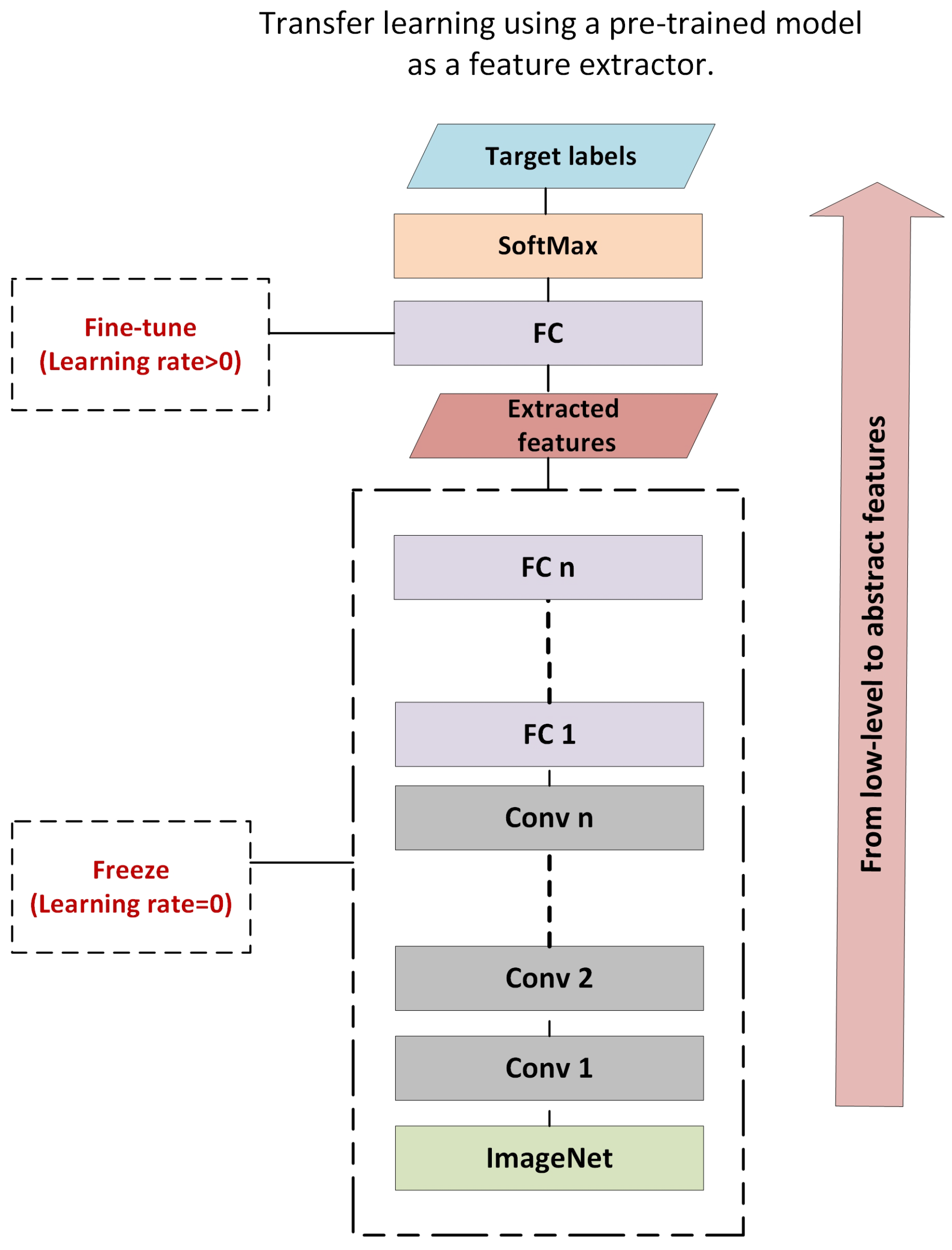
9.2. Deep Learning Feature Extraction Based on Transfer Learning
10. Discussion and Future Research Directions
- Determining how to automatically choose the best parameters for the preprocessing methods discussed in the literature (resizing, rescaling, normalization).
- Evaluating the effectiveness of COVID-19 detection systems using various preprocessing techniques.
11. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | Linear dichroism |
References
- Rehman, A.; Saba, T.; Tariq, U.; Ayesha, N. Deep learning-based COVID-19 detection using CT and X-ray images: Current analytics and comparisons. IT Prof. 2021, 23, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Kaur, S.P.; Gupta, V. COVID-19 Vaccine: A comprehensive status report. Virus Res. 2020, 288, 198114. [Google Scholar] [CrossRef] [PubMed]
- Alsharif, M.; Alsharif, Y.; Yahya, K.; Alomari, O.; Albreem, M.; Jahid, A. Deep learning applications to combat the dissemination of COVID-19 disease: A review. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 11455–11460. [Google Scholar]
- Ibrahim, A.U.; Ozsoz, M.; Serte, S.; Al-Turjman, F.; Yakoi, P.S. Pneumonia classification using deep learning from chest X-ray images during COVID-19. Cogn. Comput. 2021, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Alzubaidi, M.; Zubaydi, H.D.; Bin-Salem, A.A.; Abd-Alrazaq, A.A.; Ahmed, A.; Househ, M. Role of deep learning in early detection of COVID-19: Scoping review. Comput. Methods Programs Biomed. Update 2021, 1, 100025. [Google Scholar] [CrossRef]
- Shoeibi, A.; Khodatars, M.; Alizadehsani, R.; Ghassemi, N.; Jafari, M.; Moridian, P.; Khadem, A.; Sadeghi, D.; Hussain, S.; Zare, A.; et al. Automated detection and forecasting of covid-19 using deep learning techniques: A review. arXiv 2020, arXiv:2007.10785. [Google Scholar]
- Mohammad-Rahimi, H.; Nadimi, M.; Ghalyanchi-Langeroudi, A.; Taheri, M.; Ghafouri-Fard, S. Application of machine learning in diagnosis of COVID-19 through X-ray and CT images: A scoping review. Front. Cardiovasc. Med. 2021, 8, 638011. [Google Scholar] [CrossRef]
- Ramteke, R.; Monali, K.Y. Automatic medical image classification and abnormality detection using k-nearest neighbour. Int. J. Adv. Comput. Res. 2012, 2, 190. [Google Scholar]
- Ranganathan, G. A study to find facts behind preprocessing on deep learning algorithms. J. Innov. Image Process. (JIIP) 2021, 3, 66–74. [Google Scholar]
- Salama, W.M.; Aly, M.H. Framework for COVID-19 segmentation and classification based on deep learning of computed tomography lung images. J. Electron. Sci. Technol. 2022, 20, 100161. [Google Scholar] [CrossRef]
- Elhassan, T.A.; Rahim, M.S.M.; Swee, T.T.; Hashim, S.Z.M.; Aljurf, M. Segmentation of White Blood Cells in Acute Myeloid Leukemia Microscopic Images: A Review. In Prognostic Models in Healthcare: AI and Statistical Approaches; Saba, T., Rehman, A., Roy, S., Eds.; Springer: Singapore, 2022; pp. 1–24. [Google Scholar]
- Iqbal, Z.; Khan, M.A.; Sharif, M.; Shah, J.H.; ur Rehman, M.H.; Javed, K. An automated detection and classification of citrus plant diseases using image processing techniques: A review. Comput. Electron. Agric. 2018, 153, 12–32. [Google Scholar] [CrossRef]
- Elhassan, T.A.M.; Rahim, M.S.M.; Swee, T.T.; Hashim, S.Z.M.; Aljurf, M. Feature Extraction of White Blood Cells Using CMYK-Moment Localization and Deep Learning in Acute Myeloid Leukemia Blood Smear Microscopic Images. IEEE Access 2022, 10, 16577–16591. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Maddikunta, P.K.R.; Pham, Q.V.; Gadekallu, T.R.; Krishnan S, S.R.; Chowdhary, C.L.; Alazab, M.; Piran, M.J. Deep learning and medical image processing for coronavirus (COVID-19) pandemic: A survey. Sustain. Cities Soc. 2021, 65, 102589. [Google Scholar] [CrossRef] [PubMed]
- Andersen, K.G.; Rambaut, A.; Lipkin, W.I.; Holmes, E.C.; Garry, R.F. The proximal origin of SARS-CoV-2. Nat. Med. 2020, 26, 450–452. [Google Scholar] [CrossRef] [PubMed]
- Ilyas, M.; Rehman, H.; Naït-Ali, A. Detection of COVID-19 from chest X-ray images using artificial intelligence: An early review. arXiv 2020, arXiv:2004.05436. [Google Scholar]
- Liu, K.; Chen, Y.; Lin, R.; Han, K. Clinical features of COVID-19 in elderly patients: A comparison with young and middle-aged patients. J. Infect. 2020, 80, e14–e18. [Google Scholar] [CrossRef] [Green Version]
- Elhassan, T.; Gaafar, A. Mathematical modeling of the COVID-19 prevalence in Saudi Arabia. medRxiv 2020. [Google Scholar] [CrossRef]
- Alvi, M.M.; Sivasankaran, S.; Singh, M. Pharmacological and non-pharmacological efforts at prevention, mitigation, and treatment for COVID-19. J. Drug Target. 2020, 28, 742–754. [Google Scholar] [CrossRef]
- Horry, M.J.; Chakraborty, S.; Paul, M.; Ulhaq, A.; Pradhan, B.; Saha, M.; Shukla, N. COVID-19 detection through transfer learning using multimodal imaging data. IEEE Access 2020, 8, 149808–149824. [Google Scholar] [CrossRef]
- Goel, N.; Yadav, A.; Singh, B.M. Medical image processing: A review. In Proceedings of the 2016 Second International Innovative Applications of Computational Intelligence on Power, Energy and Controls with their Impact on Humanity (CIPECH), Ghaziabad, India, 18–19 November 2016; pp. 57–62. [Google Scholar]
- Huang, H.; Aberle, D.R.; Lufkin, R.; Grant, E.G.; Hanafee, W.N.; Kangarloo, H. Advances in medical imaging. Ann. Intern. Med. 1990, 112, 203–220. [Google Scholar] [CrossRef]
- Born, J.; Brändle, G.; Cossio, M.; Disdier, M.; Goulet, J.; Roulin, J.; Wiedemann, N. POCOVID-Net: Automatic detection of COVID-19 from a new lung ultrasound imaging dataset (POCUS). arXiv 2020, arXiv:2004.12084. [Google Scholar]
- Wein, W.; Brunke, S.; Khamene, A.; Callstrom, M.R.; Navab, N. Automatic CT-ultrasound registration for diagnostic imaging and image-guided intervention. Med. Image Anal. 2008, 12, 577–585. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.M.; Karray, F.; Alhajj, R.; Zeng, J. A review on deep learning techniques for the diagnosis of novel coronavirus (COVID-19). IEEE Access 2021, 9, 30551–30572. [Google Scholar] [CrossRef] [PubMed]
- Alghamdi, H.S.; Amoudi, G.; Elhag, S.; Saeedi, K.; Nasser, J. Deep learning approaches for detecting COVID-19 from chest X-ray images: A survey. IEEE Access 2021, 9, 20235–20254. [Google Scholar] [CrossRef]
- Sufian, A.; Ghosh, A.; Sadiq, A.S.; Smarandache, F. A survey on deep transfer learning to edge computing for mitigating the COVID-19 pandemic. J. Syst. Archit. 2020, 108, 101830. [Google Scholar] [CrossRef]
- Subramanian, N.; Elharrouss, O.; Al-Maadeed, S.; Chowdhury, M. A review of deep learning-based detection methods for COVID-19. Comput. Biol. Med. 2022, 143, 105233. [Google Scholar] [CrossRef]
- Chen, Y.; Jiang, G.; Li, Y.; Tang, Y.; Xu, Y.; Ding, S.; Xin, Y.; Lu, Y. A survey on artificial intelligence in chest imaging of COVID-19. BIO Integr. 2020, 1, 137–146. [Google Scholar] [CrossRef]
- Khan, A.; Khan, S.H.; Saif, M.; Batool, A.; Sohail, A.; Khan, M.W. A Survey of Deep Learning Techniques for the Analysis of COVID-19 and their usability for Detecting Omicron. arXiv 2022, arXiv:2202.06372. [Google Scholar]
- Aishwarya, T.; Ravi Kumar, V. Machine learning and deep learning approaches to analyze and detect COVID-19: A review. SN Comput. Sci. 2021, 2, 1–9. [Google Scholar] [CrossRef]
- Shyni, H.M.; Chitra, E. A comparative study of X-ray and CT images in COVID-19 detection using image processing and deep learning techniques. Comput. Methods Programs Biomed. Update 2022, 2, 100054. [Google Scholar] [CrossRef] [PubMed]
- Awassa, L.; Jdey, I.; Dhahri, H.; Hcini, G.; Mahmood, A.; Othman, E.; Haneef, M. Study of Different Deep Learning Methods for Coronavirus (COVID-19) Pandemic: Taxonomy, Survey and Insights. Sensors 2022, 22, 1890. [Google Scholar] [CrossRef] [PubMed]
- Alam, N.-A.-; Ahsan, M.; Based, M.; Haider, J.; Kowalski, M. COVID-19 detection from chest X-ray images using feature fusion and deep learning. Sensors 2021, 21, 1480. [Google Scholar] [CrossRef]
- Panwar, H.; Gupta, P.; Siddiqui, M.K.; Morales-Menendez, R.; Singh, V. Application of deep learning for fast detection of COVID-19 in X-rays using nCOVnet. Chaos Solitons Fractals 2020, 138, 109944. [Google Scholar] [CrossRef] [PubMed]
- Ouchicha, C.; Ammor, O.; Meknassi, M. CVDNet: A novel deep learning architecture for detection of coronavirus (COVID-19) from chest X-ray images. Chaos Solitons Fractals 2020, 140, 110245. [Google Scholar] [CrossRef] [PubMed]
- Ismael, A.M.; Şengür, A. Deep learning approaches for COVID-19 detection based on chest X-ray images. Expert Syst. Appl. 2021, 164, 114054. [Google Scholar] [CrossRef]
- Arias-Garzón, D.; Alzate-Grisales, J.A.; Orozco-Arias, S.; Arteaga-Arteaga, H.B.; Bravo-Ortiz, M.A.; Mora-Rubio, A.; Saborit-Torres, J.M.; Serrano, J.Á.M.; de la Iglesia Vayá, M.; Cardona-Morales, O.; et al. COVID-19 detection in X-ray images using convolutional neural networks. Mach. Learn. Appl. 2021, 6, 100138. [Google Scholar] [CrossRef]
- Aswathy, A.; Hareendran, A.; SS, V.C. COVID-19 diagnosis and severity detection from CT-images using transfer learning and back propagation neural network. J. Infect. Public Health 2021, 14, 1435–1445. [Google Scholar]
- Hemdan, E.E.D.; Shouman, M.A.; Karar, M.E. Covidx-net: A framework of deep learning classifiers to diagnose COVID-19 in X-ray images. arXiv 2020, arXiv:2003.11055. [Google Scholar]
- Nayak, S.R.; Nayak, D.R.; Sinha, U.; Arora, V.; Pachori, R.B. Application of deep learning techniques for detection of COVID-19 cases using chest X-ray images: A comprehensive study. Biomed. Signal Process. Control 2021, 64, 102365. [Google Scholar] [CrossRef]
- Ibrahim, D.M.; Elshennawy, N.M.; Sarhan, A.M. Deep-chest: Multi-classification deep learning model for diagnosing COVID-19, pneumonia, and lung cancer chest diseases. Comput. Biol. Med. 2021, 132, 104348. [Google Scholar] [CrossRef]
- Hall, L.O.; Paul, R.; Goldgof, D.B.; Goldgof, G.M. Finding COVID-19 from chest x-rays using deep learning on a small dataset. arXiv 2020, arXiv:2004.02060. [Google Scholar]
- Das, A.K.; Kalam, S.; Kumar, C.; Sinha, D. TLCoV-An automated Covid-19 screening model using Transfer Learning from chest X-ray images. Chaos Solitons Fractals 2021, 144, 110713. [Google Scholar] [CrossRef] [PubMed]
- Saha, P.; Sadi, M.S.; Islam, M.M. EMCNet: Automated COVID-19 diagnosis from X-ray images using convolutional neural network and ensemble of machine learning classifiers. Inform. Med. Unlocked 2021, 22, 100505. [Google Scholar] [CrossRef]
- Zhang, J.; Xi, P.; Ebadi, A.; Azimi, H.; Tremblay, S.; Wong, A. COVID-19 Detection from Chest X-ray Images using Imprinted Weights Approach. arXiv 2021, arXiv:2105.01710. [Google Scholar]
- Shorfuzzaman, M.; Masud, M.; Alhumyani, H.; Anand, D.; Singh, A. Artificial Neural Network-Based Deep Learning Model for COVID-19 Patient Detection Using X-ray Chest Images. J. Healthc. Eng. 2021, 2021. [Google Scholar] [CrossRef] [PubMed]
- Ben Jabra, M.; Koubaa, A.; Benjdira, B.; Ammar, A.; Hamam, H. COVID-19 Diagnosis in Chest X-rays Using Deep Learning and Majority Voting. Appl. Sci. 2021, 11, 2884. [Google Scholar] [CrossRef]
- Feki, I.; Ammar, S.; Kessentini, Y.; Muhammad, K. Federated learning for COVID-19 screening from Chest X-ray images. Appl. Soft Comput. 2021, 106, 107330. [Google Scholar] [CrossRef]
- Ghoshal, B.; Tucker, A. Estimating uncertainty and interpretability in deep learning for coronavirus (COVID-19) detection. arXiv 2020, arXiv:2003.10769. [Google Scholar]
- Li, J.; Zhao, G.; Tao, Y.; Zhai, P.; Chen, H.; He, H.; Cai, T. Multi-task contrastive learning for automatic CT and X-ray diagnosis of COVID-19. Pattern Recognition 2021, 114, 107848. [Google Scholar] [CrossRef]
- Xu, Y.; Lam, H.K.; Jia, G. MANet: A two-stage deep learning method for classification of COVID-19 from Chest X-ray images. Neurocomputing 2021, 443, 96–105. [Google Scholar] [CrossRef]
- Vaid, S.; Kalantar, R.; Bhandari, M. Deep learning COVID-19 detection bias: Accuracy through artificial intelligence. Int. Orthop. 2020, 44, 1539–1542. [Google Scholar] [CrossRef] [PubMed]
- Jain, G.; Mittal, D.; Thakur, D.; Mittal, M.K. A deep learning approach to detect COVID-19 coronavirus with X-ray images. Biocybern. Biomed. Eng. 2020, 40, 1391–1405. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, F.; Bukhari, S.A.C.; Keshtkar, F. A deep learning approach for COVID-19 8 viral pneumonia screening with x-ray images. Digit. Gov. Res. Pract. 2021, 2, 1–12. [Google Scholar] [CrossRef]
- Ardakani, A.A.; Kanafi, A.R.; Acharya, U.R.; Khadem, N.; Mohammadi, A. Application of deep learning technique to manage COVID-19 in routine clinical practice using CT images: Results of 10 convolutional neural networks. Comput. Biol. Med. 2020, 121, 103795. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, F.; Khan, M.U.G.; Javed, K. Deep learning model for distinguishing novel coronavirus from other chest related infections in X-ray images. Comput. Biol. Med. 2021, 134, 104401. [Google Scholar] [CrossRef]
- Zhu, Y.; Huang, C. An improved median filtering algorithm for image noise reduction. Phys. Procedia 2012, 25, 609–616. [Google Scholar] [CrossRef] [Green Version]
- Rajaraman, S.; Siegelman, J.; Alderson, P.O.; Folio, L.S.; Folio, L.R.; Antani, S.K. Iteratively pruned deep learning ensembles for COVID-19 detection in chest X-rays. IEEE Access 2020, 8, 115041–115050. [Google Scholar] [CrossRef]
- Medhi, K.; Jamil, M.; Hussain, I. Automatic detection of COVID-19 infection from chest X-ray using deep learning. medRxiv 2020. [Google Scholar] [CrossRef]
- Arnal, J.; Súcar, L. Hybrid filter based on fuzzy techniques for mixed noise reduction in color images. Appl. Sci. 2020, 10, 243. [Google Scholar] [CrossRef] [Green Version]
- Toğaçar, M.; Ergen, B.; Cömert, Z. COVID-19 detection using deep learning models to exploit Social Mimic Optimization and structured chest X-ray images using fuzzy color and stacking approaches. Comput. Biol. Med. 2020, 121, 103805. [Google Scholar] [CrossRef]
- Sharifrazi, D.; Alizadehsani, R.; Roshanzamir, M.; Joloudari, J.H.; Shoeibi, A.; Jafari, M.; Hussain, S.; Sani, Z.A.; Hasanzadeh, F.; Khozeimeh, F.; et al. Fusion of convolution neural network, support vector machine and Sobel filter for accurate detection of COVID-19 patients using X-ray images. Biomed. Signal Process. Control 2021, 68, 102622. [Google Scholar] [CrossRef] [PubMed]
- Canayaz, M. MH-COVIDNet: Diagnosis of COVID-19 using deep neural networks and meta-heuristic-based feature selection on X-ray images. Biomed. Signal Process. Control 2021, 64, 102257. [Google Scholar] [CrossRef] [PubMed]
- Jain, R.; Gupta, M.; Taneja, S.; Hemanth, D.J. Deep learning based detection and analysis of COVID-19 on chest X-ray images. Appl. Intell. 2021, 51, 1690–1700. [Google Scholar] [CrossRef] [PubMed]
- Joshi, R.C.; Yadav, S.; Pathak, V.K.; Malhotra, H.S.; Khokhar, H.V.S.; Parihar, A.; Kohli, N.; Himanshu, D.; Garg, R.K.; Bhatt, M.L.B.; et al. A deep learning-based COVID-19 automatic diagnostic framework using chest X-ray images. Biocybern. Biomed. Eng. 2021, 41, 239–254. [Google Scholar] [CrossRef]
- Park, J.; Kwak, I.Y.; Lim, C. A Deep Learning Model with Self-Supervised Learning and Attention Mechanism for COVID-19 Diagnosis Using Chest X-ray Images. Electronics 2021, 10, 1996. [Google Scholar] [CrossRef]
- Chowdhury, M.E.; Rahman, T.; Khandakar, A.; Mazhar, R.; Kadir, M.A.; Mahbub, Z.B.; Islam, K.R.; Khan, M.S.; Iqbal, A.; Al Emadi, N.; et al. Can AI help in screening viral and COVID-19 pneumonia? IEEE Access 2020, 8, 132665–132676. [Google Scholar] [CrossRef]
- Ahuja, S.; Panigrahi, B.K.; Dey, N.; Rajinikanth, V.; Gandhi, T.K. Deep transfer learning-based automated detection of COVID-19 from lung CT scan slices. Appl. Intell. 2021, 51, 571–585. [Google Scholar] [CrossRef]
- Yoo, S.H.; Geng, H.; Chiu, T.L.; Yu, S.K.; Cho, D.C.; Heo, J.; Choi, M.S.; Choi, I.H.; Cung Van, C.; Nhung, N.V.; et al. Deep learning-based decision-tree classifier for COVID-19 diagnosis from chest X-ray imaging. Front. Med. 2020, 7, 427. [Google Scholar] [CrossRef]
- Abbas, A.; Abdelsamea, M.M.; Gaber, M.M. Classification of COVID-19 in chest X-ray images using DeTraC deep convolutional neural network. Appl. Intell. 2021, 51, 854–864. [Google Scholar] [CrossRef]
- Chandra, T.B.; Verma, K.; Singh, B.K.; Jain, D.; Netam, S.S. Coronavirus disease (COVID-19) detection in chest X-ray images using majority voting based classifier ensemble. Expert Syst. Appl. 2021, 165, 113909. [Google Scholar] [CrossRef]
- Xu, X.; Jiang, X.; Ma, C.; Du, P.; Li, X.; Lv, S.; Yu, L.; Ni, Q.; Chen, Y.; Su, J.; et al. A deep learning system to screen novel coronavirus disease 2019 pneumonia. Engineering 2020, 6, 1122–1129. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Kang, B.; Ma, J.; Zeng, X.; Xiao, M.; Guo, J.; Cai, M.; Yang, J.; Li, Y.; Meng, X.; et al. A deep learning algorithm using CT images to screen for Corona Virus Disease (COVID-19). Eur. Radiol. 2021, 31, 6096–6104. [Google Scholar] [CrossRef] [PubMed]
- Alshazly, H.; Linse, C.; Barth, E.; Martinetz, T. Explainable COVID-19 detection using chest ct scans and deep learning. Sensors 2021, 21, 455. [Google Scholar] [CrossRef] [PubMed]
- Sedik, A.; Iliyasu, A.M.; El-Rahiem, A.; Abdel Samea, M.E.; Abdel-Raheem, A.; Hammad, M.; Peng, J.; El-Samie, A.; Fathi, E.; El-Latif, A.; et al. Deploying machine and deep learning models for efficient data-augmented detection of COVID-19 infections. Viruses 2020, 12, 769. [Google Scholar] [CrossRef]
- Khalifa, N.E.M.; Taha, M.H.N.; Hassanien, A.E.; Elghamrawy, S. Detection of coronavirus (COVID-19) associated pneumonia based on generative adversarial networks and a fine-tuned deep transfer learning model using chest X-ray dataset. arXiv 2020, arXiv:2004.01184. [Google Scholar]
- Loey, M.; Manogaran, G.; Khalifa, N.E.M. A deep transfer learning model with classical data augmentation and CGAN to detect COVID-19 from chest CT radiography digital images. Neural Comput. Appl. 2020, 1–13. [Google Scholar] [CrossRef]
- Shi, F.; Wang, J.; Shi, J.; Wu, Z.; Wang, Q.; Tang, Z.; He, K.; Shi, Y.; Shen, D. Review of artificial intelligence techniques in imaging data acquisition, segmentation, and diagnosis for COVID-19. IEEE Rev. Biomed. Eng. 2020, 14, 4–15. [Google Scholar] [CrossRef] [Green Version]
- Gozes, O.; Frid-Adar, M.; Greenspan, H.; Browning, P.D.; Zhang, H.; Ji, W.; Bernheim, A.; Siegel, E. Rapid ai development cycle for the coronavirus (COVID-19) pandemic: Initial results for automated detection & patient monitoring using deep learning ct image analysis. arXiv 2020, arXiv:2003.05037. [Google Scholar]
- Tang, L.; Zhang, X.; Wang, Y.; Zeng, X. Severe COVID-19 pneumonia: Assessing inflammation burden with volume-rendered chest CT. Radiol. Cardiothorac. Imaging 2020, 2, e200044. [Google Scholar] [CrossRef] [Green Version]
- Cao, Y.; Xu, Z.; Feng, J.; Jin, C.; Han, X.; Wu, H.; Shi, H. Longitudinal assessment of COVID-19 using a deep learning–based quantitative CT pipeline: Illustration of two cases. Radiol. Cardiothorac. Imaging 2020, 2, e200082. [Google Scholar] [CrossRef] [Green Version]
- Long, J.; Shelhamer, E.; Darrell, T. Fully convolutional networks for semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 3431–3440. [Google Scholar]
- Badrinarayanan, V.; Kendall, A.; Cipolla, R. Segnet: A deep convolutional encoder-decoder architecture for image segmentation. IEEE Trans. Pattern Anal. Mach. Intell. 2017, 39, 2481–2495. [Google Scholar] [CrossRef] [PubMed]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional networks for biomedical image segmentation. In Medical Image Computing and Computer-Assisted Intervention; Springer: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Zheng, C.; Deng, X.; Fu, Q.; Zhou, Q.; Feng, J.; Ma, H.; Liu, W.; Wang, X. Deep learning-based detection for COVID-19 from chest CT using weak label. medRxiv 2020, 26. [Google Scholar] [CrossRef] [Green Version]
- Huang, L.; Han, R.; Ai, T.; Yu, P.; Kang, H.; Tao, Q.; Xia, L. Serial quantitative chest CT assessment of COVID-19: A deep learning approach. Radiol. Cardiothorac. Imaging 2020, 2, e200075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, S.; Cheng, M.M.; Zhao, K.; Zhang, X.Y.; Yang, M.H.; Torr, P.H. Res2net: A new multi-scale backbone architecture. IEEE Trans. Pattern Anal. Mach. Intell. 2019, 43, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Lu, H.; Yang, Z.; Qiu, S.; Huo, B.; Dong, Y. The ensemble deep learning model for novel COVID-19 on CT images. Appl. Soft Comput. 2021, 98, 106885. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Deng, X.; Fu, Q.; Zhou, Q.; Feng, J.; Ma, H.; Liu, W.; Zheng, C. A weakly-supervised framework for COVID-19 classification and lesion localization from chest CT. IEEE Trans. Med. Imaging 2020, 39, 2615–2625. [Google Scholar] [CrossRef]
- Shan, F.; Gao, Y.; Wang, J.; Shi, W.; Shi, N.; Han, M.; Xue, Z.; Shen, D.; Shi, Y. Lung infection quantification of COVID-19 in CT images with deep learning. arXiv 2020, arXiv:2003.04655. [Google Scholar]
- Chen, J.; Wu, L.; Zhang, J.; Zhang, L.; Gong, D.; Zhao, Y.; Chen, Q.; Huang, S.; Yang, M.; Yang, X.; et al. Deep learning-based model for detecting 2019 novel coronavirus pneumonia on high-resolution computed tomography. Sci. Rep. 2020, 10, 19196. [Google Scholar] [CrossRef]
- Alom, M.Z.; Rahman, M.; Nasrin, M.S.; Taha, T.M.; Asari, V.K. COVID_MTNet: COVID-19 detection with multi-task deep learning approaches. arXiv 2020, arXiv:2004.03747. [Google Scholar]
- Rajinikanth, V.; Kadry, S.; Thanaraj, K.P.; Kamalanand, K.; Seo, S. Firefly-algorithm supported scheme to detect COVID-19 lesion in lung ct scan images using Shannon entropy and Markov-random-field. arXiv 2020, arXiv:2004.09239. [Google Scholar]
- Kassania, S.H.; Kassanib, P.H.; Wesolowskic, M.J.; Schneidera, K.A.; Detersa, R. Automatic detection of coronavirus disease (COVID-19) in X-ray and CT images: A machine learning based approach. Biocybern. Biomed. Eng. 2021, 41, 867–879. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A.; Alshamrani, A.M.; Alrasheedi, A.F.; Alnowibet, K.A.; Mohamed, A.W. A Hybrid Approach Based on Principal Component Analysis for Power Quality Event Classification Using Support Vector Machines. Mathematics 2022, 10, 2780. [Google Scholar] [CrossRef]
- Apostolopoulos, I.D.; Mpesiana, T.A. COVID-19: Automatic detection from X-ray images utilizing transfer learning with convolutional neural networks. Phys. Eng. Sci. Med. 2020, 43, 635–640. [Google Scholar] [CrossRef] [Green Version]
- Mucahid, B.; Umut, O.; Saban, O. Classification of Coronavirus Images using Shrunken Features. medRxiv 2020. [Google Scholar] [CrossRef]
- Barstugan, M.; Ozkaya, U.; Ozturk, S. Coronavirus (COVID-19) classification using ct images by machine learning methods. arXiv 2020, arXiv:2003.09424. [Google Scholar]
- Tuncer, T.; Dogan, S.; Ozyurt, F. An automated residual exemplar local binary pattern and iterative ReliefF based COVID-19 detection method using chest X-ray image. Chemom. Intell. Lab. Syst. 2020, 203, 104054. [Google Scholar] [CrossRef]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016; Available online: http://www.deeplearningbook.org (accessed on 7 December 2022).
- Tan, C.; Sun, F.; Kong, T.; Zhang, W.; Yang, C.; Liu, C. A survey on deep transfer learning. In Artificial Neural Networks; Springer: Cham, Switzerland, 2018; pp. 270–279. [Google Scholar]
- Basu, S.; Mitra, S.; Saha, N. Deep learning for screening COVID-19 using chest X-ray images. In Proceedings of the 2020 IEEE Symposium Series on Computational Intelligence (SSCI), Canberra, Australia, 1–4 December 2020; pp. 2521–2527. [Google Scholar]
- Brunese, L.; Mercaldo, F.; Reginelli, A.; Santone, A. Explainable deep learning for pulmonary disease and coronavirus COVID-19 detection from X-rays. Comput. Methods Programs Biomed. 2020, 196, 105608. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Jiang, W.; Qiu, X. Deep learning for COVID-19 detection based on CT images. Sci. Rep. 2021, 11, 14353. [Google Scholar] [CrossRef] [PubMed]
- Maghdid, H.S.; Asaad, A.T.; Ghafoor, K.Z.; Sadiq, A.S.; Mirjalili, S.; Khan, M.K. Diagnosing COVID-19 pneumonia from X-ray and CT images using deep learning and transfer learning algorithms. In Proceedings of the Multimodal Image Exploitation and Learning 2021; SPIE: Bellingham, WA, USA, 2021; Volume 11734, pp. 99–110. [Google Scholar]
- He, X.; Yang, X.; Zhang, S.; Zhao, J.; Zhang, Y.; Xing, E.; Xie, P. Sample-efficient deep learning for COVID-19 diagnosis based on CT scans. medRxiv 2020. [Google Scholar] [CrossRef]
- Ko, H.; Chung, H.; Kang, W.S.; Kim, K.W.; Shin, Y.; Kang, S.J.; Lee, J.H.; Kim, Y.J.; Kim, N.Y.; Jung, H.; et al. COVID-19 pneumonia diagnosis using a simple 2D deep learning framework with a single chest CT image: Model development and validation. J. Med. Internet Res. 2020, 22, e19569. [Google Scholar] [CrossRef]
- Serte, S.; Demirel, H. Deep learning for diagnosis of COVID-19 using 3D CT scans. Comput. Biol. Med. 2021, 132, 104306. [Google Scholar] [CrossRef] [PubMed]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 770–778. [Google Scholar]
- Wu, Z.; Shen, C.; Van Den Hengel, A. Wider or deeper: Revisiting the resnet model for visual recognition. Pattern Recognit. 2019, 90, 119–133. [Google Scholar] [CrossRef] [Green Version]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the inception architecture for computer vision. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 2818–2826. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Delving deep into rectifiers: Surpassing human-level performance on imagenet classification. In Proceedings of the IEEE International Conference on Computer Vision, Santiago, Chile, 7–13 December 2015; pp. 1026–1034. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. Adv. Neural Inf. Process. Syst. 2012, 5, 1106–1114. [Google Scholar] [CrossRef] [Green Version]
- Howard, A.G.; Zhu, M.; Chen, B.; Kalenichenko, D.; Wang, W.; Weyand, T.; Andreetto, M.; Adam, H. Mobilenets: Efficient convolutional neural networks for mobile vision applications. arXiv 2017, arXiv:1704.04861. [Google Scholar]
- Iandola, F.N.; Han, S.; Moskewicz, M.W.; Ashraf, K.; Dally, W.J.; Keutzer, K. SqueezeNet: AlexNet-level accuracy with 50× fewer parameters and <0.5 MB model size. arXiv 2017, arXiv:1602.0736. [Google Scholar]
- Nanni, L.; Ghidoni, S.; Brahnam, S. Handcrafted vs. non-handcrafted features for computer vision classification. Pattern Recognit. 2017, 71, 158–172. [Google Scholar] [CrossRef]
- Hegde, R.B.; Prasad, K.; Hebbar, H.; Singh, B.M.K. Feature extraction using traditional image processing and convolutional neural network methods to classify white blood cells: A study. Australas. Phys. Eng. Sci. Med. 2019, 42, 627–638. [Google Scholar] [CrossRef]
- Bora, K.; Chowdhury, M.; Mahanta, L.B.; Kundu, M.K.; Das, A.K. Pap smear image classification using convolutional neural network. In Proceedings of the Tenth Indian Conference on Computer Vision, Graphics and Image Processing, Guwahati, India, 18–22 December 2016; pp. 1–8. [Google Scholar]
- Hoshyar, A.N.; Al-Jumaily, A.; Hoshyar, A.N. The beneficial techniques in preprocessing step of skin cancer detection system comparing. Procedia Comput. Sci. 2014, 42, 25–31. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Datasets | Description | Source | References |
|---|---|---|---|
| COVID-19, SARS, MERS X-ray Images Dataset | Includes 423 COVID-19, 134 SARS, and 144 MERS images with the corresponding lung masks | Developed by researchers from Qatar University and the University of Dhaka | Yazan Qiblawey (2022) Last updated: 12 January 2022 http://doi.org/10.34740/kaggle/dsv/3034344 |
| COVID-19 Pneumonia-Normal Chest X-ray Images | Includes COVID-19, normal, and pneumonia images | Collected from different sources including GitHub, Radiopaedia, The Cancer Imaging Archive (TCIA), and the Italian Society of Radiology (SIRM) | Sachin Kumar (2022) Last updated: 14 June 2022 http://doi.org/10.17632/dvntn9yhd2.1 |
| COVID-19 Digital X-rays Forgery Dataset | Includes COVID-19, CM COVID-19, S COVID-19, Normal images, CM Normal, S Normal, Viral Pneumonia, S Viral Pneumonia, and CM Viral Pneumonia | Modified dataset from “COVID-19 Radiography Database” | Nour Eldeen Khalifa (2022) Last updated: 17 March 2022 http://doi.org/10.17632/3bzv6t24ts.1 |
| QaTa-COV19 Dataset | Contains two datasets: the QaTa-COV19 Dataset (Extended) includes 9258 COVID-19 chest X-ray images, while the Early-QaTa-COV19 Dataset includes 1065 chest X-rays | Developed by researchers from Qatar university and Tampere university | aysendegerli (2022) Last updated: 22 February 2022 https://www.kaggle.com/aysendegerli/qatacov19-dataset |
| Chest X-ray Dataset for Respiratory Disease Classification | Includes five classes from 32,687 chest X-ray radiography images with reasonable resolution (COVID-19, pneumonia, tuberculosis, lung opacity, and normal) | Combination of multiple different datasets gathered from diverse sources | Harvard Dataverse (2022) Last updated: 10 February 2022 http://doi.org/10.7910/DVN/WNQ3GI |
| COVID Pneumonia dataset | Includes 1950 X-ray images with three classes (COVID, normal, and pneumonia) | Italian Society of Medical, Radiopaedia, and NIH Clinical Center | Redwanul Islam (2022) Last updated: 3 January 2022 https://www.kaggle.com/redwan1010/covid-pneumonia-dataset |
| xray-binary-covid | Processed COVID-19 X-ray images for DL models. Includes 2000 COVID and 2000 normal images | Information is not available | Aravind Lade (2022) Last updated: 8 February 2022 https://www.kaggle.com/aravindlade/xray-binary-covid |
| COVID-19 Chest X-ray Image Repository | Includes 900 images. Several of the images are of children or early-stage patients for whom the radiologist noticed no unique imaging findings | Gathered from a variety of online sources | Arman Haghanifar; Mahdiyar Molahasani Majdabadi; Seokbum Ko (2022) Last updated: 2 February 2022 http://doi.org/10.6084/m9.figshare.12580328.v3 |
| COVID-19 Radiography Database | Includes lung masks and 3616 COVID-19 chest X-ray pictures | Developed by researchers from Qatar University, and the University of Dhaka along with their Pakistani and Malaysian counterparts, and medical practitioners conducted the study | Tawsifur Rahman (2022) Last updated: 19 March 2022 https://www.kaggle.com/tawsifurrahman/COVID19-radiography-database |
| X-ray Image Dataset For COVID-19 Detection (A) | Includes 392 X-ray images (COVID and normal) | Collected from “COVID-chestxray-dataset” in GitHub and “chest-xray-pneumonia” in kaggle | Mohammed Ali-11 (2022) Last updated: 22 March 2022 https://www.kaggle.com/datasets/mohammedali11/xray-image-dataset-for-covid19-detection-a |
| Curated COVID-19 Chest X-ray Dataset | Includes 9208 chest x-rays (normal, COVID-19, and pneumonia) | Derived from the “Curated Dataset for COVID-19 Posterior-Anterior Chest Radiography Images (X-rays)” | Francis Jesmar Montalbo (2022) Last updated: 25 March 2022 https://www.kaggle.com/datasets/francismon/curated-covid19-chest-xray-dataset |
| COVID-19 Pakistani Patients X-ray Image Dataset | Includes 390 COVID-19 and 60 normal chest X-ray Images | Developed by researchers from Edinburgh Napier University UK, HITEC University Taxila, and PNEC Karachi, Pakistan along with their collaborators from Kingdom of Saudi Arabia and in collaboration with medical doctors | Muhammad Shahbaz Khan (2022) Last updated: 21 May 2022 https://www.kaggle.com/datasets/muhammadshahbazkhan/covid19-pakistani-patients-xray-image-dataset |
| Datasets | Description | Source | References |
|---|---|---|---|
| COVID-CTset: A Large COVID-19 CT Scans dataset | Includes 63,849 CT images of 377 patients (15,589 obtained from 95 COVID-19 patients and 48,260 CT scan from 282 normal individuals). One of the largest COVID-19 CT scan datasets for AI researchers | Iran’s Negin medical center, located in the city of Sari | Mohammad Rahimzadeh (2022) Last updated: 7 March 2022 https://www.kaggle.com/mohammadrahimzadeh/covidctset-a-large-covid19-ct-scans-dataset |
| HRCTv1-COVID-19 | Includes 181,106 images obtained from 395 patients: GGO (288 cases), Crazy Paving (57 cases), and Air Space Consolidation (27 cases), as well as 23 cases with a negative diagnosis | Sfahan University of Technology, Arak University of Medical Sciences, Isfahan University of Medical Sciences, Islamic Azad University Science and Research Branch | Iraj abedi (2022) Last updated: 5 May 2022 http://doi.org/10.17632/nc5g3zs7g7.2 |
| COVID-19 CT Dataset | Includes 368 medical findings in Chinese and 1104 chest CT scans | Constructed by Shenzhen Research Institute of Big Data (SRIBD), Future Network of Intelligence Institute (FNii) and CUHKSZ-JD Joint AI Lab | Chinese University of Hongkong, Shenzhen, China (2022) https://paperswithcode.com/dataset/covid-dataset accessed on 7 December 2022 |
| COVID-19 Omicron and Delta Variant Lung CT Scans | Includes 14,482 CT scans (12,231 positive for COVID-19 and 2251 negative); data are available as 512 × 512 px JPG images | Collected from patients in radiology centers of teaching hospitals of Tehran, Iran | M Amir Eshraghi (2022) Last updated: 7 February 2022 https://www.kaggle.com/mohammadamireshraghi/covid19-omicron-and-delta-variant-ct-scan-dataset |
| Datasets | Description | Source | References |
|---|---|---|---|
| Data from: Use of lung ultrasound in neonates during the COVID-19 pandemic | Includes 27 ultrasound images of the lungs of newborns with a suspected or confirmed diagnosis of COVID-19, differentiating between disease-related and non-disease-related alterations | - | Marcia Wang Matsuoka (2021) Last updated: 25 March 2021 http://doi.org/10.6084/m9.figshare.14278767.v1 |
| COVID-19 Dataset | Includes ultrasound images grouped as COVID, pneumonia, and regular | Kafrelsheikh University | Ahmed sedik (2020) Last updated: 9 May 2022 http://doi.org/10.17632/6rs5mnvktk.1 |
| References | Preliminary Stages Before the Detection Process | Database Description | |||
|---|---|---|---|---|---|
| Preprocessing | Augmentations | Segmentation | Feature Extraction | ||
| [6] | no | no | yes | no | Brief (low) |
| [14] | no | no | yes | no | Medium |
| [26] | no | no | no | no | Detail (high) |
| [29] | no | no | yes | no | Medium |
| [31] | no | no | yes | no | Brief (low) |
| [27] | no | no | no | no | Medium |
| [30] | no | yes | yes | no | Detail (high) |
| [28] | no | no | no | no | Detail (high) |
| [33] | no | no | yes | no | Detail (high) |
| [32] | yes | yes | yes | no | Brief (low) |
| Our Study | yes | yes | yes | yes | Detail (high) |
| Augmentation Methods | Purpose | Augmentation Techniques | Dataset | Author |
|---|---|---|---|---|
| Geometric Transformations | Reduce the bias caused by the properties of CXR images | flipping, zooming, shifting | CXR images | [67] |
| Increase dataset size | rotating, scaling | CXR images | [66] | |
| Propose a robust technique for automatic detection of COVID-19 pneumonia | rotating, scaling, translation | X-ray images | [68] | |
| Increase dataset size to achieve efficient and consistent accuracy | flipping, rotating, skewing | X-ray and CT images | [42] | |
| Solve overfitting problem | rotating, shearing, translation, novel data augmentation | CT images | [69] | |
| Improve CNN model training and classification accuracy | flipping, rotating, translation | X-ray images | [70] | |
| Generate more samples | flipping, rotating, translation | X-ray images | [71] | |
| Prevent overfitting | rotating, zooming, shearing. | X-ray images | [65] | |
| Increase training set size | flipping, rotating, scaling, Gaussian noise addition | X-ray images | [41] | |
| Photometric Transformations | Enhance images | sharpening, blurring, brightness, contrast adjustment | X-ray images | [72] |
| Avoid model overfitting | blurring, sharpening, contrast adjustment | CT images | [73,74] | |
| Avoid model overfitting | blurring, sharpening, contrast adjustment | X-ray images | [68] | |
| Geometric and Photometric Transformations | Increase training samples and improve generalization | cropping, blurring, Gaussian noise addition, brightness and contrast adjustment, flipping | CXR images | [53] |
| Increase training samples and improved generalization | cropping, blurring, Gaussian noise addition, brightness and contrast adjustment, flipping | CT images | [75] | |
| DL Augmentation | Improve COVID-19 detection | Augmentation based on basic image alteration and GANs | X-ray and CT images | [76] |
| Overcome overfitting problem and generate more images | GAN | X-ray images | [77] | |
| Traditional and DL Augmentation | Generate a balanced training set | Rotation and translation (CNNs) | X-ray images | [68] |
| Assess data augmentation impact on the accuracy of COVID-19 detection | Variety of traditional image transformations and GANs | X-ray and CT images | [76] | |
| Generate additional images and improve classification performance. | Traditional data augmentations with CGAN | CT images | [78] |
| Pre-Trained CNN Models | X-rays Studies | CT-Scans Studies | Advantages | Disadvantages |
|---|---|---|---|---|
| VGG-family [110] | [34,41,53,103,104] | [41,108] |
|
|
| ResNet-family [111,112] | [41,54,103] | [56,89,108,109] |
| Increased overhead due to:
|
| Inception- family [113,114] | [41,54] | [56,89,108] |
|
|
| AlexNet [115] | [41,103] | [56,89] |
|
|
| MobileNet [116] | [41] | [56] |
|
|
| SqueezeNet [117] | [41] | [56] |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alhaj, T.A.; Idris, I.; Elhaj, F.A.; Elhassan, T.A.; Remli, M.A.; Siraj, M.M.; Mohd Rahim, M.S. Preliminary Stages for COVID-19 Detection Using Image Processing. Diagnostics 2022, 12, 3171. https://doi.org/10.3390/diagnostics12123171
Alhaj TA, Idris I, Elhaj FA, Elhassan TA, Remli MA, Siraj MM, Mohd Rahim MS. Preliminary Stages for COVID-19 Detection Using Image Processing. Diagnostics. 2022; 12(12):3171. https://doi.org/10.3390/diagnostics12123171
Chicago/Turabian StyleAlhaj, Taqwa Ahmed, Inshirah Idris, Fatin A. Elhaj, Tusneem A. Elhassan, Muhammad Akmal Remli, Maheyzah Md Siraj, and Mohd Shafry Mohd Rahim. 2022. "Preliminary Stages for COVID-19 Detection Using Image Processing" Diagnostics 12, no. 12: 3171. https://doi.org/10.3390/diagnostics12123171