
Thyrotropin Levels in Patients with Coronavirus Disease 2019: Assessment during Hospitalization and in the Medium Term after Discharge
 ,
,
Abstract
:1. Introduction
2. Patients, Materials, and Methods
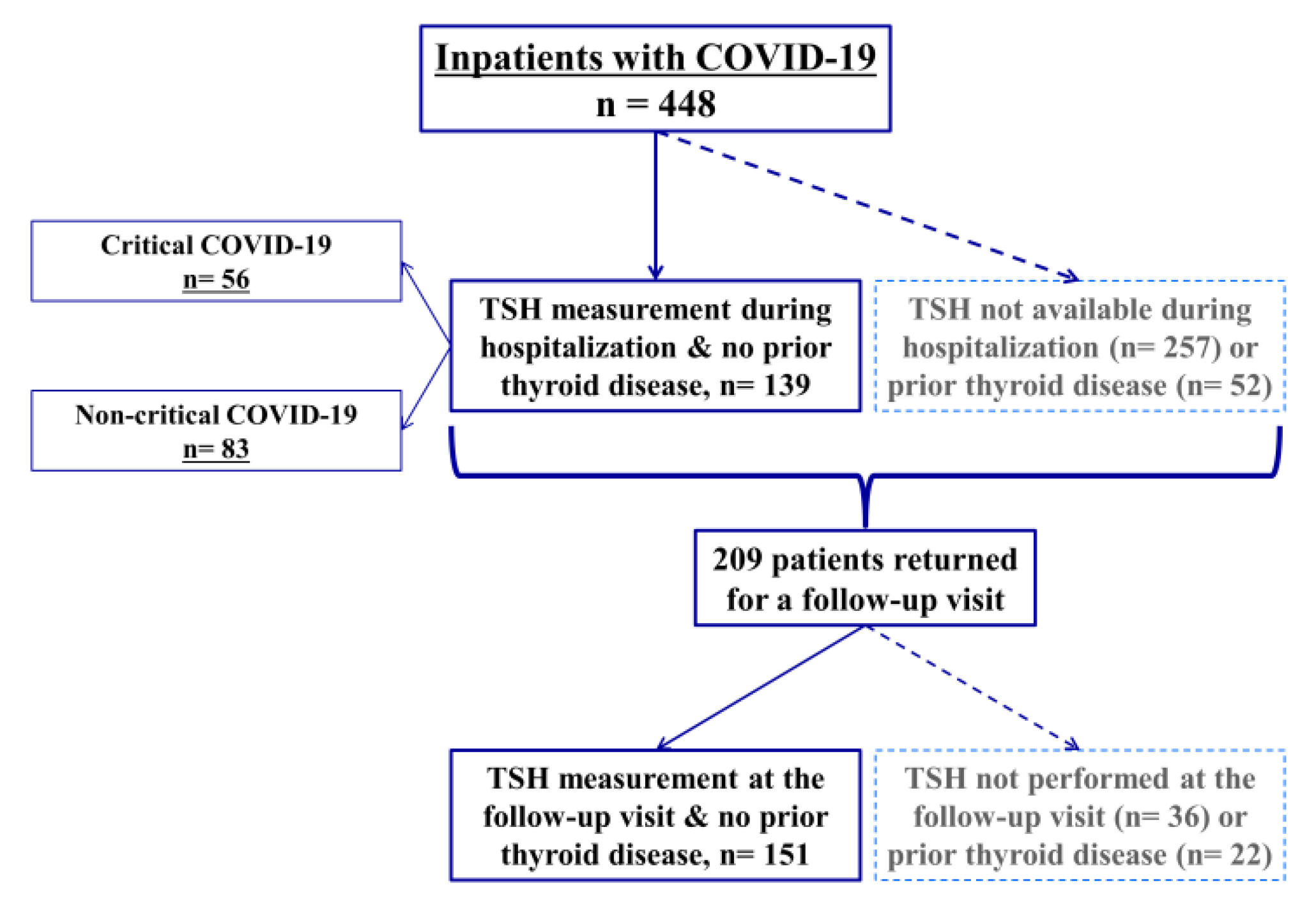
2.1. Study Population and Data Collection
2.2. Study Groups and Outcomes
2.3. Materials
2.4. Statistical Analysis
3. Results
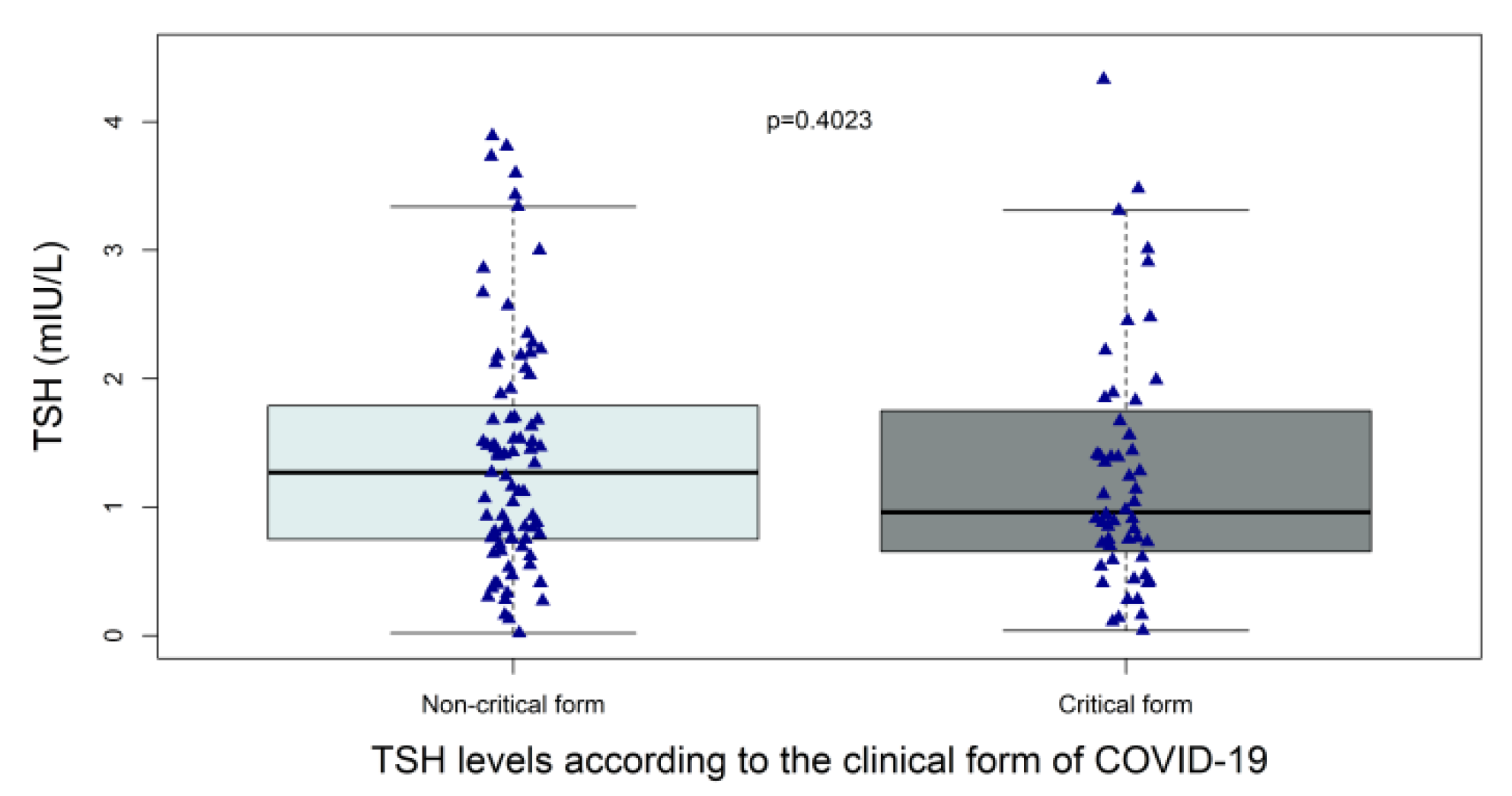
3.1. TSH Levels in the Acute Phase (the M0 Group)
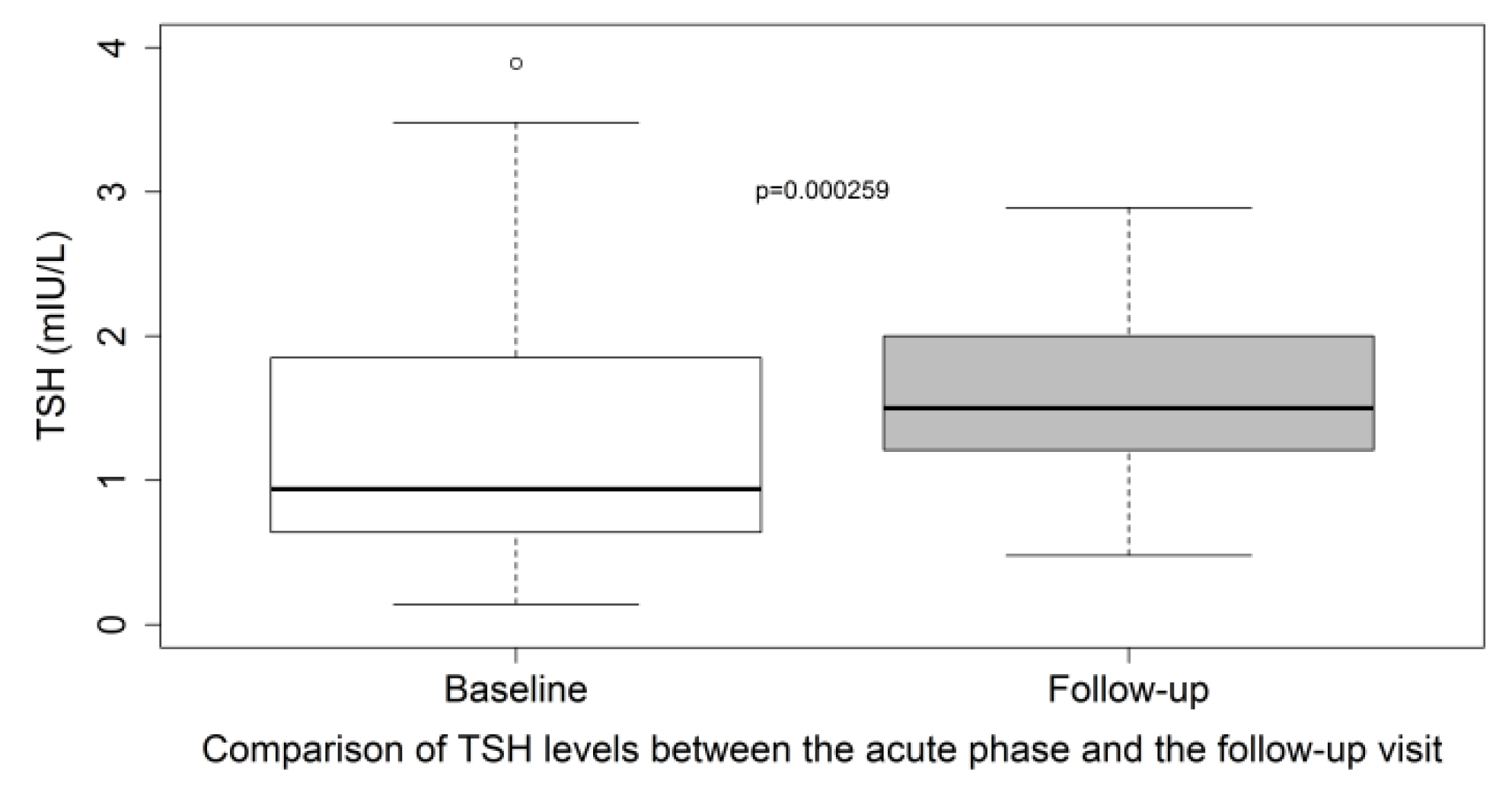
3.2. TSH Levels at the Three-Month Post-Discharge Visit (the M3 Group)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Myers, L.C.; Parodi, S.M.; Escobar, G.J.; Liu, V.X. Characteristics of Hospitalized Adults With COVID-19 in an Integrated Health Care System in California. JAMA 2020, 323, 2195–2198. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Langouche, L.; Jacobs, A.; Van den Berghe, G. Nonthyroidal Illness Syndrome Across the Ages. J. Endocr. Soc. 2019, 3, 2313–2325. [Google Scholar] [CrossRef] [Green Version]
- de Vries, E.M.; Fliers, E.; Boelen, A. The Molecular Basis of the Non-Thyroidal Illness Syndrome. J. Endocrinol. 2015, 225, R67–R81. [Google Scholar] [CrossRef] [Green Version]
- Fliers, E.; Bianco, A.C.; Langouche, L.; Boelen, A. Thyroid Function in Critically Ill Patients. Lancet Diabetes Endocrinol. 2015, 3, 816–825. [Google Scholar] [CrossRef] [Green Version]
- Van den Berghe, G. Non-Thyroidal Illness in the ICU: A Syndrome with Different Faces. Thyroid Off. J. Am. Thyroid Assoc. 2014, 24, 1456–1465. [Google Scholar] [CrossRef]
- Wei, L.; Sun, S.; Zhang, J.; Zhu, H.; Xu, Y.; Ma, Q.; McNutt, M.A.; Korteweg, C.; Gu, J. Endocrine Cells of the Adenohypophysis in Severe Acute Respiratory Syndrome (SARS). Biochem. Cell Biol. Biochim. Biol. Cell. 2010, 88, 723–730. [Google Scholar] [CrossRef]
- Sun, S.; Wei, L.; Zhang, J.; Xu, Y.; He, F.-J.; Gu, J. Pathology and immunohistochemistry of thyroid in severe acute respiratory syndrome. Zhonghua Yi Xue Za Zhi 2005, 85, 667–670. [Google Scholar]
- Wei, L.; Sun, S.; Xu, C.-H.; Zhang, J.; Xu, Y.; Zhu, H.; Peh, S.-C.; Korteweg, C.; McNutt, M.A.; Gu, J. Pathology of the Thyroid in Severe Acute Respiratory Syndrome. Hum. Pathol. 2007, 38, 95–102. [Google Scholar] [CrossRef]
- Dworakowska, D.; Grossman, A.B. Thyroid Disease in the Time of COVID-19. Endocrine 2020, 68, 471–474. [Google Scholar] [CrossRef]
- Leow, M.K.-S.; Kwek, D.S.-K.; Ng, A.W.-K.; Ong, K.-C.; Kaw, G.J.-L.; Lee, L.S.-U. Hypocortisolism in Survivors of Severe Acute Respiratory Syndrome (SARS). Clin. Endocrinol. 2005, 63, 197–202. [Google Scholar] [CrossRef] [PubMed]
- Brancatella, A.; Ricci, D.; Viola, N.; Sgrò, D.; Santini, F.; Latrofa, F. Subacute Thyroiditis After Sars-COV-2 Infection. J. Clin. Endocrinol. Metab. 2020, 105, dgaa276. [Google Scholar] [CrossRef] [PubMed]
- Brancatella, A.; Ricci, D.; Cappellani, D.; Viola, N.; Sgrò, D.; Santini, F.; Latrofa, F. Is Subacute Thyroiditis an Underestimated Manifestation of SARS-CoV-2 Infection? Insights From a Case Series. J. Clin. Endocrinol. Metab. 2020, 105, dgaa537. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.H.; Li, T.Y.; He, Z.C.; Ping, Y.F.; Liu, H.W.; Yu, S.C.; Mou, H.M.; Wang, L.H.; Zhang, H.R.; Fu, W.J.; et al. A pathological report of three COVID-19 cases by minimal invasive autopsies. Zhonghua Bing Li Xue Za Zhi 2020, 49, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Baughn, L.B.; Sharma, N.; Elhaik, E.; Sekulic, A.; Bryce, A.H.; Fonseca, R. Targeting TMPRSS2 in SARS-CoV-2 Infection. Mayo Clin. Proc. 2020, 95, 1989–1999. [Google Scholar] [CrossRef]
- Li, M.-Y.; Li, L.; Zhang, Y.; Wang, X.-S. Expression of the SARS-CoV-2 Cell Receptor Gene ACE2 in a Wide Variety of Human Tissues. Infect. Dis. Poverty 2020, 9, 45. [Google Scholar] [CrossRef]
- Rotondi, M.; Coperchini, F.; Ricci, G.; Denegri, M.; Croce, L.; Ngnitejeu, S.T.; Villani, L.; Magri, F.; Latrofa, F.; Chiovato, L. Detection of SARS-COV-2 Receptor ACE-2 MRNA in Thyroid Cells: A Clue for COVID-19-Related Subacute Thyroiditis. J. Endocrinol. Investig. 2021, 44, 1085–1090. [Google Scholar] [CrossRef]
- Wong, D.W.L.; Klinkhammer, B.M.; Djudjaj, S.; Villwock, S.; Timm, M.C.; Buhl, E.M.; Wucherpfennig, S.; Cacchi, C.; Braunschweig, T.; Knüchel-Clarke, R.; et al. Multisystemic Cellular Tropism of SARS-CoV-2 in Autopsies of COVID-19 Patients. Cells 2021, 10, 1900. [Google Scholar] [CrossRef]
- Lee, S.Y.; Rhee, C.M.; Leung, A.M.; Braverman, L.E.; Brent, G.A.; Pearce, E.N. A Review: Radiographic Iodinated Contrast Media-Induced Thyroid Dysfunction. J. Clin. Endocrinol. Metab. 2015, 100, 376–383. [Google Scholar] [CrossRef] [Green Version]
- Burch, H.B. Drug Effects on the Thyroid. N. Engl. J. Med. 2019, 381, 749–761. [Google Scholar] [CrossRef]
- Gao, W.; Guo, W.; Guo, Y.; Shi, M.; Dong, G.; Wang, G.; Ge, Q.; Zhu, J.; Zhou, X. Thyroid Hormone Concentrations in Severely or Critically Ill Patients with COVID-19. J. Endocrinol. Investig. 2021, 44, 1031–1040. [Google Scholar] [CrossRef] [PubMed]
- Lui, D.T.W.; Lee, C.H.; Chow, W.S.; Lee, A.C.H.; Tam, A.R.; Fong, C.H.Y.; Law, C.Y.; Leung, E.K.H.; To, K.K.W.; Tan, K.C.B.; et al. Thyroid Dysfunction in Relation to Immune Profile, Disease Status, and Outcome in 191 Patients with COVID-19. J. Clin. Endocrinol. Metab. 2021, 106, e926–e935. [Google Scholar] [CrossRef] [PubMed]
- Khoo, B.; Tan, T.; Clarke, S.A.; Mills, E.G.; Patel, B.; Modi, M.; Phylactou, M.; Eng, P.C.; Thurston, L.; Alexander, E.C.; et al. Thyroid Function Before, During, and After COVID-19. J. Clin. Endocrinol. Metab. 2021, 106, e803–e811. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Cui, Z.; Shi, N.; Tian, S.; Chen, T.; Zhong, X.; Qiu, K.; Zhang, J.; Zeng, T.; Chen, L.; et al. Suppression of the Hypothalamic-Pituitary-Thyroid Axis Is Associated with the Severity of Prognosis in Hospitalized Patients with COVID-19. BMC Endocr. Disord. 2021, 21, 228. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Lee, M.K.; Lee, J.H.; Sohn, S.Y. Thyroid Hormone Profile and Its Prognostic Impact on the Coronavirus Disease 2019 in Korean Patients. Endocrinol. Metab. Seoul Korea 2021, 36, 769–777. [Google Scholar] [CrossRef]
- Chen, M.; Zhou, W.; Xu, W. Thyroid Function Analysis in 50 Patients with COVID-19: A Retrospective Study. Thyroid Off. J. Am. Thyroid Assoc. 2021, 31, 8–11. [Google Scholar] [CrossRef]
- Lania, A.; Sandri, M.T.; Cellini, M.; Mirani, M.; Lavezzi, E.; Mazziotti, G. Thyrotoxicosis in Patients with COVID-19: The THYRCOV Study. Eur. J. Endocrinol. 2020, 183, 381–387. [Google Scholar] [CrossRef]
- Świątkowska-Stodulska, R.; Berlińska, A.; Puchalska-Reglińska, E. Thyroid Function, Inflammatory Response, and Glucocorticoids in COVID-19. Front. Endocrinol. 2022, 13, 939842. [Google Scholar] [CrossRef]
- Muller, I.; Cannavaro, D.; Dazzi, D.; Covelli, D.; Mantovani, G.; Muscatello, A.; Ferrante, E.; Orsi, E.; Resi, V.; Longari, V.; et al. SARS-CoV-2-Related Atypical Thyroiditis. Lancet Diabetes Endocrinol. 2020, 8, 739–741. [Google Scholar] [CrossRef]
- Asghar, M.S.; Yasmin, F.; Dapke, K.; Phadke, R.; Shah, S.M.I.; Bin Zafar, M.D. Derangements of Biochemical Markers and Thyroid Function Analysis among COVID-19-Positive Patients: A Developing Country Single-Center Experience. J. Med. Virol. 2021, 93, 5712–5717. [Google Scholar] [CrossRef]
- Chen, Y.; Li, X.; Dai, Y.; Zhang, J. The Association Between COVID-19 and Thyroxine Levels: A Meta-Analysis. Front. Endocrinol. 2021, 12, 779692. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Su, X.; Ding, Y.; Fan, W.; Zhou, W.; Su, J.; Chen, Z.; Zhao, H.; Xu, K.; Ni, Q.; et al. Thyroid Function Abnormalities in COVID-19 Patients. Front. Endocrinol. 2020, 11, 623792. [Google Scholar] [CrossRef] [PubMed]
- Malik, J.; Malik, A.; Javaid, M.; Zahid, T.; Ishaq, U.; Shoaib, M. Thyroid Function Analysis in COVID-19: A Retrospective Study from a Single Center. PLoS ONE 2021, 16, e0249421. [Google Scholar] [CrossRef] [PubMed]
- Baldelli, R.; Nicastri, E.; Petrosillo, N.; Marchioni, L.; Gubbiotti, A.; Sperduti, I.; Di Giacinto, P.; Rizza, L.; Rota, F.; Franco, M.; et al. Thyroid Dysfunction in COVID-19 Patients. J. Endocrinol. Investig. 2021, 44, 2735–2739. [Google Scholar] [CrossRef]
- Beltrão, F.E.d.L.; Beltrão, D.C.d.A.; Carvalhal, G.; Beltrão, F.E.d.L.; Brito, A.d.S.; Capistrano, K.H.R.d.; Bastos, I.H.d.A.; Hecht, F.; Daltro, C.H.d.C.; Bianco, A.C.; et al. Thyroid Hormone Levels During Hospital Admission Inform Disease Severity and Mortality in COVID-19 Patients. Thyroid Off. J. Am. Thyroid Assoc. 2021, 31, 1639–1649. [Google Scholar] [CrossRef] [PubMed]
- Llamas, M.; Garo, M.L.; Giovanella, L. Low Free-T3 Serum Levels and Prognosis of COVID-19: Systematic Review and Meta-Analysis. Clin. Chem. Lab. Med. 2021, 59, 1906–1913. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Lin, F.; Tu, W.; Zhang, J.; Choudhry, A.A.; Ahmed, O.; Cheng, J.; Cui, Y.; Liu, B.; Dai, M.; et al. Thyroid Dysfunction May Be Associated with Poor Outcomes in Patients with COVID-19. Mol. Cell. Endocrinol. 2021, 521, 111097. [Google Scholar] [CrossRef]
- Lang, S.; Liu, Y.; Qu, X.; Lu, R.; Fu, W.; Zhang, W.; Wang, H.; Hong, T. Association between Thyroid Function and Prognosis of COVID-19: A Retrospective Observational Study. Endocr. Res. 2021, 46, 170–177. [Google Scholar] [CrossRef]
- Zou, R.; Wu, C.; Zhang, S.; Wang, G.; Zhang, Q.; Yu, B.; Wu, Y.; Dong, H.; Wu, G.; Wu, S.; et al. Euthyroid Sick Syndrome in Patients With COVID-19. Front. Endocrinol. 2020, 11, 566439. [Google Scholar] [CrossRef]
- Clarke, S.A.; Phylactou, M.; Patel, B.; Mills, E.G.; Muzi, B.; Izzi-Engbeaya, C.; Choudhury, S.; Khoo, B.; Meeran, K.; Comninos, A.N.; et al. Normal Adrenal and Thyroid Function in Patients Who Survive COVID-19 Infection. J. Clin. Endocrinol. Metab. 2021, 106, 2208–2220. [Google Scholar] [CrossRef]
- Lui, D.T.W.; Lee, C.H.; Chow, W.S.; Lee, A.C.H.; Tam, A.R.; Pang, P.; Ho, T.Y.; Fong, C.H.Y.; Law, C.Y.; Leung, E.K.H.; et al. Long COVID in Patients With Mild to Moderate Disease: Do Thyroid Function and Autoimmunity Play a Role? Endocr. Pract. Off. J. Am. Coll. Endocrinol. Am. Assoc. Clin. Endocrinol. 2021, 27, 894–902. [Google Scholar] [CrossRef] [PubMed]
- Pizzocaro, A.; Colombo, P.; Vena, W.; Ariano, S.; Magnoni, P.; Reggiani, F.; Favacchio, G.; Mirani, M.; Lavezzi, E.; Voza, A.; et al. Outcome of Sars-COV-2-Related Thyrotoxicosis in Survivors of Covid-19: A Prospective Study. Endocrine 2021, 73, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Lui, D.T.W.; Lee, C.H.; Chow, W.S.; Lee, A.C.H.; Tam, A.R.; Fong, C.H.Y.; Law, C.Y.; Leung, E.K.H.; To, K.K.W.; Tan, K.C.B.; et al. Insights from a Prospective Follow-up of Thyroid Function and Autoimmunity among COVID-19 Survivors. Endocrinol. Metab. Seoul Korea 2021, 36, 582–589. [Google Scholar] [CrossRef] [PubMed]
- Vassiliadi, D.A.; Ilias, I.; Pratikaki, M.; Jahaj, E.; Vassiliou, A.G.; Detsika, M.; Ampelakiotou, K.; Koulenti, M.; Manolopoulos, K.N.; Tsipilis, S.; et al. Thyroid Hormone Alterations in Critically and Non-Critically Ill Patients with SARS-CoV-2 Infection. Endocr. Connect. 2021, 10, 646–655. [Google Scholar] [CrossRef]
- Li, G.H.-Y.; Tang, C.-M.; Cheung, C.-L. COVID-19 and Thyroid Function: A Bi-Directional Two-Sample Mendelian Randomization Study. Thyroid Off. J. Am. Thyroid Assoc. 2022, 32, 1037–1050. [Google Scholar] [CrossRef] [PubMed]
- Poma, A.M.; Proietti, A.; Macerola, E.; Bonuccelli, D.; Conti, M.; Salvetti, A.; Dolo, V.; Chillà, A.; Basolo, A.; Santini, F.; et al. Suppression of Pituitary Hormone Genes in Subjects Who Died From COVID-19 Independently of Virus Detection in the Gland. J. Clin. Endocrinol. Metab. 2022, 107, 2243–2253. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | TSH Assay Data not Available at M0 (N = 257) | TSH Assay Data Available at M0 (N = 191) | p Value | |||
|---|---|---|---|---|---|---|
| Median (IQR) or n (%) | Missing Data | Median (IQR) or n (%) | Missing Data | |||
| Demographic data | ||||||
| Age (year) | 69 (56–82) | 0 | 78 (66–86) | 0 | <0.0001 | |
| Men | 155 (60.3%) | 0 | 89 (46.6%) | 0 | 0.0041 | |
| Body mass index (kg/m²) | 29.0 (24.1–32.9) | 62 | 26.5 (22.5–31.2) | 38 | 0.0054 | |
| Smoking history | 77 | 64 | 0.593 | |||
| Never | 112 (43.6%) | 84 (44.0%) | ||||
| Former smoker | 59 (23.0%) | 35 (18.3%) | ||||
| Current smoker | 9 (3.5%) | 8 (4.2%) | ||||
| Coexisting conditions | ||||||
| Obesity | 91 (35.4%) | 56 | 52 (27.2%) | 34 | 0.0225 | |
| Diabetes | 66 (25.7%) | 0 | 61 (31.9%) | 0 | 0.168 | |
| Arterial hypertension | 144 (56.0%) | 0 | 127 (66.5%) | 0 | 0.0314 | |
| Hyperlipidemia | 81 (31.5%) | 1 | 72 (37.7%) | 0 | 0.191 | |
| Cardiovascular diseases | 134 (42.4%) | 0 | 62 (45.5%) | 0 | 0.563 | |
| Pulmonary Disease | 39 (15.2%) | 0 | 23 (12.0%) | 0.407 | ||
| Chronic kidney disease | 37 (14.4%) | 0 | 31 (16.2%) | 0 | 0.597 | |
| Cancer | 41 (15.9%) | 0 | 33 (17.3%) | 0 | 0.797 | |
| Thyroid disease | 18 (7.0%) | 0 | 52 (27.2%) | 0 | <0.0001 | |
| Main laboratory findings on admission | ||||||
| Glycaemia (mmol/L) | 6.7 (5.8–7.9) | 27 | 6.5 (5.6–8.5) | 12 | 0.691 | |
| GFR (MDRD mL/min/1.73 m²) | 81.5 (56–110) | 5 | 79 (55–99) | 0 | 0.507 | |
| ALAT >40 U/L | 81 (31.5%) | 32 | 51 (26.7%) | 11 | 0.110 | |
| ASAT > 40 U/L | 127 (49.4%) | 31 | 93 (48.7%) | 11 | 0.367 | |
| GGT > ULN | 107 (41.6%) | 42 | 84 (44%) | 17 | 0.838 | |
| WBC × 109 per L | 6.4 (5–9.1) | 6 | 6.5 (4.6–9.2) | 0 | 0.868 | |
| Lymphocytes × 109 per L | 0.9 (0.6–1.2) | 6 | 0.8 (0.6–1.2) | 0 | 0.340 | |
| CRP mg/L | 89.2 (42.0–152.1) | 7 | 82 (25.3–160.6) | 0 | 0.332 | |
| Patient N° | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | 51 | 81 | 69 | 71 | 70 | 80 | 64 | 89 | 67 | 88 | 56 | 29 | 92 | 45 | 72 | 59 | 65 |
| Sex (M = Male, W = female) | M | M | W | W | M | W | M | W | M | W | M | M | W | W | M | W | M |
| TSH (N: 0.4–4 mIU/L) | 0.33 | 0.28 | 0.13 | 0.28 | 0.37 | 0.3 | 0.16 | 0.27 | 0.04 | 0.16 | 0.11 | 0.14 | 0.02 | 0.28 | 7.3 | 4.3 | 15.0 |
| fT4 (N: 11.5–22.7 pmol/L) | NA | NA | 15.9 | 16 | 16.9 | 17.2 | 8.5 | NA | NA | 17.9 | 11.6 | 10.7 | NA | 15.5 | 10.1 | NA | 9.4 |
| fT3 (N: 3.5–6.5 pmol/L) | NA | NA | 4.6 | 3.8 | 2.94 | NA | 2.7 | NA | NA | 3.3 | 2.8 | 3.4 | 4.6 | 3.0 | 3.6 | NA | 4.1 |
| Critical form of COVID-19 | No | No | No | Yes | No | No | Yes | No | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes |
| Patient N° | I | II | III | IV | V | VI | VII |
|---|---|---|---|---|---|---|---|
| Age (years) | 43 | 69 | 67 | 51 | 56 | 38 | 77 |
| Sex (M = Male, W = female) | W | W | M | W | W | M | W |
| TSH (mIU/L) | 0.31 | 0.36 | 0.27 | 4.5 | 5.8 | 7.5 | 10.4 |
| fT4 (pmol/L) | 13.6 | 1.5 | 12.9 | 13.3 | 14.9 | 15.7 | 15.5 |
| fT4 within normal limits | Yes | Low | Yes | Yes | Yes | Yes | Yes |
| fT3 (pmol/L) | NA | NA | NA | NA | NA | NA | NA |
| Interval between admission and TSH assay (days) | 147 | 99 | 167 | 84 | 144 | 95 | 129 |
| TSH during hospitalization | NA | NA | NA | NA | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Salameh, A.; Scherman, N.; Adda, I.; André, J.; Zerbib, Y.; Maizel, J.; Lalau, J.-D.; Brochot, E.; Andrejak, C.; Desailloud, R. Thyrotropin Levels in Patients with Coronavirus Disease 2019: Assessment during Hospitalization and in the Medium Term after Discharge. Life 2022, 12, 2014. https://doi.org/10.3390/life12122014
Al-Salameh A, Scherman N, Adda I, André J, Zerbib Y, Maizel J, Lalau J-D, Brochot E, Andrejak C, Desailloud R. Thyrotropin Levels in Patients with Coronavirus Disease 2019: Assessment during Hospitalization and in the Medium Term after Discharge. Life. 2022; 12(12):2014. https://doi.org/10.3390/life12122014
Chicago/Turabian StyleAl-Salameh, Abdallah, Noémie Scherman, Imane Adda, Juliette André, Yoann Zerbib, Julien Maizel, Jean-Daniel Lalau, Etienne Brochot, Claire Andrejak, and Rachel Desailloud. 2022. "Thyrotropin Levels in Patients with Coronavirus Disease 2019: Assessment during Hospitalization and in the Medium Term after Discharge" Life 12, no. 12: 2014. https://doi.org/10.3390/life12122014