
Signs, Symptoms, and Side-Effects Presented by Different Types of COVID-19 Vaccines: A Prospective Cohort Study


Abstract
:1. Introduction
The COVID-19 Vaccination in Iran
2. Method
2.1. Study Population and Data Collection
2.2. Ethics Approval and Consent to Participate
2.3. Inclusion and Exclusion Criteria
2.4. Instrument
2.5. Statistical Analysis and Sample Size
3. Results
3.1. Basic Characteristics
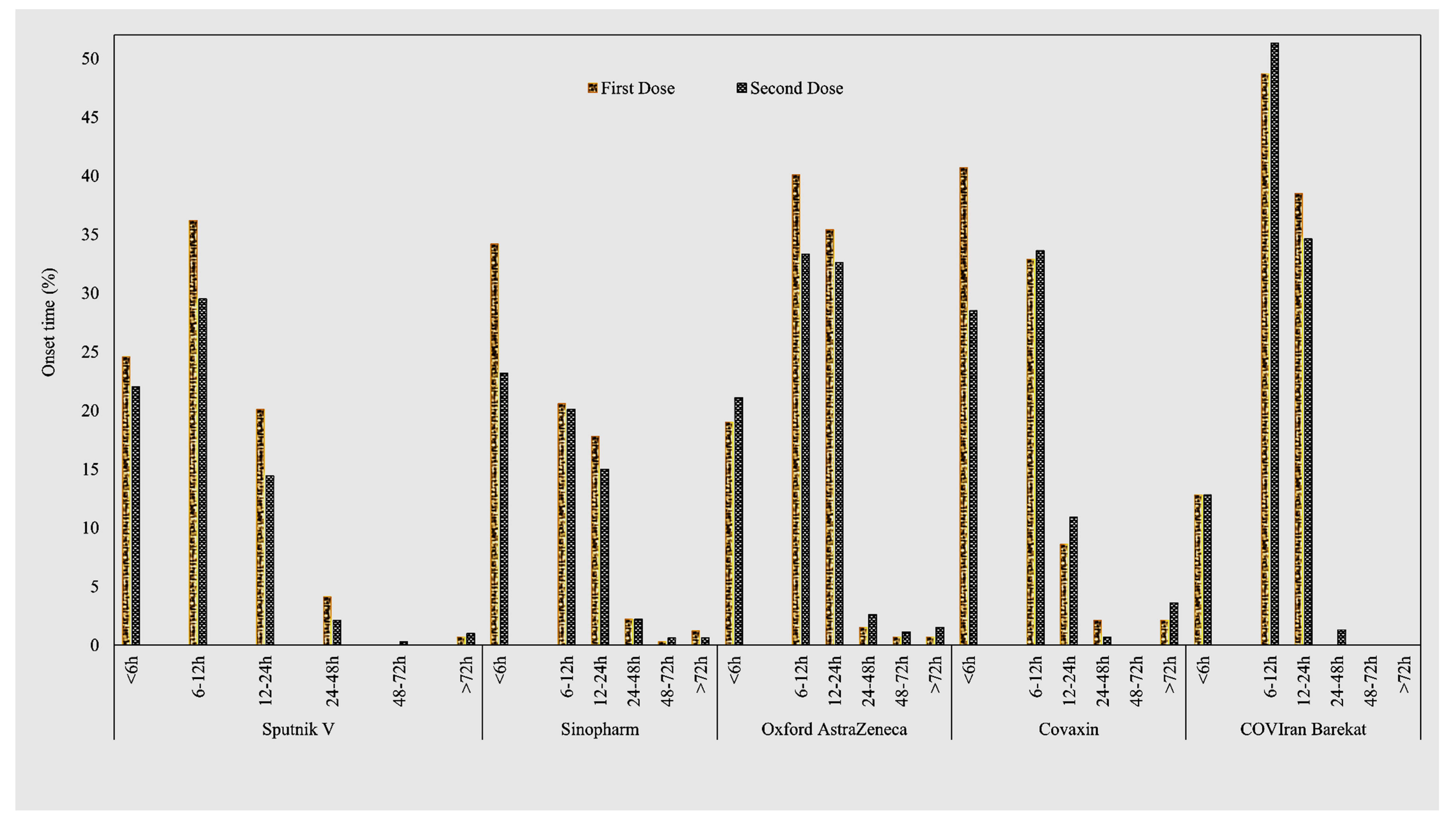
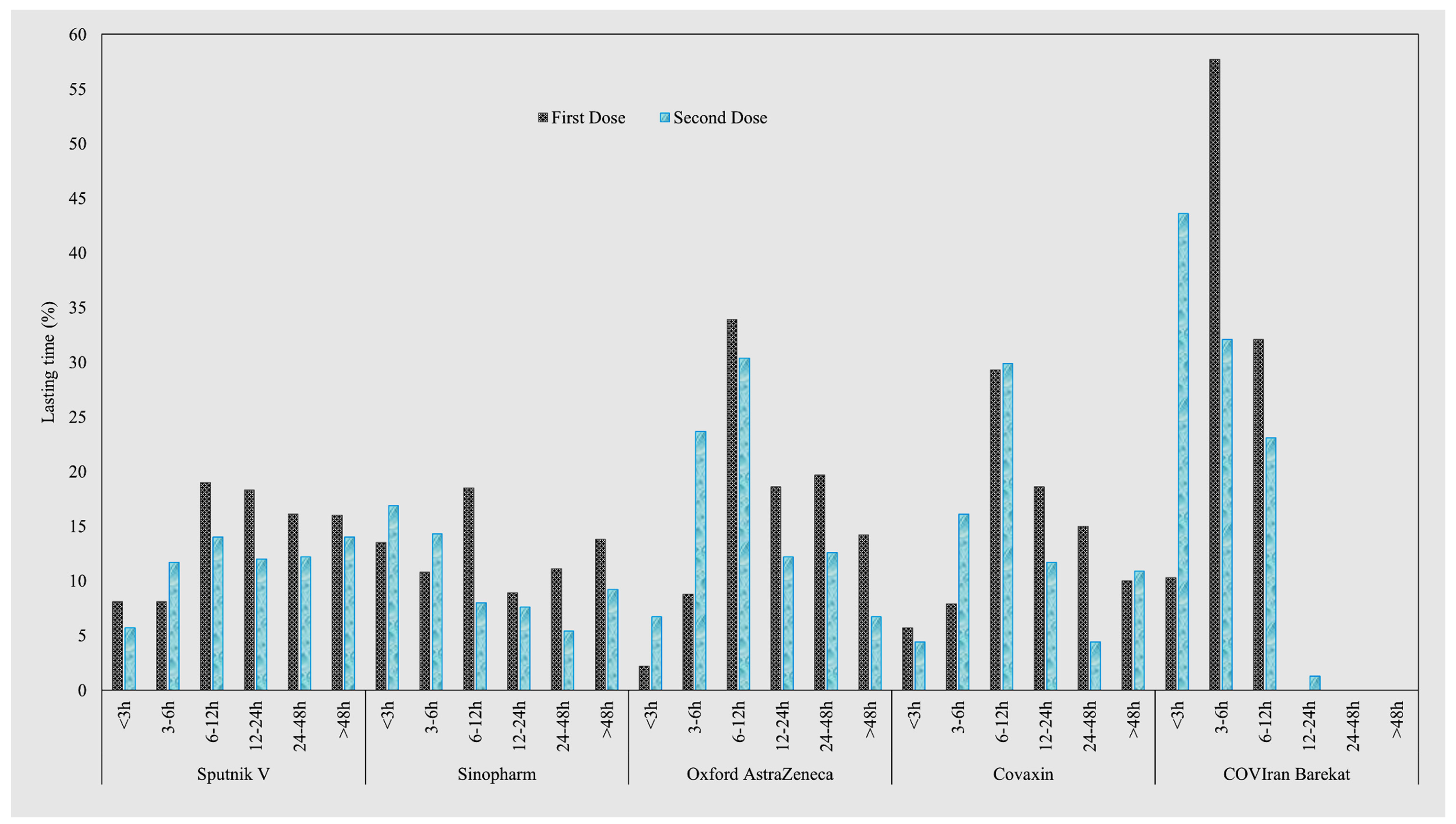
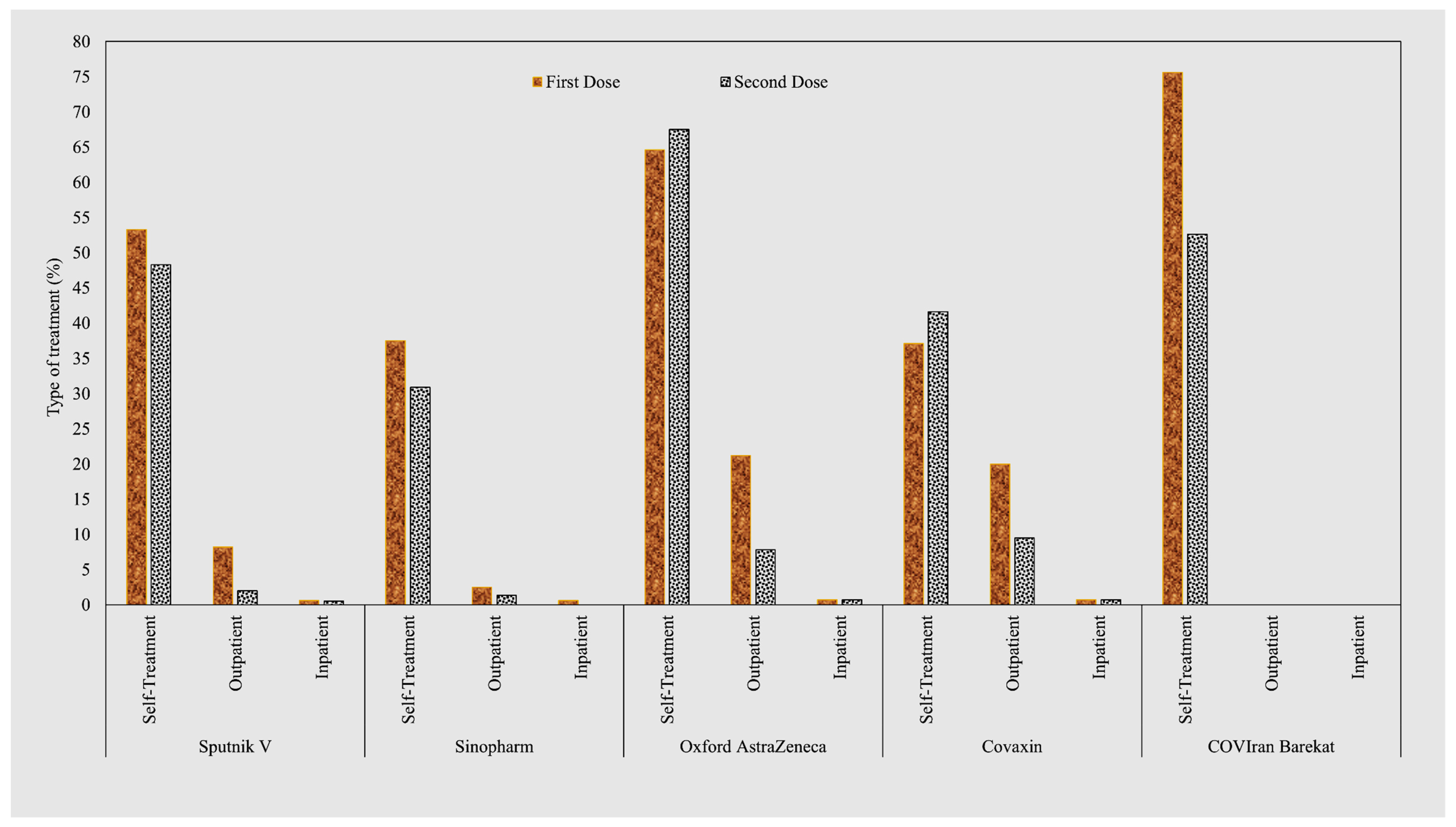
3.2. Characteristics of Post-COVID-19 Vaccination Signs and Symptoms
3.3. Post-COVID-19 Vaccination Local Signs and Symptoms Following the First and Second Doses
3.4. Post-COVID-19 Vaccination Systemic Signs and Symptoms Following the First and Second Doses
4. Discussion
5. Strength and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 7 January 2022).
- Virus Taxonomy: Classification and Nomenclature of Viruses. Seventh Report of the International Committee on Taxonomy of Viruses. Available online: https://www.cabdirect.org/cabdirect/abstract/20013040876 (accessed on 27 November 2022).
- Saied, E.M.; El-Maradny, Y.A.; Osman, A.A.; Darwish, A.M.G.; Abo Nahas, H.H.; Niedbała, G.; Piekutowska, M.; Abdel-Rahman, M.A.; Balbool, B.A.; Abdel-Azeem, A.M. A Comprehensive Review about the Molecular Structure of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): Insights into Natural Products against COVID-19. Pharmaceutics 2021, 13, 1759. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, A.A.T.; Fatima, K.; Mohammad, T.; Fatima, U.; Singh, I.K.; Singh, A.; Atif, S.M.; Hariprasad, G.; Hasan, G.M.; Hassan, M.I. Insights into SARS-CoV-2 genome, structure, evolution, pathogenesis and therapies: Structural genomics approach. Biochim. Biophys. Acta BBA—Mol. Basis Dis. 2020, 1866, 165878. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. COVID-19 Strategic Preparedness and Response Plan: Operational Planning Guideline: 1 February 2021 to 31 January 2022; World Health Organization: Geneva, Switzerland, 2021.
- Mirzaei, F.; Vafaei, S.A.; Abbasi-Oshaghi, E. Regarding the Article: Coronavirus Disease (COVID-19): Current Status and Prospects for Drug and Vaccine Development. Arch. Med. Res. 2021, 52, 456. [Google Scholar] [CrossRef] [PubMed]
- Bogdanov, G.; Bogdanov, I.; Kazandjieva, J.; Tsankov, N. Cutaneous adverse effects of the available COVID-19 vaccines. Clin. Dermatol. 2021, 39, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Cavaleri, M.; Enzmann, H.; Straus, S.; Cooke, E. The European Medicines Agency’s EU conditional marketing authorisations for COVID-19 vaccines. The Lancet 2021, 397, 355–357. [Google Scholar] [CrossRef] [PubMed]
- Coronavirus Vaccination Information from Other Organisations. Available online: https://www.england.nhs.uk/coronavirus/covid-19-vaccination-programme/key-vaccination-information/ (accessed on 7 January 2022).
- Possible Side Effects After Getting a COVID-19 Vaccine|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/expect/after.html (accessed on 7 January 2022).
- Side Effects of COVID-19 Vaccines. Available online: https://www.who.int/news-room/feature-stories/detail/side-effects-of-covid-19-vaccines (accessed on 7 January 2022).
- Zare, H.; Rezapour, H.; Mahmoodzadeh, S.; Fereidouni, M. Prevalence of COVID-19 vaccines (Sputnik V, AZD-1222, and Covaxin) side effects among healthcare workers in Birjand city, Iran. Int. Immunopharmacol. 2021, 101, 108351. [Google Scholar] [CrossRef] [PubMed]
- Hatmal, M.M.; Al-Hatamleh, M.A.; Olaimat, A.N.; Hatmal, M.; Alhaj-Qasem, D.M.; Olaimat, T.M.; Mohamud, R. Side Effects and Perceptions Following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects. Vaccines 2021, 9, 556. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021, 21, 939–949. [Google Scholar] [CrossRef] [PubMed]
- Klugar, M.; Riad, A.; Mekhemar, M.; Conrad, J.; Buchbender, M.; Howaldt, H.P.; Attia, S. Side Effects of mRNA-Based and Viral Vector-Based COVID-19 Vaccines among German Healthcare Workers. Biology 2021, 10, 752. [Google Scholar] [CrossRef] [PubMed]
- Lounis, M.; Rais, M.A.; Bencherit, D.; Aouissi, H.A.; Oudjedi, A.; Klugarová, J.; Pokorná, A.; Klugar, M.; Riad, A. Side Effects of COVID-19 Inactivated Virus vs. Adenoviral Vector Vaccines: Experience of Algerian Healthcare Workers. Front. Public Health 2022, 10, 896343. [Google Scholar] [CrossRef] [PubMed]
- COVID, C.; Team, R. Allergic reactions including anaphylaxis after receipt of the first dose of Pfizer-BioNTech COVID-19 vaccine—United States, December 14–23, 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 46. [Google Scholar]
- Tsilingiris, D.; Vallianou, N.G.; Karampela, I.; Dalamaga, M. Vaccine induced thrombotic thrombocytopenia: The shady chapter of a success story. Metab. Open 2021, 11, 100101. [Google Scholar] [CrossRef] [PubMed]
- CDC COVID-19 Vaccination. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/adverse-events.html (accessed on 7 January 2022).
- Tavilani, A.; Abbasi, E.; Ara, F.K.; Darini, A.; Asefy, Z. COVID-19 vaccines: Current evidence and considerations. Metab. Open 2021, 12, 100124. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Operational Guidance: COVID-19 Immunization Service Delivery Modalities; World Health Organization: Geneva, Switzerland; Regional Office for Europe: Copenhagen, Denmark, 2021.
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef] [PubMed]
- Solomon, Y.; Eshete, T.; Mekasha, B.; Assefa, W. COVID-19 Vaccine: Side Effects After the First Dose of the Oxford AstraZeneca Vaccine Among Health Professionals in Low-Income Country: Ethiopia. J. Multidiscip. Healthc. 2021, 14, 2577. [Google Scholar] [CrossRef]
- Iran Reports Its First 2 Cases of the New Coronavirus. New York Times—Google Search. Available online: https://www.timesofisrael.com/iran-reports-its-first-2-cases-of-the-new-coronavirus/ (accessed on 7 January 2022).
- Iran COVID—Coronavirus Statistics—Worldometer. Available online: https://www.worldometers.info/coronavirus/country/iran/ (accessed on 10 January 2022).
- Iran (Islamic Republic of)—COVID19 Vaccine Tracker. Available online: https://covid19.trackvaccines.org/country/iran-islamic-republic-of/ (accessed on 7 January 2022).
- Challenges of COVID-19 Vaccination in Iran: In the Fourth Wave of Pandemic Spread | Prehospital and Disaster Medicine | Cambridge Core. Available online: https://www.cambridge.org/core/journals/prehospital-and-disaster-medicine/article/challenges-of-covid19-vaccination-in-iran-in-the-fourth-wave-of-pandemic-spread/84160F25E169A52DDDBF48C8F252CFB0# (accessed on 7 January 2022).
- Chapin-Bardales, J.; Gee, J.; Myers, T. Reactogenicity following receipt of mRNA-based COVID-19 vaccines. JAMA 2021, 325, 2201–2202. [Google Scholar] [CrossRef]
- Kadali, R.A.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 Vaccine Side Effects among Healthcare Workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef]
- Saeed, B.Q.; Al-Shahrabi, R.; Alhaj, S.S.; Alkokhardi, Z.M.; Adrees, A.O. Side effects and perceptions following Sinopharm COVID-19 vaccination. Int. J. Infect. Dis. 2021, 111, 219–226. [Google Scholar] [CrossRef]
- Fathizadeh, H.; Afshar, S.; Masoudi, M.R.; Gholizadeh, P.; Asgharzadeh, M.; Ganbarov, K.; Köse, Ş.; Yousefi, M.; Kafil, H.S. SARS-CoV-2 (COVID-19) vaccines structure, mechanisms and effectiveness: A review. Int. J. Biol. Macromol. 2021, 188, 740–750. [Google Scholar] [CrossRef] [PubMed]
- Babamahmoodi, F.; Saeedi, M.; Alizadeh-Navaei, R.; Hedayatizadeh-Omran, A.; Mousavi, S.A.; Ovaise, G.; Kordi, S.; Akbari, Z.; Azordeh, M.; Ahangarkani, F. Side effects and Immunogenicity following administration of the Sputnik V COVID-19 vaccine in health care workers in Iran. Sci. Rep. 2021, 11, 21464. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | N (%) | |
|---|---|---|
| Gender | Male | 651 (43.3) |
| Female | 849 (56.6) | |
| Occupation | Healthcare professionals | 1077(71.8) |
| Technicians | 267 (17.8) | |
| Clerks | 156 (10.4) | |
| Previous COVID-19 | Yes | 871 (58.1) |
| No | 629 (41.9) | |
| Comorbidity | No | 1362 (90.8) |
| DM | 15 (1) | |
| HTM | 25 (1.7) | |
| HTN and DM | 6 (0.4) | |
| TD | 23 (1.5) | |
| Others | 69 (4.6) | |
| Vaccine Type | FD N (%) | SD N (%) | Age (Mean-SD) | Gender N (%) | COVID-19 Positive History N (%) | Comorbidity N (%) |
|---|---|---|---|---|---|---|
| Sputnik V | 683 (45.53) | 667 (45.49%) | 35.56 (8.02) | M: 287 (42) F: 396 (58) | 350 (51.2) | DM: 8 (1.2) HTN: 9 (1.3) DM+HTN: 2 (0.3) TD: 16 (2.3) Other: 27 (3.9) |
| Sinopharm | 325 (21.66) | 314 (21.41) | 37.57 (8.98) | M: 152 (46.8) F: 173 (53.2) | 210 (64.6) | DM: 4 (1.2) HTN: 8 (2.5) DM+HTN: 3 (0.9) TD: 4 (1.2) Other: 27 (8.3) |
| Oxford AstraZeneca | 274 (16.46) | 270 (18.41) | 36.59 (7.75) | M: 138 (50.4) F: 136 (49.6) | 171 (62.4) | DM: 3 (1.1) HTN: 5 (1.8) DM+HTN: 0 (0) TD: 1 (0.4) Other: 7 (2.55) |
| Covaxin | 140 (0.09) | 137 (0.09) | 37.08 (6.29) | M: 40 (28.6) F: 100 (71.4) | 81 (57.9) | DM: 0 (0) HTN: 1 (0.7) DM+HTN: 0 (0) TD: 2 (1.4) Other: 7 (5) |
| COVIran Barekat | 78 (0.05) | 78 (0.05) | 36.50 (6.17) | M: 34 (43.6) F: 44 (56.4) | 59 (75.6) | DM: 0 (0) HTN: 2 (2.6) DM+HTN: 1 (1.3) TD: 0(0) Other: 1 (1.3) |
| Total | 1500 | 1466 | ||||
| Test p-Value | Kruskal–Wallis p-Value = 0.003 | χ2p-Value = 0.001 | χ2p-Value < 0.001 | χ2p-Value = 0.859 | ||
| Vaccine Name | Onset Time | Lasting Time | ||
|---|---|---|---|---|
| FD MR | SD MR | FD MR | SD MR | |
| Sinopharm and Covaxin | 618.57–629.79 | 623.28–708.51 * | 635.98–750.91 | 590.76–765.92 ** |
| Sinopharm and Sputnik V | 618.57–748.20 ** | 623.28–681.50 * | 635.98–784.13 ** | 590.76–758.98 ** |
| Sinopharm and Oxford AstraZeneca | 618.57–915.52 ** | 623.28–925.58 ** | 635.98–880.52 ** | 590.76–849.78 ** |
| Sinopharm and COVIran Barekat | 618.57–957.35 ** | 623.28–1000.85 ** | 635.98–475.75 * | 590.76–621.72 |
| Covaxin and Sputnik V | 629.79–748.20 * | 708.51–681.50 | 750.91–784.13 | 765.92–758.98 |
| Covaxin and Oxford AstraZeneca | 629.79–915.52 ** | 708.51–925.58 ** | 750.91–880.52 * | 765.92–849.78 |
| Covaxin and COVIran Barekat | 629.79–957.35 ** | 708.51–1000.85 ** | 750.91–475.75 ** | 765.92–621.72 |
| Sputnik V and Oxford AstraZeneca | 748.20–915.52 ** | 681.50–925.58 ** | 784.13–880.52 * | 758.98–849.78 * |
| Sputnik V and COVIran Barekat | 748.20–957.35 ** | 681.50–1000.85 ** | 784.13–475.75 ** | 758.98–621.72 * |
| Oxford AstraZeneca and COVIran Barekat | 915.52–957.35 | 925.58–1000.85 | 880.52–475.75 ** | 849.78–621.72 ** |
| Local Signs and Symptoms | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vaccine Name | N | N | Pain N (%) | Tenderness N (%) | Redness N (%) | Bruising N (%) | Swelling N (%) | Petechia N (%) | Itching N (%) | Firmness N (%) | Swollen Lymph Nodes N (%) | |||||||||
| FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | |
| Sputnik V | 683 | 667 | 305 (44.7) | 219 (32.8) | 143 (20.9) | 59 (8.8) | 19 (2.8) | 3 (0.4) | 3 (0.4) | 8 (1.2) | 27 (4) | 11 (1.6) | 4 (0.6) | 2 (0.3) | 3 (0.4) | 3 (0.4) | 44 (6.4) | 18 (2.7) | 4 (0.6) | 3 (0.4) |
| Sinopharm | 325 | 314 | 127 (39.1) | 83 (26.4) | 53 (16.3) | 26 (8.3) | 2 (0.6) | 5 (1.6) | 1 (0.3) | 0 (0.0) | 6 (1.8) | 4 (1.3) | 0 (0) | 0 (0) | 3 (0.9) | 0 (0) | 11 (3.4) | 4 (1.3) | 0 (0.0) | 0 (0.0) |
| Oxford AstraZeneca | 274 | 270 | 160 (58.4) | 131 (48.5) | 112 (40.9) | 85 (31.5) | 17 (6.2) | 4 (1.5) | 6 (2.2) | 6 (2.2) | 31 (11.3) | 12 (4.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 2 (0.7) | 45 (16.4) | 17 (6.3) | 0 (0.0) | 0 (0.0) |
| Covaxin | 140 | 137 | 62 (44.3) | 36 (26.3) | 44 (31.4) | 16 (11.7) | 2 (1.4) | 1 (0.7) | 1 (0.7) | 3 (2.2) | 23 (16.4) | 3 (2.2) | 2 (1.4) | 1 (0.7) | 1 (0.7) | 3 (2.2) | 21 (15) | 7 (5.1) | 1 (0.7) | 1 (0.7) |
| COVIran Barekat | 78 | 78 | 12 (15.4) | 5 (6.4) | 34 (43.6) | 14 (17.9) | 2 (2.6) | 0 (0) | 0 (0) | 0 (0) | 5 (6.4) | 3 (3.8) | 0 (0) | 0 (0) | 1 (1.3) | 0 (0) | 2 (2.6) | 1 (1.3) | 0 (0.0) | 0 (0.0) |
| Total | 1500 | 1466 | 666 (44.4) | 474 (31.6) | 386 (25.7) | 200 (13.6) | 42 (2.8) | 13 (0.9) | 11 (0.7) | 17 (1.2) | 92 (6.1) | 33 (2.3) | 6 (0.4) | 3 (0.2) | 8 (0.5) | 8 (0.5) | 123 (8.2) | 47 (3.2) | 5 (0.3) | 4 (0.3) |
| χ2p-Value | <0.001 | <0.001 | <0.001 | <0.001 | 0.001 | 0.282 | 0.037 | 0.074 | <0.001 | 0.055 | 0.134 | 0.477 | 0.489 | 0.055 | <0.001 | 0.004 | 0.382 | 0.458 | ||
| Systemic Signs and Symptoms | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Vaccine Type | N | N | Fever N (%) | Muscle Pain N (%) | Join Pain N (%) | Chills N (%) | Malaise N (%) | Dyspnoea N (%) | Headache N (%) | Blurred Vision N (%) | Nausea and Vomiting N (%) | |||||||||
| FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | |
| Sputnik V | 683 | 667 | 310 (45.4) | 220 (33) | 288 (42.2) | 193 (28.9) | 160 (23.4) | 117 (17.5) | 237 (34.7) | 158 (23.7) | 229 (33.5) | 126 (18.9) | 12 (1.8) | 7 (1.0) | 193 (28.3) | 124 (18.6) | 11 (1.6) | 6 (0.9) | 37 (5.4) | 20 (3) |
| Sinopharm | 325 | 314 | 79 (24.3) | 51 (16.2) | 52 (16) | 33 (10.5) | 17 (5.2) | 8 (2.5) | 40 (12.3) | 31 (9.9) | 57 (17.5) | 43 (13.7) | 6 (1.8) | 2 (0.6) | 78 (24) | 61 (19.4) | 2 (0.6) | 7 (2.2) | 10 (3.1) | 9 (2.9) |
| Oxford AstraZeneca | 274 | 270 | 201 (73.4) | 118 (43.7) | 178 (65) | 124 (45.9) | 136 (49.6) | 93 (34.4) | 174 (63.5) | 100 (37) | 128 (46.7) | 99 (36.7) | 8 (2.9) | 0 (0.0) | 124 (45.3) | 82 (30.4) | 8 (2.9) | 15 (5.6) | 12 (4.4) | 10 (3.7) |
| Covaxin | 140 | 137 | 54 (38.6) | 16 (11.7) | 43 (30.7) | 20 (14.6) | 15 (10.7) | 9 (6.6) | 40 (28.6) | 11 (8) | 24 (17.1) | 24 (17.5) | 1 (0.7) | 0 (0.0) | 59 (42.1) | 53 (38.7) | 2 (1.4) | 1 (0.7) | 31 (22.1) | 20 (14.6) |
| COVIran Barekat | 78 | 78 | 47 (60.3) | 23 (29.5) | 24 (30.8) | 12 (15.4) | 3 (3.8) | 6 (7.7) | 29 (37.2) | 14 (17.9) | 17 (21.8) | 13 (16.7) | 0 (0) | 0 (0.0) | 21 (26.9) | 9 (11.5) | 5 (6.4) | 1 (1.3) | 0 (0) | 0 (0) |
| Total | 1500 | 1466 | 691 (46.1) | 428 (29.2) | 585 (39) | 382 (26.1) | 331 (22.1) | 233 (15.9) | 520 (34.7) | 314 (21.4) | 455 (30.3) | 305 (20.8) | 27 (1.8) | 9 (0.6) | 475 (31.7) | 329 (22.5) | 28 (1.9) | 30 (2) | 90 (6) | 59 (4) |
| χ2 p-Value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.365 | 0.280 | <0.001 | <0.001 | 0.009 | <0.001 | <0.001 | <0.001 | ||
| Vaccine Type | N | N | Diarrhoea N (%) | Chest Pain N (%) | Abdominal Pain N (%) | Seizure N (%) | Drowsiness N (%) | Sweating N (%) | Pruritus N (%) | Palpitation N (%) | Allergic Reactions N (%) | |||||||||
| FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | FD | SD | |
| Sputnik V | 683 | 667 | 8 (1.2) | 5 (0.7) | 13 (1.9) | 13 (1.9) | 9 (1.3) | 8 (1.2) | 1 (0.1) | 0 (0) | 84 (12.3) | 50 (7.5) | 54 (7.9) | 20 (3) | 2 (0.3) | 2 (0.3) | 26 (3.8) | 28 (4.2) | 1 (0.1) | 0 (0) |
| Sinopharm | 325 | 314 | 9 (2.8) | 10 (3.2) | 6 (1.8) | 8 (2.5) | 3 (0.9) | 3 (1) | 0 (0) | 0 (0) | 33 (10.2) | 35 (11.1) | 4 (1.2) | 7 (2.2) | 2 (0.6) | 0 (0) | 8 (2.5) | 12 (3.8) | 3 (0.9) | 2 (0.6) |
| Oxford AstraZeneca | 274 | 270 | 5 (1.8) | 14 (5.2) | 9 (3.3) | 6 (2.2) | 0 (0) | 2 (0.7) | 0 (0) | 0 (0) | 57 (20.8) | 64 (23.7) | 34 (12.4) | 18 (6.7) | 0 (0) | 0 (0) | 18 (6.6) | 12 (4.4) | 0 (0) | 2 (0.7) |
| Covaxin | 140 | 137 | 39 (27.9) | 24 (17.5) | 0 (0) | 2 (1.5) | 30 (21.4) | 17 (12.4) | 0 (0) | 0 (0) | 12 (8.6) | 11 (8) | 7 (5) | 10 (7.3) | 0 (0) | 0 (0) | 3 (2.1) | 2 (1.5) | 0 (0) | 0 (0) |
| COVIran Barekat | 78 | 78 | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 58 (74.4) | 54 (69.2) | 2 (2.6) | 2 (2.6) | 0 (0) | 0 (0) | 0 (0) | 2 (2.6) | 0 (0) | 0 (0) |
| Total | 1500 | 1466 | 61 (4.1) | 53 (3.6) | 28 (1.9) | 29 (2) | 42 (2.8) | 30 (2) | 1 (0.1) | 0 (0) | 244 (16.3) | 214 (14.6) | 101 (6.7) | 57 (3.9) | 4 (0.3) | 2 (0.1) | 55 (3.7) | 56 (3.8) | 4 (0.3) | 4 (0.3) |
| χ2p-Value | <0.001 | <0.001 | 0.128 | 0.667 | <0.001 | <0.001 | 0.879 | <0.001 | <0.001 | <0.001 | 0.008 | 0.589 | 0.663 | 0.019 | 0.565 | 0.138 | 0.191 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zare, Z.; Assarroudi, A.; Armat, M.R.; Laal Ahangar, M.; Estaji, M.; MoghaddamHosseini, V.; Dianatinasab, M. Signs, Symptoms, and Side-Effects Presented by Different Types of COVID-19 Vaccines: A Prospective Cohort Study. Life 2022, 12, 2046. https://doi.org/10.3390/life12122046
Zare Z, Assarroudi A, Armat MR, Laal Ahangar M, Estaji M, MoghaddamHosseini V, Dianatinasab M. Signs, Symptoms, and Side-Effects Presented by Different Types of COVID-19 Vaccines: A Prospective Cohort Study. Life. 2022; 12(12):2046. https://doi.org/10.3390/life12122046
Chicago/Turabian StyleZare, Zahra, Abdolghader Assarroudi, Mohammad Reza Armat, Mojtaba Laal Ahangar, Mahdie Estaji, Vahideh MoghaddamHosseini, and Mostafa Dianatinasab. 2022. "Signs, Symptoms, and Side-Effects Presented by Different Types of COVID-19 Vaccines: A Prospective Cohort Study" Life 12, no. 12: 2046. https://doi.org/10.3390/life12122046